Primary and secondary hyperaldosteronism. Zsolt Turóczi, M.D. 2nd Department of Internal Medicine
|
|
|
- Hugo Collins
- 6 years ago
- Views:
Transcription
1 Primary and secondary hyperaldosteronism Zsolt Turóczi, M.D. 2nd Department of Internal Medicine

2 Adrenal gland

3 Adrenal cortex
4
5 Carey RM. Primary aldosteronism. Journal of Surgical Oncology 2012: 106;
6 Carey RM. Primary aldosteronism. Journal of Surgical Oncology 2012: 106;
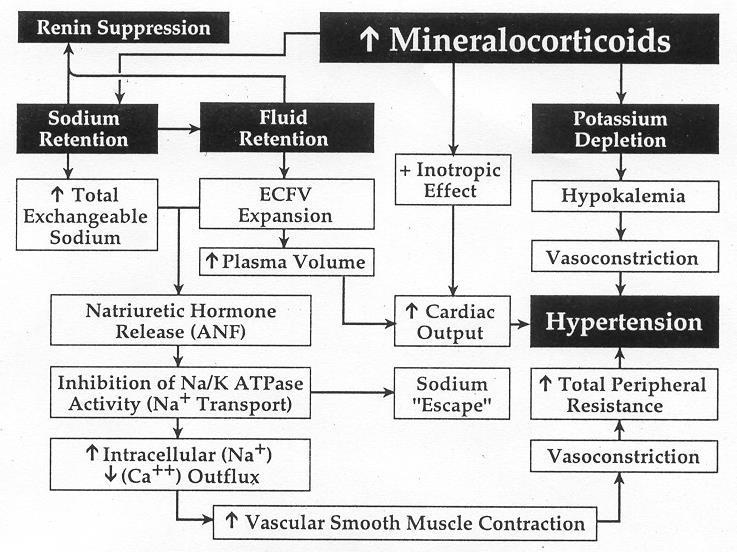
7 Non-genomic effects oxidative stress, systemic inflammation (chronic) Insulin resistance Endothel dysfunction, relaxation disorder hypertension Heart cardiac fibrosis, remodelling, hypertrophia impaired diastolic function CVD (14-35%) Kidneys glomerular damage (membrane integrity disorder) proteinuria renovascularis effects interstitialis effects Chronic renal failure (8-24%)
:")
8 Sowers et al Ann Intern Med. 2009; 150(11):
9 Mineralocorticoid overproduction Primary hyperaldosteronism Dezoxicorticosterone-producing adrenal tumors Congenital adrenal hyperplasia 11 -hydroxylase defect 17 -hidroxylase/17,20-liase defect Cortisol resistance Apparent mineralocorticoid excess Mineralocorticoid receptor mutations (activating) Liddle-syndrome Secundary hyperaldosteronism

10 Professor Jerome W. Conn, M.D., Sc.D. University of Michigen

11 Primary hyperaldosteronism (first documented case) apr.: 34 years old female. mild hypertension, hypokalaemia, hypernatraemic alkalosis, sustained renal function 1954 dec.: exploratory laparotomy: rigth adrenalectomy 1955: case report (J Lab Clin Med 45:661, 1955)
12
13 Prevalence suggested by Conn JAMA 190:220 (1964) I suggest....that as many as 20% of patients with so-called essential hypertension might be suffering from primary aldosteronism while still maintaining normal levels of serum electrolytes.
14 Prevalence suggested by Kaplan Clinical Hypertension textbook 5. ed. (1990) Primary aldosteronism [] has generated as many publications as the number of patients found to have it.
