Spectrum of Hypertension & Hypokalemia
|
|
|
- Anna Austin
- 6 years ago
- Views:
Transcription



1 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests.
2 OBJECTIVES: 1. Clinical presentation of primary hyperaldosteronism 2. Work up and investigations 3. Treatment of primary hyperaldosteronism 4. Outcomes
3 Case # 1 44 y/o female self referred in 06/2016 for BP management. PMHx: Hx of pre-eclampsia in 2003, 2005 and Did not require meds between pregnancies, however after last delivery needed anti-hypertensives (amlodipine 5mg). MRA Abdomen negative for Renal Artery Stenosis (2006) Normal thyroid function No evidence of Cushing s or pheochromocytoma History of hypokalemia and needed supplements Family Hx of hypertension father in 60s. Started on Edarby-clor 40/12.5mg unable to tolerate due to SE switched to lisinopril 40mg, amlodipine 10mg and HCTZ 25mg.
4 Labs 06/29/2016 BLOOD Normal range Patient Potassium Aldosterone < 21 ng/dl 26 Renin <0.6 URINE Normal range Patient 24 hr aldosterone < 12 mcg/24hr 19.5 mcg/24hr 24 hr sodium mmol/24hr 186 mmol/24hr 24 hr creatinine g/24hr 1.47 g/24hr

5 Radiology CT Abdomen w/ and w/o contrast 07/14/16: - Right adrenal gland lesion measuring 1.6 x 1.0 cm. Measures 10HU on unenhanced CT and is compatible with adenoma.
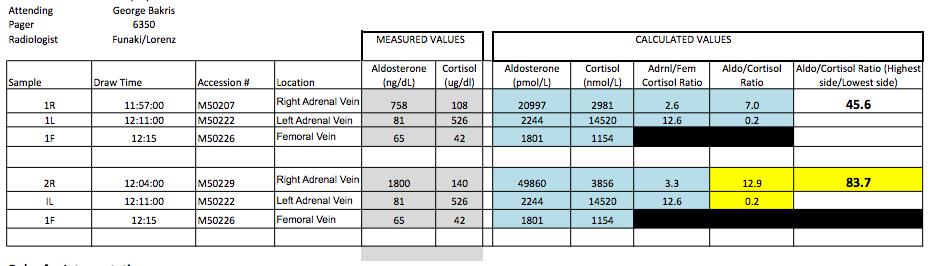
6 AVS 08/29/2016
7 Outcome: Right robotic adrenalectomy 11/10/2016 Pathology: benign adrenal adenoma Able to come off lisinopril and HCTZ. Still on Amlodipine 5mg. BP controlled. Off potassium supplements Potassium 10 days post op 4.7
8 Case # 2 30 y/o female referred by PCP as had Hx of hypertension since age 22 and currently 6 weeks pregnant. Meds switched to labetalol. Delivered without complication at term without pre-eclampsia Switched to amlodipine 5mg after delivery. Had to be switched to diltiazem. Evaluation for primary hyperaldosteronism started as Hx of hypokalemia on and off PMHx: Hypertension, Anxiety. PSHx: none. Exam: non-contributory
9 Labs BLOOD Normal range Patient Potassium (on replacement) as low as 2.8 previously Aldosterone < 21 ng/dl 33 Renin <0.6 URINE Normal range Patient 24 hr aldosterone < 12 mcg/24hr 49 mcg/24hr 24 hr sodium mmol/24hr 153 mmol/24hr 24 hr creatinine mg/24hr 1482 mg/24hr

10 Radiology CT Abdomen w/ and w/o contrast 09/14/2015: - Right adrenal gland lesion measuring 1.3 x 0.6 cm. Measures 28HU pre-contrast, 10 minute delay 33HU and is compatible with lipid poor adrenal adenoma.
