Knee dislocation. Rare in children Physeal seperation > dislocation or ligament injury If dislocation occurs: Vascular compromise Compartment syndrome
|
|
|
- Barnard Anderson
- 5 years ago
- Views:
Transcription





1 인제대학교일산백병원 주석규



2 Knee dislocation Rare in children Physeal seperation > dislocation or ligament injury If dislocation occurs: Vascular compromise Compartment syndrome
3 Patellar dislocation Common in adolescent and teenager Typically Female Loose jointed Genu valgum with increased femoral anteversion Who are trying sports



4 Patellar dislocation Reduced before patient comes to the hospital P/E Hemarthrosis, tenderness along medial border of patella Lateral position of patella Fairbanks sign X-ray Loose fragment Lateral femoral condyle Medial edge of the patella 5-10% osteochondral fracture


5 Patellar dislocation F/13

6 Patellar dislocation F/13
7 Patellar dislocation Treatment 3-4wks of immobilization Early PT to strengthen vastus medialis Fracture of medial patella or lateral femoral condyle Acute arthrotomy Ligament repair Excision or fixation of the fracture Repair of the medial capsule and patellofemoral ligament
 A. Lateral retinacular release and medial imbrication. B.")
8 Patellar dislocation Recurrent dislocation 15-20% Due to faulty anatomy Increased quadriceps angle Femoral condyle hypoplasia Shallow femoral sulcus Atrophy of vastus medialis Lateral patellar tilt Lax joint Treatment Soft tissue realignment Semitenidnosus tenodesis to patella Tibial tubercle transfer (after physeal closure) A. Lateral retinacular release and medial imbrication. B. Semitendinosis tenodesis. C. Elmslie-Trillat procedure.




9 Patellar fractures Bipartite patella Located superolaterally 40% bilateral Fracture line may propagate through the synchondrosis difficult diagnosis Sleeve fracture Avulsion fracture of the lower pole With little or no bone Difficult to recognizeextensor lag Open reduction

10 Tibial eminance fracture 8 to 14 yrs old Bicycle injury and other sports activity 40%: meniscus, capsule or collateral ligaments or with osteochondral fracture

11 ACL insertion 10 to 14 mm behind the anterior border of the tibia Extends to the medial and lateral tibial eminence

12 Classification Meyer and McKeever(1959) Type I: Nondisplaced Type II: Anterior cortical displacement with intact posterior cortex Type III: completely displaced with no bone contact Type IV: comminuted Type I Type II Type III Type IV

13 Immobilization 6wks 20 degrees flexion or full extension Late displacement of type I does occur Unreduced displaced fracture Impingement Extension limitation Irreducible fracture Bowstringing or bucket-handle mechanism Anterior horn of the lateral meniscus is torn from its tibial attachment but remains attached to the fracture piece Interposition of Anterior horn of the medial meniscus, Anterior horn of the lateral meniscus Intermeniscal ligament


14 Suture or screw fixation Suture: small comminuted frgament Screws: larger than 15mm fragment Irritate the joint May require removal Complications LOM: impingement, arthrofibrosis Nonunion Maluniondebridement and notchplasty Quadriceps atrophy Growth arrest Ligament laxity: elongation of the ACL?

15 Tibial tubercle fracture Closure of the physis of the tubercle Girls: Boys: Injury Common in boys between 12 and 17 Eccentric contracture of the quadriceps
 Type III: Extends into the knee joint (subtype B: comminuted fragment) X-ray: better viewed with")
16 Watson-Jones, Ogden classification Type I: avulsion of a small fragment of the distal tubercle (subtype B: fragment seperated from metaphysis) Type II: involves the entire secondary ossification center, apex is at the level of the proximal tibial physis (subtype B: comminuted ossification center) Type III: Extends into the knee joint (subtype B: comminuted fragment) X-ray: better viewed with knee slight internal rotation

17 4-6wks of immobilization ORIF from type IB Complications Anterior tibial recurrent artery Physeal arrest
18 Proximal tibial physeal fracture More physeal seperation in distal femur than proximal tibia 1) MCL attached to tibial metaphysis and femoral epiphysis, protecting from valgus injury 2) Upper end of fibula acts as lateral buttress 3) Semimembranosus muscle inserts distal to the physis posteromedially 4) Tibial tubercle projects from the epiphysis over the metaphysis
19 Proximal tibial physeal fracture More physeal seperation in distal femur than proximal tibia 1) MCL attached to tibial metaphysis and femoral epiphysis, protecting from valgus injury 2) Upper end of fibula acts as lateral buttress 3) Semimembranosus muscle inserts distal to the physis posteromedially 4) Tibial tubercle projects from the epiphysis over the metaphysis
20 Proximal tibial physeal fracture More physeal seperation in distal femur than proximal tibia 1) MCL attached to tibial metaphysis and femoral epiphysis, protecting from valgus injury 2) Upper end of fibula acts as lateral buttress 3) Semimembranosus muscle inserts distal to the physis posteromedially 4) Tibial tubercle projects from the epiphysis over the metaphysis
 Upper end of fibula acts as lateral buttress 3) Semimembranosus muscle inserts distal to the physis posteromedially 4) Tibial tubercle projects from the epiphysis over the")
21 Proximal tibial physeal fracture More physeal seperation in distal femur than proximal tibia 1) MCL attached to tibial metaphysis and femoral epiphysis, protecting from valgus injury 2) Upper end of fibula acts as lateral buttress 3) Semimembranosus muscle inserts distal to the physis posteromedially 4) Tibial tubercle projects from the epiphysis over the metaphysis