15 Prevalence of hyperaldosteronism Reality: 5-10% Fardella CE, et al. J. Clin Endocrinol Metab Lim PO, et al. J Hum Hypertens : Mosso L, et al. Hypertension : Rossi GP, & PAPY Study Investigators. J Am Coll Card Lars C. et al. Dtsch Arztebl Int 2009; 106(18): Therapy resistent hypertension 17-22% Calhoun DA, et al. Hypertension 2002; 40: Strauch B, J Hum Hypertens 2003;17:
16 Case detection, diagnosis, and treatment of patients with primary aldosteronism: an Endocrine Society clinical practice guideline. Funder J, Carey R, Fardella C, Gomez-Sanchez C, Mantero F, Stowasser M, Young W, Montori VM. J Clin Endocrinol Metab 2008, 93(9):
17 Primary hyperaldosteronism
18 Symptoms In 100% of the patients Hypertension Suppressed plasma renin activity Elevated plasma aldosteron levels in less than 50% Paraesthesia Seeing disorder Intermitting muscle paralysis Tetany In 50 90% Headaches Hypokalaemia/hypernatraemia Muscle weakness/tiredness Arrthymias, Polyuria/polydipsia Impaired glucose tolerancy Alkalosis
19 Suspect for primary hyperaldosteronism Hypertension and hypokalaemia Therapy resistant hypertension (3 or more antihypertensive drug combination with maximal dose) Adrenal incidentaloma and hypertension Anamnesis Young age (under 20 y), stroke under 40 years Severe hypertension (>160/100 mm Hg)
20 Screening Aldosteron-renin ratio (ARR) Standardized sample collection (morning, 15 min rest, normokalaemia) Drug interactions ACE-I, duretics, hypokalaemia: decrease beta-blockers, central alpha2 agonists: increase Funder J, et. al. J Clin Endocrinol Metab 2008, 93(9):
21 Evaluation of ARR Can not be assessed spironolacton eplerenon amilorid False positive results Beta blockers Alpha-methyldopa Clonidin NSAIDs False negative results ACE-inhibitors ARBs Other diuretics Dihidropiridin calciumchannel blockers Estrogenes
22 Correct evaluation For 6 weeks spironolactone eplerenone amilorid Estrogenes Do not need to Doxazosin Prazosin Verapamil Hidralazin For 2 weeks ACE-inhibitors ARBs Diuretics Dihidropiridin calcium-channel inhibitors Beta blockers Alpha-methyldopa Clonidin NSAIDs
23 Normal values aldosterone (1 ng/dl 27,7 pmol/l) plasma renin activity (1 ng/ml/h 12,8 pmol/l/h) direct renin assessment (1 ng/ml/h 5,2 vs. 7,6ng/l) Primary hyperaldosteronism: Aldosterone-renin ratio > (ng/dl) / (ng/ml/h) (30%) Secondary hyperaldosteronism: <10 (ng/dl) / (ng/ml/h) Funder J, et. al. J Clin Endocrinol Metab 2008, 93(9):