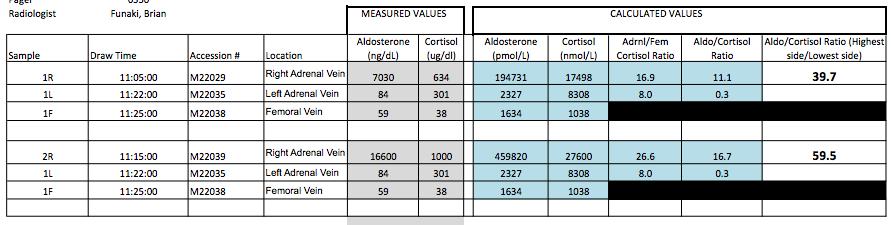
11 AVS 10/03/2016
12 Outcome: Right robotic adrenalectomy 11/10/2016 Pathology: benign adrenal adenoma Able to come off diltiazem and BP controlled off meds Off potassium supplements
13 Hypertension Hypertension: About 70 million American adults (29%) have high blood pressure that s 1 of every 3 adults (1) Only about half (52%) of people with high blood pressure have their condition under control (1) Nearly 1 of 3 American adults have pre-hypertension (1) 90-95% essential or primary hypertension 5-10% secondary hypertension. PA: Consists of 9-13% of cases of secondary hypertension. 1. CDC data 2013 Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the US: National Health and Nutrition Examination Survey, NCHS Data Brief, No Hyattsville, MD: National Center for Health Statistics, Centers for Disease Control and Prevention, US Dept of Health and Human Services, 2013.

14 Primary Hyperaldosternosim ~ Conn s syndrome Hypertension, Hypokalemia, suppressed plasma renin activity (PRA), and increased aldosterone excretion characterize the syndrome of primary aldosteronism, which was first described in 1955 at the University of Michigan. Dr. Jerome Conn, was an endocrinologist whose major work during World War II in the 1940s was focused on the regulation of salt loss in the sweat of subjects exposed to elevated heat and humidity, as was of military concern in the South Pacific at the time.
15 First case: In 1955, Dr. Conn described a case of a 34 year old female patient who had been complaining of seven years of episodic muscle weakness, muscle spasms and cramping of her hands. Dr. Conn hypothesized that endogenous corticoids might have also played a role in this patients pathophysiology, and so was able to demonstrate that the patient had elevated mineralocorticoid levels compared to normotensive controls. The patients condition greatly improved after removal of a 4cm unilateral adrenal tumor
16 Group of disorders in which aldosterone production is inappropriately high, relatively autonomous from the renin-angiotensin system, and nonsuppressible by sodium loading. Such inappropriate production of aldosterone causes cardiovascular damage, suppression of plasma renin, hypertension, sodium retention, and potassium excretion that if prolonged and severe may lead to hypokalemia. PA is commonly caused by an adrenal adenoma, by unilateral or bilateral adrenal hyperplasia, or in rare cases by the inherited condition of GRA. In recent studies, only a minority of patients with PA (9 37%) had hypokalemia (1) Thus, normokalemic hypertension constitutes the most common presentation of the disease, with hypokalemia probably present in only the more severe cases. 1. Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD, Mosso L, Gomez-Sanchez CE, Veglio F, Young Jr WF 2004 Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab 89:
17 Role for adrenal venous sampling in primary aldosteronism. William F. Young Jr., MD, Anthony W. Stanson, MD, Geoffrey B. Thompson, MD, Clive S. Grant, MD, David R. Farley, MD, Jon A. van Heerden, MB, ChBAmerican Association of Endocrine Surgeon. Volume 136, Issue 6, December 2004, Pages
18 Who to evaluate for Primary Hyperaldosteronism??
19 Who to evaluate for PA: According to the Endocrine society guidelines (2016), screen: 1. patients with sustained BP above 150/100 mm Hg on each of three measurements obtained on different days, 2. hypertension (BP140/90 mm Hg) resistant to three conventional antihypertensive drugs (including a diuretic), or 3. controlled BP (140/90 mm Hg) on four or more antihypertensive drugs; 4. hypertension and spontaneous or diuretic-induced hypokalemia; 5. hypertension and adrenal incidentaloma; 6. hypertension and sleep apnea; 7. hypertension and a family history of early onset hypertension or cerebrovascular accident at a young age (40 years); and 8. all hypertensive first-degree relatives of patients with PA. Clinical Practice Guidelines - The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. John W. Funder, Robert M. Carey, Franco Mantero, M. Hassan Murad, Martin Reincke, Hirotaka Shibata, Michael Stowasser, and William F. Young, Jr. March 2016.
:2208 2213.")
20 Work-up: Mini-review: Primary Aldosternosim Changing concepts in diagnosis and treatment. William F. Young, JR. 2005, Endocrinology 144(6):
21 Confirmation testing: 1. ORAL SALT LOADING: - Patients increase their sodium intake to 200 mmol/d ( ~ 6 g/d) for 3 d, verified by 24-h urine sodium content. - Adequate potassium supplementation to maintain plasma potassium in the normal range hr Urinary aldosterone, sodium and creatinine measured. - urine aldosterone >12ug/24hr with urine Na >200mmol/24hr 2. SALINE SUPPRESSION TEST: - Patient stays in the recumbent position for at least 1 h before and during the infusion of 2 liters of 0.9% saline iv over 4 h, starting at h. - Blood samples for renin, aldosterone, cortisol, and plasma potassium are drawn at time zero and after 4 h, with blood pressure and heart rate monitored throughout the test. - Post-infusion plasma aldosterone levels >10ng/ dl suggestive of PA; <5 ng/dl makes the diagnosis unlikely, and values between 5 and 10 ng/dl are indeterminate.
22 3. FLUDROCORTISONE SUPPRESSION: mg oral fludrocortisone every 6 h for 4 d, - potassium supplements (every 6 h) keep K=4.0 mmol/l - NaCl supplements and sufficient dietary salt to maintain a urinary sodium excretion rate of at least 3 mmol/kg body wt. - On day 4, plasma aldosterone and PRA are measured at 1000 h with the patient in the seated posture, and plasma cortisol is measured at 0700 and 1000 h. - Upright plasma aldosterone > 6 ng/dl on day 4 at 1000 h confirms PA, provided PRA is < 1 ng/ml h and plasma cortisol concentration is lower than the value obtained at 0700 h (to exclude a confounding ACTH effect) 4. CAPTOPRIL CHALLENGE TEST: mg captopril orally after sitting or standing for at least 1 h. - Blood samples are drawn for measurement of PRA, PAC & cortisol at time 0, 1 and 2 hr after challenge, with the patient remaining seated during this period. - Plasma aldosterone is normally suppressed by captopril ( 30%). - In patients with PA, it remains elevated and PRA remains suppressed.

23 AVS In 1967, selective adrenal venous sampling (AVS) for aldosterone was first proposed as a test to distinguish between APA and IHA.
24 How to interpret AVS: Step 1: Selectivity Index (SI): Adrenal vein : femoral vein cortisol ratio. - Successful catheterization of the adrenal vein is reflected in a SI 3:1 with co-syntropin [5:1 at U of C] SI 2:1 without co-syntropin. [3:1 at U of C] Step 2: Lateralization index (LI): Highest side adrenal:cortisol ratio of adrenal vein : lowest side adrenal:cortisol ratio. - LI 4:1 denotes a unilateral adenoma - LI 3:1 denotes bilateral adrenal hyperplasia - LI 3 4: grey area.
25 # 1

26 #2:
27 PAH: Primary Adrenal Hyperplasia APA: Aldosterone producing adenoma IHA: idiopathic hyperalodsteronism Role for adrenal venous sampling in primary aldosteronism. William F. Young Jr., MD, Anthony W. Stanson, MD, Geoffrey B. Thompson, MD, Clive S. Grant, MD, David R. Farley, MD, Jon A. van Heerden, MB, ChBAmerican Association of Endocrine Surgeon. Volume 136, Issue 6, December 2004, Pages
28 Who does not need AVS prior to surgery?
29 No need for AVS if: Younger patients (age less than 35 years) with spontaneous hypokalemia, marked aldosterone excess and unilateral adrenal lesions with radiological features consistent with a cortical adenoma on adrenal CT scan may not need AVS before proceeding to unilateral adrenalectomy. Patients not interested in pursuing surgery.
. Overall effective cure rate was 95.5% (resolution of autonomous aldosterone secretion). Hypertension was cured in 41.7% and improved in 46.")
30 J Clin Endocrinol Metab 99: , 2014) Retrospective observational study at the Mayo Clinic. 263 pts over 19 yrs ( ) who underwent unilateral adrenalectomy for treatment of PA. Long term post op f/u in 143 patients (54.45%). Overall effective cure rate was 95.5% (resolution of autonomous aldosterone secretion). Hypertension was cured in 41.7% and improved in 46.5% (BP<140/90 without meds 4.2% patients not cured Adrenal imaging and AVS were concordant to the surgically documented side in 58.6% and 97.1% respectively.
31
32
33 Predictors of improved clinical outcomes after surgery???
34 Predictors of improved clinical outcomes after surgery: 1. 2 or fewer antihypertensive medications, 2. body mass index < or =25 kg/m, 3. duration of hypertension < or =6 years, and 4. female sex. Based on the resulting 4-item aldosteronoma resolution score (ARS), 3 likelihood levels for complete resolution were identified: low (0-1) 27% resolution medium (2-3) 46% resolution high (4) 75% resolution
![1. BMI < 30 had improved outcomes Vs BMI >30 (27.4 Vs 32.7) [p=0.02] 2. Duration of Hypertension (9.1yrs Vs 14.9 yrs) [p=0.02] 3. No.](/docs-images/74/70897404/images/35-0.jpg "of pre-op anti-hypertensives (2.1 Vs 3.7) [p=0.002] 4. Serum creatinine (0.94 Vs 1.32mg/dL) [p=0.016] 5. Pre-op systolic BP (147.5 Vs 159.")
35 1. BMI < 30 had improved outcomes Vs BMI >30 (27.4 Vs 32.7) [p=0.02] 2. Duration of Hypertension (9.1yrs Vs 14.9 yrs) [p=0.02] 3. No. of pre-op anti-hypertensives (2.1 Vs 3.7) [p=0.002] 4. Serum creatinine (0.94 Vs 1.32mg/dL) [p=0.016] 5. Pre-op systolic BP (147.5 Vs 159.7) [p=0.47]

36 Primary hyper-aldosteronism is under diagnosed in pregnancy Review from only reported 47 cases of PA in pregnancy Associated with significant fetal mortality and maternal morbidity and mortality Complications: 5 IUFD; 2 neonatal deaths, 8 IUGR; 6 placental abruptions; 10 cases of pre-eclampsia and 3 cases of HELLP syndrome. Elevated progesterone levels acts as antagonist at mineralocorticoid receptors, hence aldosterone levels rise in parellel with changes in progesterone. Plasma Aldosterone increases by 3-8 fold during gestation, platue in 3 rd trimester. Estrogen stimulates renin secretion, PRA increases by 4 fold at 8wks, 7 fold at term. Fall in ARR during gestation, giving false negatives. An elevated ARR together with PRA less than 4 ng/ml/h make the diagnosis of PA likely.
37 Best time to check for PA is pre pregnancy or 3 months post partum. From above cases: 9 subjects underwent laparoscopic adrenalectomy between weeks (second trimester). Spironolactone not recommended in pregnancy due to antiandrogenic effect on male fetus. Prior to 1980 spiro was used in Tx of HTN, pre-eclampsia, liver disease in pregnancy. 1975: No evidence of anti-androgenic effect in male rats whose mothers were exposed to 400mg of spironolactone from Day 14 of pregnancy to delivery. (1) 1980: study reported de-masculanization of external genitalia of exposed rats (1) Spironolactone used in 6 pregnancies in women with PA: 2 used from prior to conception till first trimester one male neonate showing no evidence of virilization (3) Spironolactone used in Bartter & Gitelman syndrome with no adverse effect in 6 male and 6 female newborns when used in first trimester (3) (1) L.I. Rose, Q. Regestein, J.M. RecklerLack of effect of spironolactone on male genital development. Invest. Urol., 13 (1975), pp (2) A. Hecker, S.H. Hasan, F. NeumannDisturbances in sexual differentiation of rat foetuses following spironolactone treatment. Acta Endocrinol. (Copenh), 95 (1980), pp (3) Primary aldosteronism and pregnancy: Adam Morton. Pregnancy Hypertension, an internation journal of womens cardiovasclar health. Volume 5, Issue 4, October 2015, Pages
38 Amiloride used in 17 pregnancies with severe hypertension, Liddle, Bartter and Gitelman syndromes without adverse effects. Eplerenone used from conception to delivery in 3 pregnancies with Gitelman syndrome with no adverse events. Spironolactone is safe for use during breastfeeding. Primary aldosteronism and pregnancy: Adam Morton. Pregnancy Hypertension, an internation journal of womens cardiovasclar health. Volume 5, Issue 4, October 2015, Pages
39 When to get pregnant after adrenalectomy for APA??
40 No data Recommended to avoid pregnancy for 6 months after surgery. No literature to support it.
41 Familial Hyperaldosteronism Type I (GRA): Autosomal dominant, responsible for 1% of cases of PA. The mutation in patients with GRA is fusion of the promoter region of the gene for CYP11B1 and the coding sequences of CYP11B2, resulting in a CYP11B1/ CYP11B2 chimeric gene. GRA is a form of hyperaldosteronism in which the hypersecretion of aldosterone is dependent upon endogenous ACTH secretion, which activates aldosterone synthesis. Presentation is highly variable, with some patients presenting with normal BP and some characterized by aldosterone excess, suppressed PRA, and hypertension of early onset that is usually severe and refractory to conventional antihypertensive therapies. Genetic testing by either Southern blot or long PCR techniques for the underlying hybrid CYP11B1/ CYP11B2 mutation is sensitive and specific. Genetic testing for GRA should be considered for PA patients with a family history of PA or of strokes at a young age, or with onset at a young age (eg, 20 years). Tx: low dose dexamethasone Clinical Practice Guidelines - The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. John W. Funder, Robert M. Carey, Franco Mantero, M. Hassan Murad, Martin Reincke, Hirotaka Shibata, Michael Stowasser, and William F. Young, Jr
42 Familial Hyperaldosteronism Type II: Autosomal dominant disorder. Unlike FH-I, the hyper-aldosteronism in FH-II does not suppress with dexamethasone, and GRA mutation testing is negative. FH-II families may have APA, IAH, or both and are clinically indistinguishable from patients with apparent nonfamilial PA. Although FH-II is more common than FH-I, accounting for at least 7% of patients with PA in one series, its true prevalence is unknown. The molecular basis for FH-II is unclear, although several linkage analyses have shown an association with chromosomal region 7p22. Few families of European decent. Clinical Practice Guidelines - The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. John W. Funder, Robert M. Carey, Franco Mantero, M. Hassan Murad, Martin Reincke, Hirotaka Shibata, Michael Stowasser, and William F. Young, Jr
43 Familial Hyperaldosteronism Type III: FH-III was first described in a family characterized by severe hypertension in early childhood associated with hyperaldosteronism, hypokalemia, and resistance to antihypertensives requiring bilateral adrenalectomy. The cause of FH-III is a mutation in the KCNJ5 gene encoding the potassium channel Kir 3.4 (potassium inwardly rectifying channel, subfamily 1, member 5). Mutations occur near the selectivity filter for potassium, resulting in increased sodium conductance and cell depolarization. This opens voltage-activated calcium channels leading to increased calcium signaling, followed by increased aldosterone production and cell proliferation. Typically a milder phenotype that other causes. Clinical Practice Guidelines - The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. John W. Funder, Robert M. Carey, Franco Mantero, M. Hassan Murad, Martin Reincke, Hirotaka Shibata, Michael Stowasser, and William F. Young, Jr
44 Thank you!
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Resistant hypertension is defined as blood. Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension.
 Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes
 ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
About 20% of the Canadian population
 Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
ENDOCRINE FORMS OF HYPERTENSION. Michael Stowasser
 ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT?
 ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Primary and secondary hyperaldosteronism. Zsolt Turóczi, M.D. 2nd Department of Internal Medicine
 Primary and secondary hyperaldosteronism Zsolt Turóczi, M.D. 2nd Department of Internal Medicine Adrenal gland Adrenal cortex Carey RM. Primary aldosteronism. Journal of Surgical Oncology 2012: 106; 575
Primary and secondary hyperaldosteronism Zsolt Turóczi, M.D. 2nd Department of Internal Medicine Adrenal gland Adrenal cortex Carey RM. Primary aldosteronism. Journal of Surgical Oncology 2012: 106; 575
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism
 Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin Ratios
 Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
Changes in the clinical manifestations of primary aldosteronism
 ORIGINAL ARTICLE Korean J Intern Med 2014;29:217-225 Changes in the clinical manifestations of primary aldosteronism Sun Hwa Kim, Jae Hee Ahn, Ho Cheol Hong, Hae Yoon Choi, Yoon Jung Kim, Nam Hoon Kim,
ORIGINAL ARTICLE Korean J Intern Med 2014;29:217-225 Changes in the clinical manifestations of primary aldosteronism Sun Hwa Kim, Jae Hee Ahn, Ho Cheol Hong, Hae Yoon Choi, Yoon Jung Kim, Nam Hoon Kim,
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism
 Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Primary Aldosteronism & Implications for Primary Hypertension
 & Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
& Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens
 Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM
 LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM Riccardo Marsili, Pietro Iacconi, Massimo Chiarugi, Giampaolo Bernini*, Alessandra Bacca*, Paolo Miccoli Department
LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM Riccardo Marsili, Pietro Iacconi, Massimo Chiarugi, Giampaolo Bernini*, Alessandra Bacca*, Paolo Miccoli Department
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
--Manuscript Draft-- Primary Aldosteronism; adrenal vein sampling; aldosterone producing adenoma. Brisbane, Queensland, AUSTRALIA
 Journal of Hypertension Repeating adrenal vein sampling when neither aldosterone/cortisol ratio exceeds peripheral yields a high incidence of aldosterone-producing adenoma --Manuscript Draft-- Manuscript
Journal of Hypertension Repeating adrenal vein sampling when neither aldosterone/cortisol ratio exceeds peripheral yields a high incidence of aldosterone-producing adenoma --Manuscript Draft-- Manuscript
Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient
 Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient Testing/ Original Article Author Information Dr Walter van der Merwe MBChB, FRACP, Consultant Nephrologist, Renal
Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient Testing/ Original Article Author Information Dr Walter van der Merwe MBChB, FRACP, Consultant Nephrologist, Renal
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment. Jamie Johnston, MD University of Pittsburgh School of Medicine
 Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Hyperaldosteronism: Conn's Syndrome
 RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
AN INDIVIDUALIZED APPROACH TO THE EVALUATION AND MANAGEMENT OF PRIMARY ALDOSTERONISM
 Review Article AN INDIVIDUALIZED APPROACH TO THE EVALUATION AND MANAGEMENT OF PRIMARY ALDOSTERONISM Anand Vaidya, MD, MMSc 1 ; Carl D. Malchoff, MD, PhD 2 ; Richard J. Auchus, MD, PhD 3 ; on behalf of
Review Article AN INDIVIDUALIZED APPROACH TO THE EVALUATION AND MANAGEMENT OF PRIMARY ALDOSTERONISM Anand Vaidya, MD, MMSc 1 ; Carl D. Malchoff, MD, PhD 2 ; Richard J. Auchus, MD, PhD 3 ; on behalf of
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Adrenal Disorders. Disclosure: I do not have any conflicts of interest
 Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Adrenal Insufficiency During Pregnancy
 Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
Is there a role for Nuclear Medicine in diagnosis and management of patients with primary aldosteronism?
 Is there a role for Nuclear Medicine in diagnosis and management of patients with primary aldosteronism? Abstract Primary aldosteronism (PA) is the most common cause of secondary hypertension. The diagnosis
Is there a role for Nuclear Medicine in diagnosis and management of patients with primary aldosteronism? Abstract Primary aldosteronism (PA) is the most common cause of secondary hypertension. The diagnosis
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
PHARMACEUTICAL INFORMATION AZILSARTAN
 AZEARLY Tablets Each Tablet Contains Azilsartan 20/40/80 mg PHARMACEUTICAL INFORMATION AZILSARTAN Generic name: Azilsartan Chemical name: 2-Ethoxy-1-{[2'-(5-oxo-2,5-dihydro-1,2,4-oxadiazol-3-yl)-4-biphenylyl]methyl}-
AZEARLY Tablets Each Tablet Contains Azilsartan 20/40/80 mg PHARMACEUTICAL INFORMATION AZILSARTAN Generic name: Azilsartan Chemical name: 2-Ethoxy-1-{[2'-(5-oxo-2,5-dihydro-1,2,4-oxadiazol-3-yl)-4-biphenylyl]methyl}-
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
Prognosis of primary aldosteronism in Japan: results from a nationwide epidemiological study
 Endocrine Journal 2013 Or i g i n a l Advance Publication doi: 10.1507/endocrj. EJ13-0353 Prognosis of primary aldosteronism in Japan: results from a nationwide epidemiological study Yoshihiro Miyake 1),
Endocrine Journal 2013 Or i g i n a l Advance Publication doi: 10.1507/endocrj. EJ13-0353 Prognosis of primary aldosteronism in Japan: results from a nationwide epidemiological study Yoshihiro Miyake 1),
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
Odise Cenaj, Harvard Medical School Year III. Gillian Lieberman, MD
 February 2012 Radiologic evaluation of adrenal masses and an atypical radiologic presentation of adrenocortical carcinoma in a patient with primary aldosteronism Odise Cenaj, Harvard Medical School Year
February 2012 Radiologic evaluation of adrenal masses and an atypical radiologic presentation of adrenocortical carcinoma in a patient with primary aldosteronism Odise Cenaj, Harvard Medical School Year
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
4/23/2015. Objectives DISCLOSURES
 2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
Incidental adrenal masses A primary care approach
 CLINICAL Incidental adrenal masses A primary care approach Rasha Gendy, Prem Rashid Background The common use of cross-sectional imaging for the investigation of abdominal and thoracic illness has resulted
CLINICAL Incidental adrenal masses A primary care approach Rasha Gendy, Prem Rashid Background The common use of cross-sectional imaging for the investigation of abdominal and thoracic illness has resulted
Prospective Study on the Prevalence of Secondary Hypertension among Hypertensive Patients Visiting a General Outpatient Clinic in Japan
 193 Original Article Prospective Study on the Prevalence of Secondary Hypertension among Hypertensive Patients Visiting a General Outpatient Clinic in Japan Masao OMURA, Jun SAITO, Kunio YAMAGUCHI, Yukio
193 Original Article Prospective Study on the Prevalence of Secondary Hypertension among Hypertensive Patients Visiting a General Outpatient Clinic in Japan Masao OMURA, Jun SAITO, Kunio YAMAGUCHI, Yukio
PREOPERATIVE DIAGNOSIS AND LOCALIZATION OF ALDOSTERONE-PRODUCING ADENOMA BY ADRENAL VENOUS SAMPLING AFTER ADMINISTRATION OF METOCLOPRAMIDE
 K.D. Wu, T.S. Liao, Y.M. Chen, et al PREOPERATIVE DIAGNOSIS AND LOCALIZATION OF ALDOSTERONE-PRODUCING ADENOMA BY ADRENAL VENOUS SAMPLING AFTER ADMINISTRATION OF METOCLOPRAMIDE Kwan-Dun Wu, Tsou-Song Liao,
K.D. Wu, T.S. Liao, Y.M. Chen, et al PREOPERATIVE DIAGNOSIS AND LOCALIZATION OF ALDOSTERONE-PRODUCING ADENOMA BY ADRENAL VENOUS SAMPLING AFTER ADMINISTRATION OF METOCLOPRAMIDE Kwan-Dun Wu, Tsou-Song Liao,
3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013
 3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013 Presentation Sisters referred by Peds Oncology to Endo clinic for adrenocortical carcinoma screening
3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013 Presentation Sisters referred by Peds Oncology to Endo clinic for adrenocortical carcinoma screening
ACTH stimulation test and computed tomography are useful for differentiating the subtype of primary aldosteronism
 2017, 64 (1), 65-73 Original ACTH stimulation test and computed tomography are useful for differentiating the subtype of primary aldosteronism Ayako Moriya 1), Masaaki Yamamoto 1), Shunsuke Kobayashi 1),
2017, 64 (1), 65-73 Original ACTH stimulation test and computed tomography are useful for differentiating the subtype of primary aldosteronism Ayako Moriya 1), Masaaki Yamamoto 1), Shunsuke Kobayashi 1),
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
A Rare Case of Subclinical Primary Aldosteronism and Subclinical Cushing s Syndrome without Cardiovascular Complications
 Tokai J Exp Clin Med., Vol. 41, No. 1, pp. 35-41, 216 A Rare Case of Subclinical Primary Aldosteronism and Subclinical Cushing s Syndrome without Cardiovascular Complications Natsumi KITAJIMA *1, Toshiro
Tokai J Exp Clin Med., Vol. 41, No. 1, pp. 35-41, 216 A Rare Case of Subclinical Primary Aldosteronism and Subclinical Cushing s Syndrome without Cardiovascular Complications Natsumi KITAJIMA *1, Toshiro
Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting Adenomas
 Case Report Endocrinol Metab 2013;28:133-137 http://dx.doi.org/10.3803/enm.2013.28.2.133 pissn 2093-596X eissn 2093-5978 Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting
Case Report Endocrinol Metab 2013;28:133-137 http://dx.doi.org/10.3803/enm.2013.28.2.133 pissn 2093-596X eissn 2093-5978 Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting
Urinary Kallikrein Excretion in Hypertensive Man
 Urinary Kallikrein Excretion in Hypertensive Man RELATIONSHIPS TO SODIUM INTAKE AND SODIUM-RETAINING STEROIDS By Harry S. Margolius, David Horwttz, John J. Pisano, and Harry R. Kelser ABSTRACT Urinary
Urinary Kallikrein Excretion in Hypertensive Man RELATIONSHIPS TO SODIUM INTAKE AND SODIUM-RETAINING STEROIDS By Harry S. Margolius, David Horwttz, John J. Pisano, and Harry R. Kelser ABSTRACT Urinary
Low renin hypertension
 Review Article Low renin hypertension Manisha Sahay, Rakesh K. Sahay 1 Deparment of Nephrology, 1 Osmania General Hospital, Hyderabad, Andhra Pradesh, India ABSTRACT Low renin hypertension is an important
Review Article Low renin hypertension Manisha Sahay, Rakesh K. Sahay 1 Deparment of Nephrology, 1 Osmania General Hospital, Hyderabad, Andhra Pradesh, India ABSTRACT Low renin hypertension is an important
Patients with primary aldosteronism (PA) are at a higher
 are at a higher") ORIGINAL ARTICLE Endocrine Care Predictors of Decreasing Glomerular Filtration Rate and Prevalence of Chronic Kidney Disease After Treatment of Primary Aldosteronism: Renal Outcome of 213 Cases Yoshitsugu
ORIGINAL ARTICLE Endocrine Care Predictors of Decreasing Glomerular Filtration Rate and Prevalence of Chronic Kidney Disease After Treatment of Primary Aldosteronism: Renal Outcome of 213 Cases Yoshitsugu
Original Article. Roberto FOGARI 1), Paola PRETI 1), Annalisa ZOPPI 1), Andrea RINALDI 1), Elena FOGARI 1), and Amedeo MUGELLINI 1) Introduction
, Paola PRETI 1), Annalisa ZOPPI 1), Andrea RINALDI 1), Elena FOGARI 1), and Amedeo MUGELLINI 1) Introduction") 111 Original Article Hypertens Res Vol.30 (2007) No.2 p.111-117 Prevalence of Primary Aldosteronism among Unselected Hypertensive Patients: A Prospective Study Based on the Use of an Aldosterone/Renin
111 Original Article Hypertens Res Vol.30 (2007) No.2 p.111-117 Prevalence of Primary Aldosteronism among Unselected Hypertensive Patients: A Prospective Study Based on the Use of an Aldosterone/Renin
3 year old boy with puberty. Katie Stanley, MD August 1, 2013
 3 year old boy with puberty Katie Stanley, MD August 1, 2013 Initial presentation 3 and 11/12 year old boy with signs of puberty Presented to outside endocrinologist in 2002 with: Pubic hair since 2.5
3 year old boy with puberty Katie Stanley, MD August 1, 2013 Initial presentation 3 and 11/12 year old boy with signs of puberty Presented to outside endocrinologist in 2002 with: Pubic hair since 2.5
ADRENAL LESIONS 10/09/2012. Adrenal + lesion. Introduction. Common causes. Anatomy. Financial disclosure. Dr. Boraiah Sreeharsha. Nothing to declare
 ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN
 Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
Guidelines for the diagnosis and treatment of primary aldosteronism -The Japan Endocrine Society 2009-
 Endocrine Journal 2011, 58 (9), 711-721 Guidelines for the diagnosis and treatment of primary aldosteronism -The Japan Endocrine Society 2009- Tetsuo Nishikawa 1), Masao Omura 2), Fumitoshi Satoh 3), Hirotaka
Endocrine Journal 2011, 58 (9), 711-721 Guidelines for the diagnosis and treatment of primary aldosteronism -The Japan Endocrine Society 2009- Tetsuo Nishikawa 1), Masao Omura 2), Fumitoshi Satoh 3), Hirotaka
Prevalence and characterization of somatic mutations in Chinese aldosterone-producing adenoma. patients. Supplemental data. First author: Baojun Wang
 Prevalence and characterization of somatic mutations in Chinese aldosterone-producing adenoma patients Supplemental data First author: Baojun Wang Patients and tumor samples A total of 87 patients with
Prevalence and characterization of somatic mutations in Chinese aldosterone-producing adenoma patients Supplemental data First author: Baojun Wang Patients and tumor samples A total of 87 patients with
Long-Term Cardio- and Cerebrovascular Events in Patients With Primary Aldosteronism
 ORIGINAL Endocrine ARTICLE Care Long-Term Cardio- and Cerebrovascular Events in atients With rimary Aldosteronism aolo Mulatero,* Silvia Monticone,* Chiara Bertello,* Andrea Viola, Davide Tizzani, Andrea
ORIGINAL Endocrine ARTICLE Care Long-Term Cardio- and Cerebrovascular Events in atients With rimary Aldosteronism aolo Mulatero,* Silvia Monticone,* Chiara Bertello,* Andrea Viola, Davide Tizzani, Andrea
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
ComprehensivePLUS Hormone Profile with hgh
 OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected