PATHOPHYSIOLOGY OF HYPERTENSION. Samuel Makar. Prof of Pediatrics and Pediatric Nephrology, Cairo University
|
|
|
- Avice Foster
- 5 years ago
- Views:
Transcription
1 PATHOPHYSIOLOGY OF HYPERTENSION Samuel Makar Prof of Pediatrics and Pediatric Nephrology, Cairo University
2 SCOPE Introduction Definition BP Measuring Types Pathophysiology Overview Pathophysiology of Specific HTN Diseases
3 INTRODUCTION There is increasing evidence that HTN has its antecedents during childhood and that atherosclerosis is already present in adolescents. Thus, early detection and intervention are crucial. The prevalence of primary HTN is increasing among school children and adolescents due to an epidemic of obesity. Younger children are more likely to have secondary HTN, The definition of HTN as well as normative values of blood pressure (BP) should be well known to clinicians in order to identify HTN
4 SCOPE Introduction Definition BP Measuring Types Pathophysiology Overview Pathophysiology of Specific HTN Diseases
5 HTN DEFINITION Definition of Pediatric HTN: Average SBP and/or DBP 95th percentile - gender, age, and height -on 3 or more separate occasions. Pre-HTN : BP levels 90th percentile but < 95th percentile is termed prehypertension.
6
7 BP MEASURING Casual Blood Pressure Ambulatory BP monitoring (ABPM) Home BP monitoring (HBPM)
8 AMBULATORY BP MONITORING (ABPM) Provides multiple readings over time enabling computation of the mean, daytime, and nighttime ambulatory BP (ABP) by measuring BP during regular activities and BP variability More reliable and reproducible than casual BP Detects white coat effect (high casual BP than 24-h or daytime ABP) or reversed white coat effect (low casual BP than 24-h or daytime ABP) ABPM correlates better with target organ damage than casual BP
9 HOME BP Self measurement of BP has the following advantages: 1. Distinguishing sustained HTN from white coat HTN(WCH) 2. Detection of masked HTN 3. Assessing response to medication, 4. Improving patient adherence to treatment 5. Reducing costs by avoiding ABPM or drug therapy. Midori Awazu, Pedatric Nephrology Textbook 2016
10 IV Diretriz Brasileira de Hipertensão Arterial. Arq Bras Cardiol 2004
11 IV Guideline for Ambulatory Blood Pressure Monitoring, Arq. Bras. Cardiol, 2005
12 TYPES OF HTN According to the cause: Primary HTN Secondary HTN According to the setting White coat HTN Reversed white coat HTN Persistent HTN

 Adults : in the office (equal to or higher than 140/90 mmhg) and by 24-hour")
13 WHITE COAT HTN (WCH) In Children : BP measured in a physician s office >95th percentile whereas average BP being <90th percentile outside of a clinical setting. (National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents, Pediatrics, 2004) Adults : in the office (equal to or higher than 140/90 mmhg) and by 24-hour ABPM (lower than 130/80 mmhg) or by HBPM (lower than 135/85 mmhg)
14 WHITE COAT HTN (WCH) In WCH casual BP is high, while the BP during ABPM is normal WCH is considered relevant when the difference is higher than 20 mmhg and 10 mmhg for systolic pressure and diastolic pressure, respectively Myers MG et al,am J Hypertens 1999
15 REVERSE WHITE COAT HYPERTENSION (MASKED HTN) Reverse WCH or WC normotension or Masked HTN (MA) MH, a high Ambulatory BP in the presence of normal office BP Recognized as a risk factor for cardiovascular complications in the adults Pickering TG et al, Hypertension 2002 High prevalence of MH in renal transplant, CKD, obesity, sicklecell disease, repaired coarctation of aorta, obstructive sleep apnea, a parental history of HTN, increased BMI, and prehypertension Lurbe E et al, Hypertension 2005
16 IV Guideline for Ambulatory Blood Pressure Monitoring, Arq. Bras. Cardiol, 2005
17 SCOPE Introduction Definition BP Measuring Types Pathophysiology Overview Pathophysiology of Specific HTN Diseases
 x Systemic")


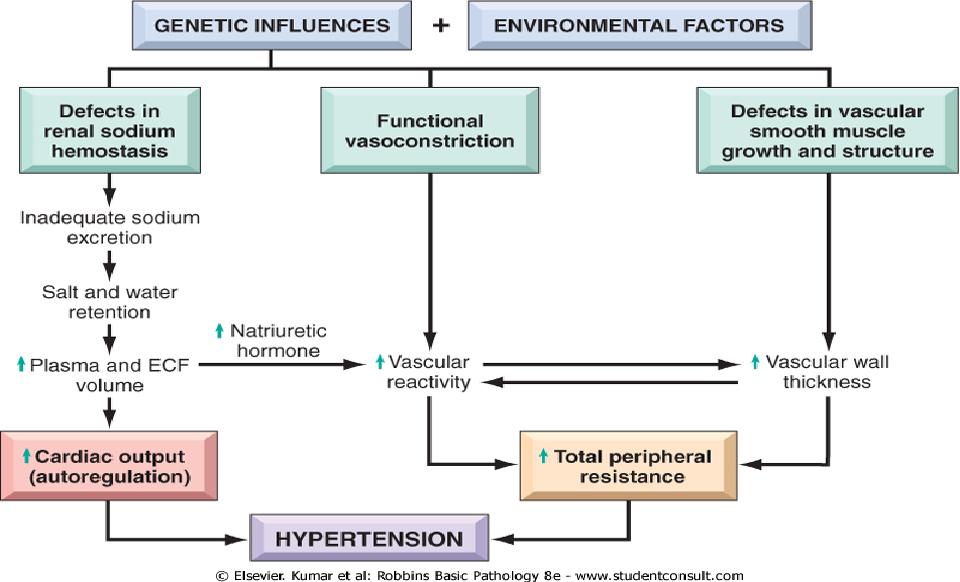
18 Pathophysiology Overview Equals: Cardiac output ( CO) x Systemic vascular resistance (SVR) SV HR Preload SympNS Force Exerted by circulating blood on artery walls Remodeling Rarefaction Stiffness
19 IMPORTANT KEY-PLAYERS IN PATHOPHYSIOLOGY OF HTN Systemic Vascular Resistance SVR RAAS Other Important Molecules
20 SYSTEMIC VASCULAR RESISTANCE (SVR) SVR mainly a function of small, peripheral arterioles Cross-sectional area of a vessel decreases, resistance to flow increases Remodeling : Thickening of the media is the earliest structural change due to matrix deposition, smooth muscle cell hypertrophy and hyperplasia creating smaller lumen Rarefaction : Finally, there may be resorption and loss of blood vessels in the periphery Stiffness: In larger vessels, the content of elastin and collagen in the media increases, and the number of smooth muscle cells decreases leading to a loss of elasticity
21 HE RENIN ANGIOTENSIN ALDOSTERONE SYSTEM (RAAS) Major stimuli for secretion of Renin: 1. Glomerular underperfusion 2. Reduced sodium intake 3. Sympathetic Nervous System activity. Renin cleaves hepatic-derived angiotensinogen to form angiotensin I (ANG-I) ACE in the lungs transforms it to angiotensin II (ANG-II). ACE also degrades bradykinin, a potent vasodilator, into inactive metabolites. ANG-II is a potent vasoconstrictor and thus directly increases BP. It also stimulates the release of aldosterone from the zona glomerulosa of the adrenal gland, which results in a further rise in BP from aldosterone-mediated sodium and water retention..
22 Midori Awazu, Pedatric Nephrology Textbook 2016

23
24 Midori Awazu, Pedatric Nephrology Textbook 2016
25 The functions of Ang-(1 9) are not completely understood, but Ang- (1 7) has vasodilatory and renoprotective effects Reduced ACE2 levels are thought to contribute to the pathogenesis of primary HTN via impaired degradation of ANG-II and reduced formation of vasodilator by-products at the level of the renal endothelium. Stergiou GS et al, Am J Hypertens. 2008
26 NB: Primary HTN is showing more and more to be NOT Primary HTN: 1. ACE 2 Mutation (reduced level of AT1-7)

27 Midori Awazu, Pedatric Nephrology Textbook 2016
28 ATRIAL NATRIURETIC PEPTIDE (ANP) Family of natriuretic peptides including B-type (BNP) and the C- type (CNP) natriuretic peptides with similar functions ANP has potent diuretic, Natriuretic ( by inhibiting tubular sodium reabsorption and renin and aldosterone biosynthesis ) Vasorelaxant effects. In the kidney ANP increases glomerular filtration rate (GFR) through vasodilatation of the afferent arteriole and vasoconstriction of the efferent arteriole. Beltowski J et al, Clin Res. 2002
29 ATRIAL NATRIURETIC PEPTIDE (ANP) Mutations in the ANP gene appear to be associated with the development of HTN in humans There is also evidence that ANP gene polymorphisms may affect the development of hypertensive sequelae such as left ventricular hypertrophy. Xue H et al Clin Sci (Lond). 2008
30 NB: Primary HTN is showing more and more to be NOT Primary HTN: 1. ACE 2 Mutation (reduced level of AT1-7) 2. ANP Polymorphism
31 RENALASE Renalase is a protein composed of 342 amino is recently discovered as a new renal hormone Renalase degrades circulating catecholamines (primarily epinephrine) via a mechanism different than monoamine oxidase Desir G. Pediatr Nephrol 2012

32
33 Renalase knockout mice are hypertensive and have evidence of increased sympathetic tone, suggesting renalase may modulate SNS activity Recombinant renalase has been developed and appears to be a potent antihypertensive agent in experimental models. Desir G. Pediatr Nephrol 2012
34 NB: Primary HTN is showing more and more to be NOT Primary HTN: 1. ACE 2 Mutation (reduced level of AT1-7) 2. ANP Polymorphism 3. Renalase activity
35 SCOPE Introduction Definition BP Measuring Types Pathophysiology Overview Pathophysiology of Specific HTN Diseases
36 PATHOPHYSIOLOGY OF SPECIFIC HTN DISEASES Primary HTN Secondary HTN
37 SECONDARY HTN A) Mendelian Forms of Hypertension (single-gene mutations ) Most of the mutations found to date affect renal sodium handling. These disorders lead to 3 groups of diseases: 1. Aberrant distal tubular sodium reabsorption and volume expansion due to hyperaldosteronism (Aldosterone is increased) 2. Defects in steroid biosynthetic enzymes (causing increased mineralocorticoid activity) 3. Activation of sodium channels or transporters (depressed Aldosterone)
38 SECONDARY HTN A) Mendelian Forms of Hypertension (single-gene mutations ) Most of the mutations found to date affect renal sodium handling. These disorders lead to 3 groups of diseases: 1. Aberrant distal tubular sodium reabsorption and volume expansion due to hyperaldosteronism (Aldosterone is increased) 2. Defects in steroid biosynthetic enzymes (causing increased mineralocorticoid activity) 3. Activation of sodium channels or transporters (depressed Aldosterone)
39 GLUCOCORTICOID-REMEDIABLE ALDOSTERONISM (GRA) FAMILIAL HYPERALDOSTERONISM TYPE 1 (FH1) (FH-I) is AD Early onset of HTN with normal or elevated aldosterone levels despite suppressed plasma renin activity Lifton RP. Proc Natl Acad Sci U S A Caused by a chimeric gene that results from unequal crossingover between the aldosterone synthase (CYP11B2) gene and the 11β-hydroxylase

40

41 The resulting chimeric gene (CYP11B1/CYP11B2) is expressed in the adrenal fasciculata and encodes a protein product with aldosterone synthase enzymatic activity whose expression is regulated by ACTH. Consequently, aldosterone synthase activity is ectopically expressed in the adrenal fasciculata under control of ACTH rather than by ANG-II or potassium.aldosterone secretion becomes linked to cortisol secretion, and maintenance of normal cortisol HTN is suppressed by Dexamethazone admmistration

42
43 ACTH Cortisol ACTH Aldoster. Dexamethazone Familial Hyperalsdosteronism I (GRA)
44 FAMILIAL HYPERALDOSTERONISM TYPE II (NON-GRA) Familial hyperaldosteronism type II (FH-II) Similar to GRA (FH-I), with excess production of mineralocorticoids, but is not suppressed by dexamethasone The molecular basis of the disorder remains to be determined.
45 FAMILIAL HYPERALDOSTERONISM TYPE III (NON-GRA) Familial hyperaldosteronism type III (FH-III) recently identified Mutations in the potassium channel KCNJ5 This results in depolarization of the glomerulosa cells, leading to increased calcium entry and aldosterone production. Massive adrenal hyperplasia with refractory HTN Geller DS, J Clin Endocrinol Metab.2008


46 KCNJ5 Aldoster. Familial Hyperalsdosteronism II and III (Non- GRA)
47 FIRST GROUP : FAMILIAL HYPERALDOSTERONISM Early onset HTN, normal or high Aldosterone FH -I..Chimeric gene GRA FH II excess production..not GRA FH-III excess production..not GRA
48 SECONDARY HTN A) Mendelian Forms of Hypertension (single-gene mutations ) Most of the mutations found to date affect renal sodium handling. These disorders lead to 3 groups of diseases: 1. Aberrant distal tubular sodium reabsorption and volume expansion due to hyperaldosteronism (Aldosterone is increased) 2. Defects in steroid biosynthetic enzymes (causing increased mineralocorticoid activity) 3. Activation of sodium channels or transporters (depressed Aldosterone)
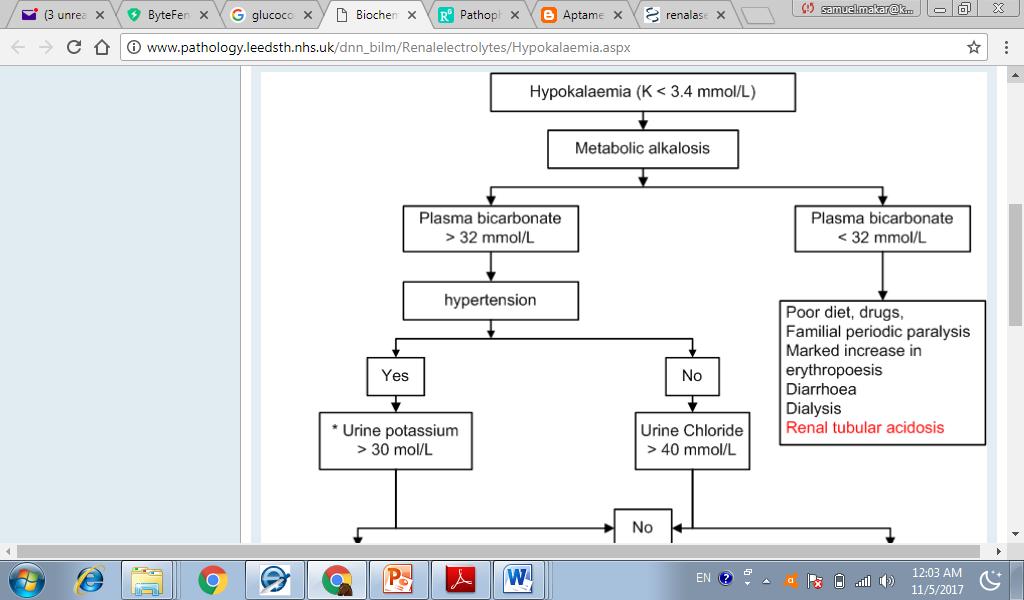
49 THE SYNDROME OF APPARENT MINERALOCORTICOID EXCESS (AME) AR Early-onset HTN with hypokalemia and metabolic alkalosis Accompanied by suppressed plasma renin activity And the virtual absence of circulating aldosterone.
50 THE SYNDROME OF APPARENT MINERALOCORTICOID EXCESS (AME) Steroids other than aldosterone activate the mineralocorticoid receptor (MR). i.e.apparent excess of MC action Cortisol activates MR with potency similar to aldosterone. Cortisol, normally, is transformed to Cortisone by 11-hydroxysteroid dehydrogenase (11HSD) enzyme Mutation in the gene encoding the renal i11-hydroxysteroid dehydrogenase (11HSD), results in impaired conversion of cortisol to cortisone. In AME, the absence of this enzyme allows cortisol to activate the MR, resulting in HTN mediated by increased sodium retention.
51 AME Aldosterone Cortisol 3BHSD2 Mineralocorticoid Receptor MR Cortisol 3BHSD2 Cortisone Epithelial Na channel ENaC Cortisone


52
53 OTHER STEROIDS CAUSING HTN Congenital adrenal hyperplasia results from two known defects: β-hydroxylase α-hydroxylase
54 SECONDARY HTN A) Mendelian Forms of Hypertension (single-gene mutations ) Most of the mutations found to date affect renal sodium handling. These disorders lead to 3 groups of diseases: 1. Aberrant distal tubular sodium reabsorption and volume expansion due to hyperaldosteronism (Aldosterone is increased) 2. Defects in steroid biosynthetic enzymes (causing increased mineralocorticoid activity) 3. Activation of sodium channels or transporters (depressed Aldosterone)
55 LIDDLE S SYNDROME AD disorder Gain mutations in the epithelial Na channel (ENaC) (Amiloride sensitive ) in the collecting ducts, which are responsible for elevated renal sodium reabsorption in Liddle s syndrome Severe HTN, metabolic alkalosis, and hypokalemia Low renin Low aldosterone. Unresponsive to Aldosterone antagonist (aldactone) but responsive to amiloride and triametrene
56
57 Liddle s Syndrome Aldosterone Aldactone Mineralocorticoid Receptor MR Epithelial Na channel ENaC(Amiloride sensitive) Amiloride triametrene Na reabsorption
58 LIDDLE S SYNDROME AND PSEUDOHYPOALDOSTERONISM TYPE I In Liddle's syndrome, gain-of-function mutations in the beta or gamma ENaC subunits have been found. In PHA-1, loss-of-function mutations in the alpha, beta, or gamma subunits have been found
59 GORDON S SYNDROME (PSEUDOHYPOALDOSTERONISM TYPE II) The WNKs [ with no lysine ] mutations of the WNK1 and WNK4 have been found to be responsible for Gordon s syndrome. Wild-type WNK1 and WNK4 inhibit the thiazide-sensitive Na-Cl cotransporter in the distal tubule. Mutations of these proteins are associated with gain of function and increased co-transporter activity, excessive chloride and sodium reabsorption, and volume expansion. Increased WNK1 expression also decreases potassium excretion by inhibiting the renal outer medullary potassium channel(romk).
60 GORDON S SYNDROME (PSEUDOHYPOALDOSTERONISM TYPE II) AD HTN hyperkalemia, hyperchloremic metabolic acidosis, and normal glomerular filtration rate. Thiazides responsive This syndrome maybe associated with short stature, intellectual impairment, dental abnormalities, muscle weakness

61
62 RENOVASCULAR HTN (RVH) 10%(5 25 %) of all secondary HTN in children. RVH is second only to coarctation of the aorta as a correctable cause of HTN in children.
63 RENOVASCULAR HTN (RVH) Fibromuscular dysplasia (FMD ) is the most common cause of RVH in children. FMD Significantly different from that in adults ( with the classic string of beads in the main artery ) FMD in children produces focal unilateral isolated web like stenosis, and the majority of the lesions are in branch vessels or accessory arteries.
64 RENOVASCULAR HTN (RVH) Genetic syndromes such as NF-I Tuberous sclerosis Williams syndrome, Marfan s syndrome, Turner s syndrome Alagille syndrome Vasculitidies such as Takayasu s disease, polyarteritis nodosa, Kawasaki
65 RENOVASCULAR HTN (RVH) Other etiologies of RVH include Extrinsic compression of the renal arteries, Radiation, Umbilical artery catheterization Trauma Congenital rubella syndrome Aneurysms AVM/AVF, Transplant renal artery stenosis
66 RENOVASCULAR HTN (RVH) The stenosis needs to occlude at least 70%of the lumen before it begins to reduce renal blood flow and raise arterial pressure In the late phase, HTN persists despite removal of the stenosis or ischemic kidney, due to hypertensive damage to the contralateral kidney and probably also due to systemic vascular changes
67 CKD/AKI HTN Depends on the etiology of underlying kidney disease rather than on the degree of renal dysfunction (children with congenital urogenital anomalies such as renal dysplasia often do not have HTN because of tubulopathy leading to salt and water wasting.) HTN resulting from renal parenchymal disease is multifactorial in origin. impaired excretion of salt and water, reduced renal blood flow Activation of the RAAS
68 POST-RX HTN The major contributing factors : History of pre-transplant HTN Persistent native kidney presumably via persistent release of renin Effects of immunosuppressive medications Transplant renal artery stenosis Chronic allograft dysfunction
69 POST-RX HTN Calcineurin inhibitors cause: Increased production of the vasoconstrictor endothelin Decreased production of vasodilatory substances Activation of the SNS. Afferent artery vasoconstriction. Na retention. Many studies suggest that calcium channel blockers can minimize calcineurin-induced vasoconstriction thereby ameliorating HTN and preventing chronic graft injury. Rose C et al, Eur J Pediatr. 2001
70 HYPERTENSION IN ENDOCRINE DISEASES Pheochromocytomas and paragangliomas Primary hyperaldosteronism (PAL) Cushing s syndrome Glucocorticoid-remediable aldosteronism (GRA) Familial hyperaldosteronism II and III Reninoma. Primary hyperparathyroidism (PHPT) Hyperthyroidism( activation of the RAAS and increased sodium reabsorption ) Diabetes mellitus (DM).

71 Drug Induced HTN
72 PRIMARY (ESSENTIAL) HTN Most HTN in adults has no identifiable underlying etiology; therefore, the term essential HTN has been utilized for those hypertensive individuals without underlying secondary causes.
73 PRIMARY (ESSENTIAL) HTN In children, primary HTN was traditionally considered uncommon, accounting for less than 25 % of hypertensive children in the early 1990s. However, recently the rate has increased (up to 90 % in some USA series) mainly due to increased obesity Din-Dzietham R et al. Circulation. 2007

74 Midori Awazu, Pedatric Nephrology Textbook 2016
75 SYMPATHETIC NERVOUS SYSTEM ACTIVATION Children with primary HTN : Resting tachycardia compared to normotensive children heightened cardiovascular reactivity to stress Elevated plasma norepinephrine levels
76 NB: Primary HTN is showing more and more to be NOT Primary HTN: 1. ACE 2 Mutation (reduced level of AT1-7) 2. ANP Polymorphism 3. Renalase activity
77
78
79
80 QUESTIONS
81 Choose one correct answer : A) Familial hyperaldosteronism type III (FH-III) has been recently identified with mutations in the potassium channel KCNJ5 and is Glucocorticoid remediable B) Familial Hyperaldosteronism Type I (Glucocorticoid Remediable Aldosteronism) shows early onset of HTN with normal or elevated aldosterone levels despite suppressed plasma renin activity C) A chimeric gene under the effect of TSH is formed in Familial Hyperaldosteronism Type I (Glucocorticoid Remediable Aldosteronism) D) Cortisone causes HTN much more than Cortisol
82 Choose one correct answer : A) Liddle s Syndrome is an AD disease with gain of function of Thiazide sensitive NCC in distal Tubules B) Gordon s Syndrome is caused by a gain of function in the Amiloride sensitive ENaC in the collecting ducts C) Aldactone is the drug of Choice in Liddle s Syndrome to treat both hypokalemia and HTN in one act D) Gordon s Syndrome shows Type IV RTA
83 Choose one correct answer : A) Renalase maybe decreased in Primary HTN B) ANP polymorphism may contribute to the pathophysiology of primary HTN C) ACE 2 mutations can lead to more vasoconstriction in primary HTN D) All of the above

84
85
86
87
88
89
90 In 2008, American Heart Association issued a guideline trying to standardize the use of ABPM in children, including the detailed recommendations for the use of ABPM and for the interpretation of the data Urbina E et al. Hypertension Subsequently, the European Society of Hypertension recommended the use of ABPM in children in certain settings Lurbe E et al. J Hypertens. 2009;
91 functional changes specifically decreased relaxation and increased contraction [9]. Decreased relaxation has been attributed primarily to endothelial dysfunction, and increased contraction has been attributed to enhanced smooth muscle cell vasoreactivity. Sensitivity to vasoconstrictors may also be increased. Decreased relaxation is an effect of impaired endothelial production of vasodilatory substances (mainly nitric oxide [NO] and prostacyclin) or increased production of vasoconstricting substances (endothelin, platelet-derived growth factor [PDGF]), or both.
92 Sympathetic Innervation/CNS Renal vessels, tubules, and the juxtaglomerular apparatus are innervated by the renal sympathetic nerves. Renal sympathetic nerve activity (RSNA) influences renal hemodynamics, solute and water handling, and hormonal release. Increased RSNA is found in animal models of HTN and also in hypertensive humans [13]. SNS activation, as confirmed by increased circulating noradrenaline, muscle sympathetic nerve traffic, and systemic noradrenaline spillover, has for many decades been established as almost universally present in primary HTN
93 that was blocked by an ANG-II receptor antagonist Increased RSNAconstricts the renal vasculature and decreases GFR and renal blood flow. The hypertensive response to chronic renal adrenergic stimulation is associated with a sustained increase in plasma renin activity and is dependent on an increase in plasma angiotensin II (ANG-II) concentration [16]. Sympathetic nerve activation appears to enhance the response to circulatingang-ii [17]. The renal effects of ANG-II on proximal tubular chloride and water reabsorption are decreased by 75 % in animals after experimental renal denervation. Thus only about 25 % of ANG-II effect is mediated directly via type 1 angiotensin receptors, with the majority of the effect being dependent on intact renal innervation. In experimental renal sympathetic nerve stimulation, ANG-II enhanced the renal venous outflow of norepinephrine, an effect
94 The AT2 receptor is a seven-transmembranetype, G protein-coupled receptor comprising 363 amino acids. It has low amino acid sequence homology (~34 %) with AT1A or AT1B receptors [36]. The expression of the AT2 receptor is upregulated by sodium depletion [48] and is inhibited by ANG-II and growth factors such as PDGF and EGF [49]. Under physiologic conditions, the AT2 receptor mainly antagonizes AT1-mediated actions. Cardiovascular effects of the AT2 receptor generally appear to be opposite to those of the AT1 receptor and may be protective [50, 51]. In the kidney, stimulation of the AT2receptor promotes natriuresis through interactions with the renal dopaminergic system [52].
95 gene (CYP11B1) on chromosome 8. Aldosterone synthase is the rate-limiting enzyme for aldosterone biosynthesis in the adrenal glomerulosa, and 11β-hydroxylase is an enzyme involved in cortisol biosynthesis in the adrenal fasciculata whose expression is regulated by adrenocorticotropic hormone (ACTH). The resulting chimeric gene (CYP11B1/CYP11B2) is expressed in the adrenal fasciculata and encodes a protein product with aldosterone synthase enzymatic activity whose expression is regulated by ACTH. Consequently, aldosterone synthase activity is ectopically

96
97 Congenital adrenal hyperplasia results from two known defects in either 11-β-hydroxylase or17-α-hydroxylase activity and may cause HTN. These defects lead to overproduction of 21-hydroxylated steroids, which activate mineralocorticoid receptors, resulting in increased sodium reabsorption in distal tubules [295, 296].

98
99

100
101 HYPERTENSION IN ENDOCRINE DISEASES Pheochromocytomas and paragangliomas Although most pheochromocytomas are sporadic, there is a familial predisposition in patients Multiple endocrine neoplasia type II(MEN II) Von Hippel Lindau disease NF-I and familial paraganglioma [ ]. Rarely, in tuberous sclerosis, Sturge Weber syndrome, and ataxia telangiectasia.
102 HYPERTENSION IN ENDOCRINE DISEASES Primary hyperaldosteronism (PAL) is now believed to be much more common than previously thought [397, 412, 413]. PAL was first reported by Conn as aldosterone-producing adenoma (APA) [414] and commonly results from adrenal hypertrophy ( idiopathic hyperaldosteronism ; IHA)
103 Hypertension in Dialysis Patients Children receiving chronic dialysis have a significant incidence of HTN: % of children receiving hemodialysis and % of children receiving peritoneal dialysis in the NAPRTCS dialysis database were receiving antihypertensive
104 The aldosterone/mr cascade exerts its effects in the so-called aldosterone-sensitive distal nephron (ASDN), which includes the late distal convoluted tubule, connecting tubule, and collecting duct. Upon binding of aldosterone, MR undergoes conformational changes, dissociation from chaperone proteins, dimerization, and translocation to the nucleus, where it binds to the responsive elements in the promoter regions of target genes to regulate transcription. Among the aldosterone-induced genes, serum/glucocorticoid regulated kinase 1 (SGK1) plays a major role in the control of sodium reabsorption. Studies have clarified the detailed mechanism of epithelial sodium channel (ENaC) regulation by SGK1 (Fig. 1). Nedd4-2 (neural precursor cell expressed, developmentally downregulated 4-2) is a HECT domain containing E3 ubiquitin ligase that interacts with the C terminus of ENaC subunits and maintains the plasma membrane ENaC at low levels through ubiquitination-dependent mechanisms. Aldosterone-induced SGK1 phosphorylates the Nedd4-2, which disrupts the tonic inhibition of ENaC by Nedd4-2, leading to indirect stimulation of sodium transport. SGK1 phosphorylation of Nedd4-2 results in binding and suppresses Nedd4-2 ENaC interaction [11]. ENaC mutations in Liddle s syndrome also affect the Nedd4-2 interaction, leading to constitutive ENaC expression and increased sodium reabsorption [12]. SGK1 may also modulate ENaC activity though a mechanism independent of Nedd4-2 [13].Fig. 1
105 The major pathophysiologic mechanism in most dialysis patients seems to be volume overload related to sodium and water retention. Evidence in favor of fluid overload being the major mechanism can be found in the many studies that demonstrate correction of HTN by increased fluid removal in both peritoneal dialysis and hemodialysis patients [359, 360]. However, numerous other factors have been implicated, including overactivity of the SNS, activation of the RAAS, erythropoietin treatment, parathyroid hormone, and nocturnal hypoxemia [361]. Recent studies have also implicated altered endothelial cell function, with increased vasoconstrictors such as endothelin and a reduction of vasodilators such as NO being involved in the pathogenesis of dialysis HTN
106
107 POST-RX HTN HTN is a common complication following renal transplantation. 85% of deceased donor recipients and 79 % of live donor recipients are receiving antihypertensive medications immediately post-transplant (decreasing to 69 % and 59 %, respectively 5 yrs after TX) [370].

108

109
110 Endothelin-1 Endothelin-1 (ET-1) is an endothelial-derived, potent vasoconstrictive peptide containing 21 amino acids [110]. Three isopeptides of endothelin (ET-1, ET-2, ET-3), encoded by separate genes, have been identified [111]. Endothelial ET-1 synthesis is activated by vasoactive hormones, growth factors, hypoxia, shear stress, lipoproteins, free radicals, endotoxin, and cyclosporine and is inhibited by NO, natriuretic peptides, heparin, and prostaglandins [112]. Apart from endothelial cells, ET-1 is also produced by
111 ET-1 primarily appears to be a locally acting paracrine substance. ET-1 closes membrane K+ channels [115], which prevents cellular efflux of K+, thereby favoring membrane depolarization, leading to smooth muscle cell contraction. In the kidney, ET-1 causes constriction of both afferent and efferent glomerular arterioles, thereby reducing both renal plasma flow and glomerular filtration rate [116]. It blocks reabsorption of sodium by inhibiting tubular Na+/K+ ATPase activity in the proximal tubule and collecting duct [117]. Endothelin signals through two receptor subtypes

112
113 NO is a vasodilator, and the balance between NO and various endothelium-derived vasoconstrictors and the SNS maintains physiologic vascular tone [133]. In addition, NO suppresses
114 platelet aggregation, leukocyte migration, and cellular adhesion to the endothelium. It attenuates vascular smooth muscle cell proliferation and migration, as well as inhibits activation and expression of certain adhesion molecules and has an influence on production of superoxide anion [134]. Endothelium-dependent relaxation is decreased in patients with primary HTN [135] and appears to be related to defective L-arginine transport.
115 Treatment with inhibitors of NO synthesis induces a hypertensive response, while L-arginine treatment prevents the development of HTN in salt-sensitive rats [137] and also causes a rapid reduction in systolic and diastolic pressures when infused into both healthy subjects and patients with primary HTN [138]. Methylated L-arginine derivatives, including NG-NG-dimethylarginine (asymmetric dimethylarginine, ADMA), an endogenous inhibitor of NOS, and symmetric dimethylarginine, its inactive isomer, are present in human plasma and urine. Elevated levels of ADMAand other markers of oxidative stress have been demonstrated in patients with primary HTN and have been postulated to contribute to the endothelial dysfunction that accompanies HTN [139].


116
117 Shibata S and Fujita T. Curr. Hypertens. Rep.2011
118 Shibata S and Fujita T. Curr. Hypertens. Rep.2011
119 UP TO DATE INTRODUCTION Liddle's syndrome and autosomal recessive pseudohypoaldosteronism type 1 are rare genetic disorders associated with abnormalities in the function of the collecting tubule sodium channel, also called the epithelial sodium channel (ENaC) or the amiloride-sensitive sodium channel: ENaC function is increased in Liddle's syndrome, leading to manifestations similar to those caused by mineralocorticoid excess, such as hypertension and, in some patients, hypokalemia and metabolic alkalosis. Presentation at a young age, which occurs in most patients, suggests the possibility of a genetic disorder rather than an adrenal adenoma. In addition, plasma and urinary aldosterone levels are reduced, not increased as in primary aldosteronism. ENaC function is decreased in autosomal recessive pseudohypoaldosteronism type 1, resulting in aldosterone resistance. Affected patients present in infancy with sodium wasting, hypovolemia, and
120 ANG II Angiotensin II and angiotensin III (ANG-II, ANG-III) induce aldosterone synthesis Potassium, endothelin, adrenocorticotropic hormone (ACTH) and vasopressin stimulate its secretion. Inhibitors of aldosterone secretion include atrial natriuretic peptide, somatostatin, and dopamine. Dietary sodium restriction increases aldosterone secretion in order to restore plasma volume. Aldosterone acts via type I mineralocorticoid receptors causing retention of sodium and potassium excretion. It also activates the SNS
Salt Sensitivity: Mechanisms, Diagnosis, and Clinical Relevance
 Salt Sensitivity: Mechanisms, Diagnosis, and Clinical Relevance Matthew R. Weir, MD Professor and Director Division of Nephrology University of Maryland School of Medicine Overview Introduction Mechanisms
Salt Sensitivity: Mechanisms, Diagnosis, and Clinical Relevance Matthew R. Weir, MD Professor and Director Division of Nephrology University of Maryland School of Medicine Overview Introduction Mechanisms
Blood Pressure Regulation 2. Faisal I. Mohammed, MD,PhD
 Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2. Faisal I. Mohammed, MD,PhD
 Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
Hyperaldosteronism: Conn's Syndrome
 RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
renoprotection therapy goals 208, 209
 Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
014 Chapter 14 Created: 9:25:14 PM CST
 014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
Adrenal gland And Pancreas
 Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
Special Lecture 11/08/2013. Hypertension Dr. HN Mayrovitz
 Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Regulation of Body Fluids: Na + and Water Linda Costanzo, Ph.D.
 Regulation of Body Fluids: Na + and Water Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. Why body sodium content determines ECF volume and the relationships
Regulation of Body Fluids: Na + and Water Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. Why body sodium content determines ECF volume and the relationships
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
HYPERTENSIVE VASCULAR DISEASE
 HYPERTENSIVE VASCULAR DISEASE Cutoffs in diagnosing hypertension in clinical practice sustained diastolic pressures >90 mm Hg, or sustained systolic pressures >140 mm Hg Malignant hypertension A small
HYPERTENSIVE VASCULAR DISEASE Cutoffs in diagnosing hypertension in clinical practice sustained diastolic pressures >90 mm Hg, or sustained systolic pressures >140 mm Hg Malignant hypertension A small
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Renovascular hypertension in children and adolescents
 Renovascular hypertension in children and adolescents M I E C Z Y S L AW L I T W I N D E P T. O F N E P H R O LO G Y & A R T E R I A L H Y P E R T E N S I O N T H E C H I L D R E N S M E M O R I A L H
Renovascular hypertension in children and adolescents M I E C Z Y S L AW L I T W I N D E P T. O F N E P H R O LO G Y & A R T E R I A L H Y P E R T E N S I O N T H E C H I L D R E N S M E M O R I A L H
Cardiovascular System B L O O D V E S S E L S 2
 Cardiovascular System B L O O D V E S S E L S 2 Blood Pressure Main factors influencing blood pressure: Cardiac output (CO) Peripheral resistance (PR) Blood volume Peripheral resistance is a major factor
Cardiovascular System B L O O D V E S S E L S 2 Blood Pressure Main factors influencing blood pressure: Cardiac output (CO) Peripheral resistance (PR) Blood volume Peripheral resistance is a major factor
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Mineralocorticoids. Introduction
 Mineralocorticoids Introduction concepts to remember: a) water, glucose, mineral metabolism; b) adrenal in stress and blood pressure 15 Renin - angiotensin (RAS) and kallikrein kinin (KKS) systems: synthesis,
Mineralocorticoids Introduction concepts to remember: a) water, glucose, mineral metabolism; b) adrenal in stress and blood pressure 15 Renin - angiotensin (RAS) and kallikrein kinin (KKS) systems: synthesis,
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1
 Lecture 18: Endocrine control of renal function. p. 1") BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
Mendelian Hypertension: Clinical Implications
 Mendelian Hypertension: Clinical Implications Anna Dominiczak MD Regius Professor of Medicine Valencia, ICHCA, 2018 Monogenic Hypertension & Hypotension Gitelman Syndrome Gordon Syndrome Modified from
Mendelian Hypertension: Clinical Implications Anna Dominiczak MD Regius Professor of Medicine Valencia, ICHCA, 2018 Monogenic Hypertension & Hypotension Gitelman Syndrome Gordon Syndrome Modified from
Regulation of Arterial Blood Pressure 2 George D. Ford, Ph.D.
 Regulation of Arterial Blood Pressure 2 George D. Ford, Ph.D. OBJECTIVES: 1. Describe the Central Nervous System Ischemic Response. 2. Describe chemical sensitivities of arterial and cardiopulmonary chemoreceptors,
Regulation of Arterial Blood Pressure 2 George D. Ford, Ph.D. OBJECTIVES: 1. Describe the Central Nervous System Ischemic Response. 2. Describe chemical sensitivities of arterial and cardiopulmonary chemoreceptors,
Pharmacology - Problem Drill 11: Vasoactive Agents
 Pharmacology - Problem Drill 11: Vasoactive Agents Question No. 1 of 10 1. Vascular smooth muscle contraction is triggered by a rise in. Question #01 (A) Luminal calcium (B) Extracellular calcium (C) Intracellular
Pharmacology - Problem Drill 11: Vasoactive Agents Question No. 1 of 10 1. Vascular smooth muscle contraction is triggered by a rise in. Question #01 (A) Luminal calcium (B) Extracellular calcium (C) Intracellular
ADRENAL GLAND. Introduction 4/21/2009. Among most important and vital endocrine organ. Small bilateral yellowish retroperitoneal organ
 Introduction Among most important and vital endocrine organ ADRENAL GLAND D.Hammoudi.MD Small bilateral yellowish retroperitoneal organ Lies just above kidney in gerota s fascia 2 1 The Adrenal Gland Anatomy
Introduction Among most important and vital endocrine organ ADRENAL GLAND D.Hammoudi.MD Small bilateral yellowish retroperitoneal organ Lies just above kidney in gerota s fascia 2 1 The Adrenal Gland Anatomy
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
CASE 13. What neural and humoral pathways regulate arterial pressure? What are two effects of angiotensin II?
 CASE 13 A 57-year-old man with long-standing diabetes mellitus and newly diagnosed hypertension presents to his primary care physician for follow-up. The patient has been trying to alter his dietary habits
CASE 13 A 57-year-old man with long-standing diabetes mellitus and newly diagnosed hypertension presents to his primary care physician for follow-up. The patient has been trying to alter his dietary habits
Secondary hypertension How to approach?
 Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Outline Urinary System. Urinary System and Excretion. Urine. Urinary System. I. Function II. Organs of the urinary system
 Outline Urinary System Urinary System and Excretion Bio105 Chapter 16 Renal will be on the Final only. I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of
Outline Urinary System Urinary System and Excretion Bio105 Chapter 16 Renal will be on the Final only. I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of
BIOH122 Session 6 Vascular Regulation
 BIOH122 Session 6 Vascular Regulation To complete this worksheet, select: Module: Distribution Title: Vascular Regulation Introduction 1. a. How do Mean Arterial Blood Pressure (MABP) and Systemic Vascular
BIOH122 Session 6 Vascular Regulation To complete this worksheet, select: Module: Distribution Title: Vascular Regulation Introduction 1. a. How do Mean Arterial Blood Pressure (MABP) and Systemic Vascular
RENAL PHYSIOLOGY. Physiology Unit 4
 RENAL PHYSIOLOGY Physiology Unit 4 Renal Functions Primary Function is to regulate the chemistry of plasma through urine formation Additional Functions Regulate concentration of waste products Regulate
RENAL PHYSIOLOGY Physiology Unit 4 Renal Functions Primary Function is to regulate the chemistry of plasma through urine formation Additional Functions Regulate concentration of waste products Regulate
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Kidneys in regulation of homeostasis
 Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Blood Pressure Regulation. Slides 9-12 Mean Arterial Pressure (MAP) = 1/3 systolic pressure + 2/3 diastolic pressure
 = 1/3 systolic pressure + 2/3 diastolic pressure") Sheet physiology(18) Sunday 24-November Blood Pressure Regulation Slides 9-12 Mean Arterial Pressure (MAP) = 1/3 systolic pressure + 2/3 diastolic pressure MAP= Diastolic Pressure+1/3 Pulse Pressure CO=MAP/TPR
Sheet physiology(18) Sunday 24-November Blood Pressure Regulation Slides 9-12 Mean Arterial Pressure (MAP) = 1/3 systolic pressure + 2/3 diastolic pressure MAP= Diastolic Pressure+1/3 Pulse Pressure CO=MAP/TPR
Hormonal Control of Osmoregulatory Functions *
 OpenStax-CNX module: m44828 1 Hormonal Control of Osmoregulatory Functions * OpenStax This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 3.0 By the end of
OpenStax-CNX module: m44828 1 Hormonal Control of Osmoregulatory Functions * OpenStax This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 3.0 By the end of
In the name of GOD. Animal models of cardiovascular diseases: myocardial infarction & hypertension
 In the name of GOD Animal models of cardiovascular diseases: myocardial infarction & hypertension 44 Presentation outline: Cardiovascular diseases Acute myocardial infarction Animal models for myocardial
In the name of GOD Animal models of cardiovascular diseases: myocardial infarction & hypertension 44 Presentation outline: Cardiovascular diseases Acute myocardial infarction Animal models for myocardial
The ability of the kidneys to regulate extracellular fluid volume by altering sodium
 REGULATION OF EXTRACELLULAR FLUID VOLUME BY INTEGRATED CONTROL OF SODIUM EXCRETION Joey P. Granger Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson, Mississippi
REGULATION OF EXTRACELLULAR FLUID VOLUME BY INTEGRATED CONTROL OF SODIUM EXCRETION Joey P. Granger Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson, Mississippi
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Where in the adrenal cortex is cortisol produced? How do glucocorticoids inhibit prostaglandin production?
 CASE 35 A 36-year-old woman presents to her gynecologist with complaints of amenorrhea and hirsutism. She has also noticed an increase in her weight (especially in the trunk region) and easy fatigability.
CASE 35 A 36-year-old woman presents to her gynecologist with complaints of amenorrhea and hirsutism. She has also noticed an increase in her weight (especially in the trunk region) and easy fatigability.
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
THE HYPERKALEMIC SYNDROMES
 THE HYPERKALEMIC SYNDROMES K + BALANCE Cells (3400 meq) ECF (60 meq) External K Pump insulin catechols Na intake Leak K ph; osmolality membrane integrity distal Na + renal { delivery output aldosterone
THE HYPERKALEMIC SYNDROMES K + BALANCE Cells (3400 meq) ECF (60 meq) External K Pump insulin catechols Na intake Leak K ph; osmolality membrane integrity distal Na + renal { delivery output aldosterone
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Blood Pressure Regulation 2. Faisal I. Mohammed, MD,PhD
 Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion.
 The Kidney Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion. The kidney has 6 roles in the maintenance of homeostasis. 6 Main Functions 1. Ion Balance
The Kidney Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion. The kidney has 6 roles in the maintenance of homeostasis. 6 Main Functions 1. Ion Balance
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology
 Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
BODY FLUID. Outline. Functions of body fluid Water distribution in the body Maintenance of body fluid. Regulation of fluid homeostasis
 BODY FLUID Nutritional Biochemistry Yue-Hwa Chen Dec 13, 2007 Chen 1 Outline Functions of body fluid Water distribution in the body Maintenance of body fluid Intake vs output Regulation of body fluid Fluid
BODY FLUID Nutritional Biochemistry Yue-Hwa Chen Dec 13, 2007 Chen 1 Outline Functions of body fluid Water distribution in the body Maintenance of body fluid Intake vs output Regulation of body fluid Fluid
Mechanism: 1- waterretention from the last part of the nephron which increases blood volume, venous return EDV, stroke volume and cardiac output.
 Blood pressure regulators: 1- Short term regulation:nervous system Occurs Within secondsof the change in BP (they are short term because after a while (2-3 days) they adapt/reset the new blood pressure
Blood pressure regulators: 1- Short term regulation:nervous system Occurs Within secondsof the change in BP (they are short term because after a while (2-3 days) they adapt/reset the new blood pressure
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 18
 Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 18 Learning Objectives for this File: 1. Learn how the macula densa monitors physiologic state and its connection with renin production based on
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 18 Learning Objectives for this File: 1. Learn how the macula densa monitors physiologic state and its connection with renin production based on
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
BIOH122 Human Biological Science 2
 BIOH122 Human Biological Science 2 Session 17 Urinary System 2 Glomerular Filtration Bioscience Department Endeavour College of Natural Health endeavour.edu.au Session Plan o Overview of Renal Physiology
BIOH122 Human Biological Science 2 Session 17 Urinary System 2 Glomerular Filtration Bioscience Department Endeavour College of Natural Health endeavour.edu.au Session Plan o Overview of Renal Physiology
Renal physiology D.HAMMOUDI.MD
 Renal physiology D.HAMMOUDI.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood glucose
Renal physiology D.HAMMOUDI.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood glucose
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Blood Pressure Regulation -1
 CVS Physiology Lecture 18 Blood Pressure Regulation -1 Please study the previous sheet before studying this one, even if the first part in this sheet is revision. In the previous lecture we were talking
CVS Physiology Lecture 18 Blood Pressure Regulation -1 Please study the previous sheet before studying this one, even if the first part in this sheet is revision. In the previous lecture we were talking
Role of Minerals in Hypertension
 Role of Minerals in Hypertension Lecture objectives By the end of the lecture students will be able to Define primary and secondary hypertention and their risk factors. Relate role of minerals with hypertention.
Role of Minerals in Hypertension Lecture objectives By the end of the lecture students will be able to Define primary and secondary hypertention and their risk factors. Relate role of minerals with hypertention.
Functional vascular disorders
 Functional vascular disorders Raynaud s phenomenon Raynaud s phenomenon Refers to Intermittent,bilateral attacks of ischemia of the fingers or toes, and sometimes ears or nose. It clinically manifests
Functional vascular disorders Raynaud s phenomenon Raynaud s phenomenon Refers to Intermittent,bilateral attacks of ischemia of the fingers or toes, and sometimes ears or nose. It clinically manifests
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
REGULATION OF CARDIOVASCULAR SYSTEM
 REGULATION OF CARDIOVASCULAR SYSTEM Jonas Addae Medical Sciences, UWI REGULATION OF CARDIOVASCULAR SYSTEM Intrinsic Coupling of cardiac and vascular functions - Autoregulation of vessel diameter Extrinsic
REGULATION OF CARDIOVASCULAR SYSTEM Jonas Addae Medical Sciences, UWI REGULATION OF CARDIOVASCULAR SYSTEM Intrinsic Coupling of cardiac and vascular functions - Autoregulation of vessel diameter Extrinsic
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Physio 12 -Summer 02 - Renal Physiology - Page 1
 Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Obesity mediated hypertension and renal dysfunction
 Obesity mediated hypertension and renal dysfunction Gergely Bodor Marion Hervouet Nicky Honnef Mariarosaria Malgadi Julie Robert Tutor: Pr Alina Parvu Objectives 1. Introduction 2. Renal structural and
Obesity mediated hypertension and renal dysfunction Gergely Bodor Marion Hervouet Nicky Honnef Mariarosaria Malgadi Julie Robert Tutor: Pr Alina Parvu Objectives 1. Introduction 2. Renal structural and
Questions? Homework due in lab 6. PreLab #6 HW 15 & 16 (follow directions, 6 points!)
") Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Pediatric Hypertension. Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019
 Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
- Dr Alia Shatnawi. 1 P a g e
 - 1 مها أبو عجمية - - - Dr Alia Shatnawi 1 P a g e A Skippable Intr0 Blood pressure normally decreases during the night. Absence of this phenomenon is called (nondipping) Wikipedia: Circadian rhythm....
- 1 مها أبو عجمية - - - Dr Alia Shatnawi 1 P a g e A Skippable Intr0 Blood pressure normally decreases during the night. Absence of this phenomenon is called (nondipping) Wikipedia: Circadian rhythm....
Renal-Related Questions
 Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Physiology Lecture 2. What controls GFR?
 Physiology Lecture 2 Too much blood is received by the glomerular capillaries, this blood contains plasma, once this plasma enters the glomerular capillaries it will be filtered to bowman s space. The
Physiology Lecture 2 Too much blood is received by the glomerular capillaries, this blood contains plasma, once this plasma enters the glomerular capillaries it will be filtered to bowman s space. The
RENAL PHYSIOLOGY. Zekeriyya ALANOGLU, MD, DESA Ahmet Onat Bermede, MD, Ankara University School of Medicine Dept. Anesthesiology and ICM
 RENAL PHYSIOLOGY Zekeriyya ALANOGLU, MD, DESA Ahmet Onat Bermede, MD, Ankara University School of Medicine Dept. Anesthesiology and ICM Kidneys Stabilize the composition of the ECF (electrolyte, H
RENAL PHYSIOLOGY Zekeriyya ALANOGLU, MD, DESA Ahmet Onat Bermede, MD, Ankara University School of Medicine Dept. Anesthesiology and ICM Kidneys Stabilize the composition of the ECF (electrolyte, H
Renal Physiology Part II. Bio 219 Napa Valley College Dr. Adam Ross
 Renal Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Fluid and Electrolyte balance As we know from our previous studies: Water and ions need to be balanced in order to maintain proper homeostatic
Renal Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Fluid and Electrolyte balance As we know from our previous studies: Water and ions need to be balanced in order to maintain proper homeostatic
Structure and organization of blood vessels
 The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
Regulation of fluid and electrolytes balance
 Regulation of fluid and electrolytes balance Three Compartment Fluid Compartments Intracellular = Cytoplasmic (inside cells) Extracellular compartment is subdivided into Interstitial = Intercellular +
Regulation of fluid and electrolytes balance Three Compartment Fluid Compartments Intracellular = Cytoplasmic (inside cells) Extracellular compartment is subdivided into Interstitial = Intercellular +
Na concentration in the extracellular compartment is 140
 هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
Nephron Anatomy Nephron Anatomy
 Kidney Functions: (Eckert 14-17) Mammalian Kidney -Paired -1% body mass -20% blood flow (Eckert 14-17) -Osmoregulation -Blood volume regulation -Maintain proper ion concentrations -Dispose of metabolic
Kidney Functions: (Eckert 14-17) Mammalian Kidney -Paired -1% body mass -20% blood flow (Eckert 14-17) -Osmoregulation -Blood volume regulation -Maintain proper ion concentrations -Dispose of metabolic
2) This is a Point and Click question. You must click on the required structure.
 This is a Point and Click question. You must click on the required structure.") Class: A&P2-1 Description: Test: Excretory Test Points: 144 Test Number: 28379 Printed: 31-March-10 12:03 1) This is a Point and Click question. You must click on the required structure. Click on the Bowman's
Class: A&P2-1 Description: Test: Excretory Test Points: 144 Test Number: 28379 Printed: 31-March-10 12:03 1) This is a Point and Click question. You must click on the required structure. Click on the Bowman's
Blood Pressure Fox Chapter 14 part 2
 Vert Phys PCB3743 Blood Pressure Fox Chapter 14 part 2 T. Houpt, Ph.D. 1 Cardiac Output and Blood Pressure How to Measure Blood Pressure Contribution of vascular resistance to blood pressure Cardiovascular
Vert Phys PCB3743 Blood Pressure Fox Chapter 14 part 2 T. Houpt, Ph.D. 1 Cardiac Output and Blood Pressure How to Measure Blood Pressure Contribution of vascular resistance to blood pressure Cardiovascular
BIOL 2402 Fluid/Electrolyte Regulation
 Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Secondary hypertension in the pediatric population
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 12-2015 Secondary hypertension in the pediatric population Ashley M. Gefen Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 12-2015 Secondary hypertension in the pediatric population Ashley M. Gefen Washington University School of Medicine
Systemic Hypertension
 BCS Theme Session Cardiovascular Block Pathology of Hypertension Department of Pathology University of Sydney Systemic Hypertension Definition of Systemic hypertension: consistent blood pressure elevation
BCS Theme Session Cardiovascular Block Pathology of Hypertension Department of Pathology University of Sydney Systemic Hypertension Definition of Systemic hypertension: consistent blood pressure elevation
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
RENAL PHYSIOLOGY. Zekeriyya ALANOGLU, MD, DESA. Ahmet Onat Bermede, MD. Ankara University School of Medicine Dept. Anesthesiology and ICM
 RENAL PHYSIOLOGY Zekeriyya ALANOGLU, MD, DESA. Ahmet Onat Bermede, MD. Ankara University School of Medicine Dept. Anesthesiology and ICM Kidneys Stabilize the composition of the ECF (electrolyte,
RENAL PHYSIOLOGY Zekeriyya ALANOGLU, MD, DESA. Ahmet Onat Bermede, MD. Ankara University School of Medicine Dept. Anesthesiology and ICM Kidneys Stabilize the composition of the ECF (electrolyte,
Chapter 17: Urinary System
 Introduction Chapter 17: Urinary System Organs of the Urinary System REFERENCE FIGURE 17.1 2 kidneys filters the blood 2 ureters transport urine from the kidneys to the urinary bladder Urinary bladder
Introduction Chapter 17: Urinary System Organs of the Urinary System REFERENCE FIGURE 17.1 2 kidneys filters the blood 2 ureters transport urine from the kidneys to the urinary bladder Urinary bladder
Paul M McKie, Alessandro Cataliotti, Guido Boerrigter, Horng C Chen, Fernando L Martin, and John C Burnett Jr
 Cardiorenal Enhancing and Aldosterone Suppressing Actions of a Novel Designer Natriuretic Peptide in Experimental Hypertension with Ventricular Pressure Overload Paul M McKie, Alessandro Cataliotti, Guido
Cardiorenal Enhancing and Aldosterone Suppressing Actions of a Novel Designer Natriuretic Peptide in Experimental Hypertension with Ventricular Pressure Overload Paul M McKie, Alessandro Cataliotti, Guido
Urinary System and Excretion. Bio105 Lecture 20 Chapter 16
 Urinary System and Excretion Bio105 Lecture 20 Chapter 16 1 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system
Urinary System and Excretion Bio105 Lecture 20 Chapter 16 1 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system
Prof. Andrzej Wiecek Department of Nephrology, Endocrinology and Metabolic Diseases Medical University of Silesia Katowice, Poland.
 What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
Hormones. Introduction to Endocrine Disorders. Hormone actions. Modulation of hormone levels. Modulation of hormone levels
 Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Monogenic forms of hypertension
 Eur J Pediatr (2012) 171:1433 1439 DOI 10.1007/s00431-011-1440-7 REVIEW Monogenic forms of hypertension Giacomo Domenico Simonetti & Markus G. Mohaupt & Mario G. Bianchetti Received: 29 December 2010 /
Eur J Pediatr (2012) 171:1433 1439 DOI 10.1007/s00431-011-1440-7 REVIEW Monogenic forms of hypertension Giacomo Domenico Simonetti & Markus G. Mohaupt & Mario G. Bianchetti Received: 29 December 2010 /