24 Confirmation Oral saline load 300 mmol (6g) Na/ die for 3 days Daily K+ control, 24 h urine collection on the last day urinary aldosterone > 12 μg/die (33.3 nmol/die) urinary Na > 200 meq/24 h Mulatero P et al. Confirmatory tests in the diagnosis of primary aldosteronism. Horm Metab Res. 2010; 42 (6):
25 Confirmation Intravenous saline load 2l 0,9% NaCl solution over 4 hours ; patient at rest (sitting position) serum aldosterone > 5 ng/dl urinary Na > 200 meq/24 h Considerations: CRF, CHF, AF Sensitivity: 90%, Specificity: 84% Mulatero P et al. Confirmatory tests in the diagnosis of primary aldosteronism. Horm Metab Res. 2010; 42 (6):
26 Confirmation Fludrocortisone suppression test 3x30 mmol Na (slow-release) + 4x0,1 mg fludrocortizone for 4 days. serum aldosterone (10 am) > 6 ng/dl (166 pmol/l) plasma renin activity < 8.4 mu/l (1 ng/ml/h) Considerations: CRF, CHF - normokalaemia - serum cortizol (8 am > 10 am) Mulatero P et al. Confirmatory tests in the diagnosis of primary aldosteronism. Horm Metab Res. 2010; 42 (6):
27 Captopril challenge Confirmation 1 hour rest mg captopril 2 hour rest serum aldosterone > ng/dl aldosterone renin ratio > ng/dl/ng/ml/h) Considerations: CRF, CHF Increased false positive, false negative results Mulatero P et al. Confirmatory tests in the diagnosis of primary aldosteronism. Horm Metab Res. 2010; 42 (6):
28 Other (less used) tests Confirmation Furosemide upright test (40 mg iv., 2h) Losartan test (50 mg po., 2h) Mulatero P et al. Confirmatory tests in the diagnosis of primary aldosteronism. Horm Metab Res. 2010; 42 (6):
29 Which test should be performed? 1. Fludrocortizon test hospitalization 2. Intravenous saline load 3. Oral saline load 4. Captopril test Mulatero P et al. Confirmatory tests in the diagnosis of primary aldosteronism. Horm Metab Res. 2010; 42 (6):
30 Subtype confirmation 1. Aldosterone producing adenoma (APA) 30-35% 2. Bilateral adrenal hyperplasia (BAH) 65% 3. Familial forms Familial hyperaldosteronism type I (FH-I) 0,66-1% Familial hyperaldosteronism type II (FH-II) 2,8-6% Familial hyperaldosteronism type III (FH-III) N/A 4. Aldosterone producing carcinoma <1% 5. Ectopic adostern producing tumor unique
31 APA vs. BAH Aldosterone-producing adenoma severe symptoms fluid excess/ortostasis does not increase the aldosterone levels aldosterone precursors (18-hydroxicorticosterone) ACTH sensitive Bilateral adrenal hyperplasia mild symptoms fluid excess/ortostasis do increase the aldosterone levels

32 APA vs. BAH
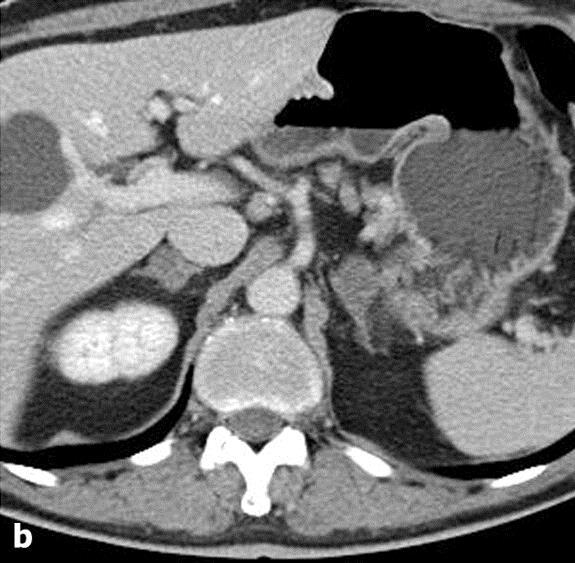
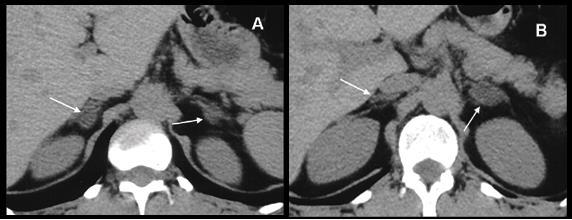
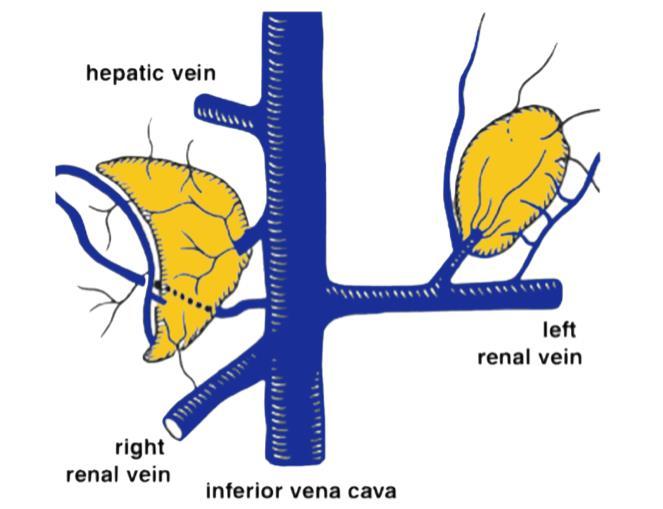
33 Subtype confirmation 1. CT (MRI) scan nodules <1 cm (most nodules are mm) functioning vs non-functioning (2-10%) nodules 2. Adrenal venous sampling gold standard procedure hard to perform (96%) not required if: patient <40 years old, nodule is >1 cm. Rossi GP. Diagnosis and treatment of primary aldosteronism. Endocrinol Metab Clin North Am. 2011; 40:

34
35
36

37
38 Adrenal venous sampling Succesful: cortisol gradient >2 or >3 Aldosteron/cortisol ratio >2 and > contralateral
39
40

41 Subtype confirmation through history

42 NP-54 SPECT
43 Glucocorticoid remediable familial hyperaldosteronism Type I autosom dominant inheritance increased production of hibrid steroids (18-hydroxi-cortisol, 18-oxo-cortisol) suppression of ACTH production abolishes the clinical symptoms CYP11B1 / CYP11B2 gene chimera (8q24) Gill JR, J Clin Endocrinol Metab 53:331, 1982.
44 Aldosterone synthase/11-hydroxylase gene chimera
45 Aldosterone synthase/11-hydroxylase gene chimera
46 Familial hyperaldosteronism type II 2 or more family members are involved Autosomal dominant inheritance Gene localized at 7p22 (FOXK1, FSCN1, RNF216, EIF2AK1 and RAC1) No mutations
47 Familial hyperaldosteronism type III Autosomal dominant inheritance Germ cell mutations in the KCNJ5 gene (Kir3.4 K+ channel) Constitutive aldosteron secretion, cell proliferation Massive bilateral adrenal hyperplasia Therapy resistent hyperaldosteronism Bilateral adrenalectomy required

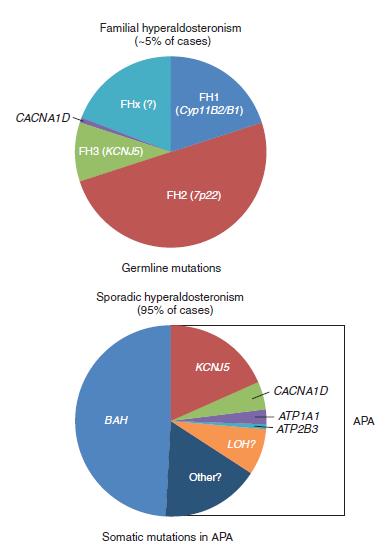
48 Monticone et al. Understanding primary aldosteronism: impact of next generation sequencing and expression profiling. Mol Cell Endocrinol. 2015; 399:
49
50
51 1. Surgery APA or BAH (highly selected cases SR: 19%) Hypertension is cured in 50% Improves self-assessed quality of life 2. Medical therapy Mineralocorticoid receptor antagonist spironolactone 12,5-50 mg/die (side effects), eplerenone mg/die (not approved) +/- angiotensin II receptor blockers Collecting duct acting diuretics Amilorid 2,5-20 mg/die Therapy

52 Mattsson C, Young WF, Primary aldosteronism: diagnostic and treatment strategies. Nat Clin Pract Nephrol. 2006; 2:
53 Steroid biosynthesis defects 11 -hydroxylase 17 -hydroxylase/17,20-liase Prevalence 1:100, published cases Symptoms hypertension, se.k hypertension, se.k hyperandrogenism hypogonadism Hormonal DOC, PRA DOC, PRA alterations androgenes sexual steroids cortisol cortisol Genetics CYP11B1 SNP CYP17 SNP (rarely del, ins) del, dupl, ins, exon del (exon 2, 7),
54 Chracteristics Symptoms of mineralocorticoid overproduction Antagonists do not decrease/abolish symptoms Intrauterin growth retardation Increased cerebrovascular complications Asypmtomatic parents (recessive inheritance?)
55 Hormonal characteristics Plasma levels of coricosteroids are normal Half-life of plasma cortisol increases from 80 to minutes low cortisone levels
56 Cortisol cortisone shuttle
57 Pathomechanism
58 Secondary hyperaldosteronism With hypertension Renovascular disease Renin-secreting tumors Malignant hypertension Pheochromocytoma Without hypertension Hyponatraemia, hypovolaemia (salt-wasting sy) Edema generating conditions congestive heart failure, nephrosis/nephritis syndrome, cirrhosis
59 Secondary hyperaldosteronism Secondary hyperaldosteronism with hypertension Arteria renalis stenosis Coarctatio aortae Malignant hypertension Chronic nephritis Renin-producing tumors Drug-induced (estrogenes)
60 Secondary hyperaldosteronism Secondary hyperaldosteronism with normotension Congestive heart failure Cirrhosis Idiopathic edema Gastrointestinal diseases (vomiting, diarrhea) Renal disease Renal tubular acidosis Nephrosis Bartter syndrome Gitelman syndrome Pseudo-Bartter syndrome
61 Secondary hyperaldosteronism Reason Hypovolaemia in the juxtaglomerular apparat Increased renin secretion Increased aldosterone secretion
62 Bartter syndrome first described in 1962, 1.7 of 100,000 defect in the thick ascending loop of Henle impaired salt reabsorption polyuria/polydypsia normotensive hypokalemic metabolic alkalosis hyperreninemic hyperaldosteronemia juxtaglomerular complex hyperplasia The prevalence of BS is 1.7 of 100,000 [7]. short stature, growth and mental retardation. BS type 3: harbor mutation in CLCNKB gene Manifests in infants or early childhood.
63 Gitelman syndrome first described in 1966 mutation in SLC12A3 gene (NaCl co-transporter (NCCT) mild manifestation, delayed presentation (in late childhood or adulthood) hypocalciuria, and hypomagnesemia [11].
64 Treatment Indometacin Spironolactone KCL Magnesium
65 Aldosterone in CHD Randomized ALdactone Evaluation Study (RALES) Duoble-blind, placebo-controlled Patients qith CHF (EF 35%) Additional spironolactone therapy (25 mg) N Engl J Med 341:709, 1999
66 Aldosterone in CHD Randomized ALdactone Evaluation Study (RALES) N Engl J Med 341:709, 1999
67 Aldosterone in CHD EPlerenone post-acute myocardial infarction HEart failure efficacy and SUrvival Study (EPHESUS) Duoble-blind, placebo-controlled Patients with CHF or previosus AMI Additional eplerenone therapy (25-50 mg) N Engl J Med 341:709, 1999
68 Aldosterone in CHD EPlerenone post-acute myocardial infarction HEart failure efficacy and SUrvival Study (EPHESUS) N Engl J Med 341:709, 1999
69
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
ENDOCRINE FORMS OF HYPERTENSION. Michael Stowasser
 ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Spectrum of Hypertension & Hypokalemia
 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Kidneycentric. Follow this and additional works at:
 Washington University School of Medicine Digital Commons@Becker All Kidneycentric 2014 Gitelman syndrome David Steflik Washington University School of Medicine in St. Louis Follow this and additional works
Washington University School of Medicine Digital Commons@Becker All Kidneycentric 2014 Gitelman syndrome David Steflik Washington University School of Medicine in St. Louis Follow this and additional works
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
About 20% of the Canadian population
 Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
4/23/2015. Objectives DISCLOSURES
 2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient
 Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient Testing/ Original Article Author Information Dr Walter van der Merwe MBChB, FRACP, Consultant Nephrologist, Renal
Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient Testing/ Original Article Author Information Dr Walter van der Merwe MBChB, FRACP, Consultant Nephrologist, Renal
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM
 LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM Riccardo Marsili, Pietro Iacconi, Massimo Chiarugi, Giampaolo Bernini*, Alessandra Bacca*, Paolo Miccoli Department
LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM Riccardo Marsili, Pietro Iacconi, Massimo Chiarugi, Giampaolo Bernini*, Alessandra Bacca*, Paolo Miccoli Department
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
TUBULOPATHY Intensive Care Unit Sina Hospital
 TUBULOPATHY Intensive Care Unit Sina Hospital A 13 years old female who is known case of Scoliosis. She was operated 2 months ago for spinal curve repair. PMH:EMG-MCV In 2 years old =>No Motoneuron Disease
TUBULOPATHY Intensive Care Unit Sina Hospital A 13 years old female who is known case of Scoliosis. She was operated 2 months ago for spinal curve repair. PMH:EMG-MCV In 2 years old =>No Motoneuron Disease
Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes
 ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Resistant hypertension is defined as blood. Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension.
 Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Aldosterone and Cardiovascular Disease
 Aldosterone and Cardiovascular Disease Krishna K. Gaddam, MD, Eduardo Pimenta, MD, Saima Husain, MD, and David A. Calhoun, MD Abstract: Aldosterone is an adrenal hormone that regulates sodium, fluid, and
Aldosterone and Cardiovascular Disease Krishna K. Gaddam, MD, Eduardo Pimenta, MD, Saima Husain, MD, and David A. Calhoun, MD Abstract: Aldosterone is an adrenal hormone that regulates sodium, fluid, and
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT?
 ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Kidneys in regulation of homeostasis
 Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin Ratios
 Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment. Jamie Johnston, MD University of Pittsburgh School of Medicine
 Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism
 Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΚΑΙ ΑΝΤΑΓΩΝΙΣΤΕΣ ΑΛΔΟΣΤΕΡΟΝΗΣ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ MD, FESC. E.Α Κ/Δ Γ.Ν.ΚΑΤΕΡΙΝΗΣ
 ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΚΑΙ ΑΝΤΑΓΩΝΙΣΤΕΣ ΑΛΔΟΣΤΕΡΟΝΗΣ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ MD, FESC. E.Α Κ/Δ Γ.Ν.ΚΑΤΕΡΙΝΗΣ Aldosterone is a mineralocorticoid hormone synthesized by the adrenal glands that has several regulatory
ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΚΑΙ ΑΝΤΑΓΩΝΙΣΤΕΣ ΑΛΔΟΣΤΕΡΟΝΗΣ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ MD, FESC. E.Α Κ/Δ Γ.Ν.ΚΑΤΕΡΙΝΗΣ Aldosterone is a mineralocorticoid hormone synthesized by the adrenal glands that has several regulatory
DIURETICS. Assoc. Prof. Bilgen Başgut
 DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE
 Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE Over 8,000 patients have been studied in two well-designed placebo-controlled outcome-driven clinical trials to evaluate the
Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE Over 8,000 patients have been studied in two well-designed placebo-controlled outcome-driven clinical trials to evaluate the
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Hyperaldosteronism: Conn's Syndrome
 RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
Low renin hypertension
 Review Article Low renin hypertension Manisha Sahay, Rakesh K. Sahay 1 Deparment of Nephrology, 1 Osmania General Hospital, Hyderabad, Andhra Pradesh, India ABSTRACT Low renin hypertension is an important
Review Article Low renin hypertension Manisha Sahay, Rakesh K. Sahay 1 Deparment of Nephrology, 1 Osmania General Hospital, Hyderabad, Andhra Pradesh, India ABSTRACT Low renin hypertension is an important
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Adrenal gland And Pancreas
 Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Hypokalemia. Etiology of hypokalemia
 Hypokalemia The total body K+ storage: 50~55 meq/kg ( approximately 3000~4000 meq) 98% of the body K+ is located in the cells The net effect is that [K+c] is about 140 meq/l and [K+e] is only 4~5 meq/l
Hypokalemia The total body K+ storage: 50~55 meq/kg ( approximately 3000~4000 meq) 98% of the body K+ is located in the cells The net effect is that [K+c] is about 140 meq/l and [K+e] is only 4~5 meq/l
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Prospective Study on the Prevalence of Secondary Hypertension among Hypertensive Patients Visiting a General Outpatient Clinic in Japan
 193 Original Article Prospective Study on the Prevalence of Secondary Hypertension among Hypertensive Patients Visiting a General Outpatient Clinic in Japan Masao OMURA, Jun SAITO, Kunio YAMAGUCHI, Yukio
193 Original Article Prospective Study on the Prevalence of Secondary Hypertension among Hypertensive Patients Visiting a General Outpatient Clinic in Japan Masao OMURA, Jun SAITO, Kunio YAMAGUCHI, Yukio
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN
 Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
RENAL TUBULAR ACIDOSIS An Overview
 RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Diuretics having the quality of exciting excessive excretion of urine. OED. Inhibitors of Sodium Reabsorption Saluretics not Aquaretics
 Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Hyperaldosteronism: recent concepts, diagnosis, and management
 Postgrad Med J 2001;77:639 644 639 Clinical Pharmacology Unit, University of Cambridge, Box 110, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK RFoo K M O Shaughnessy M J Brown Correspondence to: Dr Foo
Postgrad Med J 2001;77:639 644 639 Clinical Pharmacology Unit, University of Cambridge, Box 110, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK RFoo K M O Shaughnessy M J Brown Correspondence to: Dr Foo
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
--Manuscript Draft-- Primary Aldosteronism; adrenal vein sampling; aldosterone producing adenoma. Brisbane, Queensland, AUSTRALIA
 Journal of Hypertension Repeating adrenal vein sampling when neither aldosterone/cortisol ratio exceeds peripheral yields a high incidence of aldosterone-producing adenoma --Manuscript Draft-- Manuscript
Journal of Hypertension Repeating adrenal vein sampling when neither aldosterone/cortisol ratio exceeds peripheral yields a high incidence of aldosterone-producing adenoma --Manuscript Draft-- Manuscript
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Adrenal Function. Aldosterone. Analyte Information
 Adrenal Function Aldosterone Analyte Information - 1-2011-01-11 Aldosterone Introduction Aldosterone is a steroid hormone and is the most potent mineralocorticoid in humans. It is secreted by the adrenal
Adrenal Function Aldosterone Analyte Information - 1-2011-01-11 Aldosterone Introduction Aldosterone is a steroid hormone and is the most potent mineralocorticoid in humans. It is secreted by the adrenal
Too Much of a Good Thing: A Woman with Hypertension and Hypokalemia
 Clinical Chemistry 55:12 2093 2097 (2009) Clinical Case Study Too Much of a Good Thing: A Woman with Hypertension and Hypokalemia Sean C. Murphy, Sean Agger, and Petrie M. Rainey * CASE A 64-year-old woman
Clinical Chemistry 55:12 2093 2097 (2009) Clinical Case Study Too Much of a Good Thing: A Woman with Hypertension and Hypokalemia Sean C. Murphy, Sean Agger, and Petrie M. Rainey * CASE A 64-year-old woman
Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism
 Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve
 Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve New Zealand s Woefully Low Diagnostic Rates? / Original Article Authors Walter van der Merwe Veronica van der Merwe
Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve New Zealand s Woefully Low Diagnostic Rates? / Original Article Authors Walter van der Merwe Veronica van der Merwe
Primary Aldosteronism & Implications for Primary Hypertension
 & Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
& Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment
 Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
Diuretic Use in Neonates
 Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx: