Tumours of the Prostate and Testis update on WHO classification, IHC and molecular Morphology
|
|
|
- Marilynn Crawford
- 5 years ago
- Views:
Transcription


1 Tumours of the Prostate and Testis update on WHO classification, IHC and molecular Morphology Glen Kristiansen Professor and Chairman Institute of Pathology, University Hospital Bonn

2 January 2016

3 WHO GU-Pathology Working Group, Zurich, March 2015

4 Prostate working Group WHO March 2015, Zurich
5 Todays Topics WHO 2016 Prostate Diagnostic Immunohistochemistry in Prostate Prognostic Immunhistochemistry in Prostate Cancer WHO 2016 Testis Diagnostic Immunohistochemistry in Testicular Tumors
6 Histological Entities and Variants of PCa Acinar Atrophic Pseudohyperplastic Microcystic Foamy Mucinous Signet ring cell-like Pleomorphic-giant cell Sarcomatoid Ductal cribriform papillary solid
, GP 1-5 Ductal")

7 The Classics... Acinar (>90%), GP 1-5 Ductal (3-5%), GP 4-5 Note: A ductal tumor component ought to be mentioned and quantified in your report


8 Atrophic Variant Signs of atrophy De novo oder following (anti-androgenic Tx) Usually accompanied by ordinary acinar PCa usually GP 3


9 Pseudohyperplastic Variant CK5/6 Pitfall: do not mix up with BPH or HGPIN GP 3


10 Microcystic Variant Cytic, often with atrophic epithelium In approx. 10% of RP specimens GP 3

 GP 3-4 (ignore mucin,")
11 Mucinous Variant GP3 > 25% extracellular mucin Can only be diagnosed on RP (use term mucinous features in Bx) GP 3-4 (ignore mucin, architecture counts)

 GP 3-4 (ignore mucin,")
12 Mucinous Variant GP4 > 25% extracellular mucin Can only be diagnosed on RP (use term mucinous features in Bx) GP 3-4 (ignore mucin, architecture counts)


13 Pleomorphic Giant Cell Variant Associated acinar PCa Extremely rare Usually associated with conventional high grade PCa Pitfall: can be mixed up with urothelial carcinoma
")
14 Intraductal Ca of the Prostate (IDC-P) M8500/2
")
15 Intraductal Ca of the Prostate (IDC-P) M8500/2

16 The fate of old tubuli entrapped in cancer is twofold. Firstly - and by far most commonly they vanish and obliterate, or secondly, their lumen will be filled by intraalveolarly growing carcinoma.

17 WHO 2016 Definition of IDC-P:
18 Differential Diagnosis of IDC-P Cribriform Hyperplasia HGPIN Ductal Carcinoma Invasive cribriform Pca Urothelial Carcinoma/CIS Colon Cancer

19

20 Ductal Carcinoma

21

22

23 p63/amacr PIN-like ductal adenocarcinoma

24 HGPIN
25 DD HGPIN vs. IDC-P Diagnostic criteria HGPIN IDC-P Basal cells + + Cytologic atypia + +(+) Luminal bridging -/(+) + Solid growth - + Dense cribriform - + Comedonecrosis - + Enlarged nuclei (6x) - -/+ IHC: ERG neg. 50% pos. PTEN pos. 60% negative.
26 Epidemiology of IDC-P Author Year Cohort size Specimen Type Kovi et al RPE 48 % IDC-P McNeal et al RPE 26.5 McNeal et al RPE 29.8 Wilcox et al RPE, pt3n Rubin et al RPE 37.7 Shah et al RPE 17.9 Miyai et al RPE 17.2 Watts et al Bx 2.8
27 Clinical Implications of IDC-P in RPE Presence of IDC-P shows strong associations... with higher Gleason Scores larger tumors positive margins extraprostatic extension (EPE) pn+
28 Clinical Implications of IDC-P in RPE Trudel et al. n=246
29 Should I grade IDC-P? e.g.? Low grade high grade


30 Should I grade IDC-P? e.g.! Low grade high grade Current WHO & ISUP 2014 recommendation: Stick to: HGPIN, ( Borderline Atypical ), IDC-P


31 Intraductal carcinoma of prostate Reproducibility issues Intraductal carcinoma of the prostate: interobserver reproducibility survey of 39 urologic pathologists Annals of Diagnostic Pathology 18: ; 2014 Microphotographs circulated PIN IDCP - Invasive 43% agreement for IDCP
 ISUP(2014)/")
")

32 Gleason Grading of Prostate Cancer Original ISUP (2005) ISUP(2014)/ WHO (2016) Dr. Donald Gleason Pattern (1-5) Gleason score=1 o +2 o International Society of Urological Pathology (ISUP) 2005/2014



33 Grading Cribriform Glands GP 3? GP 4? Is the outer contour decisive?

34 Grading Cribriform Glands GP 3? GP 4?...or inner values?



35 ISUP2014/WHO2016 All cribriform glands are reported as GP 4

36 ISUP2014/WHO2016 All glomeruloid glands are reported as GP4 (beginning of Cribriform growth)
37 Grade groups: Gleason score 2-6 Grade Group 1 Gleason score 3+4=7 Grade Group 2 Gleason score 4+3=7 Grade Group 3 Gleason score 8 Grade Group 4 Gleason score 9-10 Grade Group 5

38 Cumulative Survival Years
39 What is the correct term for these grades? Epstein grade? ISUP grade? WHO grade? ISUP/WHO: Grade Groups! Note: this was meant as a provisional term.

 Gleason")
, Grade Group 3 Gleason Score WHO: 4+5=9,")
40 Problem: Gleason Grading on RPE * * * * Gleason pattern 4 50% Gleason pattern 3 40% Gleason score classic : =7 Gleason pattern 5 10% Gleason score ISUP 2005: 4+3= 7 (5) Gleason Score ISUP 2014:??? (4+3=7 (50% GP4; tert. 5), Grade Group 3 Gleason Score WHO: 4+5=9, Grade Group 5
41 IHC in Prostate Diagnostics


42 Typical diagnostic problem: carcinoma vs. atrophy/reactive changes? HE CK5/6
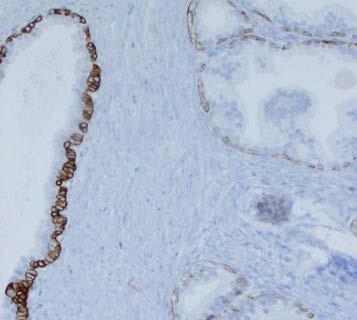

43 Cytokeratins or p63/p40? CK5/6 p63 PZ TZ PZ TZ




44 New tools new pitfalls... p63 p63-positive PCa! Prevalence: 1%.



45 p63 or p40?


46 Positive Markers of Malignancy: AMACR

47 p63/amacr

48 p63/amacr

49 AMACR in benign glands 3 bilder: Hp, pin, HP

50 AMACR in Partial Atrophy

51 Alternatives to AMACR: 1. FASN

52 Alternatives to AMACR: 2. GOLM1


53 Alternatives to AMACR: 3. GSTpi Problem: 25% of benign glands are negative, which limits the value of this marker

54 Alternatives to AMACR: 4. ERG positive in only 50% of PCa

55 Confirmation of Prostatic Origin Highly specific, tends to get lost with progression Highly specific, tends to get lost with progression Relatively specific, Increases with progression

56 Confirmation of Prostatic Origin unspecific, but typically increases with progression Highly specific, tends to get lost with progression Highly specific in ERG-positive cases (30-50%)

57 Confirmation of Prostatic Origin: NKX3.1

58 Confirmation of Prostatic Origin: HOXB13


59 HOXB13 vs. NKX3.1 which one is better? Comparison on 52 lymph node mets of PCa HOXB13 NKX3.1


60 HOXB13 vs. NKX3.1 which one is better? Comparison on 52 lymph node mets of PCa HoxB13 NKX3.1 negative 40% 2% weakmoderate 33% 37% strong 27% 61% HOXB13 NKX3.1 Kristiansen et al., Int. J. Mol. Sci. 2017, 18, 1151
 ( but do not over-use this diagnosis) Use and interpret IHC with respect and caution. Morphology rules!")
61 How to avoid (prostatic) disasters Don t rush. Take your time reading slides. 10X is a fine lens! Be aware of benign mimickers. The good thing about IHC is, that it gives you another day... David Grignon Diagnose atypia or suspicious for cancer when in doubt (>5 minutes) ( but do not over-use this diagnosis) Use and interpret IHC with respect and caution. Morphology rules!
62 Prognostic IHC in Prostate Cancer

63 Lack of prognostic markers in Prostate Cancer? on average: 10 new prognostic markers per month!
64 How reproducible are immunohistochemical prognostic markers? Pubmed: identification of 30 independent prognostic markers Br J Cancer Jan 6;112(1):140-8.
65 Validating published immunohistochemical prognostic markers: Validation cohort- 238 RPE cases (Zurich) on TMAs, 1 core/case median follow up: 5.3 years Automated immunohistochemistry (Ventana/Bond) Supervised reading of slide by a single investigator



























66 Staining Patterns of evaluated Prognostic Markers ADAM9 AKT1 ALCAM AR BCL-2 CB1R CD10 CD24 CD138 CRISP3 CRGA ECAD ERa ERb EZH2 HDAC2 HSP27 Ki-67 MUC1 NCAD NFKB p21 p27 p53 PSMA SPINK1 Fabian VIM Huber
67 Result: Forrest Plot of prognostic data Many studies are over-optimistic and insufficiently validated: Follow REMARK-guidelines red non significant A retrospective observation does not necessarily allow black a prospective significant application (p<0.05%) Quantitative cut off-based IHC is problematic Establishing a robust immunohistochemical prognostic test for patient care is difficult Br J Cancer Jan 6;112(1):140-8.
68 Ki-67 is a strong prognostic marker in.. Watchful waiting cohorts Radical prostatectomy cohorts Radiation therapy cohorts Why then is it not used in clinical practice?
69 Studies endorsing Ki-67 as a Prognostic Marker in PCa:
70 Studies endorsing Ki-67 as a Prognostic Marker in PCa: Marked Differences: - Cohort type

71 Studies endorsing Ki-67 as a Prognostic Marker in PCa: Marked Differences: - Cohort type - Endpoints
72 Studies endorsing Ki-67 as a Prognostic Marker in PCa: Marked Differences: - Cohort type - Endpoints - Cut off values
73 Studies endorsing Ki-67 as a Prognostic Marker in PCa: Marked Differences: - Cohort type - Endpoints - Cut off values - Statistics
74 Ki-67 in general: How can we standardize the staining? Pre-analytics: Analytics: - time to fixation - time in fixative, temperature - fixative (additives?) - embedding - storage conditions - sectioning - Antibody (clone Mib-1?) - IHC-protocol: HIER? Detection?
75 Is inter-lab Variability an Issue? 100 BrCa cases In TMA format Central staining 8-28% Polley et al,. J Natl Cancer Inst Dec 18;105(24):
76 Is inter-lab Variability an Issue? 100 BrCa cases In TMA format Local staining 5-33% Polley et al,. J Natl Cancer Inst Dec 18;105(24):



77 Establishing Antibody Titrations which one is optimal? 1:80 1:640 1:2500 Tolkach et al., in preparation

78 Influence of Ki-67 Antibody Dilution on Proliferation 1:80 1:640 1:2,500 1:10,000 The dilution titrates the proliferative fraction! Image analysis alone is not the solution... 1:20 1:80 1:320 1:640 1:1200 1:2500 1:5K 1:10K 1:20K Tolkach et al., in preparation


79 Testis working Group WHO March 2015, Zurich
80 New Nomenclature for Precursor lesion CIS IGCNU TIN
81 New Nomenclature for Precursor lesion CIS IGCNU TIN It is no carcinoma!
82 New Nomenclature for Precursor lesion CIS IGCNU TIN It is not intraepithelial!

83 Neue Nomenklatur für Vorläuferläsion CIS IGCNU TIN unclassified or unknown? - sounds stupid.
84 New Nomenclature for Precursor lesion CIS IGCNU IGCN GCNI GCNIS? IGCNU

85 GCNIS!!!
86 WHO 2016 Testicular Germ Cell Neoplasms GCNIS + GCNIS - Seminoma Embryonal carcinoma Yolk sac tumor postpupertal type Trophoblastic tumors Teratoma, postpubertal type Teratoma with somatic malignancy Spermatocytic Tumor Teratoma, prepubertal type Dermoid cyst Epidermoid cyst well differentiated neuroendocrine Tumor (monodermal Teratoma) Yolk sac tumor, pre-pubertal type Mixed teratoma and yolk sac tumors, pre-pubertal type
87 Trophoblastic Tumors Choriocarcinoma non-chorio-carcinomatous trophoblastic tumors: Placental site trophoblastic tumor (PSTT) Epitheloid trophoblastic tumor (ETT) Cystic trophoblastic tumor (CTT)

88

89 Epitheloid trophoblastic tumor (ETT) Trophoblastic tumor, supposedly originating from intermediate trophoblastic cells of the chorionic laeve Squamoid monophasic trophoblast cells with ample eosinophilic cytoplasm Prominent cell boundaries, cytoplasmic/extracellular eosinophilic globuli

90

91 Immunoprofile Courtesy Prof. Dan Berney, London

92 Spermatocytic Tumour Immunophenotype: PLAP and Oct3/4-negative, CD117-positive Formerly known as Spermatocytic Seminoma
93 OCT3/4 (POUF5F1) Transcription factor of embryonal stem cells, pluripotent 100% sensitivity for GCNIS, Seminoma and Embryonal Carcinoma (EC) Useful for: - Diagnosis of GCNIS - Seminoma vs. Yolk Sac Tumor or Sertoli Cell Tumor
94 Podoplanin (D2-40) Transmembranous mucoprotein, expressed in fetal germ cells, lymphangio-endothelium and mesothelium Very high sensitivity for GCNIS and Seminoma Note: up to 30% of EC are focally positive (apically, membranous) Useful for: - Diagnosis of GCNIS - Seminoma vs. Yolk Sac Tumor or Embryonal Ca
95 Placental Alkaline Phosphatase (PLAP) Enzyme of placental trophoblasts high sensitivity for GCNIS and Seminoma Note: up to 50% (!) positivity in EC/YST/CC Negative in Spermatocytic tumour and Sertoli Cell Tumor (SCT) Useful for: - Diagnosis of GCNIS - Seminoma vs. Spermatocytic Tumour / SCT

96 GCNIS

97 OCT3/4

98 D2-40

99 PLAP

100 Only Seminoma?

101 D2-40 EC component
102 CD30 (Ki-1,Ber-H2) TNF-Receptor family Membranous/Golgi staining Most EC are positive (95%) Negative in other Germ Cell Tumors Useful for: - Embryonal Carcinoma vs. Seminoma

103 CD30 EC component
104 CD117 (c-kit) Receptor Tyrosine Kinase Membranous expression in GCNIS and Seminoma Note: spermatogonia may be positive, hence not recommended to diagnose GCNIS Variable expression in YST and Spermatocytic Tumour (SpT) Negative in EC and CC Useful for: - Seminoma vs. Embryonal Carcinoma
105 SOX17 (SRY-box 17) Transcription factor of embryonal stem cells Positive in GCNIS (100%), SE (95%), YST (50%), rarely Teratoma Note: sertoli cells positive- do not use to diagnose GCNIS! Negative in EC, CC & SpT Useful for: - Seminoma vs. Embryonal Carcinoma
106 SOX2 (SRY-box 2) Transcription factor of embryonal stem cells Positive in EC (95%) and < 1% SE Note: sertoli cells positive- do not use to diagnose GCNIS! Negative in CGNIS, YST and CC Useful for: - Embryonal Carcinoma vs. Seminoma

107 SOX2 (SRY-box 2)
108 Alpha Feto-Protein (AFP) Plasmaprotein produced by YS and fetal hepatocytes Positive in YST, but quite variable... lack of staining does not rule out YST! Negative in other Germ Cell Tumors Note: glands in teratoma may be positive Useful for: - YST vs. others (less sensitive than GPC3)
109 Glypican 3 (GPC3) Membrane bound proteoglycan Positive in YST (80-100%), CC (80%), TE ( immature, 20%) and EC (5%) Negative in GCNIS and SE Note: syncytiotrophoblastic giant cells may be positive Negative in CGNIS, YST and CC Useful for: - YST vs. others (less specific than AFP)
 Solid")
110 Glypican 3 (GPC3) Solid YST
111 Human Chorionic Gonadotropin (HCG) Glycoprotein produced by placental troophoblasts and most syncytiotrophoblasts Positive in CC (100%) Note: non-diagnostic syncytiotrophoblast cells in other GCT are positive as well Useful for: - Confirmation of CC
112 GATA-3 Member of the ZNF-transcription factor family, regulates Differentiation (T-Cells, Breast, Urothelium...) Positive in a variety of malignancies: breast, urothelium, basal cell carcinomas, mesothelioma, skin SCC etc. Trophoblast cells in CC are positive Syncytiotrophoblast cells usually negative Useful for: - Confirmation of CC

113 GATA-3

114 ISUP 2013 Immunohistochemical Workflow to Diagnose Testicular Germ Cell Tumors Seminoma Embryonal Carcinoma Yolk Sac Tumor Spermatocytic tumour Choriocarcinoma
115 SALL4 Member of the ZNF-transcription factor family, involved in embryogenesis Positive in CGNIS, SE, EC & YST. 70% CCs, 50% TE. Negative in non-germ Cell Tumours. Useful for: - Sensitive Detection of Germ Cell Tumours - DD of metastatic tumours of unknown origin
116 Inhibin Glycoprotein-dimer of TGF-β family, inhibits secretion of gonadotropins Positive in Sex-cord Stroma Tumors (SCST): 100% Leydig Cell Tumors (LCT), 90% Sertoli Cell Tumors (SCT) Negative in TGCT, only syncyciotrophoblasts are positive Useful for: - SCST vs. TGCT
117 Calretinin 29 kda calclium-binding protein Positive in 100% Leydig Cell Tumors (LCT), but only few Sertoli Cell Tumors (SCT) Germ Cell Tumors are negative Note: a negative Calretin stain does not rule out sex-cord stroma tumor Useful for: - SCST vs. TGCT

118 ISUP 2013 Immunohistochemical Workflow, when SCST is in the Differential Diagnosis
119 WHO 2016 Testis: in a Nutshell GCNIS: New name for Precursor Lesion New Classification according to GCNIS/pathogenesis of disease Spermatocytic Tumor: avoiding dangers of mistreatment Robust and growing panel of Immunohistochemistry markers for accurate diagnosis


120 DISKUS 205 Thank you for your attention! The help of Prof. Dan Berney, Prof. Stefan Schweyer and Muhammad Idrees in the testis part Is greatly acknowledged.
Testicular Germ Cell Tumors; A Simplistic Approach
 Testicular Germ Cell Tumors; A Simplistic Approach Merce Jorda, MD, PhD, MBA Professor and Vice Chair, Director of Anatomic Pathology Director of Genitourinary Pathology Service Interim Director of Cytopathology
Testicular Germ Cell Tumors; A Simplistic Approach Merce Jorda, MD, PhD, MBA Professor and Vice Chair, Director of Anatomic Pathology Director of Genitourinary Pathology Service Interim Director of Cytopathology
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE. Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT
 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
Testicular Tumors: What s New, True, Important Cristina Magi-Galluzzi, MD, PhD
 Testicular Tumors: What s New, True, Important Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology, Lerner College
Testicular Tumors: What s New, True, Important Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology, Lerner College
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Pathology of the Prostate. PathoBasic Tatjana Vlajnic
 Pathology of the Prostate PathoBasic 24.01.17 Tatjana Vlajnic Overview Adenocarcinoma of the prostate Grading Special variants Mimickers of prostate adenocarcinoma Atrophy Inflammatory conditions Granulomatous
Pathology of the Prostate PathoBasic 24.01.17 Tatjana Vlajnic Overview Adenocarcinoma of the prostate Grading Special variants Mimickers of prostate adenocarcinoma Atrophy Inflammatory conditions Granulomatous
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Male Genital Cancers in the US in Frequency of Types
 Germ Cell Tumors of the Testis Pathology, Immunohistochemistry, and the Often Confusing Appearance of Their Metastases Charles Zaloudek, MD Department of Pathology UCSF Male Genital Cancers in the US in
Germ Cell Tumors of the Testis Pathology, Immunohistochemistry, and the Often Confusing Appearance of Their Metastases Charles Zaloudek, MD Department of Pathology UCSF Male Genital Cancers in the US in
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency
 Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Diagnosis, pathology and prognosis including variant pathology
 PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
BEST PRACTICES IN THE APPLICATION OF IMMUNOHISTOCHEMISTRY TO DIAGNOSTIC UROLOGIC PATHOLOGY: LESSONS FROM USES & ABUSES
 BEST PRACTICES IN THE APPLICATION OF IMMUNOHISTOCHEMISTRY TO DIAGNOSTIC UROLOGIC PATHOLOGY: LESSONS FROM USES & ABUSES Mahul B. Amin Professor & Chairman Department of Pathology & Laboratory Medicine Cedars-Sinai
BEST PRACTICES IN THE APPLICATION OF IMMUNOHISTOCHEMISTRY TO DIAGNOSTIC UROLOGIC PATHOLOGY: LESSONS FROM USES & ABUSES Mahul B. Amin Professor & Chairman Department of Pathology & Laboratory Medicine Cedars-Sinai
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA
 PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
-The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
- In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA
 Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA Learners Objectives u Latest changes per ISUP 2014 that impact
Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA Learners Objectives u Latest changes per ISUP 2014 that impact
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Immunohistochemistry. Literature Interpretation: Caveats. Must be aware of staining pattern of antibody in the relevant tissue
 IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD
 Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology,
Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology,
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
5/21/2018. Difficulty in Underdiagnosing Prostate Cancer. Diagnosis of Prostate Cancer. Evaluation of Prostate Cancer and Atypical on Needle Biopsy
 Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
Grading Prostate Cancer: Recent Changes and Refinements
 USPSTF: 2012 Report on serum PSA Screening Recommendation rating of D Reduced screening, Reduced biopsies, reduced incidence Refinements currently occurring in 2017. WHY? Grading Prostate Cancer: Recent
USPSTF: 2012 Report on serum PSA Screening Recommendation rating of D Reduced screening, Reduced biopsies, reduced incidence Refinements currently occurring in 2017. WHY? Grading Prostate Cancer: Recent
Uropathology January Jon Oxley
 Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
3/23/2017. Significant Changes in Prostate Cancer Classification, Grading, Staging and Reporting. Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Prof. Dr. med. Beata BODE-LESNIEWSKA Institute of Pathology and Molecular Pathology University Hospital; Zurich
 Prof. Dr. med. Beata BODE-LESNIEWSKA Institute of Pathology and Molecular Pathology University Hospital; Zurich 32 year old man 2 months history of growing left supraclavicular lymph nodes Antibiotic treatment
Prof. Dr. med. Beata BODE-LESNIEWSKA Institute of Pathology and Molecular Pathology University Hospital; Zurich 32 year old man 2 months history of growing left supraclavicular lymph nodes Antibiotic treatment
Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma
 Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Disclosure of Relevant Financial Relationships
 Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Macro- and microacinar proliferations of the prostate
 Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Germ cell tumours UK SH. Ivo Leuschner. Kiel Pediatric Tumor Registry, Institute of Pathology University Hospital of Schleswig-Holstein Campus Kiel
 Germ cell tumours Ivo Leuschner Kiel Pediatric Tumor Registry, Institute of Pathology University Hospital of Schleswig-Holstein Campus Kiel UK SH Old histogenetic Concept of Germ cell tumours Pluripotent
Germ cell tumours Ivo Leuschner Kiel Pediatric Tumor Registry, Institute of Pathology University Hospital of Schleswig-Holstein Campus Kiel UK SH Old histogenetic Concept of Germ cell tumours Pluripotent
Ovarian Clear Cell Carcinoma
 Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
New Developments in Immunohistochemistry for Gynecologic Pathology
 New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
Prostate Biopsy Interpretation: An Illustrated Guide
 Prostate Biopsy Interpretation: An Illustrated Guide Authors Prostate Biopsy Interpretation: An Illustrated Guide Rajal B. Shah, M.D. Director, Urologic Pathology Caris Life Sciences 6655 North MacArthur
Prostate Biopsy Interpretation: An Illustrated Guide Authors Prostate Biopsy Interpretation: An Illustrated Guide Rajal B. Shah, M.D. Director, Urologic Pathology Caris Life Sciences 6655 North MacArthur
Immunohistochemistry in prostate pathology: Recent Advances
 Immunohistochemistry in prostate pathology: Recent Advances Jae Y. Ro, M.D., Ph.D. Weill Medical College of Cornell University, Methodist Hospital, and UT MD Anderson Cancer Center, Houston, TX Yonsei
Immunohistochemistry in prostate pathology: Recent Advances Jae Y. Ro, M.D., Ph.D. Weill Medical College of Cornell University, Methodist Hospital, and UT MD Anderson Cancer Center, Houston, TX Yonsei
Testis. Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies.
 Testis Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies. Protocol revision date: January 2005 Based on AJCC/UICC
Testis Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies. Protocol revision date: January 2005 Based on AJCC/UICC
Breast cancer: IHC classification. Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
 Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Update on Reporting Prostate Cancer Pathology
 Update on Reporting Prostate Cancer Pathology Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON None Disclosures Learning Objectives
Update on Reporting Prostate Cancer Pathology Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON None Disclosures Learning Objectives
Protocol for the Examination of Lymphadenectomy Specimens From Patients With Malignant Germ Cell and Sex Cord-Stromal Tumors of the Testis
 Protocol for the Examination of Specimens From Patients With Malignant Germ Cell and Sex Cord-Stromal Tumors of the Testis Version: Testis 4.0.1.1 Protocol Posting Date: February 2019 Accreditation Requirements
Protocol for the Examination of Specimens From Patients With Malignant Germ Cell and Sex Cord-Stromal Tumors of the Testis Version: Testis 4.0.1.1 Protocol Posting Date: February 2019 Accreditation Requirements
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Intratubular Germ Cell Neoplasia of the Testis
 Intratubular Germ Cell Neoplasia of the Testis KS Ngoo Department of Urology Hospital Selayang Advanced Urology Course 15 Aug 2014 MUA Office Clinical scenario A 33 years old man has bilateral testicular
Intratubular Germ Cell Neoplasia of the Testis KS Ngoo Department of Urology Hospital Selayang Advanced Urology Course 15 Aug 2014 MUA Office Clinical scenario A 33 years old man has bilateral testicular
The Pathology of Germ Cell Tumours of the Ovary
 The Pathology of Germ Cell Tumours of the Ovary Professor Mike Wells University of Sheffield Amman, Jordan November 2013 Professor Francisco Paco Nogales I. Primitive germ cell tumors A. Dysgerminoma
The Pathology of Germ Cell Tumours of the Ovary Professor Mike Wells University of Sheffield Amman, Jordan November 2013 Professor Francisco Paco Nogales I. Primitive germ cell tumors A. Dysgerminoma
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Precursor lesions to most urologic malignancies are
 Precursor Lesions of Urologic Malignancies Francesca Khani, MD; Brian D. Robinson, MD Context. Precursor lesions of urologic malignancies are established histopathologic entities, which are important not
Precursor Lesions of Urologic Malignancies Francesca Khani, MD; Brian D. Robinson, MD Context. Precursor lesions of urologic malignancies are established histopathologic entities, which are important not
A re-audit of Prostate biopsies from January to December 2010 and 2013.
 A re-audit of Prostate biopsies from January to December 2010 and 2013. Dr. M S Siddiqui Consultant Histopathologist University Hospital of North Tees Stockton on Tees. Objectives To assess and compare
A re-audit of Prostate biopsies from January to December 2010 and 2013. Dr. M S Siddiqui Consultant Histopathologist University Hospital of North Tees Stockton on Tees. Objectives To assess and compare
OMPRN Pathology Matters Meeting 2017
 OMPRN Pathology Matters Meeting 2017 Pathology of Aggressive Prostate Cancer Intraductal Carcinoma and Cribriform Carcinoma Dr. Michelle Downes, Staff Urologic Pathologist Sunnybrook Health Sciences Centre,
OMPRN Pathology Matters Meeting 2017 Pathology of Aggressive Prostate Cancer Intraductal Carcinoma and Cribriform Carcinoma Dr. Michelle Downes, Staff Urologic Pathologist Sunnybrook Health Sciences Centre,
Establishing a definitive pathologic diagnosis in surgical
 SPECIAL ARTICLE Best Practices in the Application of Immunohistochemistry in Urologic Pathology Report From the International Society of Urological Pathology Consensus Conference Mahul B. Amin, MD,* Jonathan
SPECIAL ARTICLE Best Practices in the Application of Immunohistochemistry in Urologic Pathology Report From the International Society of Urological Pathology Consensus Conference Mahul B. Amin, MD,* Jonathan
Cardiff MRCS OSCE Courses Testicular Cancer
 Testicular Cancer Scenario: A 40-year-old male presents to the surgical out-patient clinic with a 6-8 week history of a painless lump in his left scrotum. He however complains of a dull ache in the scrotum
Testicular Cancer Scenario: A 40-year-old male presents to the surgical out-patient clinic with a 6-8 week history of a painless lump in his left scrotum. He however complains of a dull ache in the scrotum
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Pathology of Ovarian Tumours. Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh
 AFMC Pune PDCC (Cytopathology) PGI Chandigarh") Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Tinh hoàn
 Tinh hoàn Tinh hoàn Tinh hoàn Tiền liệt tuyến Tiền liệt tuyến Mào tinh hoàn Mào tinh hoàn Túi tinh Túi tinh Túi tinh Túi tinh So-called cystadenoma of seminal vesicle. Gross appearance of granulomatous
Tinh hoàn Tinh hoàn Tinh hoàn Tiền liệt tuyến Tiền liệt tuyến Mào tinh hoàn Mào tinh hoàn Túi tinh Túi tinh Túi tinh Túi tinh So-called cystadenoma of seminal vesicle. Gross appearance of granulomatous
Prostatic ductal adenocarcinoma is a subtype of
 ORIGINAL ARTICLE High-grade Prostatic Intraepithelial Neoplasialike Ductal Adenocarcinoma of the Prostate: A Clinicopathologic Study of 28 Cases Fabio Tavora, MD* and Jonathan I. Epstein, MD*w z Abstract:
ORIGINAL ARTICLE High-grade Prostatic Intraepithelial Neoplasialike Ductal Adenocarcinoma of the Prostate: A Clinicopathologic Study of 28 Cases Fabio Tavora, MD* and Jonathan I. Epstein, MD*w z Abstract:
Although current American Cancer Society guidelines
 ORIGINAL ARTICLE Diffuse Adenosis of the Peripheral Zone in Prostate Needle Biopsy and Prostatectomy Specimens Tamara L. Lotan, MD* and Jonathan I. Epstein, MD*w z Abstract: We have observed a group of
ORIGINAL ARTICLE Diffuse Adenosis of the Peripheral Zone in Prostate Needle Biopsy and Prostatectomy Specimens Tamara L. Lotan, MD* and Jonathan I. Epstein, MD*w z Abstract: We have observed a group of
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Testicular Tumors Including Secondary and Unusual Tumors of the Testis
 Testicular Tumors Including Secondary and Unusual Tumors of the Testis Milton W. Datta Partner, Hospital Pathology Associates University of Minnesota Minneapolis, MN Topics Review Features of Germ Cell
Testicular Tumors Including Secondary and Unusual Tumors of the Testis Milton W. Datta Partner, Hospital Pathology Associates University of Minnesota Minneapolis, MN Topics Review Features of Germ Cell
Diagnostic IHC in lung and pleura pathology
 Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Genetic Studies of Dysgerminoma
 Genetic Studies of Chromosome 12p abnormalities are characteristic of germ cell tumors isochromosome 12p and 12p overrepresentation Some can be detected by karyotyping FISH study of 21 dysgerminomas showed
Genetic Studies of Chromosome 12p abnormalities are characteristic of germ cell tumors isochromosome 12p and 12p overrepresentation Some can be detected by karyotyping FISH study of 21 dysgerminomas showed
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
2% of all malignancies Male predominance Patients usually more than 60 years old
 Benign Bladder Tumors Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma 90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
Benign Bladder Tumors Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma 90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
Outline (1) Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer
 Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer") Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Pathology of the lower urinary tract and male genital system
 Pathology of the lower urinary tract and male genital system Neoplasms of the lower urinary tract Incidence: Urinary bladder > upper urinary tract; male:female=3:1 Symptoms: painless hematuria, hydronephrosis
Pathology of the lower urinary tract and male genital system Neoplasms of the lower urinary tract Incidence: Urinary bladder > upper urinary tract; male:female=3:1 Symptoms: painless hematuria, hydronephrosis
Recently, there has been an increasing incidence among women and younger persons
 Bladder Tumors Benign Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma 90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
Bladder Tumors Benign Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma 90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Intraductal Carcinoma of the Prostate
 Intraductal Carcinoma of the Prostate Morphologic Features, Differential Diagnoses, Significance, and Reporting Practices The differential diagnosis for atypical cribriform lesions of the prostate has
Intraductal Carcinoma of the Prostate Morphologic Features, Differential Diagnoses, Significance, and Reporting Practices The differential diagnosis for atypical cribriform lesions of the prostate has
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Immunohistochemical classification of lung carcinomas and mesotheliomas. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Inverted (hobnail) high grade prostatic intraepithelial neoplasia and invasive inverted pattern
 high grade prostatic intraepithelial neoplasia and invasive inverted pattern") ONCOLOGY LETTERS 10: 2395-2399, 2015 Inverted (hobnail) high grade prostatic intraepithelial neoplasia and invasive inverted pattern MELTEM ÖZNUR 1, SEVIM BAYKAL KOCA 2, PELIN YILDIZ 3, BURAK BAHADIR 4
ONCOLOGY LETTERS 10: 2395-2399, 2015 Inverted (hobnail) high grade prostatic intraepithelial neoplasia and invasive inverted pattern MELTEM ÖZNUR 1, SEVIM BAYKAL KOCA 2, PELIN YILDIZ 3, BURAK BAHADIR 4
Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018
 Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018 Dr. Tzahi Neuman Dep.Of Pathology Hadassah Medical Center Jerusalem, Israel, (tneuman@hadassah.org.il) Disclosure: 1 no conflicts of
Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018 Dr. Tzahi Neuman Dep.Of Pathology Hadassah Medical Center Jerusalem, Israel, (tneuman@hadassah.org.il) Disclosure: 1 no conflicts of
Morphologic Aspects Aspects
 Testicular Testicular Germ Germ Cell Cell Neoplasia: Neoplasia: Molecular Molecular Pathways Pathways & Challenging Morphologic Aspects Aspects George George J. J. Netto, Netto, M.D. M.D. Johns Johns Hopkins
Testicular Testicular Germ Germ Cell Cell Neoplasia: Neoplasia: Molecular Molecular Pathways Pathways & Challenging Morphologic Aspects Aspects George George J. J. Netto, Netto, M.D. M.D. Johns Johns Hopkins
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Case E1. Female aged 63 years Right Nephrectomy Two separate tumours Section of each tumour
 Case E1 Female aged 63 years Right Nephrectomy Two separate tumours Section of each tumour Tumour 1 Upper pole tumour 28mm macro diameter Circumscribed Friable cut surface Tumour 2 Middle pole Part solid
Case E1 Female aged 63 years Right Nephrectomy Two separate tumours Section of each tumour Tumour 1 Upper pole tumour 28mm macro diameter Circumscribed Friable cut surface Tumour 2 Middle pole Part solid
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Quiz 1. Assign Race 1, Race 2 and Spanish Hispanic Origin to the following scenarios.
 Quiz 1 Assign Race 1, Race 2 and Spanish Hispanic Origin to the following scenarios. 1. 62 year old Brazilian female Race 1 Race 2 Spanish/Hispanic Origin 2. 43 year old Asian male born in Japan Race 1
Quiz 1 Assign Race 1, Race 2 and Spanish Hispanic Origin to the following scenarios. 1. 62 year old Brazilian female Race 1 Race 2 Spanish/Hispanic Origin 2. 43 year old Asian male born in Japan Race 1
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
6/3/2010. Outline of Talk. Lobular Breast Cancer: Definition of lobular differentiation. Common Problems in Diagnosing LCIS in Core Biopsies
 Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Review of the AP Part II Practical Examination. Dr David Clift Co Chief Examiner
 Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
The pathology of unusual subtypes of prostate cancer
 Review Article The pathology of unusual subtypes of prostate cancer Jing Li, Zhe Wang State Key Laboratory of Cancer Biology, Department of Pathology, Xi Jing Hospital, Fourth Military Medical University,
Review Article The pathology of unusual subtypes of prostate cancer Jing Li, Zhe Wang State Key Laboratory of Cancer Biology, Department of Pathology, Xi Jing Hospital, Fourth Military Medical University,
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
Transitional Cell Papilloma 2-3% Inverted Papilloma Rare
 BLADDER TUMORS Benign Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
BLADDER TUMORS Benign Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma