BEST PRACTICES IN THE APPLICATION OF IMMUNOHISTOCHEMISTRY TO DIAGNOSTIC UROLOGIC PATHOLOGY: LESSONS FROM USES & ABUSES
|
|
|
- June Poole
- 5 years ago
- Views:
Transcription
1 BEST PRACTICES IN THE APPLICATION OF IMMUNOHISTOCHEMISTRY TO DIAGNOSTIC UROLOGIC PATHOLOGY: LESSONS FROM USES & ABUSES Mahul B. Amin Professor & Chairman Department of Pathology & Laboratory Medicine Cedars-Sinai Medical Center Los Angeles, CA Best Special Studies in Surgical Pathology Good thin section and well stained H&E slides Additional sections, recuts and levels A phone call to the clinician (or reviewing the electronic medical records) Another trust-worthy pair of eyes (colleague) Placing the diagnostic dilemma in context of the clinical situation and management considerations Having a best practice approach immunohistochemistry Toward Best Practice IHC use in routine practice When IHC stains exceed H&E stain - complex case OR - Lack of best practice approach
2 Toward Best Practice IHC use in routine practice Foundation is the integration of clinical history, gross examination & microscopy Cornerstone is still the H&E with appropriate and judicious IHC support IHC guides and does not dictate the diagnosis Practice made considerably more objective by ancillary techniques e.g. IHC Toward Best Practice IHC use in routine practice Serious misdiagnoses are made by inappropriate use of IHC or incomplete knowledge of antibody/ies More is not necessarily better IHC adjunctive method, histology key If you have no idea, don t mark it Start with a question based on morphology Apply a judiciously constructed panel based on the differential diagnosis generated by the case Toward Best Practice IHC use in routine practice Panel should include expected positive and expected negatives There are no absolutely specific or sensitive antibodies Anomalous stuff happens Sensitivity and specificity is not inherent to the antibody, but to the antibody applied in a given setting Evaluate the stain paying attention to pattern (nuclear, cytoplasmic, membranous, etc.) ALWAYS evaluate the controls (positive and negative) Diagnose the case after review of IHC only in the context of the morphology and the clinical situation
3 GOWN S LAWS OF IMMUNOCYTOCHEMISTRY There is no perfect marker of any tumor There is no perfect fixative for all antibodies If everything in the tissue section appears positive, nothing is actually positive All that turns brown (or black, or red, etc.) on the slide is not positive Under inappropriate conditions, any antibody can be made to appear positive on any tissue In any given immunocytochemical run involving multiple slides, tissue will fall off the slide corresponding to the most critical antibody The diagnostic power of any immunocytochemical preparation is no greater than the knowledge and wisdom of the pathologist interpreting it SELECT BEST PRACTICE IHC APPLICATIONS IN UROLOGIC PATHOLOGY Bladder: - Proving origin/differentiation in unusual primary or at a metastatic site - IHC in flat intraepithelial lesions Prostate: - Proving origin at a metastatic site - Issues related to triple cocktail use in prostate biopsies Kidney: - Proving renal origin at a metastatic site Testis: - Screening panels for tumors involving testis primary or metastatic sites - Characterizing the various germ cell components PROVING UROTHELIAL DIFFERENTIATION Carcinoma of unknown origin or patient with history of bladder cancer: Lymph node Lung Liver Bone Prostate Unusual carcinoma in the bladder Metastatic tumors to the bladder: Melanoma Prostate Colorectal Cervix Ovary Renal Primary urothelial carcinoma: UCa with small tubules Plasmacytoid Micropapillary Etc
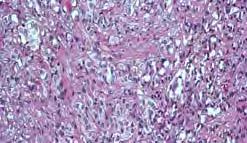
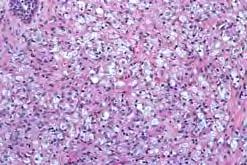
 Challenges: - Poorly differentiated carcinoma - Characterless : solid, nested & trabecular")

4 CA in a cervical LN. CA in the bladder, h.o of lung cancer UROTHELIAL CARCINOMA (Prim. or Metastatic site) Challenges: - Poorly differentiated carcinoma - Characterless : solid, nested & trabecular architecture Hallmarks: - Frequent squamous and / or glandular diff. - Cells with nuclear grooves - Nuclear atypia obvious +/- anaplasia Approach - Clinical history (invasive, usually high stage carcinoma) - Compare with primary - Judicious IHC:? Best markers



")
 (50-80%) Histogenesis")
 (20-50%)")
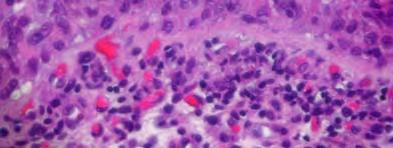
5 Paraganglioma Epith. LMS PEComa Melanoma URINARY BLADDER - IHC Diagnosis of metastatic urothelial cancer CK7 (+) (>90%) CK20 (+) (40-70%) Traditional, Broad Markers p63 (+) (60-90%) High molecular weight cytokeratin 34ßE12 (+) (60-90%) GATA3 (60-70%) Uroplakin II (+) (50-80%) Histogenesis Associated S100P (70-80%) Uroplakin III (+) (20-50%) Thrombomodulin (+) (60-75%) CEA, Leu-M1 (±) (minimal value)




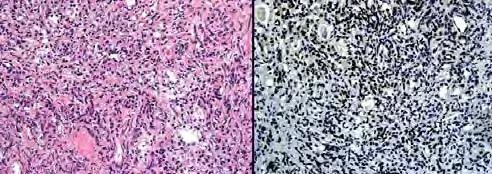
6 Plasmacytoid U Ca Plasmacytoid U.Ca - CK20 Markers of urothelium and urothelial carcinoma by cdna microarray GATA 3 & S100P Am J Surg Pathol 2007;31:






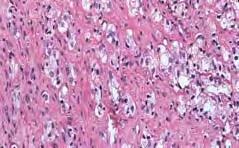
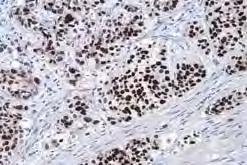
7 S100P(commercial) Nuclear staining accompanied by cytoplasmic staining More sensitive but less specific than GATA3 Other tumors stainedpancreaticobiliary, breast? S100P S100P GATA3 GATA3 A-F: S100P,G: GATA; H: CK 5/6; I: p63 Nuclear staining lower sensitivity but higher specificity than S100P for urothelium GATA3




, with higher sensitivity (73% vs 37%, respectively, p=0.001). Smith et al.")
8 GATA3 Wide Range of Expression Positive in Breast, trophoblastic tumors, paragangliomas, salivary gland neoplasms, squamous carcinomas, basal cell carcinomas, yolk sac tumors, pancreatic ductal adenocarcinomas Mietinnen et al. Am J Surg Pathol 2013 Uroplakins II and III Protein constituents of the urothelial plaques in vesicles of urothelium Vital role in expansion and contraction through vesicle cycling Subunits uroplakins Ia, Ib, II, and IIIa Unique and characteristic feature of urothelium Previous data for UP3, new data for UP2 Uroplakin 3 Uroplakin 2 versus Uroplakin 3 UP3 UP2. Among UC metastases, UP2 showed greater intensity and proportion, (both p<0.001), with higher sensitivity (73% vs 37%, respectively, p=0.001). Smith et al. Histopathology. In press





9 Uroplakin 2 versus Uroplakin 3 UP3 UP2 Villoglandular variant simulates colorectal carcinoma Smith et al. Histopathology. In press CIS REACTIVE ATYPIA CIS REACTIVE
, CK20 Indications: Marked denudation residual basal cells vs clinging")
 Pathologist favors CIS but has reservations making diagnosis CIS")

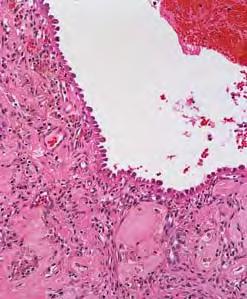
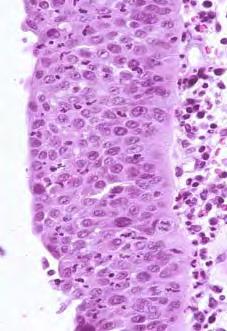
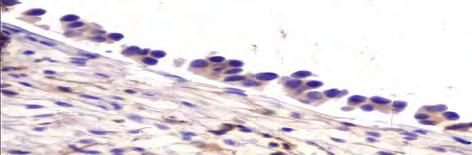
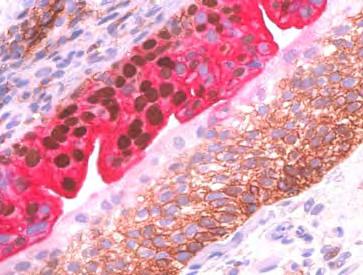
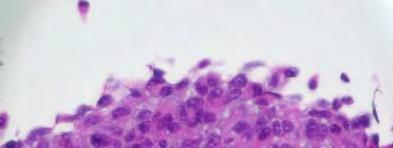
10 IMMUNOHISTOCHEMISTRY IN FLAT LESIONS OF THE BLADDER Panel: p53, CD44 (standard isoform), CK20 Indications: Marked denudation residual basal cells vs clinging CIS Distinction between reactive atypia and CIS (large cell nonpleomorphic or small cell) Pathologist favors CIS but has reservations making diagnosis CIS with unusual morphology Pagetoid, undermining, etc. Caveats: Not applicable for dysplasia vs CIS Greater caution while evaluaiting post-treatment biopsies NORMAL NORMAL p53



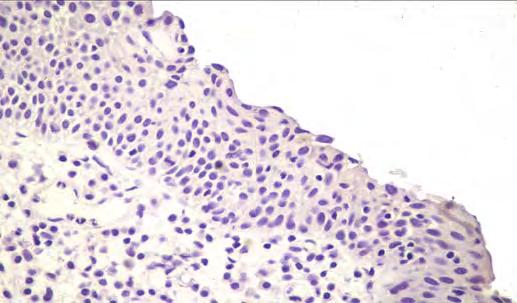
11 CK-20 CD-44 REACTIVE UROTHELIUM


12 p53 CK-20 CD-44





13 Reactive CD44 Reactive- CK20 Reactive- p53 Fig 9C CA-INSITU



14 p53: 55-80% of CIS p53 CK-20 CK20 (+) : % of CIS CD44 CD44 (-) : % of CIS


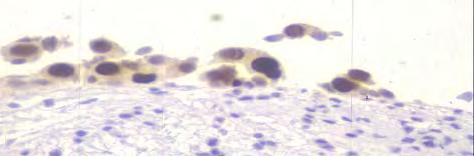


15 CIS CK20 Regenerative basal cells vs. clinging CIS p53 CK20 (+) CD44(-)



16 PAGETOID CIS p53 CK20






17 CD44 CIS Reactive Am J Surg Pathol 2013 CK20/p53/CD44 Triple Stain

: Granular")

: Membranous - Prostatic")
18 UROTHELIAL ASSOCIATED-MARKERS Prostate vs. Urothelial Carcinoma - Often in bladder neck specimens - Therapeutically critical differential PSA PSAP NKX1.3 Prostein (P501S) ERG-TMPRSS2 PSMA CAUTION: Both may coexist! CK20 P63 or MWCK GATA3 Uroplakin 2 S100p Uroplakin 3 New Prostate Lineage Associated Markers Prostein (P501S): Granular Golgi Pattern - Prostatic carcinoma independent of Gleason pattern and metastatic status - Rarely in villous adenoma and adenocarcinoma of bladder NKX3.1: Nuclear Pattern - Prostatic epithelium, testis, bronchial mucous glands, rare ureteral urothelial cells - Prostatic carcinoma and infiltrating lobular carcinoma Prostate Specific Membrane Antigen (PSMA): Membranous - Prostatic epithelium, endometrial glands, duodenal mucosa, proximal renal tubules, urothelium, neuroendocrine cells of colonic crypts and endothelium - Prostatic adenocarcinoma, gastric carcinoma, small cell carcinoma of lung, urothelial carcinoma and GBM

19 GATA- 3 NKX3.1 S100P PSMA p501s Concurrent PCa & UCa









20 ?Urothelial Carcinoma vs.?prostatic Carcinoma UCa PCa?Urothelial Carcinoma vs.?prostatic Carcinoma UCa PCa UCa GATA3 CK5/6 S100P







21 PCa PCa NKX3.1 P501S PSMA ERG IHC Urothelial carcinoma Prostatic adenocarcinoma Prostatic adenocarcinoma

 Post treatment")
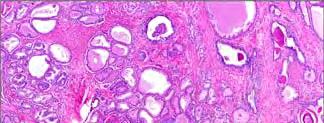
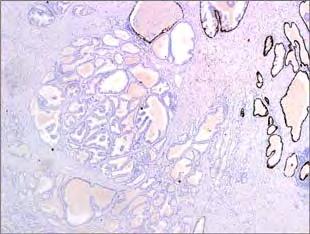
22 Atypical focus Prostatic origin Non prostatic origin Mimics of malignancy: Atrophy Basal hyperplasia etc PIN ASAP v/s Carcinoma NA Mesonephric remnants Cowper glands Architecture Basal layer Nuclear features Quantity Additional morphologic features IHC Indications for IHC Needle Biopsy Atypical small cell proliferations To confirm focus as cancer Confirm benignity in ASAP felt to be benign Unusual patterns Atrophic Pseudohyperplastic Double layer PIN-like Atypical large acinar proliferations (intraductal patterns) Post treatment setting
23 IHC in a pt. with one (+) core Confirm bilaterality- clinical staging - almost 50% patients with prostate cancer treated with RT Accurate assessment of # of cores involved Active surveillance Quantitation of cancer Active surveillance (>50% may exclude) Quantitation of Tumor Involvement 2 mm 8 mm 2 mm Eyeball estimate: 10% Linear measurement: 4 mm % of core involvement: 4 mm 20 mm 20 mm = 20 % Work-up of Atypical Foci with Definite Cancer in Other Parts Patient with Gleason score 3+4 or higher grade cancer on at least one part.? Work up other parts with small foci of possible 3+3=6 Generally, not indicated, as additional IHC confirmation will likely not change management

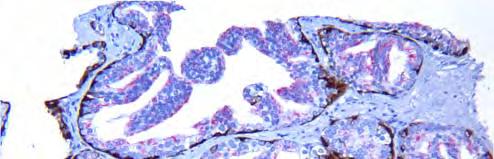
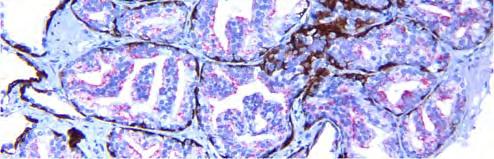
24 IHC in Prostate Needle Bxs. Basal cell cocktail - p63 and 34 E12 Triple cocktail PIN cocktail - p63/34 E12/AMACR ERG immunohistochemistry - Additional marker, only if triple not conclusive PSA to prove prostate origin NA, Cowper's glands Triple cocktail HWCK/p63 (CK5/6) basal cells AMACR cancer cells 37 68% of atypical cases were confirmed as cancer Overcomes problems associated with individual markers Foci often limited
, HMCK(-), AMACR(+) Benign small cancer mimics:")
, AMACR(+) Intraductal component: p63, HMCK(+), AMACR(+) Urothelial cancer: p63,")
25 p63 Review with respect to external & titration of antibody is very important internal controls Triple cocktail Expected reactions PCa: p63(-), HMCK(-), AMACR(+) Benign small cancer mimics: p63, HMCK(+), AMACR(-) HGPIN: p63, HMCK(+), AMACR(-/+) Ductal cancer: Invasive component: p63, HMCK(-), AMACR(+) Intraductal component: p63, HMCK(+), AMACR(+) Urothelial cancer: p63, HMCK(+/-), AMACR(+)





26 P63, HMWCK and AMACR cocktail




27

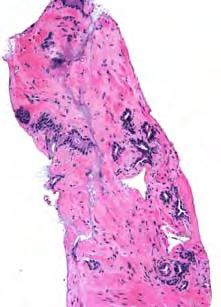

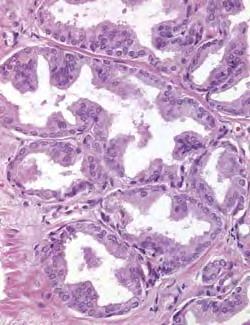
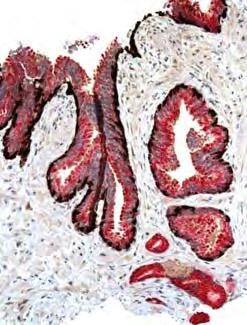
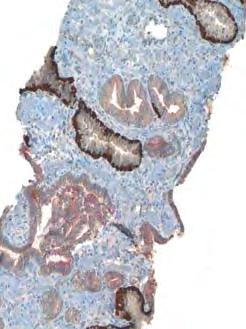
28 PCa with atrophic appearance Atrophy CANCER WITH ATROPHIC PATTERN PIN LIKE PCa


29 PIN LIKE PCa PIN LIKE P Ca




30 12 cores, only 1 positive core with 2 atypical ducts



31


32 EQUIVOCAL IHC Results not entirely complimentary - Unexpected basal cell layer staining - Results supportive but all glands in an already small or difficult focus not represented in the IHC






33 HGPIN + ASAP p63, HMWCK and AMACR cocktail


34 Atrophic/basloid aberrant p63 (+)



35 p63, HMWCK and AMACR cocktail PSA






36 ERG Immunohistochemistry 60% of PCa harbor any ETS-rearrangement 50% of PCa TMPRSS2-ERG Detection by IHC or FISH High concordance in hormone naive IHC detection in ~30% in needle setting Do we need a 4 th marker? Helps in about 5% of cases with equivocal triple cocktail Additional: Marker of prostate histogenesis



37




38 Post-treatment Prostate Cancer Recommended panel CK to detect isolated PCa cells PIN cocktail (or HMCK/p63+/- racemase) to confirm malignancy Biologic potential of cancer MIB1 (investigational) IHC IN KIDNEY SURGICAL PATHOLOGY Confirming Renal origin Histologic subtyping of RCC Metastatic sites Primary tumors Small biopsies and FNAS PEComa Urothelial Ca Adrenocortical Ca Melanoma
39 CONFIRMING RENAL ORIGIN Carcinoma of unknown origin or patient with history of RCC: Lymph node Lung Liver Bone Other Unusual carcinoma in the kidney Epithelioid PEComa Urothelial Carcinoma Metastatic carcinoma to the kidney versus Poorly differentiated, high grade RCC (unclassified) versus Lymphoma, sarcoma, melanoma, other APPROACH TO APPLICATION OF IHC IN RENAL TUMORS Is the neoplasm a carcinoma?: rule out Epi AML (PEComa), lymphoma, sarcoma, melanoma etc Is the carcinoma a renal primary?: rule out urothelial carcinoma, metastasis Can you subtype the renal cell carcinoma?: Clear cell vs papillary vs chromophone vs oncocytoma vs translocation associated Ca.. CONFIRMING RENAL ORIGIN Is the neoplasm a carcinoma?: Renal related AE1/AE3 (+) EMA (+) Vimentin (+) CK7 (-), CK20 (-) Is the carcinoma a renal primary?: Renal associated RCC marker (80%) PAX 2 or PAX8 (>90%) S100A1* CD10 (+) (94%)
 and Ksp-Cadherin (+) Consider: Epithelioid")
 Papillary RCC (95%) Oncocytoma & Chromophome (-/+) Collecting duct Ca (- /+) RCC")

40 If history of renal mass and renal histogenesis markers are negative? Consider: Chromophobe carcinoma CD117 (+) and Ksp-Cadherin (+) Consider: Epithelioid PEComa and translocation carcinoma Cathepsin K, MelanA/HMB45 RCC types Clear cell RCC (85%) Papillary RCC (95%) Oncocytoma & Chromophome (-/+) Collecting duct Ca (- /+) RCC antigen Monoclonal antibody against brush border of healthy PCT Other tumors Breast ca Parathyroid ca Embryonal ca, testis Lung Prostate Ovary Melanoma Epididymal cystadenoma Mesothelioma RCC CD10

 RCC types Clear cell RCC Ca (- /+) PAX8 Paired box transcription factor, similar to PAX2 Predominantly data from polyclonal antibody new monoclonal Other tumors Similar to Pax2 Thyroid")
41 PAX2 Pax2 is a transcription factor - normal organogenesis of the kidney, Mullerian organs, brain, eye during fetal life Other tumors Nephrogenic adenoma Parathyroid adenoma & carcinoma Clear cell adenocarcinoma Uterine and ovarian serous and endometrioid tumors Adnexal tumors Breast carcinomas Lung tumors Colonic malignancies Lymphoma Melanoma Prostate carcinoma RCC types Clear cell RCC (>95%) Papillary RCC (>95%) Wilms tumor Metanephric (+) adenoma Oncocytoma (+) Chromophobe RCC (-/+) Collecting duct Ca (-/+) Translocation assoc. Ca (- /+) RCC types Clear cell RCC (>95%) Papillary RCC (>95%) Wilms tumor Metanephric (+) adenoma Oncocytoma (+) Chromophobe RCC (-/+) Collecting duct Ca (-/+) Translocation assoc. Ca (- /+) PAX8 Paired box transcription factor, similar to PAX2 Predominantly data from polyclonal antibody new monoclonal Other tumors Similar to Pax2 Thyroid neoplasms Extensive GYN positivity Metastatic Clear cell RCC (Bone) 85 % of met RCC are PAX 2 (+)

 Pap RCC (80%)")



 Other")
42 PARATHYROID CARCINOMA PAX-2 Clear cell RCC Papillary RCC PAX 2 Positive in RCC Clear cell RCC (60%) Pap RCC (80%) Clear cell-pap RCC Oncocytoma S100A1 Among the 13 member S100 protein family. Expressed in numerous cell types, not well studied Translocation assoc RCC Chromophobe RCC (-) Other tumors Ovarian Ca (serous, clear) Endometrial Ca
 Papillary RCC (+/-) Chromophobe RCC (-) Oncocytoma (-) Urothelial Ca (+/-) Other tumors")

")
43 S100A1 Picture Carbonic anhydrase IX Family of zinc containing metalloproteinase that regulates cell proliferation, adhesion and metastasis Kidney tumors Clear cell RCC (+) Papillary RCC (+/-) Chromophobe RCC (-) Oncocytoma (-) Urothelial Ca (+/-) Other tumors Most carcinomas of endometrium, stomach, lung, cervix, liver, breast etc. Prognostic utility of CA IX in clear cell RCC Carbonic Anhydrase IX Predictive/Prognostic Prognostic value: controversial with some studies showing low expression (<=85%) correlated with worse overall survival in metastatic RCC High CAIX expression (>85%) predictive of response to IL-2, but final results are awaiting a prospective phase 2 SELECT trial High CAIX expression (>85%) associated with more tumor shrinkage in response to Sorafenib treatment







44 CARBONIC ANHYDRASE IX \ CLEAR CELL PAPILLARY RCC UCa Ca IX Ksp-cadherin in distal convoluted tubules


: >85% cases, diffuse t(x;17):")

45 Ksp-cadherin Oncocytoma Chromophobe RCC Cathepsin K Expression is related to overexpression of MiTF PEComas: moderate to strong and diffuse cytoplasmic staining is seen in all variants co-expressed with other melanocytic markers (more diffuse than HMB-45) MiTF-TFE3 translocation associated carcinomas t(x;1): >85% cases, diffuse t(x;17): 0% t(6;11): 100% of cases, diffuse Other renal tumors: Negative except nonspecific in necrotic areas Cathepsin K PEComa (E-AML)
46 Histologic subtyping of renal epithelial tumors Clear RCC vs. Chromophobe RCC: CA-9, PAX2/8, RCC, vimentin, CD10 vs. Kspcadherin, CD117 Clear RCC vs. Papillary RCC CK7 and racemase Renal Oncocytic Tumors Oncocytoma CK 7 (- / +) EPCAM (- / +) PAX -2 (+) Claudin 7 (-) S100 A1 (+) Chromophobe RCC CK 7 (+ / -) EPCAM (+/ -) PAX -2 (-/+) Claudin 7 (+) S100A1 (-) Amylase 1A (AMY1A) and Caveolin 1 - Investigational *Not adequately studied: preliminary data Not tested in hybrid oncocytic tumors* Histologic subtyping of renal epithelial tumors Papillary RCC vs Metanephric adenoma CK 7, racemase vs WT1,CD57 Papillary, MTS cell ca: CK7, Racemase (both+ in both tumors) Conv. RCC vs.translocation carcinoma: Keratin, Cathepsin K, TFE3, TFEB, MelanA/HMB-45
 Vimentin (+) CA-9 (+) CK7 & racemase (-) Papillary RCC only RCC (+) CK7 (+)")
")
,")
47 Renal Clear and Papillary Tumors Clear cell & Papillary RCC RCC (+) Pax2, Pax8 (+) Vimentin (+) CA-9 (+) CK7 & racemase (-) Papillary RCC only RCC (+) CK7 (+) Racemase (+) Clear Papillary RCC CK 7(+) Racemase (-) RCC(-) HMCK (+) CD 117 TESTIS IHC: Screening panels Germ cell tumors - OCT 3/4 - SALL4 - PLAP - EMA(-) - Vimentin (-) Sex cord tumors -SF1 - Melan A - Inhibin -Calretinin - CD99 - Synaptophysin - S-100 Lymphoma: CD-45, CD3, L26 Visceral malignancy: EMA (+), vimentin (±)
 fixed sections Adequate sampling is key - the # of IHCs should NEVER exceed the H&E slides Remember what matters in germ cell")
48 LEYDIG CELL TUMOR INHIBIN SERTOLI CELL TUMOR CALRETININ IHC in characterizing the different germ cell components There is no substitute to well (overnight) fixed sections Adequate sampling is key - the # of IHCs should NEVER exceed the H&E slides Remember what matters in germ cell tumors
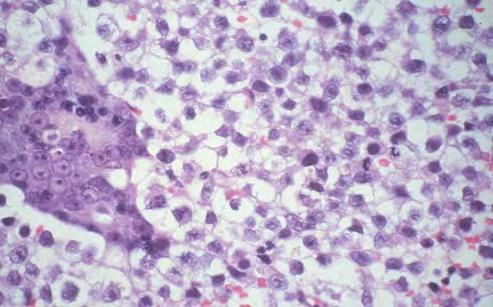
49 GERM CELL TUMOR What really matters? One does not necessarily have to characterize every morphologically different focus Pure classic Seminoma vs. non-seminomatous components Mixed germ cell tumor -Specify components (as accurately as you can) ->80% or pure embryonal carcinoma ( ) ->50% teratoma ( ) Vascular-lymphatic invasion pathologic stage Margin status IHC IN GERM CELL TUMORS ITGCN: Oct3/4, c- kit SALL4, Podoplanin,, PLAP Seminoma: Oct3/4, c-kit, Podoplanin Embryonal Ca: Oct3/4, CD30, Keratin weak, SOX2 YST: Glypican, AFP, Keratin strong CC: HPL, βhcg, Glypican-syncytiotrophoblasts Cytokeratin AE1/AE3: E Ca, YST, T, CC Oct 3/4: Seminoma, E Ca PLAP: Minimal / no value except in ITGCN Useful Antibodies for Testicular Neoplasms: SALL4 Zinc finger nuclear transcription factor with role in embryonic development ~100% sensitive for IGCNU, seminoma, EC & YST; 69% of CCs & 52% of teratomas Negative in other testis tumors Other + tumors: ALCL, rhabdoid tumor, Wilms tumor, precursor B-cell ALL, AML & ~ 5% of GI tract adenoca Caveat: Non-neoplastic germ cells are + Overview: Sensitive general GCT marker valuable for GCT vs non-gct of testis and in DX of metastatic GCTs; sensitive YST marker, unlike OCT4



50 Useful Antibodies for Testicular Neoplasms: SOX2 (SRY-box 2) Member of the SOX family of nuclear transcription factors involved in embryonic development; needed for pluripotency of undifferentiated embryonic stem cells Positive in 96% of ECs & <1% of seminomas Negative in YSTs, CCs & IGCNU Other nuclear + tumors: immature elements in teratoma, melanoma & rhabdoid tumors Caveat: Non-neoplastic Sertoli cells are + Overview: Mostly useful for seminoma vs EC. May become a preferred marker for seminoma vs EC but the panelists considered it currently technically difficult MALIGNANT SERTOLI CELL TUMOR MALIGNANT SERTOLI CELL TUMOR

 Seminoma 0% ITGCN 0%")
51 MALIGNANT SERTOLI CELL TUMOR Keratin AE1/AE3 Glypican-3 expression in testicular germ cell tumors Yolk sac tumor 100% Embryonal carcinoma 0-8% Choriocarcinoma % Teratoma 0-40% (*immature elements) Seminoma 0% ITGCN 0% ITGCN





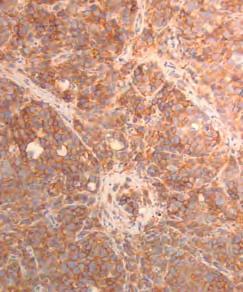
52 PLAP CKIT OCT3 Pitfall: normal spermatogonia in adult testis Pitfall: normal spermatogonia in adult testis C KIT false (+) Oct 3 more specific for ITGCN
53 GERM CELL TUMORS - IHC Intratubular germ cell neoplasia Oct 3/4 (+) c-kit (+) Podoplanin (+) PLAP (+) Classic seminoma Oct 3/4, c-kit, & Podoplanin (+) AE 1 /AE 3, CAM 5.2: usually (-) (or focal) Sox2 (-) CD30: usually (-) (or focal) AFP: (-) Spermatocytic seminoma Negative for most markers except CD117 (+/-), GERM CELL TUMORS - IHC Embryonal carcinoma AE 1 /AE 3, CAM 5.2: (+) CD30 : (+) Oct 3/4 (+) Sox2 (+) AFP(-) c-kit: (-) Endodermal sinus tumor (YST) AE 1 /AE 3, CAM 5.2: (+) AFP: (+) Glypican 3 (+) CD30 (Ber-H2): (-) c-kit: (-) Oct 3/4 (-) Choriocarcinoma AE 1 /AE 3, CAM 5.2: (+) ßHCG: (+) Human placental lactogen: (+) Oct 3/4 (-) SEMINOMA PLAP OCT3 CKIT




54 Oct 4



55 AE1/AE3 SEMINOMA: CLASSIC VS SPERMATOCYTIC CD117 Spermatocytic seminoma: (-) for Oct3/4 Weak CD117 and SALL4 OCT3/4 SALL4
 Membrane anchored heparan")
, CCs (80%), teratomas ( immature )")



56 Useful Antibodies for Testicular Neoplasms: Glypican 3 (GPC3) Membrane anchored heparan sulfate proteoglycan Positive in YSTs (100%), CCs (80%), teratomas ( immature ) (17%) & rare ECs (5%) Negative in IGCNU & seminoma Other + tumors: hepatocellular and gastric cancers Caveats: Syncytiotrophoblast cells are often positive (71%) Overview: More sensitive but less specific for YST among testis GCTs than AFP YST Glypican CC Glypican
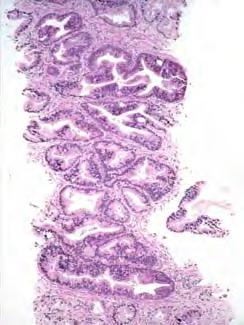
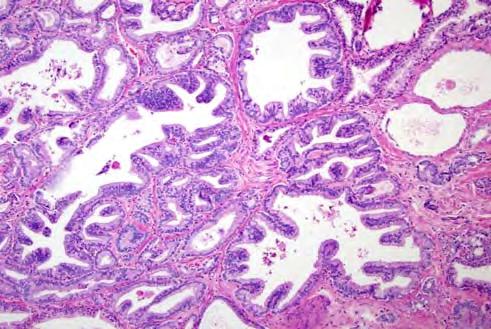
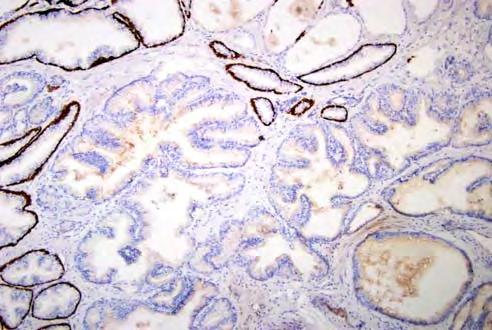
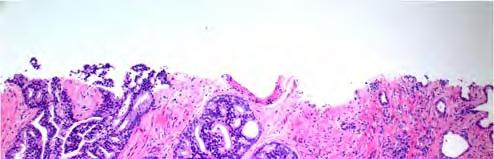
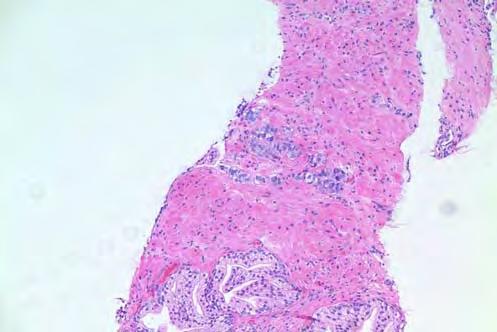
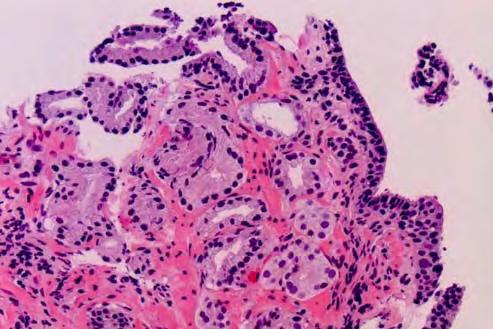
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
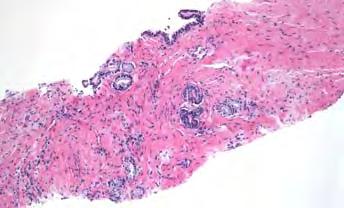
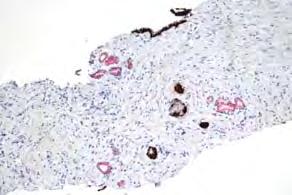
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Testicular Germ Cell Tumors; A Simplistic Approach
 Testicular Germ Cell Tumors; A Simplistic Approach Merce Jorda, MD, PhD, MBA Professor and Vice Chair, Director of Anatomic Pathology Director of Genitourinary Pathology Service Interim Director of Cytopathology
Testicular Germ Cell Tumors; A Simplistic Approach Merce Jorda, MD, PhD, MBA Professor and Vice Chair, Director of Anatomic Pathology Director of Genitourinary Pathology Service Interim Director of Cytopathology
IMMUNOPROFILES OF THE MAJOR RENAL NEOPLASMS (%staining)
") Stain Clear Cell Papillary IMMUNOPROFILES OF THE MAJOR RENAL NEOPLASMS (%staining) Chromophobe Collecting Duct Carcinom a Sarcomatoid Xp11 Translocat ion Dr Jon Oxley See also www.jonoxley.com Page 1 MTSCC
Stain Clear Cell Papillary IMMUNOPROFILES OF THE MAJOR RENAL NEOPLASMS (%staining) Chromophobe Collecting Duct Carcinom a Sarcomatoid Xp11 Translocat ion Dr Jon Oxley See also www.jonoxley.com Page 1 MTSCC
New Developments in Immunohistochemistry for Gynecologic Pathology
 New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Male Genital Cancers in the US in Frequency of Types
 Germ Cell Tumors of the Testis Pathology, Immunohistochemistry, and the Often Confusing Appearance of Their Metastases Charles Zaloudek, MD Department of Pathology UCSF Male Genital Cancers in the US in
Germ Cell Tumors of the Testis Pathology, Immunohistochemistry, and the Often Confusing Appearance of Their Metastases Charles Zaloudek, MD Department of Pathology UCSF Male Genital Cancers in the US in
Differential diagnosis of HCC
 Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA
 PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
Establishing a definitive pathologic diagnosis in surgical
 SPECIAL ARTICLE Best Practices in the Application of Immunohistochemistry in Urologic Pathology Report From the International Society of Urological Pathology Consensus Conference Mahul B. Amin, MD,* Jonathan
SPECIAL ARTICLE Best Practices in the Application of Immunohistochemistry in Urologic Pathology Report From the International Society of Urological Pathology Consensus Conference Mahul B. Amin, MD,* Jonathan
The Panel Approach to Diagnostics. Lauren Hopson International Product Specialist Cell Marque Corporation
 The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
Prostate Immunohistochemistry. Literature Interpretation: Caveats. Must be aware of staining pattern of antibody in the relevant tissue
 IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Renal tumours: use of immunohistochemistry & molecular pathology. Dr Lisa Browning John Radcliffe Hospital Oxford
 Renal tumours: use of immunohistochemistry & molecular pathology Dr Lisa Browning John Radcliffe Hospital Oxford Renal tumours: the use of immunohistochemistry & molecular pathology Classification of RCC
Renal tumours: use of immunohistochemistry & molecular pathology Dr Lisa Browning John Radcliffe Hospital Oxford Renal tumours: the use of immunohistochemistry & molecular pathology Classification of RCC
Diagnostic IHC in lung and pleura pathology
 Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Breast cancer: IHC classification. Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
 Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
NEW IHC A n t i b o d i e s
 NEW IHC Antibodies TABLE OF CONTENTS NEW IHC ANTIBODIES from Cell Marque CITED1 (5H6).... 1 Claudin 7 (5D10F3).... 1 GATA1 (4F5).... 1 Transgelin (2A10C2).... 1 NEW IHC ANTIBODIES using RabMAb Technology
NEW IHC Antibodies TABLE OF CONTENTS NEW IHC ANTIBODIES from Cell Marque CITED1 (5H6).... 1 Claudin 7 (5D10F3).... 1 GATA1 (4F5).... 1 Transgelin (2A10C2).... 1 NEW IHC ANTIBODIES using RabMAb Technology
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
INTERPRETATION OF IMMUNOHISTOCHEMICAL STAINS - DIFFICULTIES AND PITFALLS. Gabor Fischer Diagnostic Services Manitoba University of Manitoba
 INTERPRETATION OF IMMUNOHISTOCHEMICAL STAINS - DIFFICULTIES AND PITFALLS Gabor Fischer Diagnostic Services Manitoba University of Manitoba IHC INTERPRETATIONS LOCAL DATA Diagnostic Services Manitoba Number
INTERPRETATION OF IMMUNOHISTOCHEMICAL STAINS - DIFFICULTIES AND PITFALLS Gabor Fischer Diagnostic Services Manitoba University of Manitoba IHC INTERPRETATIONS LOCAL DATA Diagnostic Services Manitoba Number
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency
 Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Histopathological diagnosis of CUP
 Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Immunohistochemical classification of lung carcinomas and mesotheliomas. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY
 CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY Jason L Hornick, MD, PhD Director of Surgical Pathology Director of Immunohistochemistry Brigham and Women s Hospital Associate
CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY Jason L Hornick, MD, PhD Director of Surgical Pathology Director of Immunohistochemistry Brigham and Women s Hospital Associate
Reporting of carcinoma of unknown primary tumour (CUP)
") Reporting of carcinoma of unknown primary tumour (CUP) Prof John Schofield Kent Oncology Centre with grateful thanks to Dr Karin Oien University of Glasgow Royal College of Pathologists Cancer datasets
Reporting of carcinoma of unknown primary tumour (CUP) Prof John Schofield Kent Oncology Centre with grateful thanks to Dr Karin Oien University of Glasgow Royal College of Pathologists Cancer datasets
Immunohistochemistry and Bladder Tumours
 Immunohistochemistry and Bladder Tumours Dr. Andrew J. Evans MD PhD FRCPC Consultant in Genitourinary Pathology University Health Network Toronto, ON Objec ves Review markers of urothelial differen a on
Immunohistochemistry and Bladder Tumours Dr. Andrew J. Evans MD PhD FRCPC Consultant in Genitourinary Pathology University Health Network Toronto, ON Objec ves Review markers of urothelial differen a on
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018
 Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018 Dr. Tzahi Neuman Dep.Of Pathology Hadassah Medical Center Jerusalem, Israel, (tneuman@hadassah.org.il) Disclosure: 1 no conflicts of
Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018 Dr. Tzahi Neuman Dep.Of Pathology Hadassah Medical Center Jerusalem, Israel, (tneuman@hadassah.org.il) Disclosure: 1 no conflicts of
Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2 on all newly diagnosed cases
 GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2 on all newly diagnosed cases") Adrenal cortical carcinoma Inhibin Synap Melan-A Calretinin Vimentin Chromogr CK7 CK20 Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2
Adrenal cortical carcinoma Inhibin Synap Melan-A Calretinin Vimentin Chromogr CK7 CK20 Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Biopsy diagnosis of renal tumors. Current applications Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Czech Republic Dealing
Enterprise Interest Nothing to declare Biopsy diagnosis of renal tumors. Current applications Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Czech Republic Dealing
5/21/2018. Difficulty in Underdiagnosing Prostate Cancer. Diagnosis of Prostate Cancer. Evaluation of Prostate Cancer and Atypical on Needle Biopsy
 Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
Unknown Slides Conference
 Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Unknown Slides Conference Jae Y. Ro, MD, PhD Weill Medical College of Cornell Univ. The Methodist Hospital, and UT MD Anderson Cancer Center Houston, TX November 9, 2013 Amman, Jordan 25 th Congress of
Pathology of the Prostate. PathoBasic Tatjana Vlajnic
 Pathology of the Prostate PathoBasic 24.01.17 Tatjana Vlajnic Overview Adenocarcinoma of the prostate Grading Special variants Mimickers of prostate adenocarcinoma Atrophy Inflammatory conditions Granulomatous
Pathology of the Prostate PathoBasic 24.01.17 Tatjana Vlajnic Overview Adenocarcinoma of the prostate Grading Special variants Mimickers of prostate adenocarcinoma Atrophy Inflammatory conditions Granulomatous
Carcinoma of Unknown Primary (CUP)
") Metasta c Carcinoma of Unknown Primary: Diagnos c Approach Using Immunohistochemistry James R. Conner, MD, PhD Mount Sinai Hospital Toronto, ON Carcinoma of Unknown Primary (CUP) 3-5% of all new malignant
Metasta c Carcinoma of Unknown Primary: Diagnos c Approach Using Immunohistochemistry James R. Conner, MD, PhD Mount Sinai Hospital Toronto, ON Carcinoma of Unknown Primary (CUP) 3-5% of all new malignant
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Carcinoma of unknown primary origin (CUP) is defined
 is defined") REVIEW ARTICLE Metastatic Carcinoma of Unknown Primary: Diagnostic Approach Using Immunohistochemistry James R. Conner, MD, PhD and Jason L. Hornick, MD, PhD Abstract: Carcinoma of unknown primary origin
REVIEW ARTICLE Metastatic Carcinoma of Unknown Primary: Diagnostic Approach Using Immunohistochemistry James R. Conner, MD, PhD and Jason L. Hornick, MD, PhD Abstract: Carcinoma of unknown primary origin
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
-The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
- In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Adenocarcinoma of the Cervix
 Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Prof. Dr. med. Beata BODE-LESNIEWSKA Institute of Pathology and Molecular Pathology University Hospital; Zurich
 Prof. Dr. med. Beata BODE-LESNIEWSKA Institute of Pathology and Molecular Pathology University Hospital; Zurich 32 year old man 2 months history of growing left supraclavicular lymph nodes Antibiotic treatment
Prof. Dr. med. Beata BODE-LESNIEWSKA Institute of Pathology and Molecular Pathology University Hospital; Zurich 32 year old man 2 months history of growing left supraclavicular lymph nodes Antibiotic treatment
FINALIZED SEER SINQ QUESTIONS
 0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
Tinh hoàn
 Tinh hoàn Tinh hoàn Tinh hoàn Tiền liệt tuyến Tiền liệt tuyến Mào tinh hoàn Mào tinh hoàn Túi tinh Túi tinh Túi tinh Túi tinh So-called cystadenoma of seminal vesicle. Gross appearance of granulomatous
Tinh hoàn Tinh hoàn Tinh hoàn Tiền liệt tuyến Tiền liệt tuyến Mào tinh hoàn Mào tinh hoàn Túi tinh Túi tinh Túi tinh Túi tinh So-called cystadenoma of seminal vesicle. Gross appearance of granulomatous
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
What I Learned from 3 Cases and 3 Antibodies
 What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships
What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
RENAL EPITHELIAL NEOPLASMS: IS THERE A ROLE OF IMMUNOSTAINS IN DIAGNOSIS?
 RENAL EPITHELIAL NEOPLASMS: IS THERE A ROLE OF IMMUNOSTAINS IN DIAGNOSIS? John C. Cheville, M.D. Mayo Clinic and Mayo Foundation Rochester, MN The majority of renal epithelial neoplasms are diagnosed on
RENAL EPITHELIAL NEOPLASMS: IS THERE A ROLE OF IMMUNOSTAINS IN DIAGNOSIS? John C. Cheville, M.D. Mayo Clinic and Mayo Foundation Rochester, MN The majority of renal epithelial neoplasms are diagnosed on
2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseudocapsule
 GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Uropathology January Jon Oxley
 Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Tumour Markers. For these reasons, only a handful of tumour markers are commonly used by most doctors.
 Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Tumours of the Prostate and Testis update on WHO classification, IHC and molecular Morphology
 Tumours of the Prostate and Testis update on WHO classification, IHC and molecular Morphology Glen Kristiansen Professor and Chairman Institute of Pathology, University Hospital Bonn January 2016 WHO GU-Pathology
Tumours of the Prostate and Testis update on WHO classification, IHC and molecular Morphology Glen Kristiansen Professor and Chairman Institute of Pathology, University Hospital Bonn January 2016 WHO GU-Pathology
Diagnosis, pathology and prognosis including variant pathology
 PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
Liver Specialty Evening Conference. Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle
 Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE. Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT
 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
List of Available TMAs in the PRN
 TMA RPCI_BrainCa01 RPCI_BrCa03 RPCI_BrCa04 RPCI_BrCa05 RPCI_BrCa0 RPCI_BrCa07 RPCI_BrCa08 RPCI_BrCa15 RPCI_BrCa1 RPCI_BrCa17 RPCI_BrCa18 RPCI_BrCa19 RPCI_BrCa20 RPCI_BrCa21 RPCI_BrCa24 RPCI_BrCa25 RPCI_BrCa2
TMA RPCI_BrainCa01 RPCI_BrCa03 RPCI_BrCa04 RPCI_BrCa05 RPCI_BrCa0 RPCI_BrCa07 RPCI_BrCa08 RPCI_BrCa15 RPCI_BrCa1 RPCI_BrCa17 RPCI_BrCa18 RPCI_BrCa19 RPCI_BrCa20 RPCI_BrCa21 RPCI_BrCa24 RPCI_BrCa25 RPCI_BrCa2
The clinically challenging entity of liver metastasis from tumors of unknown primary
 The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Disclosure of Relevant Financial Relationships
 Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Immunohistochemistry in prostate pathology: Recent Advances
 Immunohistochemistry in prostate pathology: Recent Advances Jae Y. Ro, M.D., Ph.D. Weill Medical College of Cornell University, Methodist Hospital, and UT MD Anderson Cancer Center, Houston, TX Yonsei
Immunohistochemistry in prostate pathology: Recent Advances Jae Y. Ro, M.D., Ph.D. Weill Medical College of Cornell University, Methodist Hospital, and UT MD Anderson Cancer Center, Houston, TX Yonsei
INTRODUCTION TO PATHOLOGICAL TECHNIQUES. 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH)
") INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
Immunohistochemical Diagnosis of Renal Neoplasms. Luan D. Truong, MD; Steven S. Shen, MD, PhD
 Immunohistochemical Diagnosis of Renal Neoplasms Luan D. Truong, MD; Steven S. Shen, MD, PhD N Context. Histologic diagnosis of renal neoplasm is usually straightforward by routine light microscopy. However,
Immunohistochemical Diagnosis of Renal Neoplasms Luan D. Truong, MD; Steven S. Shen, MD, PhD N Context. Histologic diagnosis of renal neoplasm is usually straightforward by routine light microscopy. However,
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
CASE 4 21/07/2017. Ectopic Prostatic Tissue in Cervix. Female 31. LLETZ for borderline nuclear abnormalities
 Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, controls and EQA (part II)
") The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
Kidney, Bladder and Prostate Neoplasia. David Bingham MD
 Kidney, Bladder and Prostate Neoplasia David Bingham MD typical malignant cytology of bladder washings 1 benign 2 malignant typical malignant cytology of bladder washings b Bladder tumor Non invasive papillary
Kidney, Bladder and Prostate Neoplasia David Bingham MD typical malignant cytology of bladder washings 1 benign 2 malignant typical malignant cytology of bladder washings b Bladder tumor Non invasive papillary
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
FNA Cytology of Metastatic Malignancies of Unknown Primary Site
 FNA Cytology of Metastatic Malignancies of Unknown Primary Site Tarik M. Elsheikh Jan F. Silverman Pathologic Diagnosis of Metastasis Smaller specimens, less invasive techniques FNA cytology is highly
FNA Cytology of Metastatic Malignancies of Unknown Primary Site Tarik M. Elsheikh Jan F. Silverman Pathologic Diagnosis of Metastasis Smaller specimens, less invasive techniques FNA cytology is highly
Other Sites. Table 2 Continued. MPH Rules 11/8/07. NAACCR Webinar Series 1
 MPH s 11/8/07 Other s 1 Table 2 Continued Use this two-page table to select combination histology codes. Compare the terms in the diagnosis to the terms in Columns 1 and 2. If the terms match, code the
MPH s 11/8/07 Other s 1 Table 2 Continued Use this two-page table to select combination histology codes. Compare the terms in the diagnosis to the terms in Columns 1 and 2. If the terms match, code the
8 years later! Next Generation Sequencing. Pathogenic Findings: HNF1A c.864delinscc, p.g292rfs*25 (NM_ ) (VAF: 59%) HNF1A Loss
 (VAF: 59%) HNF1A Loss") 8 years later! Next Generation Sequencing Pathogenic Findings: HNF1A c.864delinscc, p.g292rfs*25 (NM_000545.6) (VAF: 59%) HNF1A Loss Interpretation HNF1A c.864delinscc, p.g292rfs*25 (NM_000545.6) This
8 years later! Next Generation Sequencing Pathogenic Findings: HNF1A c.864delinscc, p.g292rfs*25 (NM_000545.6) (VAF: 59%) HNF1A Loss Interpretation HNF1A c.864delinscc, p.g292rfs*25 (NM_000545.6) This
Testicular Tumors: What s New, True, Important Cristina Magi-Galluzzi, MD, PhD
 Testicular Tumors: What s New, True, Important Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology, Lerner College
Testicular Tumors: What s New, True, Important Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology, Lerner College
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseud
 GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
CODING TUMOUR MORPHOLOGY. Otto Visser
 CODING TUMOUR MORPHOLOGY Otto Visser INTRODUCTION The morphology describes the tissue of the tumour closest to normal tissue Well differentiated tumours are closest to normal Undifferentiated tumours show
CODING TUMOUR MORPHOLOGY Otto Visser INTRODUCTION The morphology describes the tissue of the tumour closest to normal tissue Well differentiated tumours are closest to normal Undifferentiated tumours show
Nordic Immunohistochemical Quality Control
 Nordic Immunohistochemical Quality Control Immunohistochemistry in the classifiation of neoplasias of the alimentary tract & External Quality Assurance of Immunohistochemistry for GI cancer markers Mogens
Nordic Immunohistochemical Quality Control Immunohistochemistry in the classifiation of neoplasias of the alimentary tract & External Quality Assurance of Immunohistochemistry for GI cancer markers Mogens
Unusual Variants of Bladder Cancer Cristina Magi-Galluzzi, MD, PhD
 Unusual Variants of Bladder Cancer Cristina Magi-Galluzzi, MD, PhD Director of Genitourinary Pathology, Professor of Pathology, Lerner College of Medicine Cleveland Clinic Objectives Update on variants
Unusual Variants of Bladder Cancer Cristina Magi-Galluzzi, MD, PhD Director of Genitourinary Pathology, Professor of Pathology, Lerner College of Medicine Cleveland Clinic Objectives Update on variants
Immunohistochemical classification of the unknown primary tumour (UPT) Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark") Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma
 Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Usefulness of GATA3 and p40 Immunostains in the Diagnosis of Metastatic Urothelial Carcinoma in Cytology Specimens
 Original Article Usefulness of GATA3 and p40 Immunostains in the Diagnosis of Metastatic Urothelial Carcinoma in Cytology Specimens Tamar C. Brandler, MD, MS 1 ; Mohamed S. Aziz, MD 1 ; Lisa M. Rosen,
Original Article Usefulness of GATA3 and p40 Immunostains in the Diagnosis of Metastatic Urothelial Carcinoma in Cytology Specimens Tamar C. Brandler, MD, MS 1 ; Mohamed S. Aziz, MD 1 ; Lisa M. Rosen,
2% of all malignancies Male predominance Patients usually more than 60 years old
 Benign Bladder Tumors Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma 90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
Benign Bladder Tumors Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma 90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
Single and Multiplex Immunohistochemistry
 Single and Multiplex Immunohistochemistry Steve Westra, BS Reagent Product Specialist Leica Biosystems IHC Theory Polyclonal vs Monoclonal Polyclonal reagents Detect a multitude of epitopes Batch to batch
Single and Multiplex Immunohistochemistry Steve Westra, BS Reagent Product Specialist Leica Biosystems IHC Theory Polyclonal vs Monoclonal Polyclonal reagents Detect a multitude of epitopes Batch to batch