ENDOCRINE FORMS OF HYPERTENSION. Michael Stowasser
|
|
|
- Megan Washington
- 6 years ago
- Views:
Transcription
1 ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia.
2 ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid Forms of Hypertension - Primary aldosteronism - DOC secreting tumors - Hypertensive forms of CAH - 11βHSD deficiency (SAME, licorice) - Mineralocorticoid receptor defects - Liddle syndrome Renovascular HT Pheochromocytoma Cushing Syndrome Acromegaly
3 TUBULE LUMEN K + α β MR Target gene transcription γ Na + Apical Sodium Channel Aldo Basolateral + + Na /K ATPase K + Aldo Na + BLOOD
4 TUBULE LUMEN K + α β MR Target gene transcription γ Na + Apical Sodium Channel DOC Aldo Basolateral + + Na /K ATPase K + DOC Aldo Na + BLOOD
5 TUBULE LUMEN K + α β γ Na + Cortisone MR Target gene transcription Apical Sodium Channel 11βHSD(2) Basolateral + + Na /K ATPase Cortisol DOC Aldo K + Cortisol DOC Aldo Na + BLOOD
6 TUBULE LUMEN K + α β γ Na + Cortisone MR Target gene transcription Apical Sodium Channel 11βHSD(2) Basolateral + + Na /K ATPase Cortisol DOC Aldo K + Cortisol DOC Aldo Na + BLOOD PRIMARY ALDO



7 Conn's first patient with primary aldosteronism, year old female with: Severe hypertension Severe hypokalemia, alkalosis Cured by removal of a 4cm aldosterone-producing adenoma situated in the right adrenal gland
8 Harrison's Principles of Internal Medicine, 1991 " primary aldosteronism accounts for less than 1% of all patients with hypertension " Clinical Hypertension, 1994 " the search for primary aldosteronism need only be undertaken in those with hypokalemia "
9 SCREENING FOR PRIMARY ALDOSTERONISM Aldosterone renin ratio Hiramatsu et al, 1981
10 Use of the Aldo/Renin Ratio at Greenslopes Hospital : Hypertension and hypokalemia : Plus resistant hypertension present: All hypertension
 21% Hypokalemic Total experience: >1400 patients >300 aldo-producing tumors removed (R Gordon & M Stowasser, et al)")
11 PRIMARY ALDOSTERONISM - Greenslopes Hospital (1970-) and Princess Alexandra Hospital (2000-) Patients Diagnosed Per Year Hypokalemic Normokalemic From all HTives screened (aldo/renin) 9.5% of 199 normokalemic hypertensive referrals 12% of 52 hypertensive drug trial volunteers Since 1992: new cases p.a. each confirmed by fludro suppression testing (FST) 21% Hypokalemic Total experience: >1400 patients >300 aldo-producing tumors removed (R Gordon & M Stowasser, et al)
12 PREVALENCE OF PAL - SINCE 1997 Some units reporting increased prevalence: Fardella, et al Gong, et al Widimsky, et al Douma, et al Benchetrit, et al Rossi, et al Mulatero, et al Nishikawa, et al (Chile) (China) (Czech Rep) (Greece) (Israel) (Italy) (Italy) (Japan) Eide, et al Loh, et al Rayner, et al MacDonald, et al Young Jr, et al Gallay, et al Calhoun, et al Schwartz, et al (Norway) (Singapore) (Sth Africa) (UK) (USA) (USA) (USA) (USA) Prevalence rates: mostly 5-15% Proportion normokalemic: %

13 John W. Funder, Robert M. Carey, Carlos Fardella, Celso E. Gomez-Sanchez, Franco Mantero, Michael Stowasser, William F. Young Jr, and Victor M. Montori J Clin Endocrinol Metab Sept 2008; 93:
