Dyslipidemia: What s New In The Guidelines?
|
|
|
- Herbert Sutton
- 6 years ago
- Views:
Transcription
1 1 Dyslipidemia: What s New In The Guidelines? Rhonda Cooper-DeHoff, Pharm D, MS Associate Professor Colleges of Pharmacy and Medicine University of Florida Disclosures 2 No actual or perceived conflicts of interest to report
2 Suggested Reading ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. JACC 2014;63: ACC/AHA Guideline on the Assessment of Cardiovascular Risk. JACC 2014;63: ACC/AHA Guideline on Lifestyle Management to Reduce Cardiovascular Risk. JACC 2014;63: Learning Objectives 4 Recognize how the new cholesterol treatment guidelines differ from previous cholesterol treatment guidelines Recall which groups of patients would benefit from treatment with a statin Promote appropriate dose of statin according to specific patient characteristics
3 Intent of the Guideline 5 Evidence foundation for treatment of cholesterol in adults ( 21 years of age) Review ASCVD related RCTs, systematic reviews and meta-analyses Prevention Primary and Secondary Goal simplify the decision regarding initiation of therapy Substantial Changes of 2013 Cholesterol Guidelines Key Points 6 No more treatment goals of LDL < 100 mg/dl or < 70 mg/dl Identified 4 groups for primary and secondary prevention Important to match up the appropriate intensity level of statin therapy to achieve relative reductions in LDL New global risk assessment tool developed Safety recommendations


4 Classification of Evidence Cholesterol Treatment Guidelines 8
5 CQ1 What is the evidence for LDL or non-hdl goals in Secondary Prevention No data regarding treatment or titration to a specific LDL-C goal in adults with CHD or CVD Insufficient evidence to support setting LDL-C goals in CHD or CVD 9 No RCTs that reported non-hdl levels CQ2 What is the evidence for LDL or non-hdl goals in Primary Prevention 10 RCT not available regarding dose titration to achieve a specific LDL goal Insufficient evidence in women without CHD or CVD to evaluate the reduction in CVD risk with achieved LDL < 130 or < 100 mg/dl Six RCTs - no evidence regarding dose titration to achieve a specific LDL-C goal in primary prevention
6 2013 Cholesterol Treatment Guidelines 11 Meant to define practices that meet the needs of patients in most circumstances Not a replacement for clinical judgment Ultimate decision about care of a particular patient must be made Shared by the healthcare Decision provider and Making patient in light of patient specific circumstances In caring for most patients, clinicians can employ the recommendations confidently to reduce the risk of ASCVD Lifestyle as the Foundation 12 Therapeutic Lifestyle Change Remains a crucial component of health promotion and ASCVD risk reduction Heart Healthy Diet vegetables, fruits and whole grains low fat dairy products, poultry, fish, legumes, nontropical vegetable oils, nuts limits sweets, sugar sweetened beverages, red meats Exercise adults should engage in aerobic physical activity to lower LDL and non-hdl cholesterol 3-4 sessions per week, lasting 40 minutes per session Moderate to vigorous intensity physical activity
7 Statin Are King 13 LDL-C lowered* Inflammation reduced Vulnerable plaques stabilized Endothelial function restored Ischemic episodes reduced Cardiac events reduced* Days Years * Time course established Initiating Statins 14 Benefit exceeds risk of initiating statins in 4 treatment groups Anyone with clinical ASCVD Anyone with LDL-C 190 mg/dl Anyone yo w/ DM & LDL mg/dl Anyone yo w/out DM, w/ 10 yr ASCVD risk 7.5%

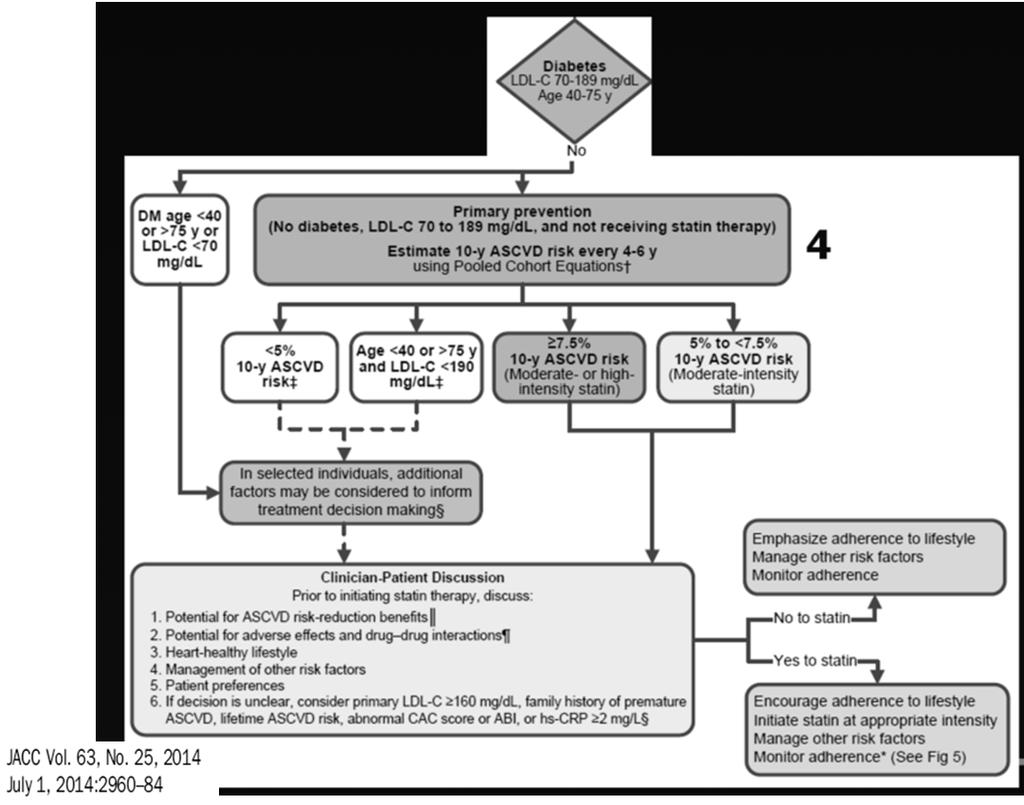
8 Initiating Statins Group Initiating Statins Group 4 16
9 High Intensity Statin Therapy 17 Daily dose lowers LDL-C, on average by 50% atorvastatin mg rosuvastatin 20 (40) mg Moderate Intensity Statin Therapy 18 Daily dose lowers LDL on average by 30% - < 50% Atorvastatin 10 (20) mg Rosuvastatin (5) 10mg Simvastatin 20-40mg Pravastatin 40 (80) mg Lovastatin 40mg Fluvastatin XL 80mg Fluvastatin 40mg bid Pitavastatin 2-4mg

10 Low Intensity Statin Therapy 19 Daily dose lowers LDL on average by < 30% Simvastatin 10 mg Pravastatin mg Lovastatin 20 mg Fluvastatin mg Pitavastatin 1 mg Initiating Statins Group
 Dose-dependent phenomenon that is usually reversible Hepatocyte 15.4% incidence of myalgias* (18.7% incidence in control arm) 0.9% incidence of myositis (0.")

11 Statin Adverse Effects 74,102 subjects in 35 randomized clinical trials with statins % incidence of elevated hepatic transaminases (1.1% incidence in control arm) Dose-dependent phenomenon that is usually reversible Hepatocyte 15.4% incidence of myalgias* (18.7% incidence in control arm) 0.9% incidence of myositis (0.4% incidence in control arm) 0.2% incidence of rhabdomyolysis (0.1% incidence in control arm) Skeletal myocyte *The rate of myalgias leading to discontinuation of atorvastatin in the TNT trial was 4.8% and 4.7% in the 80 mg and 10 mg arms, respectively Source: Kashani A et al. Circulation 2006;114: Statin Safety (CQ3) 22 Characteristics predisposing to statin AEs Multiple comorbidities, impaired renal or liver fxn Hx of statin intolerance or muscle disorders Unexplained ALT elevations 3 x ULN Concomitant use of drugs affecting statin metabolism Age > 75 yo Hx hemorrhagic stroke Asian ancestry
12 Statin Safety (CQ3) 23 Creatine Kinase (CK) Baseline CK should not be measured routinely before starting statin Baseline CK reasonable for patient believed to be at increased risk for adverse muscle events During statin therapy, reasonable to measure CK in patients with muscle symptoms Hepatic Transaminase (ALT) Baseline ALT should be obtained before starting statin During statin therapy, reasonable to measure ALT if patient has symptoms of hepatotoxicity Statin Safety (CQ3) 24 Decreasing the statin dose may be considered when 2 consecutive values of LDL are < 40 mg/dl Harmful to initiate simvastatin at 80mg qd or increase dose to 80mg qd Glucose should be monitored routinely if diabetes develops, not an indication to stop statin






")


13 Statin Safety (CQ3) 25 Obtain history of prior or current muscle symptoms to establish baseline If unexplained severe muscle symptoms or fatigue develop If mild to moderate muscle symptoms develop Confusion or memory impairment Pain, tenderness, stiffness, cramping, weakness, fatigue Promptly discontinue statin Address possibility of rhabdo (CK, creatinine, UA for myoglobin) Discontinue statin Evaluate for other conditions that might contribute If symptoms resolve rechallenge statin (same or lower dose) Evaluate for nonstatin causes as well as statin association Statin Safety - FDA Feb 2012 Update 26 Simvastatin dosing guidelines (CYP3A4) Patients taking diltiazem or verapamil 5-10mg, 10mg max Patients taking amiodarone, amlodipine or ranolazine 5-20 mg, 20 mg max Due to risk of developing myopathy and/or rhabdomyolysis on the combo Contraindicated with Lovastatin (and RYR)

14 Statin Monitoring 27 Statin Monitoring Adherence to statin and TLC Fasting lipids panel within 4-12 weeks after initiation or dose adjustment of statin Fasting lipid panel every 3-12 months after dose stable 28 Optimize statin therapy Maximum tolerated intensity of statin should be used if recommended intensity is not tolerated Insufficient response to statin therapy Reinforce adherence (statin and TLC) Exclude secondary causes of hyperlipidemia High intensity statin 50% LDL reduction Moderate intensity statin 30-50% LDL reduction LDL levels and % reduction used only to assess response and adherence
15 Non Statin Therapies Offer No Benefit 29 Statins response not as expected Statins not tolerated at recommended intensity Statin intolerance Treatment of hypertriglyceridemia (TG > < 500) 30 Intensive Life-style modifications weight control (reduction if necessary) increased physical activity restriction of alcohol restriction of dietary fat in extreme cases Diabetes GOOD GLYCEMIC CONTROL IS CENTRAL TO CONTROLLING TRIGLYCERIDES

16 Fibric Acids: Place in therapy 31 Lower TG but not CV risk Do not initiate gemfibriozil in patient on statin increased risk for muscle symptoms Consider fenofibrate in combo with low or moderate intensity statin when TG 500 mg/dl Monitor renal status when fenobribrate is prescribed Omega 3 Fatty Acids Can be used if TG 500 mg/dl 32 Not associated with decreased risk for CVD 3-4g/day of DHA+EPA 45% in TG 2 fish meals/week can provide about mg/day of DHA+EPA
 is the product of yeast (Monascus purpureus) grown on rice.")




17 Red Yeast Rice (RYR) 33 Name Red Yeast Rice ~ mg bid Red yeast rice (RYR) is the product of yeast (Monascus purpureus) grown on rice. Used as a condiment in Asia. Efficacy Becker DJ et al. Ann Intern Med. 2009,150: Double Blind, Placebo Control, 62 statin intolerant pts (myalgias) x 24 wks Dose 6.12mg monacolin K qd, LDL 35mg/dl, no diff in pain severity score at 12 or 24 wk Halbert SC et al. Am J Cardiol. 2010;105: Double Blind, prava 20mg vs RYR 2400mg bid, 43 statin intolerant pts (myalgias) x 12 wks Dose 9.96mg monacolin K qd, PO w/drawal of tx no difference in PO (1 RYR v 2 Prava), no diff in muscle strength, LDL RYR 30%, Prava 27% 34 Gordon RY et al. Arch Int Med 2010;170:




18 Evidence Gaps 35 Other race/ethnic groups Younger diabetics Use of statins for primary prevention in adults > 75 Benefits of various lipid therapy combos in ASCVD risk reduction (not lipid changes) Risk of new onset diabetes associated with statin therapy No specific recommendations on NYHA Class II-IV heart failure or patients on maintenance hemodialysis 36
19 Take Home Messages Pharmacist Involvement Screening identification of patients at risk Monitoring and management of adverse effects Partnering with the patient for adherence strategies Identification of appropriate statin intensity Health coaching emphasis on lifestyle modifications 37 Change of mindset with monitoring No longer focused on LDL level Despite criticisms, implementation has happened Millions more treated with statins Issues with access, cost, long term effects of new DM Take Home Messages 38 Who should get which therapy at what intensity Focus on statin intensity in high risk groups instead of specific target LDL level 4 groups for statin therapy New global risk assess tool Considers risk reduction benefits and adverse effects of statin treatment Clinical ASCVD LDL level 190 mg/dl Patients with DM age w/ LDL mg/dl 7.5% estimated 10 year ASCVD risk and age 40-75
20 39 HYPERLIPIDEMIA CASES Stephen, a 52-year-old white jogger with a BMI of 25, wants you to assess his cardiovascular risks. He had scheduled his visit after taking his father to another physician to discuss his father s blindness, which is related to type 2 diabetes. Both his parents have hypertension that is controlled with medication; neither smokes. Stephen is here to discuss the results of blood tests that had been performed before the day of the visit. I m an accountant, Doc, and I live by the numbers. I don t want to be my father in 20 years, he says. He tells you that he has recently increased his running regimen to 3 miles a day and that he smokes a halfpack a day during tax season, when he is under stress. 40
21 41 Total cholesterol level is 180 mg/dl, HDL is 35 mg/dl, triglyceride level is 150 mg/dl, and the calculated low-density lipoprotein (LDL) cholesterol level is 115 mg/dl. His blood pressure is 130/85 mm Hg. You think this is a great opportunity for shared decision making and explain that although his LDL cholesterol level is not high, he has three risk factors for heart disease and stroke low HDL, smokes, and is a man You explain his estimated 10 -year risk of an event such as a heart attack or stroke is 10.9% What do you want to do????? Do not begin a statin 2. Begin a statin but monitor LDL 3. Begin a statin and do not monitor LDL
22 43 Polling Results 44 Readers from 97 countries cast 1641 votes 57% (931 readers) favored not starting a statin at all 26% (432) would start therapy but monitor the LDL cholesterol level 17% (278) would start a statin and not monitor the LDL cholesterol level Responses were independent of geography
23 Reader Comments 45 Many advocated for lifestyle modifications, including improved diet and exercise, stress management, and, most of all, smoking cessation They stated that statins should not be considered a substitute for interventions that could contribute much more substantially to lifelong health for Stephen Some were concerned that statin treatment might actually reduce the motivation to adopt a healthier lifestyle Many acknowledged a lack of consensus regarding how long physicians should wait before they initiate statin treatment Case A 63-year-old man is seen in the office 2 weeks after a STelevation myocardial infarction (MI). A former smoker with hypertension, he was discharged on atorvastatin 80mg daily, dual anti-platelet therapy, long-acting metoprolol, and an ACE inhibitor. One year before the acute MI, he was prescribed simvastatin 40 mg which was then increased to simvastatin 80 mg. He stopped the simavastatin 80 mg 2 weeks later after developing muscle cramps in his legs. At that time he was also on a calcium channel blocker for his hypertension. Although he has no muscle symptoms since he started the atorvastatin 80 mg, he is concerned about having had muscle cramps in the past on a statin and would like to decrease the atorvastatin to 20 mg daily.
24 Case Example Which of the following statements is the best answer? a) Randomized trials of high intensity statin therapy versus moderate intensity statin therapy have not shown a significant difference in outcomes. He should decrease the atorvastatin to 20 mg to minimize adverse effects. b) Systematic meta-analyses of randomized clinical trials support using an intensive statin dose such as atorvastatin 80 mg/day over a moderate intensity statin. He should stay on atorvastatin 80 mg. c) He should be followed with creatine kinase (CK) values when his lipids are checked at each visit for the first year. d) Although his liver panel was normal in the hospital, he should have an alanine aminotransferase (ALT) done at each subsequent visit. Case Example After 2 years of treatment with atorvastatin 80 mg daily free of muscle symptoms, the patient developed progressive muscle pains in both lower legs. He stopped the statin 2 weeks prior to his clinic visit but the muscle pain and weakness did not noticeably improve. He now wants to know if he can be switched to red yeast rice. On examination, he has mild difficulty getting out of a chair and also has weakness after doing 3 squats. He remembers he felt fine doing squats at the gym about 6 months ago.
25 Case Example Which of the following is the best answer? a) He should be switched from the atorvastatin 80 mg daily to red yeast rice based on evidence in U.S. studies. b) He should be switched to rosuvastatin 40 mg daily and given CoQ10. c) He should be rechallenged with atorvastatin 80 mg daily. d) He should stay off the statin until he is evaluated for possible causes of his muscle problems. A useful approach is to look for exogenous causes (e.g., medications, alcohol), systemic causes (examples include hypothyroidism, rheumatologic disorders such as polymyalgia rheumatica), and primary muscle disorders. He should be questionedabout a family history of primary muscle disorders or others in the family with muscle problems taking a statin. e) If he is African-American, CK levels are not useful in evaluating muscle symptoms. Case Example A 44-year-old woman has a 10-year history of type 2 diabetes. She is a nonsmoker with well-controlled hypertension and microalbuminuria. She is on dietary management, metformin, and takes one omega-3 fatty acid capsule with 840 mg of EPA and DHA. She also takes lisinopril and hydrochlorothiazide for her blood pressure. She has a family history of diabetes, but not premature ASCVD. She has a BP 134/78 and a BMI of Her fasting lipid panel reveals an LDL-C 95 mg/dl, triglycerides 350 mg/dl, and HDL-C 38 mg/dl. Her hemoglobin A1c is 7.5%.
26 Case Example Which of the following statements is the best answer? a) Her LDL-C is under 100 mg/dl so she is at "goal" and does not require a statin. b) She should start simvastatin 20 mg and fenofibrate 160 mg daily. c) To reduce her risk of an ASCVD event, the dose of omega-3 fatty acid should be increased to 4 capsules daily to lower her triglycerides. d) If she does not want to start a statin, a bile acid sequestrant is the next best choice for her. e) Her 10-year ASCVD risk should be calculated to determine if she needs a high- or moderate-intensity statin. Case Example A 26-year-old woman has an LDL-C of 260 mg/dl, HDL-C of 51 mg/dl, and triglycerides of 102 mg/dl. She reports having elevated LDL-C levels of over 200 mg/ dl since her teens and has tried various diets without success but has never taken a drug to lower her cholesterol. She is worried because her father died suddenly at age 38 and her father's brother had a myocardial infarction at age 32. Both were smokers. She is currently on a 2nd generation oral contraceptive and wonders if she should get off the contraceptive pill since she is engaged to be married in 6 months. She has an occasional cigarette and says that it is "social smoking." On exam, BP is 110/60 mm Hg and BMI is 24. She has bilateral inferior pole corneal arcus, no xanthelasma, and thickened Achilles tendons. Her cardiovascular examination is normal.
27 Case Example Which of the following is the best answer? a) She likely has heterozygous familial hypercholesterolemia and should start a high-intensity statin. b) If her fiancee has normal cholesterol values, the likelihood of her child having her genetic condition is 1 in 4. c) Cigarette smoking should be stopped because she is thinking about becoming pregnant. d) She should have her oral contraceptive stopped and started on a high- intensity statin. e) She should have an estimation of her 10-year risk of an ASCVD event before deciding if she needs statin therapy Case Example A 60-year-old African-American woman has asked whether she should be taking a statin to reduce her risk of stroke, but is worried about the statin causing diabetes. Her mother had diabetes and had a stroke at age 62. She is a nonsmoker. Blood pressure is 142/88 mm Hg on 2 antihypertensive medications and BMI is 31. Her fasting lipid panel reveals a total cholesterol 200 mg/dl, HDL-C 55 mg/dl, triglyceride 100 mg/dl, and LDL-C 125 mg/dl. Her fasting blood sugar is 109 mg/dl and hemoglobin A1c is 5.9%. According to the Pooled Cohort Equation for African-American Women, her estimated 10-year ASCVD risk is 8.7 %.
28 Case Example Which of the following statements is the best answer? a) She should focus on lifestyle change to improve her risk factors because lifestyle has been shown to reduce ASCVD events more than statin therapy. b) The risk of progression to diabetes with a statin outweighs any ASCVD risk reduction benefits from statin therapy. The decision about a statin should be deferred. c) She should start a moderate or high intensity statin. d) A high-sensitivity C-reactive protein (hs-crp) >2 would be needed before the decision can be made whether to start a statin. Case Example A 35-year-old man has a strong family history of premature coronary disease, with both father and brother having an MI before age 55. He is a nonsmoker, nondiabetic and exercises for 150 minutes/week. He has gained 10 lbs since age 18. His BP is 140/90 mm Hg, weight is 170 pounds, height is 5 8, and BMI is On a fasting lipid panel, his LDL-C is 160 mg/dl, HDL-C 45 mg/dl and triglyceride 100 mg/dl. His fasting blood glucose is 92 mg/dl. He is on a heart-healthy diet and exercises 150 minutes a week. He and his wife would like to discuss statin therapy given his strong family history.
29 Case Example Which of the following is likely to be helpful in making a decision regarding statin therapy in this patient? a) Strong family history of premature ASCVD b) Coronary calcium score of 300 units or more c) hs-crp 2.0 mg/l d) Lifetime risk of ASCVD e) LDL-C 160 mg/dl f) All of these factors can be considered Clinical Case A 32-year-old Caucasian man has gained 35 pounds since he graduated from college and started working as computer programmer. He has never smoked. He has treated hypertension. He has tried several popular diets to lose weight and lost about 20 pounds each time, but he always regains the weight lost within one year. He bowls once a week. He weighs 220 lbs and his BMI is 32.5, and the highest it has ever been. His BP is 138/92. His labs show total cholesterol 218 mg/dl, triglycerides 188 mg/dl, HDL-C 40 mg/dl, LDL-C 138 mg/dl, and non HDL-C 178 mg/dl. His fasting glucose is 101 mg/dl. His father died of an MI at age 73.
30 Clinical Case Which of the following should be incorporated into your advice for ASCVD risk reduction for him? a) Refer to a program providing a series of group counseling comprehensive lifestyle change sessions. b) Start a moderate intensity statin. c) Try to encourage a diet that will get at least pounds off in 6 weeks so he can keep his motivation for weight loss high. d) Reassure him that by following a strict diet he does not need to increase his physical activity and will be able to maintain his weight over the long haul. e) Refer for bariatric surgery. Case Example This 55-year-old man developed exertional chest pain. He had a positive stress exercise test and a coronary angiogram that revealed 2-vessel nonobstructive coronary disease. His risk profile indicates he is a nonsmoker with treated hypertension, and a low HDL-C. His father had an MI at age 67. His mother had type 2 diabetes diagnosed at age 60. He is on a low dose aspirin, long acting beta blocker, a high-intensity statin, and an ACE inhibitor. His BP 135/86, pulse 58, weight 183 lbs and BMI His LDL-C is 95 mg/dl, his HDL-C 39 mg/d and triglycerides are 145 mg/dl. His fasting glucose is 109 mg/dl. He wants to know what dietary change recommendations you would make. His cardiologist has given him physical activity recommendations.
31 Case Example - 9 The best answer is: 61 a) His lifestyle is not important as long as he is on a statin and beta blocker. b) He should consume a dietary pattern that emphasizes vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils and nuts; and limits intake of sweets, sugar- sweetened beverages and red meats. c) Fatty meats should be restricted, but not processed meats. d) Not adding salt is crucial because the salt in food is negligible. e) A Mediterranean style diet that allows commercial baked goods and French fries. Case Example A 48-year-old man with familial hypercholesterolemia and history of 3-vessel coronary artery bypass surgery 7 years ago sees you now for statin intolerance. The maximum dose of statin that he can tolerate is rosuvastatin 10 mg twice a week. On more frequent dosing he developed shoulder, low back, and thigh aching without weakness and a normal CK level. He had similar symptoms on low doses of simvastatin, atorvastatin and pravastatin. On rosuvastatin 10 mg twice a week, his most recent LDL-C was 168 mg/dl, triglycerides were 138 mg/dl, and HDL-C was 46 mg/dl.
32 Case Example - 10 Which of the following statements is the most correct answer? 63 a) Ezetimibe has been shown to further reduce ASCVD events when added to statin therapy. He should continue the rosuvastatin and ezetimibe 10 mg should be added. b) Gemfibrozil has been shown to reduce ASCVD events when used as monotherapy in men with coronary heart disease. He should continue the rosuvastatin and gemfibrozil 600 mg twice daily should be added. c) Bile acid sequestrants have been shown to reduce ASCVD events when used as monotherapy in men with primary hypercholesterolemia. He should continue the rosuvastatin and cholestyramine 4 g packet twice daily should be added. d) He should discontinue the rosuvastatin and begin lovastatin 40 mg daily.
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Pharmacology Challenges: Managing Statin Myalgia
 Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Major recommendations for statin therapy for ASCVD prevention
 2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Treatment of Cholesterol in 2018: Time to Level Up. Most Important Slide. Three Things Learned that Will be Applied
 Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
CPE Session 7. Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction
 CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation,
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation,
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Lipid Update AHA/ACC 2013 Guidelines
 Lipid Update AHA/ACC 2013 Guidelines Jessica M. Fleagle (Bender) D.O. University of Missouri School of Medicine Assistant Professor of Clinical Medicine Associate Program Director of Medicine Residency
Lipid Update AHA/ACC 2013 Guidelines Jessica M. Fleagle (Bender) D.O. University of Missouri School of Medicine Assistant Professor of Clinical Medicine Associate Program Director of Medicine Residency
Primary Prevention Patients aged 85yrs and over
 Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Lecture 36 Dyslipidemia Therapeutics Barry LIPIDS:
 LIPIDS: PATHOPHYSIOLOGY: TC or LDL-C = CVD HDL-C = CVD Association between TG and CVD not established o HyperTG associated with pancreatitis o Reducing TG w/ drug therapy doesn t CVD TYPES OF DYSLIPIDEMIA:
LIPIDS: PATHOPHYSIOLOGY: TC or LDL-C = CVD HDL-C = CVD Association between TG and CVD not established o HyperTG associated with pancreatitis o Reducing TG w/ drug therapy doesn t CVD TYPES OF DYSLIPIDEMIA:
2.3 CONTACT HOURS. Managing. By Kristine Anne Scordo, PhD, RN, ACNP-BC, FAANP
 2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients
 Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients Joe Anderson, PharmD, PhC, BCPS James Nawarskas, PharmD, PhC, BCPS Gretchen Ray, PharmD, PhC, BCACP University of
Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients Joe Anderson, PharmD, PhC, BCPS James Nawarskas, PharmD, PhC, BCPS Gretchen Ray, PharmD, PhC, BCACP University of
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
FORTH VALLEY. LIPID LOWERING GUIDELINE v5 2016
 FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Pharmacy Management Drug Policy
 SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Clinical Policy: Lomitapide (Juxtapid) Reference Number: ERX.SPA.170 Effective Date:
 Reference Number: ERX.SPA.170 Effective Date:") Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Coronary Artery Disease Clinical Practice Guidelines
 Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
DYSLIPIDEMIA PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Praluent. Praluent (alirocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Volume 2; Number 11 July 2008
 Volume 2; Number 11 July 2008 CONTENTS Page 1 NICE Clinical Guideline 67: Lipid Modification (May 2008) Page 7 NICE Technology Appraisal 132: Ezetimibe for the treatment of primary (heterozygous familial
Volume 2; Number 11 July 2008 CONTENTS Page 1 NICE Clinical Guideline 67: Lipid Modification (May 2008) Page 7 NICE Technology Appraisal 132: Ezetimibe for the treatment of primary (heterozygous familial
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Disclosure. A New Partnership. Objectives 03/27/2014. What is the main way you have obtained information about the 2013 ACC/AHA Cholesterol Guideline?
 Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Objec ves To discuss the process of formulation of guidelines and how this may differ among professional societies 5/14/15
 Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Achieving Lipid Goals: 2008 Update. Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy
 Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Supplement Table 2. Categorization of Statin Intensity Based on Potential Low-Density Lipoprotein Cholesterol Reduction
 Supplement: Tables Supplement Table 1. Study Eligibility Criteria Supplement Table 2. Categorization of Statin Intensity Based on Potential Low-Density Lipoprotein Cholesterol Reduction Supplement Table
Supplement: Tables Supplement Table 1. Study Eligibility Criteria Supplement Table 2. Categorization of Statin Intensity Based on Potential Low-Density Lipoprotein Cholesterol Reduction Supplement Table
1/14/2013 Pediatric Cardiovascular Disease and the Future of our Children Linda Alwine FNP-BC Objectives Identify the prevalence and epidemiology of h
 Pediatric Cardiovascular Disease and the Future of our Children Linda Alwine FNP-BC Objectives Identify the prevalence and epidemiology of hyperlipidemia. Identify risk factors that lead to the development
Pediatric Cardiovascular Disease and the Future of our Children Linda Alwine FNP-BC Objectives Identify the prevalence and epidemiology of hyperlipidemia. Identify risk factors that lead to the development
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Helen Williams Consultant Pharmacist for CV Disease - South London
 Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
Guidelines on Lowering LDL-C Levels
 Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha