Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
|
|
|
- Kathlyn Gordon
- 6 years ago
- Views:
Transcription

1 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
2 Exercise echocardiography Dobutamine echocardiography

3 Usefulness of exercise echo in VHD (Lancellotti P, EHJ CVI 2016;17:1191) 76 yo male At 33 yo, abnormal ECG pointed At 63 yo, exertional dyspnea occurred Diagnosed as idiopathic DCM by cath and myocardial biopsy and B-blocker started Repeated admissions due to HF symptoms EF 19%, +1-2 Mr, +1Tr, TRPG 16 mmhg What is the cause of HF symptoms?





 Secondary MR Increase in MR")
4 pre 15W 30W 45W dyspnea SPAP 15 mmhg 35 mmhg 40 mmhg 66 mmhg BP 100/56 116/68 128/70 154/76 HR Ex-induced PH and increase in MR may be causes of HF symptoms. Indications of intervention for MR Appearance of symptoms in asymptomatic patient Primary MR Poor prognosticators Dynamic PH (SPAP Limited CR (<5% increase in EF, <2% increase in GLS) Limited RVCR (TAPSE <19 mm) Secondary MR Increase in MR (increase in ERO 2 ) Dynamic
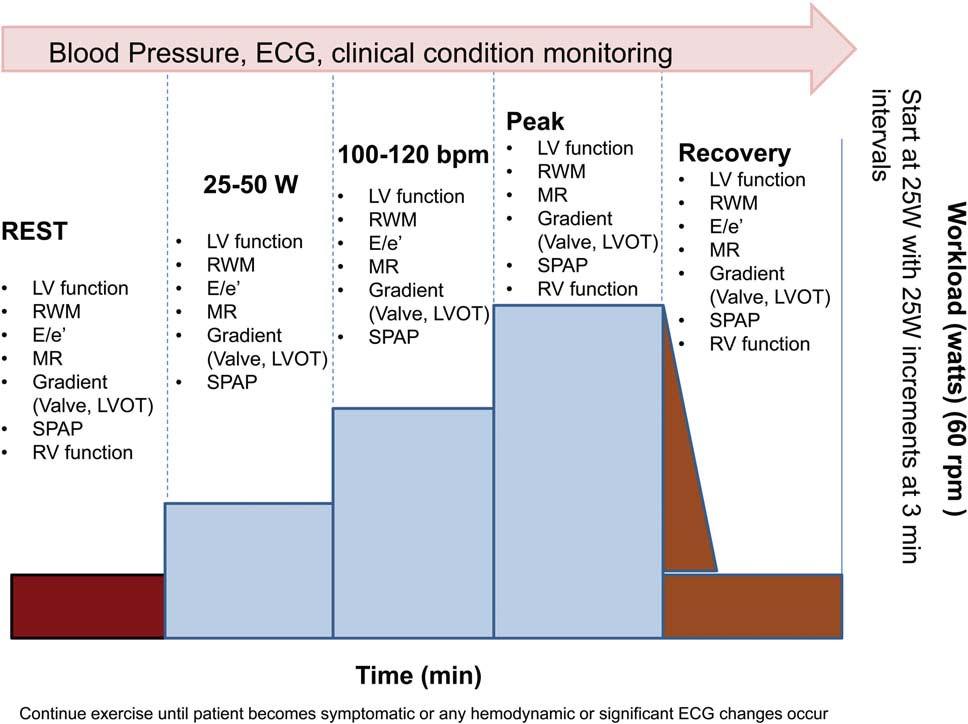
5 Indications of intervention for MS Exercise stress echo mpg >15 mmhg on exertion SPAP >60 mmhg on exertion Dobutamine stress echo (if the patient cannot exercise) mpg >18 mmhg 62 yo female At 58 yo, diastolic heart murmur pointed Diagnosed as MS (MVA = 1.6 cm 2 ) At 60 yo, exertional dyspnea occurred MVA = 1.6 cm 2 (planimetry), 1.4 cm 2 (PHT), cm 2 (continuity equation) mpg = 6 7 mmhg TRPG = 19 mmhg







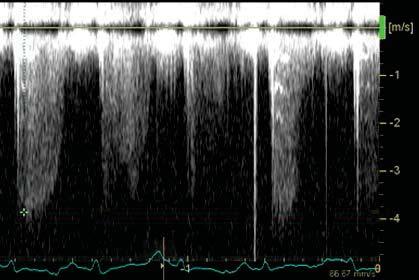
6 Echo at rest pre 25W 50W 75W mpg 6 mmhg 13 mmhg 21 mmhg 20 mmhg TRPG 24 mmhg 53 mmhg 59 mmhg 60 mmhg Surgery was recommended.
7 Indications of intervention for AR Appearance of symptoms in asymptomatic patient Limited CR (<5% increase in EF) ) Dynamic MR However, there is limited evidence. Indications of stress echo in AS Asymptomatic severe AS Low-flow, low-gradient AS With reduced EF (classical LFLG AS) Pseudo-severe AS True-severe AS With preserved EF (paradoxical AS)
8 Indications of intervention for asymptomatic severe AS Appearance of symptoms Ex-induced hypotension Increase in mpg -20 mmhg) Limited CR (<1.4% increase in GLS*) Induced PH (SPAP >60 mmhg) (*, Donal E, EHJ CVI 2011;12:235) Low-flow, low-gradient AS AVA <1.0 cm 2, mpg <40 mmhg, LVEF <50% True severe AS Severe AS Low SV due to LV systolic dysfunction low PG Pseudo severe AS Moderate AS Low SV due to LV systolic dysfunction cannot open AV small AVA and low PG Paradoxical low-flow, low-gradient AS EF >50% but low SV (SVi <35 ml/m 2 ) DSE
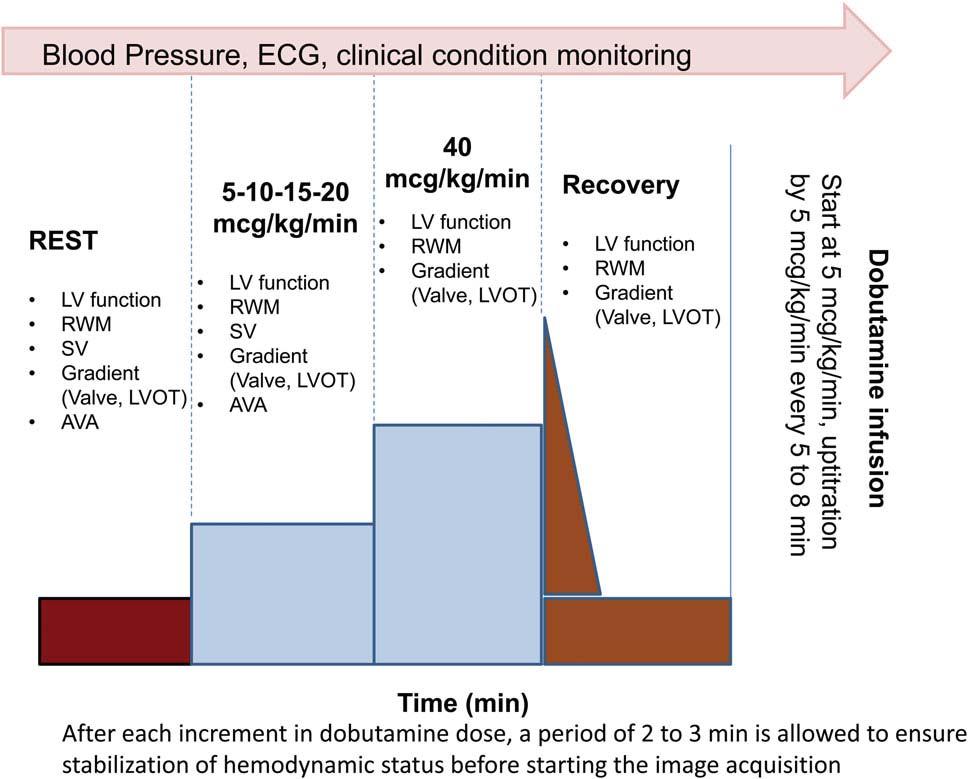
9 Dobutamine stress echo in AS Start from 5 /kg/min Increase DOB by 5 /kg/min every 5 min until 20 /kg/min % increase in SV 20% contractile reserve (+) mpg 2 severe AS mpg < 2 moderate AS % increase in SV <20% contractile reserve (-) Severe calcification severe AS Mild calcification moderate AS CT score is helpful. CT score>1650 u, JACC2012;60: yo male Prior MI, chronic HF, post CRT-D implantation LVEDD = 72 mm, LVESD = 66 mm, EF = 25% AVA = 0.68 cm 2, mpg = 28 mmhg, SVi = 29 ml/m 2 Mild MR, mild AR Pseudo-severe AS or true-severe AS?

 150 202 199 242")

 AVA at peak DSE = 0.94 <1.")
10 Echo at rest Dobutamine stress echo Pre 5 g/kg/min 10 g/kg/min 20 g/kg/min SV (ml) ET (ms) Flow rate (ml/s) mpg (mmhg) AVA (cm2) SV = (63 45) / 45 = 40% >20% Flow reserve (+) AVA at peak DSE = 0.94 <1.0 cm 2 True-severe AS TAVI was performed.



11 After TAVI AVA: from 0.68 to 1.17 cm 2 LVEDD: from 72 to 65 mm, LVESD: from 66 to 57 mm, EF: from 25 to 31% NYHA class: from III to I 70 yo female (A case when I was young ) History of present illness Exertional dyspnea starting 9 yrs ago. Diagnosed as HHD at 8 yrs ago by cath and biopsy. Repeated admission due to CHF. Had nocturnal dyspnea recently. Past medical history Hypertension since 50 y/o, DM, hyperlipidemia PCI to mid LAD in 5 yrs ago with residual stenosis at Dx br ECG Atrial fibrillation with wide QRS complex (CLBBB)

 25 25 34 36 TVI (cm) 50 47 54 44 TVI x HR 4200 3995 6372")
12 70 yo female with LV dysfunction EF = 17% AV PG = 30 mmhg AVA = 0.73 cm 2 Low dose DSE Rest 5 g/kg/min 10 g/kg/min 20 g/kg/min HR BP 102/54 95/66 101/55 90/49 AVA (cm 2 ) Peak PG (mmhg) TVI (cm) TVI x HR No LV flow reserve!


13 Intraoperative finding No calcification, pliable cusps! TTE TEE is important. If no CR, you cannot determine the severity. Look at the valve closely or use CT. Assess the grade of calcification and pliability of cusps.
 with AVR. However, limited CR does not predict absence of LV function improvement after AVR.")
14 Limited CR (flow reserve) Limited CR is due to: Afterload mismatch Associated CAD Myocardial damage due to prior MI or myocardial fibrosis Limited CR is seen in 1/3 of patients and is associated with high operative mortality (6 33%) with AVR. However, limited CR does not predict absence of LV function improvement after AVR. Projected AVA (AVA at flow rate of 250 ml/s) should be calculated to differentiate pseudo-severe AS and true-severe AVA proj = Projected AVA AVA Q x (250 Q rest ) + AVA rest (Q = SV / LVET) AVA proj = AVA at normal flow rate (250 ml/s), AVA rest = AVA at rest, AVA = absolute changes in AVA during DSE, Q rest = mean transvalvular flow rate at rest, Q = absolute changes in mean transvalvular flow rate during DSE. Projected AVA AVA proj = 1.02 cm 2 AVA (cm 2 ) Concerns: Slope determination from only 4 points. Accuracy of Q (esp. ET) Are you confident with this measurement? (Blais C, Circulation 2006;113:711)

15 Simplified projected AVA AVA proj = AVA peak AVA rest Q peak -Q rest x (250 Q rest ) + AVA rest (Q = SV / LVET) AVA proj = AVA at normal flow rate (250 ml/s), AVA rest = AVA at rest, AVA peak = AVA at peak, Q rest = mean transvalvular flow rate at rest, Q peak = mean transvalvular flow rate at peak Calculation of projected AVA and simplified projected AVA should be carefully performed. Concerns: Slope determination from only 2 points. Accuracy of Q (esp. ET) (Clavel MA, JASE 2010;23:380)
16 Indications of stress echo in VHD Identify patients in need of intervention Severe VHD without symptoms Truly asymptomatic or not? Non-severe VHD with symptoms Stress echo Hemodynamic disturbances or not? (Ex-induced hypotension, arrhythmia, PH) Intervention VHD with low flow Truly severe or not?
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment
 Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes
 Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Workshop Facing the challenge of TAVI 2016
 Workshop Facing the challenge of TAVI 2016 Congrès annuel de la SSC Lausanne 15 Juin 2016 Pitfalls in the severity assessment of aortic stenosis by echocardiography Hajo Müller, unité d échocardiographie,
Workshop Facing the challenge of TAVI 2016 Congrès annuel de la SSC Lausanne 15 Juin 2016 Pitfalls in the severity assessment of aortic stenosis by echocardiography Hajo Müller, unité d échocardiographie,
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece
 A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
The best in heart valve disease Aortic valve stenosis
 The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
CASES IN ADVANCED IMAGING
 CASES IN ADVANCED IMAGING DAVID A. ORSINELLI, MD PROFESSOR, CLINICAL INTERNAL MEDICINE THE OHIO STATE UNIVERSITY DIVISION OF CARDIOVASCULAR MEDICINE OHIO ACC ANNUAL CONFERENCE OCTOBER 2010 WHICH IMAGING
CASES IN ADVANCED IMAGING DAVID A. ORSINELLI, MD PROFESSOR, CLINICAL INTERNAL MEDICINE THE OHIO STATE UNIVERSITY DIVISION OF CARDIOVASCULAR MEDICINE OHIO ACC ANNUAL CONFERENCE OCTOBER 2010 WHICH IMAGING
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Michigan Society of Echocardiography 30 th Year Jubilee
 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Blank DISCLOSURES 1/17/2017 COMPLEX VALVE CASES CHALLENGES IN EVALUATING AND MANAGING MULTIVALVULAR HEART DISEASE ECHO HAWAII 1/23/17 NONE
 Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Exercise PHT in valvular heart disease. Julien Magne CHU Limoges, France
 Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Imaging and heart failure
 Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ;
 Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
ESC / EACTS new valvular guidelines- Update
 ESC / EACTS new valvular guidelines- Update Yaron Shapira, MD The Dan Sheingarten echocardiography & valve clinic Rabin Medical Center, Beilinson Hospital, Petah-Tiqva Tel-Aviv University ESC valve guidelines
ESC / EACTS new valvular guidelines- Update Yaron Shapira, MD The Dan Sheingarten echocardiography & valve clinic Rabin Medical Center, Beilinson Hospital, Petah-Tiqva Tel-Aviv University ESC valve guidelines
Aortic stenosis with concomitant mitral regurgitation
 Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Cases in Stress Echo DISCLOSURE
 Cases in Stress Echo Susan Wilansky, MD, FRCP(C), FACC, FASE Mayo Clinic, AZ DISCLOSURE Relevant Financial Relationship(s) None Off Label Usage None 1 Exercise Testing in Patients with HCM (Class IIa)
Cases in Stress Echo Susan Wilansky, MD, FRCP(C), FACC, FASE Mayo Clinic, AZ DISCLOSURE Relevant Financial Relationship(s) None Off Label Usage None 1 Exercise Testing in Patients with HCM (Class IIa)
Athlete s Heart: Clinical Relevance. Athlete's Heart vs. Cardiac Pathology Clinical Approaches. Echo Florida Conflicts of Interest: None
 Athlete's Heart vs. Cardiac Pathology Clinical Approaches Echo Florida 2012 Aaron L. Baggish MD Cardiovascular Performance Program Cardiac Ultrasound Laboratory Division of Cardiology Massachusetts General
Athlete's Heart vs. Cardiac Pathology Clinical Approaches Echo Florida 2012 Aaron L. Baggish MD Cardiovascular Performance Program Cardiac Ultrasound Laboratory Division of Cardiology Massachusetts General
Imaging in dilated cardiomyopathy : factors associated with a poor outcome
 Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
Advanced Evaluation of Left Ventricular Function in Degenerative MR. Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium
 Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
Diastolic Function Assessment New Guideline Update Practical Approach
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Strain Imaging: Myocardial Mechanics Simplified and Applied
 9/28/217 Strain Imaging: Myocardial Mechanics Simplified and Applied John Gorcsan III, MD Professor of Medicine Director of Clinical Research Division of Cardiology VECTORS OF CONTRACTION Shortening Thickening
9/28/217 Strain Imaging: Myocardial Mechanics Simplified and Applied John Gorcsan III, MD Professor of Medicine Director of Clinical Research Division of Cardiology VECTORS OF CONTRACTION Shortening Thickening
Clinical Outcome in Patients with Aortic Stenosis
 Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
History of Stress Testing. Disclosure. Overview. Stress Echocardiography New Applications. and Comparison with Other Stress.
 Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
New Imaging for Aortic Valve Disease. Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego
 New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
Low gradient severe aortic stenosis with preserved left ventricular ejection fraction
 Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Aortic valve Stenosis: Insights in the evaluation of LV function. Erwan DONAL Cardiologie CHU Rennes
 Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None
, FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None") Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 2,000 Noninvasive Procedures 1,600 Units of Service/ 1,000 Beneficiaries 1,200 800 Evaluation and
Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 2,000 Noninvasive Procedures 1,600 Units of Service/ 1,000 Beneficiaries 1,200 800 Evaluation and
New imaging modalities for assessment of TAVI procedure and results. R Dulgheru, MD Heart Valve Clinic CHU, Liege
 New imaging modalities for assessment of TAVI procedure and results R Dulgheru, MD Heart Valve Clinic CHU, Liege Disclosure of Interest I, Raluca Dulgheru, DO NOT HAVE a financial interest/arrangement
New imaging modalities for assessment of TAVI procedure and results R Dulgheru, MD Heart Valve Clinic CHU, Liege Disclosure of Interest I, Raluca Dulgheru, DO NOT HAVE a financial interest/arrangement
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Constriction vs Restriction Case-based Discussion
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Constriction vs Restriction Case-based Discussion Jae K. Oh, MD Samsung Professor
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Constriction vs Restriction Case-based Discussion Jae K. Oh, MD Samsung Professor
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Echo evaluation for TAVR. From the General Cardiologist to the Interventional Echocardiologist
 Echo evaluation for TAVR From the General Cardiologist to the Interventional Echocardiologist Disclosures Proctoring activities for Abbott Vascular I and the HYGEIA Hospital «Heart Team» have received
Echo evaluation for TAVR From the General Cardiologist to the Interventional Echocardiologist Disclosures Proctoring activities for Abbott Vascular I and the HYGEIA Hospital «Heart Team» have received
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Stress Echocardiography in VHD: is myocardial contrac8on a reliable marker for ischemia?
 Stress Echocardiography in VHD: is myocardial contrac8on a reliable marker for ischemia? Rosa Sicari CNR, Ins8tute of Clinical Physiology, Pisa, Italy Milano 8 maggio 2012 Stress Echo and Cardiac death
Stress Echocardiography in VHD: is myocardial contrac8on a reliable marker for ischemia? Rosa Sicari CNR, Ins8tute of Clinical Physiology, Pisa, Italy Milano 8 maggio 2012 Stress Echo and Cardiac death
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이
 Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
HIGHLIGHT SESSION. Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips
 Disclosures: Speaker Philips") Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Cardiac Care Network of Ontario
 Cardiac Care Network of Ontario Cardiac Wait Times Patient Triage Business Rules December 2016 TABLE OF CONTENTS 1. Introduction... 3 1.1. Document Purpose... 3 1.2. Document Structure... 3 2. Algorithms...
Cardiac Care Network of Ontario Cardiac Wait Times Patient Triage Business Rules December 2016 TABLE OF CONTENTS 1. Introduction... 3 1.1. Document Purpose... 3 1.2. Document Structure... 3 2. Algorithms...
The correlation of AVA measured by transthoracic, transesophageal echocardiography and cardiac CT
 The correlation of AVA measured by transthoracic, transesophageal echocardiography and cardiac CT R.Petr, H.Linkova, J.Knot, E.Paskova, J.Daniel, M.Labos Cardiocenter of University Hospital Kralovske Vinohrady
The correlation of AVA measured by transthoracic, transesophageal echocardiography and cardiac CT R.Petr, H.Linkova, J.Knot, E.Paskova, J.Daniel, M.Labos Cardiocenter of University Hospital Kralovske Vinohrady
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong
 Pol.Col.Dr.Kasem Ratanasumawong") Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Aortic Stenosis.
 Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD
 Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD Board Review Course 2017 43 year old health assistant Severe resistant HTN LT BSA 2 Height 64 1 Here is the M mode echocardiogram
Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD Board Review Course 2017 43 year old health assistant Severe resistant HTN LT BSA 2 Height 64 1 Here is the M mode echocardiogram
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization
 Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization + K Spargias, MD, PhD THV Director Hygeia Hospital Disclosures - Proctor
Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization + K Spargias, MD, PhD THV Director Hygeia Hospital Disclosures - Proctor
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors
 Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Cardiac Perioperative Risk Assessment American Heart Association Guidelines
 Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
2017 ESC/EACTS Guidelines for the management of valvular heart disease
 2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
1. LV function and remodeling. 2. Contribution of myocardial ischemia due to CAD, and
 1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides
 Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
LA Function analysis Marcia Barbosa Vice Presidente - Brazilian Soc of Cardiology President-elect - Interamerican Soc of Cardiology
 LA Function analysis Marcia Barbosa Vice Presidente - Brazilian Soc of Cardiology President-elect - Interamerican Soc of Cardiology Belo Horizonte Brazil DECLARATION OF CONFLICT OF INTEREST Nothing to
LA Function analysis Marcia Barbosa Vice Presidente - Brazilian Soc of Cardiology President-elect - Interamerican Soc of Cardiology Belo Horizonte Brazil DECLARATION OF CONFLICT OF INTEREST Nothing to
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent