Blank DISCLOSURES 1/17/2017 COMPLEX VALVE CASES CHALLENGES IN EVALUATING AND MANAGING MULTIVALVULAR HEART DISEASE ECHO HAWAII 1/23/17 NONE
|
|
|
- Tamsyn Davidson
- 5 years ago
- Views:
Transcription

1 Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio Maryellen H. Orsinelli, RN, RDCS, FASE Lead Cardiac Sonographer The Richard M. Ross Heart Hospital The Ohio State University Wexner Medical Center Columbus, Ohio DISCLOSURES NONE 2 1
2 CURRENT GUIDELINES FOR THE EVALUATION and MANAGEMENT OF VALVE DISEASE ADDRESS EACH VALVE LESION IN ISOLATION LITTLE DATA and LIMITED GUIDELINES ON THE ASSESSMENT OF MIXED OR MULTIVALVE DISEASE NO GUIDELINES ON MULTIVALVE DISEASE MANAGEMENT OFTEN DIFFICULT TO QUANTITATE LESION SEVERITY IN MULTI-VALVE DISEASE CHALLENGING TO DETERMINE WHICH LESION IS RESPONSIBLE FOR SYMPTOMS 3 CHALLENGES IN EVALUATING TWO CASES OF AORTIC STENOSIS WITH MITRAL VALVE DISEASE HOW DOES THE PRESENCE OF MITRAL VALVE DISEASE AFFECT THE ASSESSMENT OF AORTIC STENOSIS? DOES THE PRESENCE OF AORTIC STENOSIS AFFECT THE EVALUATION OF MITRAL REGURGITATION? PATIENT 1 IS IN ATRIAL FIBRILLATION 4 2




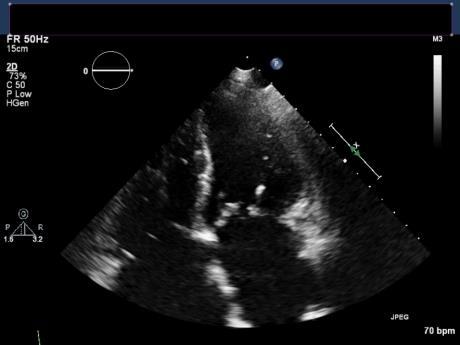
3 CASE 1 86 Y/O WOMAN WITH A PRIOR HISTORY OF AORTIC STENOSIS AND CAD, s/p CABG AND AVR WITH A BIOPROSTHETIC VALVE 11YRS PTA HISTORY OF HTN, CKD3 AND DM FAIRLY ACTIVE AND INDEPENDENT BUT HAS HAD PROGRESSIVE MODEST DOE PRESENTS WITH ABRUPT SUBACUTE WORSENING OF HER CHRONIC DYSPNEA OVER A 2 WEEK PERIOD ON EXAM, THERE IS A 3/6 SEM, NO AR AND A BLOWING 3/6 APICAL HOLOSYTOLIC MURMUR TTE PERFORMED ON ADMISSION 5 CASE 1 ECHO DATA 6 3







4 CASE 1 ECHO DATA 7 CASE 1 QUANTITATIVE ECHO DATA Vm 4.7 M/s MEAN GRADIENT 38 MM Hg 8 4

5 CASE 1 HEMODYNAMIC SUMMARY PATIENT IS IN AFIB NORMAL EF BIOPROSTHETIC AV Vm 4.7 M/s MEAN GRADIENT 38 MM Hg AVA 0.4 CM 2 DI 0.21 ACCELERATION TIME 113 ms MITRAL VALVE VC 0.98 cm PISA ERO 0.49 CM 2 REGURGITANT VOLUME 63 cc 9 ASSESSING PROSTHETIC AV DYSFUNCTION OUR PATIENT Zoghbi et al. JASE Sept


6 PRIMARY MR EVALUATION OUR PATIENT 11 Nishimura et al. ACC / AHA Valve Guidelines 2014 ECHO / DOPPLER PARAMETERS FOR ASSESSING MR Zoghbi et al JASE 2003:16:
7 QUALITATIVE / QUANTITATIVE PARAMETERS FOR THE ASSESSMENT OF MR Zoghbi et al JASE 2003:16: CASE 2 74 Y/O WOMAN WITH A HISTORY OF RHEUMATIC FEVER, s/p OPEN MV COMMISSUROTOMY 25 YEARS AGO PRESENTS WITH PROGRESSIVE DOE AND FATIGUE OTHERWISE HEALTHY WITH WELL CONTROLLED HTN AND DM TTE REVEALS AORTIC STENOSIS AND MITRAL STENOSIS, OUTSIDE SURGEON QUOTED A 20% PERI-OPERATIVE MORTALITY RISK SHE PRESENTS FOR A SECOND OPINION re OTHER POTENTIAL OPTIONS OUTSIDE TTE REVIEWED 14 7





8 CASE 2 ECHO EVALUATION 15 CASE 2 QUANTITATIVE ECHO EVALUATION 16 8
 17 GRADING NATIVE VALVE AORTIC STENOSIS Stage D3 AS o AVA < 1.")
9 CASE 2 HEMODYNAMIC SUMMARY (TTE DATA) MV DATA MEAN GRADIENT 12 MM Hg MVA (PHT 200 ms) 1.1 CM 2 MILD MR AV DATA MILD AR MEAN GRADIENT 24 MM Hg AVA 0.72 CM 2 SVI 21 cc /M 2 TV DATA 3+ TR MEAN GRADIENT 10 MM Hg PHT 177 ms (TVA 1.1 CM 2 ) 17 GRADING NATIVE VALVE AORTIC STENOSIS Stage D3 AS o AVA < 1.0 cm 2 o Mean gradient < 40 mm Hg o SVI < 35 cc/ m 2 18 Nishimura et al. ACC / AHA Valve Guidelines
 SIGNIFICANT AR CAN RESULT IN UNDERESTIMATING MS SEVERITY BY PHT (shortened) DOES THE PRESENCE OF AORTIC STENOSIS AFFECT THE EVALUATION OF")
10 ASSESSING MITRAL STENOSIS Nishimura et al. ACC / AHA Valve Guidelines CHALLENGES IN EVALUATING HOW DOES THE PRESENCE OF MV DISEASE AFFECT THE ASSESSMENT OF AORTIC STENOSIS? SIGNIFICANT MS or MR MAY RESULT IN LOW SV (LOW GRADIENT AS) SIGNIFICANT AR CAN RESULT IN UNDERESTIMATING MS SEVERITY BY PHT (shortened) DOES THE PRESENCE OF AORTIC STENOSIS AFFECT THE EVALUATION OF MITRAL REGURGITATION? MAY INCREASE JET AREA (increased driving pressure) MR V m will be significantly higher than predicted by SBP CONCOMMITANT AR CONFOUNDS RV / RF ASSESSMENT BY SPECTRAL DOPPLER PATIENT 1 IS IN ATRIAL FIBRILLATION NEED TO OBTAIN HEMODYNAMIC DATA WITH MULTIPLE CONSECTIVE BEATS AND AVERAGE 10




11 CHALLENGES IN MANAGING MULTIVALVULAR HEART DISEASE BOTH CASES HAVE AORTIC STENOSIS AND MITRAL DISEASE ARE THE SYMPTOMS DUE TO THE AS? TAVR ARE THE SYMPTOMS DUE TO THE MV DISEASE? MITRACLIP or BMV ARE BOTH LESIONS RESPONSIBLE? MANAGEMENT OPTIONS: TAVR AND MV (CLIP or BMV) STAGED OR SIMULTANEOUS SURGICAL AVR / MVR 21 CASE 1 TEE DATA 22 11
 TEE DATA SEVERE MR DUE")
 2 *38.5 = 0.")




12 CASE 1 (PROSTHETIC AS and MR) TEE DATA SEVERE MR DUE TO A FLAIL A 2 PISA ERO = 2π (1.1) 2 *38.5 = 0.56 CM ERO PROBABLY OVERESTIMATED SEVERE PROSTHETIC AS DUE TO LEAFLET CALCIFICATION 23 CASE 1 MANAGEMENT VIV TAVR AND / OR MITRACLIP STAGED? SIMULTANEOUS? OPTED TO DO MITRACLIP CHALLENGING ANATOMY 2 CLIPS DEPLOYED MR DECREASED TO








13 CASE 1 MANAGEMENT BASELINE V WAVE 15 SBP 100 POST CLIP 2 MR IMPROVED, EXTUBATED AND DISCHARGED READMITTED WITH CHF 2 WEEKS LATER AND VIV TAVR PERFORMED 25 CASE 1 3 MONTHS POST PRESENTATION o o MITRAL VALVE o MEAN GRADIENT 6 mm HG o 1-2+ MR AORTIC VALVE o MEAN GRADIENT 11 mm Hg o AVA 0.8 CM 2 o DI 0.28 o SVI 21 cc/m



 AVA 0.")
14 CASE 2 (RHEUMATIC AS AND MS) TEE EVALUATION 27 CASE 2 HEMODYNAMIC SUMMARY WILKINS SCORE (MOSTLY DUE TO SUBMITRAL DISEASE AND LEAFLET IMMOBILITY) MILD MR MVA BY PLANIMETRY 1.0 CM 2 SEVERE AS LOW FLOW, LOW GRADIENT (SVI 21 cc/m 2 ) AVA 0.8 CM 2 (PLANIMETRY) AVA 0.72 CM 2 (TTE VTI) 28 14
15 CASE 2 MANAGEMENT PATIENT CONCERNED RE HIGH SURGICAL RISK QUOTED BY OSH? BMV +/ - TAVR? TAVR +/- BMV BASED ON TTE AND TEE NOT FELT TO BE AN OPTIMAL BMV CANDIDATE PRIOR COMMISSUROTOMY HIGH WILKINS SCORE (11) TV DISEASE AVR / MVR WITH BIOPROSTHETIC VALVES AND TVR DID WELL, D/C POD 8 29 THANK YOU 30 15



16 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU 52 y/o WOMAN WITH A HISTORY OF POLYSUBSTANCE ABUSE, INCLUDING IV OPIATES and COCAINE PRESENTED 4 MONTHS PTA WITH FEVERS, RIGORS AND DYSPNEA ECHO REVEALED AV VEGETATIONS AND AR BLOOD CULTURES POSITIVE FOR ENTEROCOCCUS TRANS TO OSU FOR MANAGEMENT TEE (SEVERE AR, LEAFLET PERFORATION R / L CUSPS), VEGETATIONS ON AV AND MV EPIDURAL ABSCESS / SPINAL OSTEO 31 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU PRESENTING TEE 32 16

17 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU INITIAL MANAGEMENT ONCE BC WERE STERILE, TO OR TRILEAFLET AV WITH PERFORATION OF R/L CUSPS, SMALL MV VEGETATION, NO ABSCESS AVR WITH A 21 mm ST JUDE TRIFECTA BIOPROSTHETIC VALVE AND DEBRIDEMENT / PATCHING OF ANT MV LEAFLET 33 DISCHARGED TO AN ECF 2 WEEKS POST OP TO COMPLETE A 6 WEEK COURSE OF ANTIBIOTICS LEFT LTACH AMA AFTER 10 DAYS, READMITTED 3 DAYS LATER WITH FEVERS / CP TTE / BC NEGATIVE D/C HOME TO COMPLETE ABX / AGREED TO DRUG TESTING (REFUSED ECF) COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU REPRESENTATION KEPT NO F/U APPTS or DRUG SCREENS / PULLED PICC LINE REPRESENTED 3 MONTHS LATER WITH FATIGUE, FEVERS AND CHILLS, SEPSIS, AKI BC POSTIVE FOR MSSA TOXICOLOGY SCREEN POSITIVE FOR OPIATES AND COCAINE TEE PERFORMED 34 17


 / SOCIAL / MEDICAL ISSUES REOPERATE?")

18 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU TEE AT REPRESENTATION 35 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU MANAGEMENT DECISIONS SEEN BY ORIGINAL SURGEON WHO DECLINED SURGICAL INTERVENTION DUE TO RISK OF REINFECTION AND CONTINUED SUBSTANCE ABUSE BC CLEAR BUT REMAINED FEBRILE NEURO IMAGING WITH NO PROGRESSION OF SPINE LESIONS ECG WITH 1 ST DEGREE AVB SECOND SURGEON ALSO DECLINED TO OFFER REDO AVR WHAT ARE THE CHALLENGES / OPTIONS FOR MANAGEMENT? SURGICAL (TECHNICAL) / SOCIAL / MEDICAL ISSUES REOPERATE? MANAGEMENT POST OP (PAIN, PLACEMENT, COMPLIANCE) IV ANTIBIOTICS FOLLOWED BY CHRONIC SUPPRESSIVE THERAPY? HOSPICE? TREATEMENT OF UNDERLYING DISEASE (ADDICTION) HOW WOULD YOUR INSTITUTION HANDLE SUCH A CASE? 36 18
 37 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU MANAGEMENT PATIENT REQUESTED A SECOND OPINION AT ANOTHER TERTIARY CARE")
19 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU OPIOD ADDICTION INCREASINGLY COMMON PROBLEM COMPLICATES MANAGEMENT HIGH RISK OF RECURRENCE INFECTION DRUG USE CHALLENGES WITH POST OP PAIN MANAGEMENT PLACEMENT ISSUES NEED TO TREAT UNDERLYING ILLNESS (SUBSTANCE ABUSE / ADDICTION) 37 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU MANAGEMENT PATIENT REQUESTED A SECOND OPINION AT ANOTHER TERTIARY CARE CENTER ARRANGEMENTS MADE TO TRANSFER, PLACED ON WAITING LIST PENDING BED REMAINED FEBRILE BUT HEMODYNAMICALLY STABLE NEW AR MURMUR APPRECIATED LIMITED TTE REVEALS PROGRESSION OF INFECTION, TV VEGETATION AND SEVERE AR 38 19





20 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU 39 COMPLEX VALVE DISEASE ENDOCARDITIS IN IVDU OUTCOME BED AVAILABLE DAY AFTER TTE AND SHE WAS TRANSFERRED EVALUATED BY SURGICAL TEAM AT SECOND HOSPITAL AND SURGERY DECLINED DUE TO CONTINUED IVDU AND PROGRESSION OF INFECTION EXPIRED 5 DAYS AFTER TRANSFER 40 20
21 THANK YOU 41 21
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Culprit vs Multivalve Transcatheter Intervention
 Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018
 1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal
1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
DISCLOSURE. Mitral ViV: why? Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? UW Medicine NONE.
 Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification. Rheumatic Mitral Stenosis 76yo male
 MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Cases of Abnormal Prosthetic Valves
 Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Mitral Valve Stenosis: What do I need to know? ACC Latin American Conference 2017
 Mitral Valve Stenosis: What do I need to know? ACC Latin American Conference 2017 Athena Poppas, MD FACC FASE Past ACC Scientific Sessions Chair, ACC Board of Trustee Professor of Medicine, Brown University
Mitral Valve Stenosis: What do I need to know? ACC Latin American Conference 2017 Athena Poppas, MD FACC FASE Past ACC Scientific Sessions Chair, ACC Board of Trustee Professor of Medicine, Brown University
Quantitation of Aortic Regurgitation ASCeXAM / ReASCE Review Course
 Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
Percutaneous Therapy for Calcific Mitral Valve Disease
 31 st Annual State of the Art Echocardiography San Diego, CA February 18, 2018 5:00 5:15 PM 15 min Percutaneous Therapy for Calcific Mitral Valve Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive
31 st Annual State of the Art Echocardiography San Diego, CA February 18, 2018 5:00 5:15 PM 15 min Percutaneous Therapy for Calcific Mitral Valve Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive
Endocarditis and Its Complications: The Role of Echocardiography
 Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
 Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Objectives. Considerations in management of multivalvular disease. Case Discussions. A Systematic Approach to Multivalve Disease.
 A Systematic Approach to Multivalve Disease James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
A Systematic Approach to Multivalve Disease James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
What to do with a Patient with Recurrent MR after Intervention
 What to do with a Patient with Recurrent MR after Intervention James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School
What to do with a Patient with Recurrent MR after Intervention James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
Michigan Society of Echocardiography 30 th Year Jubilee
 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Management of TR in Patients Undergoing Mitral Interventions
 Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors
 Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle
 Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
CASES IN ADVANCED IMAGING
 CASES IN ADVANCED IMAGING DAVID A. ORSINELLI, MD PROFESSOR, CLINICAL INTERNAL MEDICINE THE OHIO STATE UNIVERSITY DIVISION OF CARDIOVASCULAR MEDICINE OHIO ACC ANNUAL CONFERENCE OCTOBER 2010 WHICH IMAGING
CASES IN ADVANCED IMAGING DAVID A. ORSINELLI, MD PROFESSOR, CLINICAL INTERNAL MEDICINE THE OHIO STATE UNIVERSITY DIVISION OF CARDIOVASCULAR MEDICINE OHIO ACC ANNUAL CONFERENCE OCTOBER 2010 WHICH IMAGING
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
DISCLOSURE. Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Clinical Value of 3D Echo: Volumes and Valves
 Clinical Value of 3D Echo: Volumes and Valves James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Conflicts: None 3D2011:1
Clinical Value of 3D Echo: Volumes and Valves James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Conflicts: None 3D2011:1
Echocardiographic Evaluation of Mitral Valve Prostheses
 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis
 TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
*Core lab for numerous trials, for which I receive no direct compensation from sponsors.
 Rebecca T. Hahn, MD, FACC, FASE Director of Interventional Echo Professor of Medicine Columbia University Company Abbott Vascular Gore&Assoc NaviGATE Medtronic Boston Scientific GE Medical Philips Healthcare
Rebecca T. Hahn, MD, FACC, FASE Director of Interventional Echo Professor of Medicine Columbia University Company Abbott Vascular Gore&Assoc NaviGATE Medtronic Boston Scientific GE Medical Philips Healthcare
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
CARDIOLOGY GRAND ROUNDS
 CARDIOLOGY GRAND ROUNDS Presentation: Speakers: Percutaneous Repair of Paravalvular Prosthetic Regurgitation Paul Sorajja, MD Director of the Center for Valve and Structural Heart Disease Minneapolis Heart
CARDIOLOGY GRAND ROUNDS Presentation: Speakers: Percutaneous Repair of Paravalvular Prosthetic Regurgitation Paul Sorajja, MD Director of the Center for Valve and Structural Heart Disease Minneapolis Heart
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Echocardiography in Endocarditis
 Echocardiography in Endocarditis Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Demographics of IE Incidence is 1.4 12.7/100,000
Echocardiography in Endocarditis Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Demographics of IE Incidence is 1.4 12.7/100,000
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
13/06/2018. Rheumatic Mitral Stenosis: What does the ESC Guideline say? Mitral Stenosis: Echo Assessment. Mitral Stenosis ESC Guidance 2017
 Rheumatic Mitral Stenosis: What does the ESC Guideline say? Mitral Stenosis: Echo Assessment Dave Northridge Edinburgh Heart Centre Rheumatic mitral stenosis Prosthetic mitral dysfunction Calcific/degenerative
Rheumatic Mitral Stenosis: What does the ESC Guideline say? Mitral Stenosis: Echo Assessment Dave Northridge Edinburgh Heart Centre Rheumatic mitral stenosis Prosthetic mitral dysfunction Calcific/degenerative
Imaging MV. Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015
 Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
 Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed?
 What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed? Robert J. Siegel, M.D., FACC Nov. 14-15, 2017, Beverly Hills Director, Cardiac Non-Invasive Laboratory
What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed? Robert J. Siegel, M.D., FACC Nov. 14-15, 2017, Beverly Hills Director, Cardiac Non-Invasive Laboratory
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
ASCeXAM / ReASCE. Practice Board Exam Questions. Monday Afternoon
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Afternoon Aortic Valve Prostheses Aortic Regurgitation Stress Echocardiography Ischemic Heart Disease and Myocardial Infarction 3D Echocardiography
ASCeXAM / ReASCE Practice Board Exam Questions Monday Afternoon Aortic Valve Prostheses Aortic Regurgitation Stress Echocardiography Ischemic Heart Disease and Myocardial Infarction 3D Echocardiography
Update on the prevention, diagnosis and management of Infective Endocarditis (IE)
") Update on the prevention, diagnosis and management of Infective Endocarditis (IE) Dr.Ahmed Yahya Mohammed Alarhabi MD, MsC,FcUSM,FACC,MAHA Consultant Interventional Cardiologist Head of Cardiac Center
Update on the prevention, diagnosis and management of Infective Endocarditis (IE) Dr.Ahmed Yahya Mohammed Alarhabi MD, MsC,FcUSM,FACC,MAHA Consultant Interventional Cardiologist Head of Cardiac Center
Case Studies in Complex Endocarditis
 Case Studies in Complex Endocarditis Vera H. Rigolin, MD Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern Memorial Hospital
Case Studies in Complex Endocarditis Vera H. Rigolin, MD Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern Memorial Hospital
Valve Disease Board Review Questions
 Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient
 Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR)
") Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR) Kathleen Harper DO FACC FACP 87 Chief, Cardiology Section VA Maine Healthcare Kathleen.Harper@va.gov Prevalence of Aortic Stenosis
Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR) Kathleen Harper DO FACC FACP 87 Chief, Cardiology Section VA Maine Healthcare Kathleen.Harper@va.gov Prevalence of Aortic Stenosis
2/4/2019. Nursing Perspective of TAVR. Disclosure. Learning Outcomes
 Nursing Perspective of TAVR Tara Whitmire, DNP, APRN-NP, NP-C, CHFN Nebraska Methodist Hospital Cardiothoracic Surgery Nurse Practitioner Danelle Homeyer, RN Methodist Physicians Clinic Director, Structural
Nursing Perspective of TAVR Tara Whitmire, DNP, APRN-NP, NP-C, CHFN Nebraska Methodist Hospital Cardiothoracic Surgery Nurse Practitioner Danelle Homeyer, RN Methodist Physicians Clinic Director, Structural
The V Wave. January, 2007 Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH. Ref: Kern MJ. Hemodynamic Rounds, 2 nd ed
 The V Wave January, 2007 Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH Ref: Kern MJ. Hemodynamic Rounds, 2 nd ed. 1999. Normal Hemodynamic Values Cardiac index 2.8-4.2 (mean 3.4 L/min/m 2 ) Stroke volume 30-65
The V Wave January, 2007 Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH Ref: Kern MJ. Hemodynamic Rounds, 2 nd ed. 1999. Normal Hemodynamic Values Cardiac index 2.8-4.2 (mean 3.4 L/min/m 2 ) Stroke volume 30-65
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management
 Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Cardiac Valve/Structural Therapies
 Property of Dr. Chad Rammohan Cardiac Valve/Structural Therapies Chad Rammohan, MD FACC Medical Director, El Camino Hospital Cardiac Catheterization Lab Director, Interventional and Structural Cardiology,
Property of Dr. Chad Rammohan Cardiac Valve/Structural Therapies Chad Rammohan, MD FACC Medical Director, El Camino Hospital Cardiac Catheterization Lab Director, Interventional and Structural Cardiology,
imagine 2018 Echocardiography Today - Do, Learn, Do More, Learn More November 3-4, 2018 Georgia Technology Hotel and Conference Center
 Piedmont Heart presents imagine 2018 Echocardiography Today - Do, Learn, Do More, Learn More November 3-4, 2018 Georgia Technology Hotel and Conference Center Program Co-Directors Mani A. Vannan MBBS FASE
Piedmont Heart presents imagine 2018 Echocardiography Today - Do, Learn, Do More, Learn More November 3-4, 2018 Georgia Technology Hotel and Conference Center Program Co-Directors Mani A. Vannan MBBS FASE
Subacute left ventricular outflow tract obstruction after transapical closure of a mitral paravalvular leak in the region of the aortomitral curtain
 DOI: 10.1111/echo.13357 CASE REPORT Subacute left ventricular outflow tract obstruction after transapical closure of a mitral paravalvular leak in the region of the aortomitral curtain Sathish Chikkabyrappa
DOI: 10.1111/echo.13357 CASE REPORT Subacute left ventricular outflow tract obstruction after transapical closure of a mitral paravalvular leak in the region of the aortomitral curtain Sathish Chikkabyrappa
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kang D-H, Kim Y-J, Kim S-H, et al. Early surgery versus conventional
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kang D-H, Kim Y-J, Kim S-H, et al. Early surgery versus conventional
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE. Sampling Rate M-Mode: 1800 / sec 2D: 30 / sec
 M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
Back to Basics: Common Errors In Quantitation In Everyday Practice
 Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
TEE Zebras. Case Cardiac Anesthesia Group
 TEE Zebras Edwin G. Avery, IV, M.D., C.P.I. Chief, Division of Cardiac Anesthesia University Hospitals Case Medical Center Associate Professor of Anesthesiology Case Western Reserve University School of
TEE Zebras Edwin G. Avery, IV, M.D., C.P.I. Chief, Division of Cardiac Anesthesia University Hospitals Case Medical Center Associate Professor of Anesthesiology Case Western Reserve University School of
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY
 OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients?
 Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients? David H. Adams, MD Cardiac Surgeon-in-Chief Mount Sinai Health System Marie Josée and Henry R. Kravis Professor and
Really Less-Invasive Trans-apical Beating Heart Mitral Valve Repair: Which Patients? David H. Adams, MD Cardiac Surgeon-in-Chief Mount Sinai Health System Marie Josée and Henry R. Kravis Professor and