22
")
23 Proximal tibial metaphyseal fracture Posterior tibial artery injury Post union valgus deformity Asymmetrical growth stimulation of the proximal tibial physis Asymmetrical growth stimulation of the medial proximal metaphysis Tibial physis stimulated more or longer than fibular physis Valgus at the time of fracture Soft tissue interposition(ex: pes anserinus) Physeal injury
24 7 post-traumatic tibia valga 11 mths to 6 yrs old Valgus appeared during fracture healing and after union Most rapid progression during 1 st year Overgrowth may accompany Clinical correction in 6/7 Conservative approach
25 32 proximal tibia fracture Avg age 7.1 yrs 28 post traumatic tibia valga(90.3%) Avg angulation 5.5 degrees 5.3mm overgrowth 11 patients more than 5 degrees angulation 6 partial and 3 complete remodeling
26 Diaphyseal fractures of tibia 15% of long bone fracture Avg age 8 yrs old Boys>girls With fibular fracture 30% Complete fracture by high energy Valgus shortening of distal fragment Without fibular fracture Rotational force Varus shortening Low energy injury A. Fractures involving the mid 1/3 of the tibia and fibula may shift into a valgus alignment due to the activity of the muscles in the anterior and the lateral compartments of the lower leg. B. Fracture of the mid tibia without fibular fracture tend to shift into varus d/t the force created by the anterior compartment musculature of the lower leg and the tethering effect of the intact fibula.


27 Isolated tibia fracture(m/7)



28 Isolated tibia fracture(m/7) Union with little callus
")
29 Isolated tibia fracture(m/7) 7months later
30 Acceptable reduction Varus valgus: 5 degrees Sagital deformity: 5 degrees Shortening: 1cm Rotation 0 Reduction correction: within 3 weeks Remodeling potential under 8 Varus 10 degrees Sagital 10 degrees Complete translation No remodeling of rotation


31 Better remodeling in Anterior, varus than posterior, valgus, deformity Overgrowth: 5 mm Surgery: Comminuted fracture Irreducible fracture Compartment syndrome Open fracture Multiple fracture Floating knee




32 Valgus tibia 1 yr 18 months
33 Valgus remodeling?
34 Stress fracture Osteoclastic breakdown>natural healing process #1 Military recruits, #2 young athletes Tibia m/c Endurance runnermetatarsal stress fracture Sports involving sudden stops(tennis, basketball, handballtibial stress fracture Heyworth and Green, Current Opinion in Pediatrics, 2008




35 Stress fracture Risk factors Female: x4 than male Late menarche: BMD increases after menarche and growth spurt Disordered eating: calcium, Vit D Threshold quantity of activity: 16hrs/week



36 16 years old girl Left leg pain for 2 months Dance practice 4 hrs/day Tenderness distal 1/3 Cortical thickening Activity modication recommended. But?
37 Fracture of distal tibia
38 Closure of distal tibial physis Physis closes at 15 for girls, 17 for boys Centermedialanterolateral Distal fibula closes 1 year later

39 Treatment CR & long leg cast Closed reduction Knee flexed Recreate force of injury: Plantar flexion, supination or adduction Longitudinal traction Bring foot around to neutral position Internal rotation Entrapped soft tissue: Remaining growth Gap





40
41 Ankle Fractures Pediatric ankle fracture by Poland 1) The growth plate forms a plane of weakness 2) Ligaments are stronger than bone 3) Certain injuries will affect growth Plus 1) Fracture rarely disturb talo-tibial relationship 2) From age 14 to 15 years onward, adult pattern of fracture emerges
42 Ankle Fractures Pediatric ankle fracture by Poland 1) The growth plate forms a plane of weakness 2) Ligaments are stronger than bone 3) Certain injuries will affect growth Plus 1) Fracture rarely disturb talo-tibial relationship 2) From age 14 to 15 years onward, adult pattern of fracture emerges

43 Classification and mechanism of injury Salter-Harris classification Lauge-Hansen classification Abduction, external rotation, extension S-H I or II Adduction S-H III Axial compression S-H V




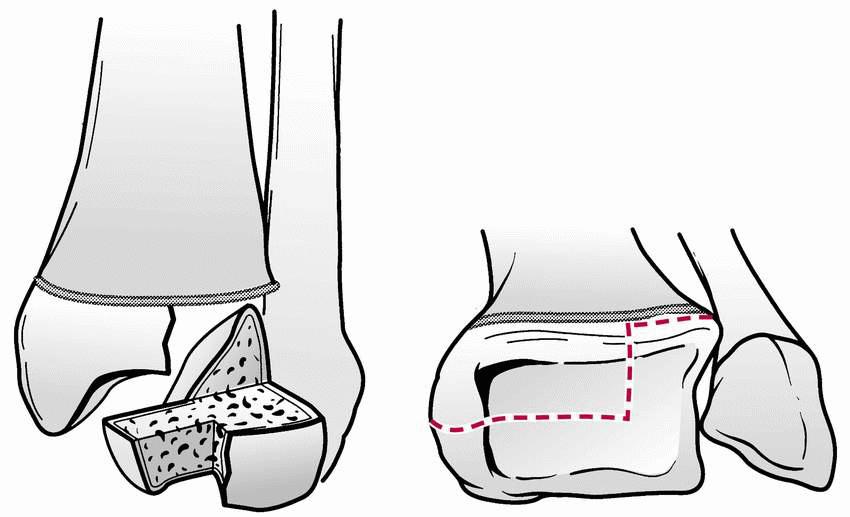
44 Tilleaux fracture 1 year before distal tibial physis closes Medial and central physis closed, anterolateral open External rotation force
45 Triplane fracture Sagital, transverse, coronal plane Along and through the physis Mostly d/t external rotation but sometimes internal rotation force Between 12 to 15, younger than Tilleaux fracture group Sports, scooter, skate, snowboard injury Fibula fracture 50%




46 X-ray AP plane: S-H III Lateral view: S-H II Axial CT: Merceds-Benz sign 2 fragment, 3fragment, 4 fragment fractures



47 4 fragment variant External rotation plus axial compression Metaphyseal comminution Extra articular variant
48 CR and cast: < 2 mm OR and IF: > 3 mm Open reduction: For articular restoration rather than to prevent growth arrest
49 Distal tibial physeal injury 45 % growth of tibia 4-6 mm / yr growth 6 to 12 months of monitor Harris growth line Growth arrest: Bone bridge resection Osteotomy Epiphyseodesis

50 Distal tibial physeal injury 50% growth of tibia 4-6 mm / yr growth 6 to 12 months of monitor Harris growth line Growth arrest: Bone bridge resection Osteotomy Epiphyseodesis
51 Distal tibial physeal injury 50% growth of tibia 4-6 mm / yr growth 6 to 12 months of monitor Harris gorwth line Growth arrest: Bone bridge resection Osteotomy Epiphyseodesis
52 Sesamoid bones of the foot

53 Fracture of talus Head, constricted neck, and body Fracture occurs in neck, body, medial and lateral process, osteochondral injuries m/c fracture: neck of the talus

54 Blood supply from Posterior tibial Dorsalis pedis Peroneal arteries
55 Forced dorsiflexion of the foot neck impinges against anteror lip of the tibia

56 Hawkins classification Hawkins I No displacement of fracture line and no incongruity of subtalar joint Hawkins II Associated with dislocation or subluxation of subtalar joint Hawkins III Talar neck fracture with dislocation of subtalar and ankle joints Hawkins IV- Associated disruption of talonavicular joint

57 X-ray: AP: 15 degrees pronation, tube 75 degrees Lateral and oblique 5 mm displacement and 5 degrees malalignment acceptable Hawkin s sign: may not appear in children!
 Thin wafer like")
 Deep, cup shaped Less symptomatic,")
58 Osteochondral fracture M/C in young adults but may occur under 10 Anterolateral(44%) Thin wafer like Usually symptomatic, associated with trauma Posteromedial(56%) Deep, cup shaped Less symptomatic, repetitive microtrauma
59 Fractures of the calcaneus Rare in children Better prognosis than adult Less intraarticular damage Occult fractures in toddlers Do well with conservative treatment
60 Lisfranc injuries Direct injury Less common Objects falling on foot and rupture of plantar ligament May associate with severe soft tissue damage Indirect injury More common Violent plantar flexion or abduction force or in combination (vertical loading in plantar flexion, heel to toe compression)


61
62 Fractures of metatarsal Most common fracture of the foot Good remodeling potential Proximal fracture Beware of Lisfranc injury

 Proximal diaphysis of the 5 th metatarsal Delayed union, nonunion Internal")
63 5th metatarsal base avulsion fracture Jones Fracture Inversion or adduction of the foot Peroneus brevis, abd digiti minimi quinti, lateral cord of plantar aponeuroisis Fractrure perpendicular to long axis of the shaft Ddx: Os peroneum, Os vesalianum(line parallel to long axis) Proximal diaphysis of the 5 th metatarsal Delayed union, nonunion Internal fixation

64
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
Lower Extremity Fracture Management. Fractures of the Hip. Lower Extremity Fractures. Vascular Anatomy. Lower Extremity Fractures in Children
 Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle.
 Radiographic Evaluation of the Ankle.") X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
Physeal Fractures and Growth Arrest
 Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Common Orthopaedic Injuries in Children
 Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Lower Extremity Alignment: Genu Varum / Valgum
 Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
No Disclosures. Topics. Pediatric ACL Tears
 Knee Injuries in Skeletally Immature Athletes No Disclosures Zachary Stinson, M.D. 2 Topics ACL Tears and Tibial Eminence Fractures Meniscus Injuries Discoid Meniscus Osteochondritis Dessicans Patellar
Knee Injuries in Skeletally Immature Athletes No Disclosures Zachary Stinson, M.D. 2 Topics ACL Tears and Tibial Eminence Fractures Meniscus Injuries Discoid Meniscus Osteochondritis Dessicans Patellar
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!!
 Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Pediatric Tibia Fractures Key Points. Christopher Iobst, MD
 Pediatric Tibia Fractures Key Points Christopher Iobst, MD Goals Bone to heal Return to full weight bearing Acceptable alignment rule of 10s 10 degrees of varus 8 degrees of valgus 12 degrees of procurvatum
Pediatric Tibia Fractures Key Points Christopher Iobst, MD Goals Bone to heal Return to full weight bearing Acceptable alignment rule of 10s 10 degrees of varus 8 degrees of valgus 12 degrees of procurvatum
Knee Injury Assessment
 Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Hip joint Type: Articulating bones:
 Ana (242 ) Hip joint Type: Synovial, ball & socket Articulating bones: Formed between head of femur and lunate surface of acetabulum of hip bone. Capsule: it is a strong fibrous sleeve connecting the articulating
Ana (242 ) Hip joint Type: Synovial, ball & socket Articulating bones: Formed between head of femur and lunate surface of acetabulum of hip bone. Capsule: it is a strong fibrous sleeve connecting the articulating
Peggers Super Summaries: Foot Injuries
 Lisfranc Injury ANATOMY Roman arch with recessed 2 nd MT base AP medial side of intermediate cuneiform to 2 nd MT base Oblique medial side of lateral cuneiform with 3 rd MT base and 4 th with medial boarder
Lisfranc Injury ANATOMY Roman arch with recessed 2 nd MT base AP medial side of intermediate cuneiform to 2 nd MT base Oblique medial side of lateral cuneiform with 3 rd MT base and 4 th with medial boarder
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University
 Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University Topics Fracture of the shaft of the femur Fractures around
Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University Topics Fracture of the shaft of the femur Fractures around
40 th Annual Symposium on Sports Medicine. Knee Injuries In The Pediatric Athlete. Disclosure
 40 th Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio Knee Injuries In The Pediatric Athlete Disclosure Dr. Travis Murray
40 th Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio Knee Injuries In The Pediatric Athlete Disclosure Dr. Travis Murray
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
The Knee. Prof. Oluwadiya Kehinde
 The Knee Prof. Oluwadiya Kehinde www.oluwadiya.sitesled.com The Knee: Introduction 3 bones: femur, tibia and patella 2 separate joints: tibiofemoral and patellofemoral. Function: i. Primarily a hinge joint,
The Knee Prof. Oluwadiya Kehinde www.oluwadiya.sitesled.com The Knee: Introduction 3 bones: femur, tibia and patella 2 separate joints: tibiofemoral and patellofemoral. Function: i. Primarily a hinge joint,
42 nd Annual Symposium on Sports Medicine. Knee Injuries In The Pediatric Athlete. Disclosure
 42 nd Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio January 23, 2015 Knee Injuries In The Pediatric Athlete Disclosure
42 nd Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio January 23, 2015 Knee Injuries In The Pediatric Athlete Disclosure
Talus Fractures: When and Why on Screws and Plates
 Talus Fractures: When and Why on Screws and Plates Frank A. Liporace, MD Associate Professor Director of Orthopaedic Research New York University / Hospital for Joint Diseases, NY, NY Director Orthopaedic
Talus Fractures: When and Why on Screws and Plates Frank A. Liporace, MD Associate Professor Director of Orthopaedic Research New York University / Hospital for Joint Diseases, NY, NY Director Orthopaedic
Radiographic Evaluation of Calcaneal Fractures. Kali Luker, PGY-1
 Radiographic Evaluation of Calcaneal Fractures Kali Luker, PGY-1 Anatomy Extraarticular Fractures Involve body, anterior process or tuberosity Treated with immobilization and NWB x 6 wks UNLESS Displaced
Radiographic Evaluation of Calcaneal Fractures Kali Luker, PGY-1 Anatomy Extraarticular Fractures Involve body, anterior process or tuberosity Treated with immobilization and NWB x 6 wks UNLESS Displaced
Knee Contusions and Stress Injuries. Laura W. Bancroft, M.D.
 Knee Contusions and Stress Injuries Laura W. Bancroft, M.D. Objectives Review 5 types of contusion patterns Pivot shift Dashboard Hyperextension Clip Lateral patellar dislocation Demonstrate various stress
Knee Contusions and Stress Injuries Laura W. Bancroft, M.D. Objectives Review 5 types of contusion patterns Pivot shift Dashboard Hyperextension Clip Lateral patellar dislocation Demonstrate various stress
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Outline. Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t
 Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
Apply this knowledge into proper management strategies and referrals
 1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
radiologymasterclass.co.uk
 http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA. Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009
 EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
ChiroCredit.com Presents Biomechanics: Focus on
 ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
Ankle Tendons in Athletes. Laura W. Bancroft, M.D.
 Ankle Tendons in Athletes Laura W. Bancroft, M.D. Outline Protocols Normal Anatomy Tendinopathy, partial and complete tears Posterior tibial, Flexor Hallucis Longus, Achilles, Peroneal and Anterior Tibial
Ankle Tendons in Athletes Laura W. Bancroft, M.D. Outline Protocols Normal Anatomy Tendinopathy, partial and complete tears Posterior tibial, Flexor Hallucis Longus, Achilles, Peroneal and Anterior Tibial
Joints of the Lower Limb II
 Joints of the Lower Limb II Lecture Objectives Describe the components of the knee and ankle joint. List the ligaments associated with these joints and their attachments. List the muscles acting on these
Joints of the Lower Limb II Lecture Objectives Describe the components of the knee and ankle joint. List the ligaments associated with these joints and their attachments. List the muscles acting on these
Lower Extremity Fractures in Children
 Lower Extremity Fractures in Children Stephanie M. Holmes, MD Department of Orthopaedic Surgery Pediatric Orthopaedic Division University of Utah School of Medicine Overview Hip injuries avulsion fractures,
Lower Extremity Fractures in Children Stephanie M. Holmes, MD Department of Orthopaedic Surgery Pediatric Orthopaedic Division University of Utah School of Medicine Overview Hip injuries avulsion fractures,
Anterior Cruciate Ligament Surgery
 Anatomy Anterior Cruciate Ligament Surgery Roger Ostrander, MD Andrews Institute Anatomy Anatomy Function Primary restraint to anterior tibial translation Secondary restraint to internal tibial rotation
Anatomy Anterior Cruciate Ligament Surgery Roger Ostrander, MD Andrews Institute Anatomy Anatomy Function Primary restraint to anterior tibial translation Secondary restraint to internal tibial rotation
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Upper Extremity Fractures
 Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
ACL Athletic Career. ACL Rupture - Warning Features Intensive pain Immediate swelling Locking Feel a Pop Dead leg Cannot continue to play
 FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
Fractures in the Immature Foot
 Fractures in the Immature Foot Kaye E. Wilkins, M.D. Clinical Professor Orthopaedics & Pediatrics University of Texas Health Science Center at San Antonio San Antonio, Texas (210) 692-1613 e-mail: drkwilkins@aol.com
Fractures in the Immature Foot Kaye E. Wilkins, M.D. Clinical Professor Orthopaedics & Pediatrics University of Texas Health Science Center at San Antonio San Antonio, Texas (210) 692-1613 e-mail: drkwilkins@aol.com
Patellofemoral Pathology
 Patellofemoral Pathology Matthew Murray, MD UT Health Science Center/UT Medicine Sports Medicine and Arthroscopic Surgery I have disclosed that I am a consultant for Biomet Orthopaedics. Anterior Knee
Patellofemoral Pathology Matthew Murray, MD UT Health Science Center/UT Medicine Sports Medicine and Arthroscopic Surgery I have disclosed that I am a consultant for Biomet Orthopaedics. Anterior Knee
MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium
 MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium Introduction Increasing sports injuries RTA and traumatic injuries
MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium Introduction Increasing sports injuries RTA and traumatic injuries
Imaging the Athlete s Knee. Peter Lowry, MD Musculoskeletal Radiology University of Colorado
 Imaging the Athlete s Knee Peter Lowry, MD Musculoskeletal Radiology University of Colorado None Disclosures Knee Imaging: Radiographs Can be performed weight-bearing or non-weight-bearing View options
Imaging the Athlete s Knee Peter Lowry, MD Musculoskeletal Radiology University of Colorado None Disclosures Knee Imaging: Radiographs Can be performed weight-bearing or non-weight-bearing View options
Will She Still Make the WNBA? Sports Injuries & Fractures
 Will She Still Make the WNBA? Sports Injuries & Fractures Aharon Z. Gladstein MD Pediatric Orthopaedic Surgery Pediatric Sports Medicine Sports Injuries Chronic (overuse) Acute Who can be treated in PCP
Will She Still Make the WNBA? Sports Injuries & Fractures Aharon Z. Gladstein MD Pediatric Orthopaedic Surgery Pediatric Sports Medicine Sports Injuries Chronic (overuse) Acute Who can be treated in PCP
BIOMECHANICS OF ANKLE FRACTURES
 BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
Fractures of the Hand in Children Which are simple? And Which have pitfalls??
 Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Doron Sher. 160 Belmore Rd, Randwick Burwood Rd, Concord. MBBS, MBiomedE, FRACS FAOrthA
 Doron Sher MBBS, MBiomedE, FRACS FAOrthA 160 Belmore Rd, Randwick 47 49 Burwood Rd, Concord www.kneedoctor.com.au www.orthosports.com.au Medial PatelloFemoral (MPFL) And AnteroLateral Ligament (ALL) Reconstruction
Doron Sher MBBS, MBiomedE, FRACS FAOrthA 160 Belmore Rd, Randwick 47 49 Burwood Rd, Concord www.kneedoctor.com.au www.orthosports.com.au Medial PatelloFemoral (MPFL) And AnteroLateral Ligament (ALL) Reconstruction
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
Overview Ligament Injuries. Anatomy. Epidemiology Very commonly injured joint. ACL Injury 20/06/2016. Meniscus Tears. Patellofemoral Problems
 Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Multiapical Deformities p. 97 Osteotomy Concepts and Frontal Plane Realignment p. 99 Angulation Correction Axis (ACA) p. 99 Bisector Lines p.
 p. 99 Bisector Lines p.") Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Knee Joint Assessment and General View
 Knee Joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The knee is the largest
Knee Joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The knee is the largest
11/5/14. I will try to make this painless. Great, a Fracture, Now What? Objectives. Basics for Fracture Workup. Basics for Fracture Workup
 Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
Running Injuries in Children and Adolescents
 Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
 17.2 A-P Lower Leg Measure: A-P at mid-lower leg Protection: Apron draped over pelvis SID: 40 Table top No Tube Angle Film: 7 x17 I.D. down or diagonal 14 x 17 www.fisiokinesiterapia.biz A-P Lower Leg
17.2 A-P Lower Leg Measure: A-P at mid-lower leg Protection: Apron draped over pelvis SID: 40 Table top No Tube Angle Film: 7 x17 I.D. down or diagonal 14 x 17 www.fisiokinesiterapia.biz A-P Lower Leg
Ankle Pain After a Sprain.
 Ankle Pain After a Sprain www.fisiokinesiterapia.biz Anterior Drawer Stress Test Talar Tilt Talar Tilt (CFL) Difficult to isolate from subtalar ROM Slight plantar flexion (dorsi = relative subtalar isolation)
Ankle Pain After a Sprain www.fisiokinesiterapia.biz Anterior Drawer Stress Test Talar Tilt Talar Tilt (CFL) Difficult to isolate from subtalar ROM Slight plantar flexion (dorsi = relative subtalar isolation)
ACL AND PCL INJURIES OF THE KNEE JOINT
 ACL AND PCL INJURIES OF THE KNEE JOINT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery,
ACL AND PCL INJURIES OF THE KNEE JOINT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery,
CASE ONE CASE ONE. RADIAL HEAD FRACTURE Mason Classification. RADIAL HEAD FRACTURE Mechanism of Injury. RADIAL HEAD FRACTURE Imaging
 CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
Copyright 2012 by The McGraw-Hill Companies, Inc. All rights reserved. McGraw-Hill/Irwin
 CHAPTER 8: THE LOWER EXTREMITY: KNEE, ANKLE, AND FOOT KINESIOLOGY Scientific Basis of Human Motion, 12 th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D., ATC Humboldt State
CHAPTER 8: THE LOWER EXTREMITY: KNEE, ANKLE, AND FOOT KINESIOLOGY Scientific Basis of Human Motion, 12 th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D., ATC Humboldt State
Patella Instability 1 st Time Dislocation
 Patella Instability 1 st Time Dislocation American Medical Society for Sports Medicine April 6, 2014 Beth E. Shubin Stein, MD Sports Medicine & Shoulder Surgery Hospital for Special Surgery Beth E. Shubin
Patella Instability 1 st Time Dislocation American Medical Society for Sports Medicine April 6, 2014 Beth E. Shubin Stein, MD Sports Medicine & Shoulder Surgery Hospital for Special Surgery Beth E. Shubin
Patellofemoral Instability Jacqueline Munch, MD April 23, 2016
 Patellofemoral Instability Jacqueline Munch, MD April 23, 2016 With many thanks to Beth Shubin Stein, MD What is the Problem??? THIS IS THE PROBLEM Patella Stability Factors contributing to stability Articular
Patellofemoral Instability Jacqueline Munch, MD April 23, 2016 With many thanks to Beth Shubin Stein, MD What is the Problem??? THIS IS THE PROBLEM Patella Stability Factors contributing to stability Articular
11/4/2018 SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING SPEAKER DISCLOSURES
 SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING Charles S. Resnik, M.D. Professor of Radiology University of Maryland School of Medicine Upon completion of this presentation, participants will be better able
SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING Charles S. Resnik, M.D. Professor of Radiology University of Maryland School of Medicine Upon completion of this presentation, participants will be better able
DEPARTMENT OF TRAUMATOLOGY AND HAND SURGERY INSTITUTE OF MUSCULOSKELETAL SURGERY ANKLE AND FOOT INJURIES
 DEPARTMENT OF TRAUMATOLOGY AND HAND SURGERY INSTITUTE OF MUSCULOSKELETAL SURGERY ANKLE AND FOOT INJURIES Presenter: Dr George Ayerh ENGLISH PROGRAM LECTURES EN_11/A - 2018 TOPICS I. Part: Ankle & Foot
DEPARTMENT OF TRAUMATOLOGY AND HAND SURGERY INSTITUTE OF MUSCULOSKELETAL SURGERY ANKLE AND FOOT INJURIES Presenter: Dr George Ayerh ENGLISH PROGRAM LECTURES EN_11/A - 2018 TOPICS I. Part: Ankle & Foot
Other Upper Extremity Trauma. Inje University Sanggye Paik Hospital Yong-Woon Shin
 Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Revolution. Unicompartmental Knee System
 Revolution Unicompartmental Knee System While Total Knee Arthroplasty (TKA) is one of the most predictable procedures in orthopedic surgery, many patients undergoing TKA are in fact excellent candidates
Revolution Unicompartmental Knee System While Total Knee Arthroplasty (TKA) is one of the most predictable procedures in orthopedic surgery, many patients undergoing TKA are in fact excellent candidates
Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science.
 IN THE NAME OF GOD Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science. Devastating injury resulting from : high-energy usually from MVC or fall from height commonly a dashboard
IN THE NAME OF GOD Mohammad Ayati,M.D Department of Orthopaedics, Yazd University of Medical Science. Devastating injury resulting from : high-energy usually from MVC or fall from height commonly a dashboard
7/20/14. Patella Instability. Alignment. PF contact areas. Tissue Restraints. Pain. Acute Blunt force trauma Disorders of the Patellafemoral Joint
 Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
Differential Diagnosis
 Case 31yo M who sustained an injury to L knee while playing Basketball approximately 2 weeks ago. He describes pivoting and hyperextending his knee, which swelled over the next few days. He now presents
Case 31yo M who sustained an injury to L knee while playing Basketball approximately 2 weeks ago. He describes pivoting and hyperextending his knee, which swelled over the next few days. He now presents
Traumatic Injuries to the Foot and Ankle
 Traumatic Injuries to the Foot and Ankle Dr. Joseph N. Daniel Clinical Associate Professor of Orthopaedic Surgery Foot and Ankle Service, The Rothman Institute Thomas Jefferson University Hospital Philadelphia,
Traumatic Injuries to the Foot and Ankle Dr. Joseph N. Daniel Clinical Associate Professor of Orthopaedic Surgery Foot and Ankle Service, The Rothman Institute Thomas Jefferson University Hospital Philadelphia,
Lower Extremity Dislocations: Management and Triage on the Field
 Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
FIBULAR & SYNDESMOSIS MALUNIONS
 FIBULAR & SYNDESMOSIS MALUNIONS MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MORTISE INHERENTLY UNSTABLE LATERAL MALLEOLUS ACTS AS BUTTRESS / POST RESIST LATERAL TRANSLATION OF TALUS
FIBULAR & SYNDESMOSIS MALUNIONS MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MORTISE INHERENTLY UNSTABLE LATERAL MALLEOLUS ACTS AS BUTTRESS / POST RESIST LATERAL TRANSLATION OF TALUS
Foot Injuries. Dr R B Kalia
 Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
Prevention and Treatment of Injuries. Anatomy. Anatomy. Tibia: the second longest bone in the body
 Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
Management of Chronic Lateral Ligament Instability
 Management of Chronic Lateral Ligament Instability Bony Anatomy Curved trochlear surface of talus produces a cone-shaped articulation whose apex is directed medially; thus the fan-shaped deltoid is all
Management of Chronic Lateral Ligament Instability Bony Anatomy Curved trochlear surface of talus produces a cone-shaped articulation whose apex is directed medially; thus the fan-shaped deltoid is all
UNUSUAL ACL CASE: Tibial Eminence Fracture in a Female Collegiate Basketball Player
 UNUSUAL ACL CASE: Tibial Eminence Fracture in a Female Collegiate Basketball Player Cheri Drysdale, MEd,, ATC Margot Putukian,, MD Jeffery Bechler,, MD Princeton University How many of you have done an
UNUSUAL ACL CASE: Tibial Eminence Fracture in a Female Collegiate Basketball Player Cheri Drysdale, MEd,, ATC Margot Putukian,, MD Jeffery Bechler,, MD Princeton University How many of you have done an
OPERATIVE TREATMENT OF THE INTERCONDYLAR FRACTURE OF THE FEMUR
 OPERATIVE TREATMENT OF THE INTERCONDYLAR FRACTURE OF THE FEMUR S G Chee, K S Lam, B K Tay, N Balachandran SYNOPSIS Operative treatment of 28 intercondylar fractures of femur were done from 98 to 985. The
OPERATIVE TREATMENT OF THE INTERCONDYLAR FRACTURE OF THE FEMUR S G Chee, K S Lam, B K Tay, N Balachandran SYNOPSIS Operative treatment of 28 intercondylar fractures of femur were done from 98 to 985. The
W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco
 Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
17/10/2017. Foot and Ankle
 17/10/2017 Alicia M. Yochum RN, DC, DACBR, RMSK Foot and Ankle Plantar Fasciitis Hallux Valgus Deformity Achilles Tendinosis Posterior Tibialis Tendon tendinopathy Stress Fracture Ligamentous tearing Turf
17/10/2017 Alicia M. Yochum RN, DC, DACBR, RMSK Foot and Ankle Plantar Fasciitis Hallux Valgus Deformity Achilles Tendinosis Posterior Tibialis Tendon tendinopathy Stress Fracture Ligamentous tearing Turf
Childhood Fractures. Incomplete fractures more common. Ligaments stronger than bone. Tendons stronger than bone. Fractures may be pathologic
 Childhood Fractures Incomplete fractures more common Plastic bowing Torus / Buckle Greenstick Ligaments stronger than bone Fracture patterns different Physeal injury, not dislocation Tendons stronger than
Childhood Fractures Incomplete fractures more common Plastic bowing Torus / Buckle Greenstick Ligaments stronger than bone Fracture patterns different Physeal injury, not dislocation Tendons stronger than
PRONATION-ABDUCTION FRACTURES
 C H A P T E R 1 2 PRONATION-ABDUCTION FRACTURES George S. Gumann, DPM (The opinions of the author should not be considered as reflecting official policy of the US Army Medical Department.) Pronation-abduction
C H A P T E R 1 2 PRONATION-ABDUCTION FRACTURES George S. Gumann, DPM (The opinions of the author should not be considered as reflecting official policy of the US Army Medical Department.) Pronation-abduction
Ankle Sprains and Their Imitators
 Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Arthritic history is similar to that of the hip. Add history of give way and locking, swelling
 KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes
 Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
PEDIATRIC OVERUSE INJURIES. Nick Monson, DO Assistant Professor University of Utah Orthopedic Center U of U Sports Medicine Symposium
 PEDIATRIC OVERUSE INJURIES Nick Monson, DO Assistant Professor University of Utah Orthopedic Center U of U Sports Medicine Symposium MINI-ME Little adults Different injury patterns Ligaments > bones Changing
PEDIATRIC OVERUSE INJURIES Nick Monson, DO Assistant Professor University of Utah Orthopedic Center U of U Sports Medicine Symposium MINI-ME Little adults Different injury patterns Ligaments > bones Changing
Additions: lumbar spine/spondy. spondy. panners? Elbow dislocation?
 Additions: lumbar spine/spondy spondy panners? Elbow dislocation? 16 y.o.. female swimmer has had right shoulder pain for the past 6 months. Ultrasound treatment and rest have failed to provide relief.
Additions: lumbar spine/spondy spondy panners? Elbow dislocation? 16 y.o.. female swimmer has had right shoulder pain for the past 6 months. Ultrasound treatment and rest have failed to provide relief.
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes
 Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Disclosures. Syndesmosis Injury. Syndesmosis Ligaments. Objectives. Mark M. Casillas, M.D.
 Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Patellofemoral Instability
 Disclaimer This movie is an educational resource only and should not be used to manage Patellofemoral Instability. All decisions about the management of Patellofemoral Instability must be made in conjunction
Disclaimer This movie is an educational resource only and should not be used to manage Patellofemoral Instability. All decisions about the management of Patellofemoral Instability must be made in conjunction
Chapter XIX.1. Fractures May 2002
 Case Based Pediatrics For Medical Students and Residents Department of Pediatrics, University of Hawaii John A. Burns School of Medicine Chapter XIX.1. Fractures May 2002 Annemarie Uliasz The skeletal
Case Based Pediatrics For Medical Students and Residents Department of Pediatrics, University of Hawaii John A. Burns School of Medicine Chapter XIX.1. Fractures May 2002 Annemarie Uliasz The skeletal
Knee Joint Anatomy 101
 Knee Joint Anatomy 101 Bone Basics There are three bones at the knee joint femur, tibia and patella commonly referred to as the thighbone, shinbone and kneecap. The fibula is not typically associated with
Knee Joint Anatomy 101 Bone Basics There are three bones at the knee joint femur, tibia and patella commonly referred to as the thighbone, shinbone and kneecap. The fibula is not typically associated with
Fractures of Lower extremity
 www.fisiokinesiterapia.biz Fractures of Lower extremity FRACTURES OF FEMORAL NECK Anatomy Neck-Shaft Angle: In the anteroposterior roentgenogram, it is the angle between the long axis of the femoral neck
www.fisiokinesiterapia.biz Fractures of Lower extremity FRACTURES OF FEMORAL NECK Anatomy Neck-Shaft Angle: In the anteroposterior roentgenogram, it is the angle between the long axis of the femoral neck
BASELINE QUESTIONNAIRE (SURGEON)
") SECTION A: STUDY INFORMATION Subject ID: - - Study Visit: Baseline Site Number: Date: / / Surgeon ID: SECTION B: INITIAL SURGEON HISTORY B1. Previous Knee Surgery: Yes No Not recorded B2. Number of Previous
SECTION A: STUDY INFORMATION Subject ID: - - Study Visit: Baseline Site Number: Date: / / Surgeon ID: SECTION B: INITIAL SURGEON HISTORY B1. Previous Knee Surgery: Yes No Not recorded B2. Number of Previous
Computed Tomographic Imaging of Foot and Ankle trauma
 Computed Tomographic Imaging of Foot and Ankle trauma Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of Medicine San Diego, California CT of Foot and Ankle Trauma
Computed Tomographic Imaging of Foot and Ankle trauma Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of Medicine San Diego, California CT of Foot and Ankle Trauma
Recurrent Fifth Metatarsal Fractures. Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California
 Recurrent Fifth Metatarsal Fractures Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California General 5th MT fracture fairly common Mechanism: Hindfoot
Recurrent Fifth Metatarsal Fractures Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California General 5th MT fracture fairly common Mechanism: Hindfoot
Peggers Super Summaries: PFJ
 Patellofemoral Joint: ANATOMY: Largest sesamoid ossifying at 3-5 years of age Multiple foci having a sec ossification centre SUPEROLATERAL Helps increase moment arm PATELLOFEMORAL OA Incidence 10% of knee
Patellofemoral Joint: ANATOMY: Largest sesamoid ossifying at 3-5 years of age Multiple foci having a sec ossification centre SUPEROLATERAL Helps increase moment arm PATELLOFEMORAL OA Incidence 10% of knee
Financial Disclosure. Turf Toe
 Seth O Brien, CP, LP Financial Disclosure Mr. Seth O'Brien has no relevant financial relationships with commercial interests to disclose. Turf Toe Common in athletes playing on firm, artificial turf Forceful
Seth O Brien, CP, LP Financial Disclosure Mr. Seth O'Brien has no relevant financial relationships with commercial interests to disclose. Turf Toe Common in athletes playing on firm, artificial turf Forceful