14 DIAGNOSTIC WORKUP FOR PRIMARY ALDOSTERONSIM Screening - Aldosterone/renin ratio Confirming the Diagnosis - Fludrocortisone suppression test Distinguishing the Subtypes Genetic test for a rare familial form (FH-I) Adrenal CT scanning Adrenal venous sampling
15 Main regulators of ALDO synthesis 1) Renin/angiotensin II 2) Potassium 3) ACTH (Acute stim then suppression) ALDOSTERONE
16 Main regulators of RENIN synthesis 1) Sodium status 2) Renal blood flow 3) SNS (beta) 4) Ang II (-ve feedback) RENIN
17 SCREENING FOR PAL: ALDO/RENIN RATIO FALSE POSITIVES Beta blockers α-methyldopa, clonidine NSAIDs Renal impairment Ageing FALSE NEGATIVES Diuretics CCBs (esp DHPs) ACEIs, ARBs V. low salt intake Renovascular HT Malignant HT Hypokalemia
18 SCREENING FOR PAL: ALDO/RENIN RATIO Correct hypokalemia Unrestricted dietary salt intake Cease diuretics (including spiro) for > 4 weeks Cease beta blockers, α-methyldopa, clonidine, NSAIDs, dihydropyridine CCBs, ACEIs and ARBs for > 2 weeks Substitute with other medications that have a lesser effect on the ratio to maintain HT control - e.g. verapamil slow-release, hydralazine, prazosin Samples collected morning after > 2 hours out of bed Patients seated
19 SCREENING FOR PAL: ALDO/RENIN RATIO NORMAL CUT-OFFS: ALDO units ng/dl RENIN units ng/ml/h (PRA) pmol/l mu/l (DRC)
20 DIAGNOSTIC WORKUP FOR PRIMARY ALDOSTERONSIM Screening - Aldosterone/renin ratio Confirming the Diagnosis - Fludrocortisone suppression test Distinguishing the Subtypes Genetic test for a rare familial form (FH-I) Adrenal CT scanning Adrenal venous sampling
21 DEFINITIVE TESTING FOR PAL - FLUDROCORTISONE SUPPRESSION TEST Plasma aldo response during 4 days of fludrocortisone (0.1 mg 6 hrly) and oral salt loading (Slow Na + 30 mmol tds and high salt diet) Failure of aldo (upright, 1000 h) to suppress to <165 pmol/l by day 4 diagnostic of PAL PROVIDED THAT 1) Renin suppressed 2) K + normal 3) No ACTH rise on morning of collection (indicated by plasma cortisol levels
22 OTHER CONFIRMATORY TESTS FOR PAL Saline infusion test - plasma aldo response during i.v. infusion of normal saline, 2L over 4h Urinary aldo after oral salt loading - 24h urinary aldo following 3 days of oral salt loading (>200 mmol sodium/day)
23 SUBTYPES OF PRIMARY ALDOSTERONISM BILATERAL ADRENAL HYPERPLASIA (BAH) - both adrenals overproducing aldo ALDOSTERONE-PRODUCING ADENOMA (APA) - a benign adrenal tumor overproducing aldo ALDOSTERONE-PRODUCING CARCINOMA - a malignant adrenal tumor overproducing aldo GLUCOCORTICOID-REMEDIABLE ALDOSTERONISM - a rare, genetic form of PAL that runs in families (Familial Hyperaldosteronism Type 1, FH-I)
24 DIAGNOSTIC WORKUP FOR PRIMARY ALDOSTERONSIM Screening - Aldosterone/renin ratio Confirming the Diagnosis - Fludrocortisone suppression test Distinguishing the Subtypes Genetic test for a rare familial form (FH-I) Adrenal CT scanning Adrenal venous sampling
25 FAMILIAL HYPERALDOSTERONISM TYPE I (FH-I, Glucocorticoid-Remediable Aldosteronism) First described Sutherland et al Often early onset of HT, and may result in early death from stroke Hyperaldosteronism and hypertension controlled by glucocorticoids in small doses Hybrid gene - Lifton et al 1992
26 FAMILIAL HYPERALDOSTERONISM TYPE 1 (Glucocorticoid-Remediable Aldosteronism) 11ß-OHase regulatory sequences HYBRID GENE Aldo Synthase coding sequences Regulated by ACTH Encodes Aldo Synthase ALDO Small doses of glucocorticoids, by suppressing ACTH, suppress the hybrid gene and ameliorate PAL and HT



27 FH-I - RESPONSE TO DEX (0.5mg q6h)

28 LONG-PCR TESTING FOR FH-I

29 FH-I - Long PCR NORMAL FH-I Aldo Synthase Hybrid Gene Aldo Synthase Hybrid Gene
30 SUBTYPES OF PRIMARY ALDOSTERONISM BILATERAL ADRENAL HYPERPLASIA (BAH) - both adrenals overproducing aldo ALDOSTERONE-PRODUCING ADENOMA (APA) - a benign adrenal tumor overproducing aldo ALDOSTERONE-PRODUCING CARCINOMA - a malignant adrenal tumor overproducing aldo GLUCOCORTICOID-REMEDIABLE ALDOSTERONISM - a rare, genetic form of PAL that runs in families (Familial Hyperaldosteronism Type 1, FH-I)
31 DIAGNOSTIC WORKUP FOR PRIMARY ALDOSTERONSIM Screening - Aldosterone/renin ratio Confirming the Diagnosis - Fludrocortisone suppression test Distinguishing the Subtypes Genetic test for a rare familial form (FH-I) Adrenal CT scanning Adrenal venous sampling
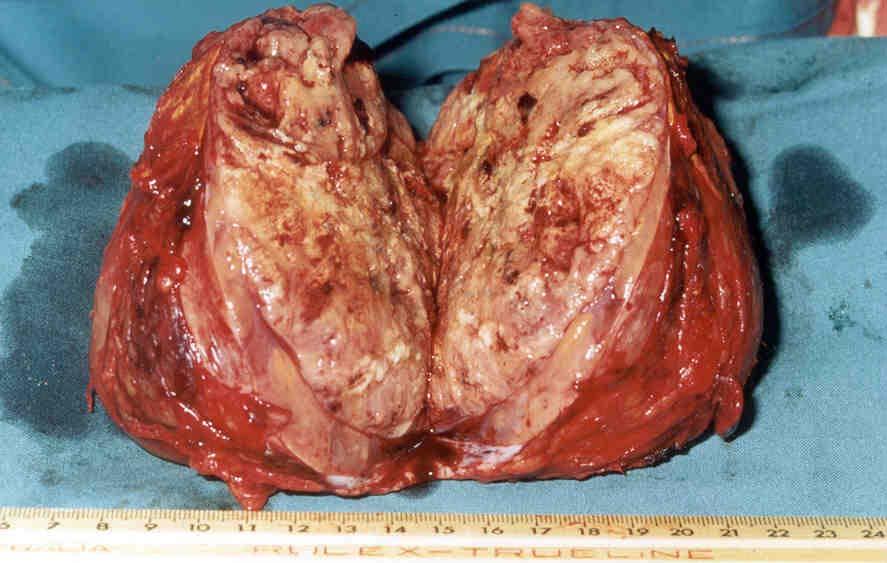
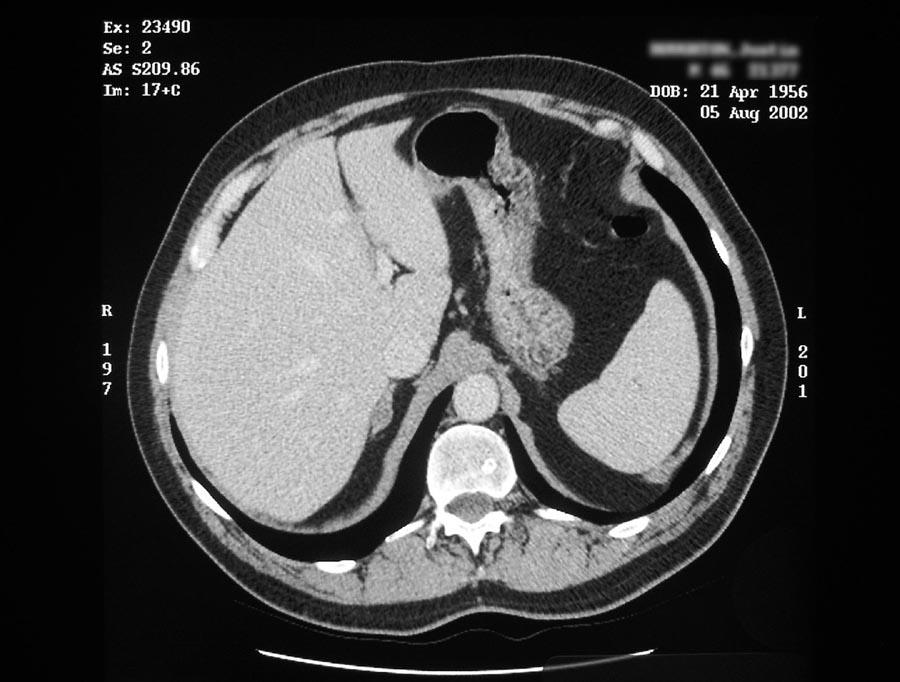
32 ALDOSTERONE-PRODUCING CARCINOMA




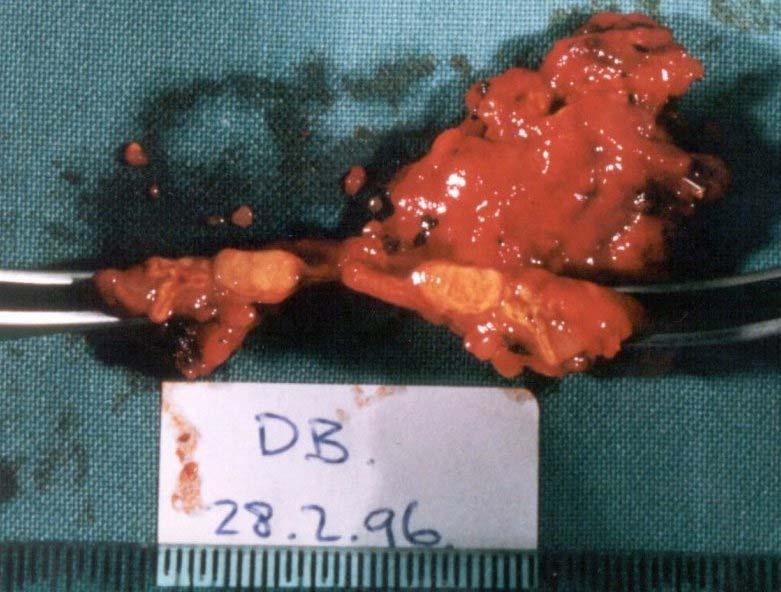
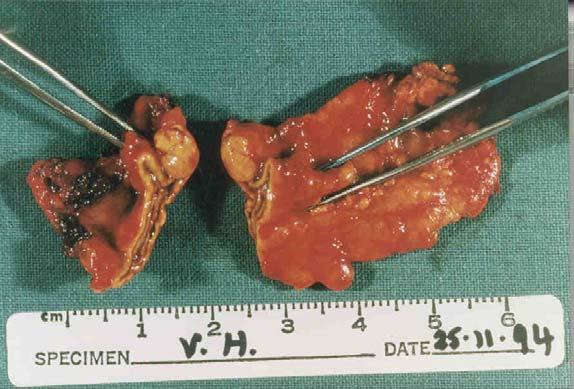
33 Examples of APAs removed from normokalemic patients with PAL In all patients: CT reported as normal; aldo lateralized on AVS; HT cured post-op
34 APAs - MASS ON CT (Jan August 1999) APA Size No. APAs Mass on CT (%) > 1 cm < 1 cm ALL (81%) 14 (24%) 56 (50%)


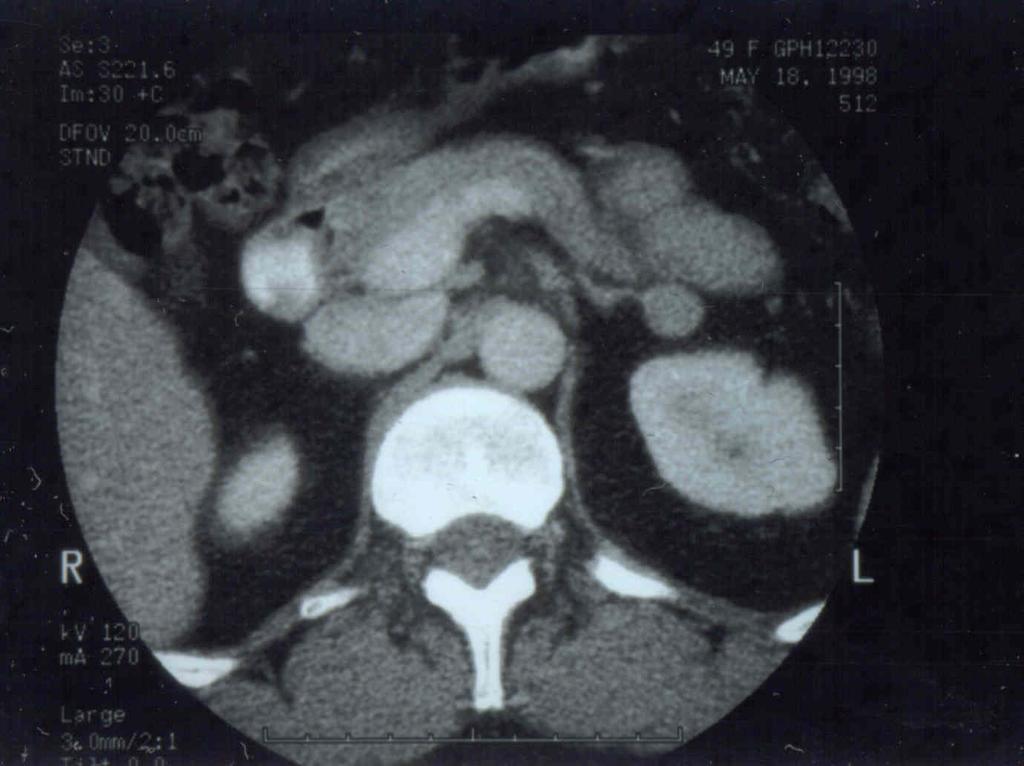
35 ALDOSTERONE- PRODUCING ADENOMA (APA) ADRENAL "INCIDENTALOMA"

36 (a) (b)
37
38 DIFFERENTIATING APA FROM BAH ADRENAL VENOUS SAMPLING - only reliable way to separate APA from BAH and lateralise APAs pre-operatively - perform in ALL patients with PAL (except those found to FH-I by genetic testing) - compare aldo:cortisol ratios in blood collected from each adrenal vein with those in peripheral venous blood
39 WHY MEASURE CORTISOL IN AVS SAMPLES? Cortisol concentrations in AVS samples are an indication of the adequacy of sampling: [Cortisol]ADRENAL VEIN of > 3 = adequate sampling [Cortisol]PERIPHERAL VEIN [Cortisol]ADRENAL VEIN of < 3 = interpretation uncertain [Cortisol]PERIPHERAL VEIN Cortisol concentration corrects for dilution
40 AVS - EXAMPLE 1 Left AV PV Right AV PV Aldo (ng%) Cortisol (ug%) A/C ratio
41 AVS - EXAMPLE 1 Left AV PV Right AV PV Right AV2 Aldo (ng%) Cortisol (ug%) A/C ratio DIAGNOSIS - BILATERAL ALDO PRODUCTION
42 AVS - EXAMPLE 2 Left AV PV Right AV PV Aldo (ng%) Cortisol (ug%) A/C ratio DIAGNOSIS - LEFT APA
43 TREATMENT OF PRIMARY ALDOSTERONISM BILATERAL ADRENAL HYPERPLASIA (BAH) - MR antagonists: spironolactone, eplerenone - epithelial Na + channel blocker: amiloride ALDOSTERONE-PRODUCING TUMOR - laparoscopic adrenalectomy GLUCOCORTICOID-REMEDIABLE ALDOSTERONISM - (Familial Hyperaldosteronism Type 1, FH-I) - small doses of dexamethasone or prednisolone
44 FAMILIAL HYPERALDOSTERONISM TYPE II (FH-II) Gordon, Stowasser et al 1990 Unlike FH-I, not glucocorticoid-remediable Not associated with the hybrid gene mutation patients (3 families); patients (49 families) Clinically, biochemically and morphologically indistinguishable from apparently non-familial PAL Linkage studies have demonstrated linkage in five families with a locus in chromosome 7 (p22)
45 TUBULE LUMEN K + α β γ Na + Cortisone MR Target gene transcription Apical Sodium Channel 11βHSD(2) Basolateral + + Na /K ATPase Cortisol DOC Aldo K + Cortisol DOC Aldo Na + BLOOD DOC TUMOR; CAH

46 HYPERTENSIVE FORMS OF CAH Cholesterol Pregnenolone 17αOHase 17-OH Pregnenolone 17/20 Lyase DHEA Progesterone 17αOHase 17-OH Progesterone 17/20 Lyase Androstenedione DOC 11-deoxycortisol Testosterone 11βOHase 11βOHase Corticosterone Cortisol 18-OH Corticosterone Aldosterone

47 11β-Hydroxylase Deficiency Recessive inheritance Hypertension Adrenal hyperplasia Excessive DOC Hypokalemia Low renin & aldo Virilization Defects in 11β-OHase (C8q) 17α-Hydroxylase Deficiency Recessive inheritance Hypertension Adrenal hyperplasia Excessive DOC Hypokalemia Low renin & aldo Feminization Defects in 17α-OHase (C10q)
48 TUBULE LUMEN K + α β γ Na + Cortisone MR Target gene transcription Apical Sodium Channel 11βHSD(2) Basolateral + + Na /K ATPase Cortisol DOC Aldo K + SAME BLOOD Cortisol DOC Aldo Na +
49 SYNDROME OF APPARENT MINERALOCORTICOID EXCESS (SAME, AME) Clinical description Enzyme defect 11βHSD(2) Raised urinary cortisol metabolites cortisone metabolites Liquorice, carbenoxolone - Recessive - Hypertension - Hypokalemia - Low renin, low aldo Genetic mutations in 11βHSD (C16q22)
50 TUBULE LUMEN MR MUTATION K + α β γ Na + Cortisone MR Target gene transcription Apical Sodium Channel 11βHSD(2) Basolateral + + Na /K ATPase Cortisol DOC Aldo K + Cortisol DOC Aldo Na + BLOOD
51 ACTIVATING MUTATION OF THE MINERALOCORTICOID RECEPTOR Geller, Lifton et al 2000 Hypertension, low aldo and renin Serum potassium usually normal Hypertension exacerbated and hypokalemia induced during pregnancy Point mutation in MR leads to a conformation change in the receptor, which causes constitutive activation, and allows progesterone to act as an agonist Spironolactone also acts as an MR agonist in vitro
52 TUBULE LUMEN K + LIDDLES S α β γ Na + Cortisone MR Target gene transcription Apical Sodium Channel 11βHSD(2) Basolateral + + Na /K ATPase Cortisol DOC Aldo K + Cortisol DOC Aldo Na + BLOOD

53 LIDDLE S SYNDROME Clinical Features Hypertension Hypokalemia Autosomal dominant Renin - low Aldo - low Spironolactone ineffective Responds to low salt and amiloride
54 LIDDLE S SYNDROME Genetic Mutations Beta subunit epithelial sodium channel (C16p) Gamma subunit epithelial sodium channel (C16p) 1999 β and γ subunits truncated loss of intracytoplasmic binding sites for Nedd4, a regulatory protein which normally functions to inactivate sodium channels by promoting endocytosis and degradation
55 TUBULE LUMEN MR MUTATION K + LIDDLES S α β γ Na + Cortisone MR Target gene transcription Apical Sodium Channel 11βHSD(2) Basolateral + + Na /K ATPase Cortisol DOC Aldo K + SAME BLOOD Cortisol DOC Aldo DOC TUMOR; CAH Na + PRIMARY ALDO

56
57
58 DIAGNOSTIC WORKUP FOR RENOVASCULAR HYPERTENSION Who to Screen? - Recent onset HT, worsening HT, resistant HT - Worsening renal function - Deterioration in renal function with ACEI, ARB - Risk factors for PVD; vasc disease elsewhere - Young women -?All hypertension?
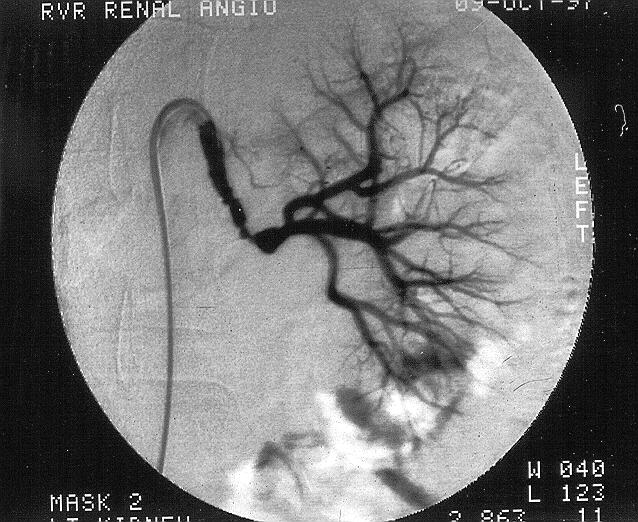
59 DIAGNOSTIC WORKUP FOR RENOVASCULAR HYPERTENSION How to Screen - Renal artery duplex U/S - Renal isotope scan (DTPA or MAG3) - CT renal angiography Confirming the Diagnosis - Renal venous renin ratios - Renal angiography
60 RENAL ARTERY DUPLEX ULTRASOUND RIGHT LEFT (N) Renal Length (cm) PSV (m/s) - Prox -Mid -Distal (<2.0) (<2.0) (<2.0) Renal Aortic Ratio (RAR) (<3.5) Acceleration Time (msec) (<70) Resistive Index (%) (<70) Consistent with a haemodynamically significant L RAS of >60%...
61
62 Renal Venous Renin Ratios Assess functional significance of RAS lesions When performed appropriately, results are highly predictive of BP response to revascularization or nephrectomy When performed without regard to factors that can complicate the interpretation of the results, high frequency of false negative results Less invasive, fewer complications than renal angiography argues for doing RVRRs first
 Right RV renin level is no higher than peripheral (i.e. suppressed) Results consistent with a left renovascular cause of hypertension")
63 Renal Venous Renin Ratio Results in a Patient with Bilateral Renal Artery Stenosis Renin levels (mu/l) Peripheral vein Right Renal V Left Renal V L/R Ratio Early Basal Post oral captopril Left/right RV renin ratio is significant (>1.5) Right RV renin level is no higher than peripheral (i.e. suppressed) Results consistent with a left renovascular cause of hypertension
64 Treatment of Renovascular HT 1) How to Treat? PTRA/stent Operative Medical Rx: - embolism, dissection, rupture - recurrence treat risk factors - endarterectomy, bypass, nephrectomy - solitary kidney or bilat RAS: avoid ACEI or ARB - treat CV risk factors 2) How to Decide? - BPs, side FX, renal function, age, comorbidities, local expertise, patient s wishes - Renovascular group - physician(s) interested in HT, nephrologist(s), vascular physician(s), vascular surgeon(s), interventional radiologist(s) Patients decides -

65 PHEOCHROMOCYTOMA
66 PHEOCHROMOCYTOMA Rare, but important not to miss (50% MR if detected at time of operation; Preoperative α and β blockade protects) Typical paroxysms in only 50% Screen by 24h urinary catechols - correct for creatinine excretion - others (plasma catechols or metanephrines; urinary metanephrines) Further investigations: - Clonidine suppression testing (plasma or urinary) - Contrast CT (α and β block first) or MRI (bright on T2) - MIBG (other scans: octreotide, PET with 6[F 18 ]fluorodopamine) - Consider familial conditions: MEN2 - RET Familial pheo - SDHD (succ dehydrog) VHL - VHL SDHB NF1 - NF1
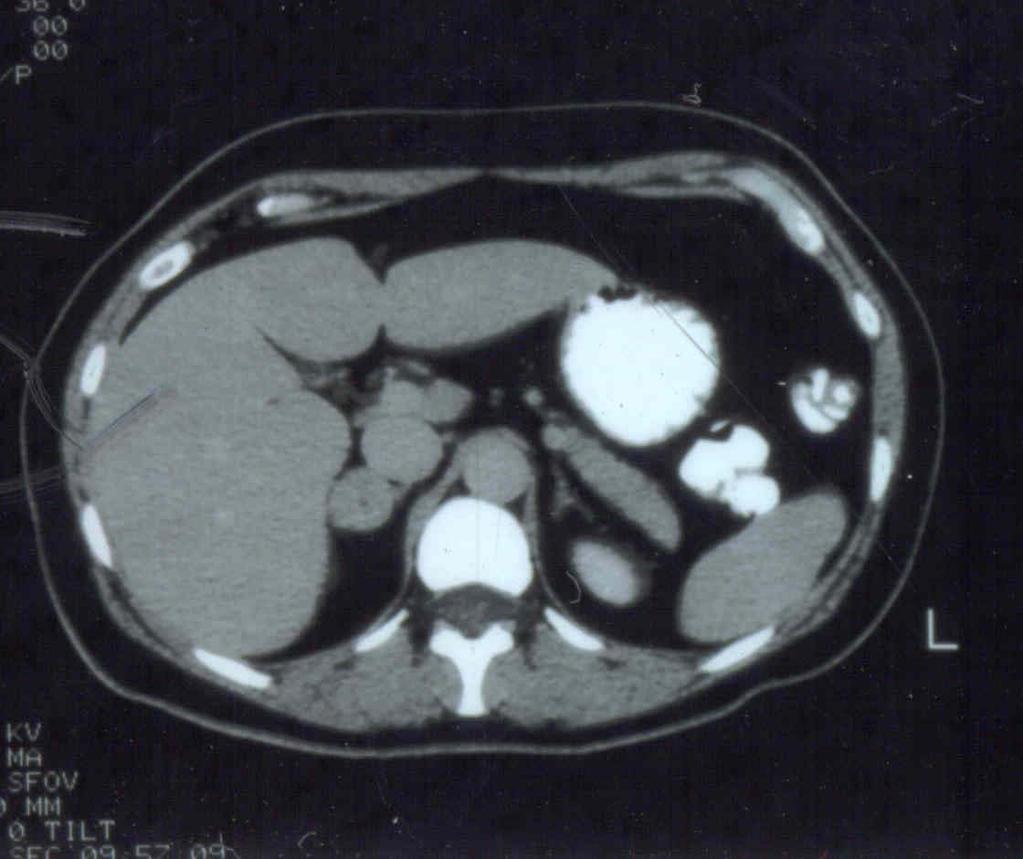
67 PHEOCHROMOCYTOMA - CT
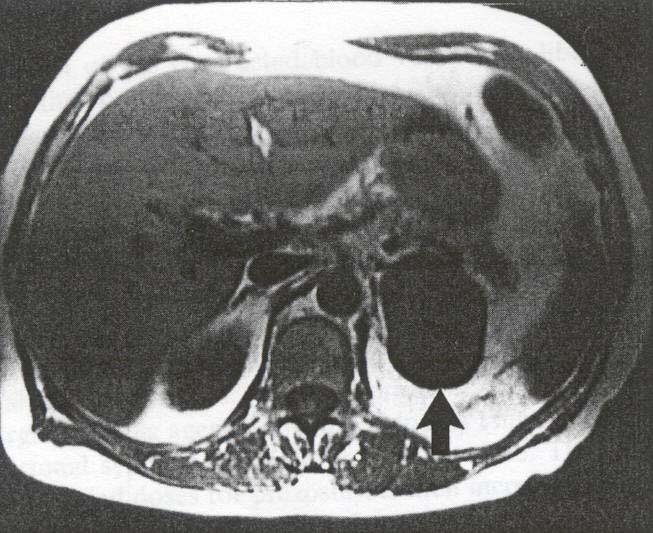
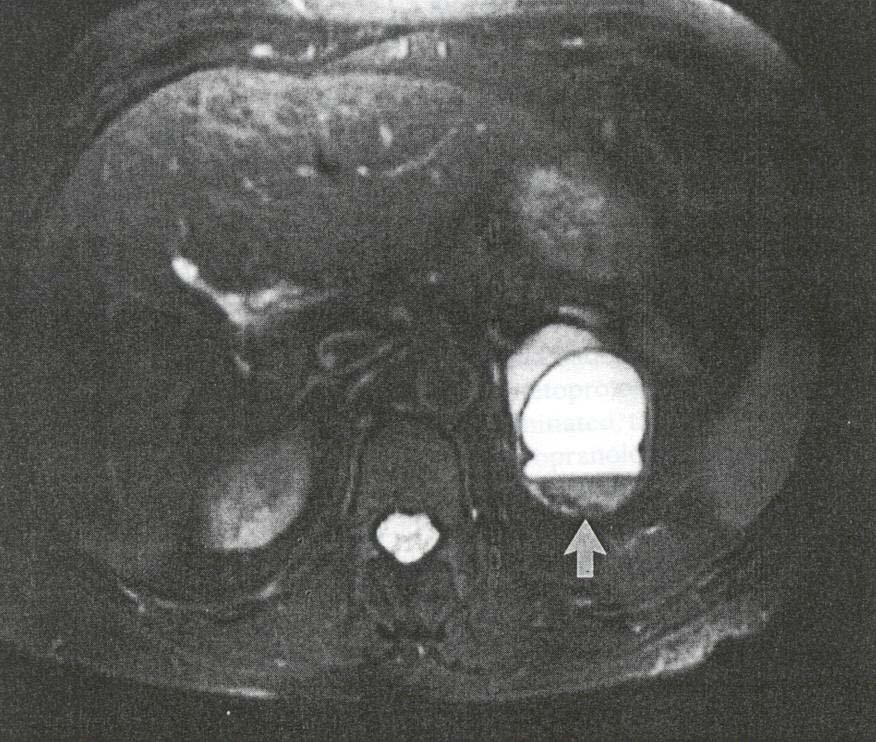
68 PHEOCHROMOCYTOMA - MRI T1 T2
69
70
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Spectrum of Hypertension & Hypokalemia
 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Primary and secondary hyperaldosteronism. Zsolt Turóczi, M.D. 2nd Department of Internal Medicine
 Primary and secondary hyperaldosteronism Zsolt Turóczi, M.D. 2nd Department of Internal Medicine Adrenal gland Adrenal cortex Carey RM. Primary aldosteronism. Journal of Surgical Oncology 2012: 106; 575
Primary and secondary hyperaldosteronism Zsolt Turóczi, M.D. 2nd Department of Internal Medicine Adrenal gland Adrenal cortex Carey RM. Primary aldosteronism. Journal of Surgical Oncology 2012: 106; 575
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Mendelian Hypertension: Clinical Implications
 Mendelian Hypertension: Clinical Implications Anna Dominiczak MD Regius Professor of Medicine Valencia, ICHCA, 2018 Monogenic Hypertension & Hypotension Gitelman Syndrome Gordon Syndrome Modified from
Mendelian Hypertension: Clinical Implications Anna Dominiczak MD Regius Professor of Medicine Valencia, ICHCA, 2018 Monogenic Hypertension & Hypotension Gitelman Syndrome Gordon Syndrome Modified from
Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient
 Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient Testing/ Original Article Author Information Dr Walter van der Merwe MBChB, FRACP, Consultant Nephrologist, Renal
Outpatient Fludrocortisone Suppression Test: A Safe and Effective Alternative to Inpatient Testing/ Original Article Author Information Dr Walter van der Merwe MBChB, FRACP, Consultant Nephrologist, Renal
--Manuscript Draft-- Primary Aldosteronism; adrenal vein sampling; aldosterone producing adenoma. Brisbane, Queensland, AUSTRALIA
 Journal of Hypertension Repeating adrenal vein sampling when neither aldosterone/cortisol ratio exceeds peripheral yields a high incidence of aldosterone-producing adenoma --Manuscript Draft-- Manuscript
Journal of Hypertension Repeating adrenal vein sampling when neither aldosterone/cortisol ratio exceeds peripheral yields a high incidence of aldosterone-producing adenoma --Manuscript Draft-- Manuscript
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Low renin hypertension
 Review Article Low renin hypertension Manisha Sahay, Rakesh K. Sahay 1 Deparment of Nephrology, 1 Osmania General Hospital, Hyderabad, Andhra Pradesh, India ABSTRACT Low renin hypertension is an important
Review Article Low renin hypertension Manisha Sahay, Rakesh K. Sahay 1 Deparment of Nephrology, 1 Osmania General Hospital, Hyderabad, Andhra Pradesh, India ABSTRACT Low renin hypertension is an important
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve
 Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve New Zealand s Woefully Low Diagnostic Rates? / Original Article Authors Walter van der Merwe Veronica van der Merwe
Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve New Zealand s Woefully Low Diagnostic Rates? / Original Article Authors Walter van der Merwe Veronica van der Merwe
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
4/23/2015. Objectives DISCLOSURES
 2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
Resistant hypertension is defined as blood. Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension.
 Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
About 20% of the Canadian population
 Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes
 ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Screening for Endocrine Hypertension: An Endocrine Society Scientific Statement
 SCIENTIFIC STATEMENT Screening for Endocrine Hypertension: An Endocrine Society Scientific Statement William F. Young Jr., 1 David A. Calhoun, 3 Jacques W.M. Lenders, 4,5 Michael Stowasser, 6,7,8 and Stephen
SCIENTIFIC STATEMENT Screening for Endocrine Hypertension: An Endocrine Society Scientific Statement William F. Young Jr., 1 David A. Calhoun, 3 Jacques W.M. Lenders, 4,5 Michael Stowasser, 6,7,8 and Stephen
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
PHEOCHROMOCYTOMA. Anita Chiu, MD Kings County Hospital Center January 13, 2011
 PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
Too Much of a Good Thing: A Woman with Hypertension and Hypokalemia
 Clinical Chemistry 55:12 2093 2097 (2009) Clinical Case Study Too Much of a Good Thing: A Woman with Hypertension and Hypokalemia Sean C. Murphy, Sean Agger, and Petrie M. Rainey * CASE A 64-year-old woman
Clinical Chemistry 55:12 2093 2097 (2009) Clinical Case Study Too Much of a Good Thing: A Woman with Hypertension and Hypokalemia Sean C. Murphy, Sean Agger, and Petrie M. Rainey * CASE A 64-year-old woman
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
Adrenal Disorders. Disclosure: I do not have any conflicts of interest
 Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT?
 ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
Hyperaldosteronism: recent concepts, diagnosis, and management
 Postgrad Med J 2001;77:639 644 639 Clinical Pharmacology Unit, University of Cambridge, Box 110, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK RFoo K M O Shaughnessy M J Brown Correspondence to: Dr Foo
Postgrad Med J 2001;77:639 644 639 Clinical Pharmacology Unit, University of Cambridge, Box 110, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK RFoo K M O Shaughnessy M J Brown Correspondence to: Dr Foo
MedKorat Endocrine Day 2018 Approach to common adrenal disorder
 MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
Secondary hypertension is defined as being
 Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens
 Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
Primary Aldosteronism & Implications for Primary Hypertension
 & Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
& Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life!
 74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
312 Index. Autonomic nervous system. See Sympathetic nervous system (SNS) Autonomous aldosterone secretion (AAS),
 Autonomous aldosterone secretion (AAS),") A Acromegaly clinical evidence, hypertension nature, 160 161 prevalence, 155 158 resolution, 158 160 hypertension mechanisms brain natriuretic peptide, 162 163 cardiovascular effects, 164 165 GH or IGF-I
A Acromegaly clinical evidence, hypertension nature, 160 161 prevalence, 155 158 resolution, 158 160 hypertension mechanisms brain natriuretic peptide, 162 163 cardiovascular effects, 164 165 GH or IGF-I
Diagnosing endocrine hypertension: a practical approach
 Nephrology 22 (2017) 663 677 Review Article Diagnosing endocrine hypertension: a practical approach JUN YANG, 1,2 JIMMY SHEN 1,2 and PETER J. FULLER 1,2 1 Centre for Endocrinology and Metabolism, Hudson
Nephrology 22 (2017) 663 677 Review Article Diagnosing endocrine hypertension: a practical approach JUN YANG, 1,2 JIMMY SHEN 1,2 and PETER J. FULLER 1,2 1 Centre for Endocrinology and Metabolism, Hudson
ComprehensivePLUS Hormone Profile with hgh
 OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
Hypertension: Who and How (and Why) to Investigate. Jessica Triay Andy Levy
 to Investigate. Jessica Triay Andy Levy") Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
My favorite hypertensive patients. Entertaining you is Friedrich C. Luft
 My favorite hypertensive patients Entertaining you is Friedrich C. Luft 37 year-old woman with fairly severe hypertension Negative family history, normal pregnancy Receives HCTZ, Amlodipine, and Valsartan
My favorite hypertensive patients Entertaining you is Friedrich C. Luft 37 year-old woman with fairly severe hypertension Negative family history, normal pregnancy Receives HCTZ, Amlodipine, and Valsartan
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism
 Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM
 LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM Riccardo Marsili, Pietro Iacconi, Massimo Chiarugi, Giampaolo Bernini*, Alessandra Bacca*, Paolo Miccoli Department
LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM Riccardo Marsili, Pietro Iacconi, Massimo Chiarugi, Giampaolo Bernini*, Alessandra Bacca*, Paolo Miccoli Department
Original Article. Roberto FOGARI 1), Paola PRETI 1), Annalisa ZOPPI 1), Andrea RINALDI 1), Elena FOGARI 1), and Amedeo MUGELLINI 1) Introduction
, Paola PRETI 1), Annalisa ZOPPI 1), Andrea RINALDI 1), Elena FOGARI 1), and Amedeo MUGELLINI 1) Introduction") 111 Original Article Hypertens Res Vol.30 (2007) No.2 p.111-117 Prevalence of Primary Aldosteronism among Unselected Hypertensive Patients: A Prospective Study Based on the Use of an Aldosterone/Renin
111 Original Article Hypertens Res Vol.30 (2007) No.2 p.111-117 Prevalence of Primary Aldosteronism among Unselected Hypertensive Patients: A Prospective Study Based on the Use of an Aldosterone/Renin
Adrenal Steroids Mineralocorticoids & Glucocorticoids. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine The Jordan University April 2014
 Adrenal Steroids Mineralocorticoids & Glucocorticoids Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine The Jordan University April 2014 Medulla (E, NE) Adrenal Gland Cortex Mineralocorticoids (Aldosterone)
Adrenal Steroids Mineralocorticoids & Glucocorticoids Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine The Jordan University April 2014 Medulla (E, NE) Adrenal Gland Cortex Mineralocorticoids (Aldosterone)
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment. Jamie Johnston, MD University of Pittsburgh School of Medicine
 Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin Ratios
 Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
The real picture. Prorenin (Renin) PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009
 PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009") The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD
The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD
Odise Cenaj, Harvard Medical School Year III. Gillian Lieberman, MD
 February 2012 Radiologic evaluation of adrenal masses and an atypical radiologic presentation of adrenocortical carcinoma in a patient with primary aldosteronism Odise Cenaj, Harvard Medical School Year
February 2012 Radiologic evaluation of adrenal masses and an atypical radiologic presentation of adrenocortical carcinoma in a patient with primary aldosteronism Odise Cenaj, Harvard Medical School Year
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Inquadramento Clinico dell IncIdentaloma SurrenalIco
 Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
RECURRENT ADRENAL DISEASE. Megan Applewhite Endorama 2/19/2015 SR , SC
 RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
Adrenal Function. Aldosterone. Analyte Information
 Adrenal Function Aldosterone Analyte Information - 1-2011-01-11 Aldosterone Introduction Aldosterone is a steroid hormone and is the most potent mineralocorticoid in humans. It is secreted by the adrenal
Adrenal Function Aldosterone Analyte Information - 1-2011-01-11 Aldosterone Introduction Aldosterone is a steroid hormone and is the most potent mineralocorticoid in humans. It is secreted by the adrenal
ADRENAL GLANDS HORMONES
 ADRNAL GLANDS HORMONS Glands Cortex 80% mesoderm Mineralococorticoids Glucocorticoids (phenylethanolamine N- methyl transferase) A Sex Hormones Catecholamines Medulla 20% PNMT, N neuroectoderm N PNMT V
ADRNAL GLANDS HORMONS Glands Cortex 80% mesoderm Mineralococorticoids Glucocorticoids (phenylethanolamine N- methyl transferase) A Sex Hormones Catecholamines Medulla 20% PNMT, N neuroectoderm N PNMT V
pharmacology sheet #9 Adrenal Steroids Mineral corticoids & Glucocorticoids
 Adrenal Steroids Mineral corticoids & Glucocorticoids Extra notes : Slide 2: - All Steroids are synthesized in the adrenal gland and secreted from it, It consists of an outer cortex and an inner medulla.
Adrenal Steroids Mineral corticoids & Glucocorticoids Extra notes : Slide 2: - All Steroids are synthesized in the adrenal gland and secreted from it, It consists of an outer cortex and an inner medulla.
Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism
 Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Secondary hypertension How to approach?
 Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Getting BP to goal: Virginia L. Hood MB.BS, MPH, FACP
 Getting BP to goal: Virginia L. Hood MB.BS, MPH, FACP Objectives: Outline pathophysiological processes that sustain high BP Design individual treatment strategies for BP not at goal Facilitate patient
Getting BP to goal: Virginia L. Hood MB.BS, MPH, FACP Objectives: Outline pathophysiological processes that sustain high BP Design individual treatment strategies for BP not at goal Facilitate patient
Monogenic forms of hypertension
 Eur J Pediatr (2012) 171:1433 1439 DOI 10.1007/s00431-011-1440-7 REVIEW Monogenic forms of hypertension Giacomo Domenico Simonetti & Markus G. Mohaupt & Mario G. Bianchetti Received: 29 December 2010 /
Eur J Pediatr (2012) 171:1433 1439 DOI 10.1007/s00431-011-1440-7 REVIEW Monogenic forms of hypertension Giacomo Domenico Simonetti & Markus G. Mohaupt & Mario G. Bianchetti Received: 29 December 2010 /