Pediatric Otolaryngology for Anesthetists followed by the delightful Airway Disorders in Infants and Children
|
|
|
- Ross Kelley
- 5 years ago
- Views:
Transcription

1 Pediatric Otolaryngology for Anesthetists followed by the delightful Airway Disorders in Infants and Children Andrew M. Shapiro, MD Private Practice, Pediatric Otolaryngology Clinical Associate Professor of Surgery Pennsylvania State University College of Medicine
2 What does a pediatric otolaryngologist do? Inflammatory, congenital and neoplastic disorders involving the head and neck Simple surgeries in fairly healthy kids Big surgeries in fairly healthy kids Simple surgeries in sick kids Big surgeries in sick kids Ear surgery Nasal and sinus surgery Airway surgery Pharyngeal surgery Craniofacial surgery Tumors and congenital anomalies of the head and neck
3 Organization Emphasize that there are distinct qualities required when caring for children Understand the anesthetic implications of otolaryngologic surgery Understand special situations and patient circumstances Review significant ENT airway conditions


4 Characteristics of pediatric anesthesia Laryngospasm, bronchospasm, concurrent illnesses Physiologic differences Higher metabolic rate O2 requirement Temperature management Chest wall compliance High closing volumes Evolving psychological status must be appreciated from neonates to adolescents Dental

5 Characteristics of Pediatric Otolaryngology Patients Healthy PedENT patients are often sick on the day of surgery Congestion, runny nose, cough a case cancelled is not a case done Sick PedENT patients tend to have chronic lung disease from prematurity, aspiration, cystic fibrosis, or reactive airway disease


6 Points of convergence The surgeon and the anesthetist are a TEAM (and I m not just saying that!) Maintain good surgical access while preserving the ability to sustain ventilation (or vice versa)
7 Otologic Cases Myringotomy and tube insertions Most common procedure under GA Mask anesthetic Older children may benefit from IV/LMA Premed? Narcotic? Tympanoplasty/tympanomastoidectomy No muscle relaxant during procedure No nitrous oxide Secure tubes and IV s; lots of turning during case

8 Nasal and Paranasal sinus surgery Expect secretions and blood Expect a generous helping of vasoconstrictors Control blood pressure Expect a touchy airway
9 Anatomic Classification Supraglottic Nose Choanal atresia NOWCA Craniofacial Dysmorphology Pierre Robin Syndrome Treacher collins Aperts Crouzons Moebius Macroglossia Beckwith Wiedemann Syndrome Down s Syndrome Tumors Hemangioma Neuroblastoma Laryngomalacia Glottic Vocal cord paralysis Tumors and cysts Laryngoceles Papillomatosis Cystic hygroma Laryngoceles Atresia Webs Subglottic Stenosis Webs Atresia Tumors Hemangioma Cystic Hygroma Cysts Trachea Tracheomalacia Stenosis Cyst Atresia Extrinsic Goiter Vascular Ring Hemangioma Cystic hygroma Teratoma Mediastinal masses
10 Introduction The Pediatric Airway Anatomy Nasal/Pharyngeal Obligate Nosebreathing Laryngeal Supraglottis Glottis Subglottis Cricoid Upper trachea

11 The Nose and Pharynx Anatomy Nasal Cavities Pharynx Nasopharynx Oropharynx Hypopharynx
12 Obligate Nosebreathing
 Often worst when asleep Often improved by positioning Neck")
13 Obstruction at the Pharyngeal Level Stertor (vs. stridor) Often worst when asleep Often improved by positioning Neck extension, sniffing position


14 Tonsils and adenoids Chronic tonsillitis Tonsillar hyperplasia OSA 2% incidence. 10%SDB Peaks 2-5 years old Second peak in adolescence Medical treatment Weight loss Management of infection CPAP Surgical therapy T/A, UPPP Highly effective in normal children
15 T & A: techniques Tonsillectomy Cold Guillotine Dissection and snare Microdebrider Hot Cautery Bipolar cautery Laser Coblation Adenoidectomy Curette Cautery Microdebrider Adjunctive measures Steroids Local Anesthetics Analgesics Antibiotics Antiemetics
16 Higher risk tonsillectomy Age < 3 years Documented profound OSA Neuromuscular disorders Chromosomal anomalies Craniofacial/airway disorders Recent upper respiratory infection Bleeding disorder Active infection or peritonsillar abscess Severe obesity
17 Upper airway obstruction in neurologically impaired children Hypotonia reduces predictability of T&A Reasonable approach if significant adenotonsillar hypertrophy is present UPPP? Kershner et al int J ped oto 2002 tracheotomy vs. salivary diversion, laryngeal diversion, supraglottoplasty, midfacial and maxillary advancements BiPAP/CPAP Increased perioperative morbidity Individualized treatment - no reasonable studies to clearly delineate best treatment options
18 Postoperative problems can be minimized by anesthetic techniques Apnea Laryngospasm Postobstructive pulmonary edema Bleeding Judicious narcotics Local anesthetic Steroids/Antiemetics Propofol Timing of extubation Immediate gentle positive pressure

19 Now, the real reason I m here
20 Introduction The Pediatric Airway Anatomy Nasal/Pharyngeal Obligate Nosebreathing Laryngeal Supraglottis Glottis Subglottis Cricoid Upper trachea
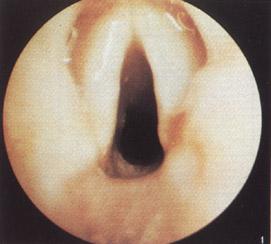
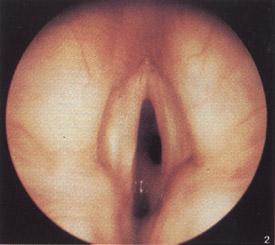
21 Stridor Definition Distinguish from stertor Causes Laryngomalacia Vocal cord paralysis Subglottis stenosis
22 Cross Sectional Airway Diameter Adult 1mm edema = 81% of normal area 20mm 5mm Term Newborn 1mm edema = 44% of normal area
23 Clinical presentation Failed extubation attempts in NICU Stridor Recurrent croup Progressive respiratory failure with stridor Feeding difficulties Failure to thrive Persistent cough Tracheotomy

24 Evaluation History Details of extubation attempts Presence, absence, and characteristics of stridor Onset/Progression Impact of position Nature of cry Feeding abnormalities Prior airway interventions Cardiopulmonary status Term or premature Apgar Birth weight/weight gain Other medical problems Physical examination Imaging Endoscopy
25 Evaluation History Physical examination Complete head and neck examination Craniofacial disorders, retrognathia, nasal obstruction, laryngomalacia, vocal cord paralysis Body Habitus Degree of dyspnea Quality of stridor Changes with position, activity Cry/Voice Auscultation of chest Imaging Endoscopy

26 Evaluation History Physical examination Imaging Hi KV AP and Lateral plain films Airway flouroscopy/barium Swallow MRI in patients with suspected vascular/mediastinal pathology Endoscopy

27 Evaluation History Physical examination Imaging Endoscopy Flexible Need for sedation and inability to control airway and ventilation Useful for proximal airway evaluation at bedside or as outpatient Distal airway evaluation in intubated patients Rigid Spontaneous ventilation Microlaryngoscopy Webs, glottic scarring, interarytenoid adhesions, fixation or paralysis Subglottis Size, maturity, length, stomal site Remainder of tracheobronchial tree Sizing of airway

28 Airway Endoscopy-Stages 1. Preparation and Communication a) Equipment b) Monitoring 2. Induction 3. Diagnostic Laryngoscopy and topical anesthetic 4. Diagnostic Suspension laryngoscopy Controlled airway for microscopy or bronchoscopy and Diagnostic Bronchoscopy 5. Therapeutic intervention
29 Anesthesia for airway endoscopy Clear communication essential Avoid jet in young children Techniques Apneic technique Spontaneous ventilation in young children Topical anesthetic? In older children (5-10 years) relaxant with controlled ventilation NEVER ABOLISH SPONTANEOUS RESPIRATION UNLESS AN ALTERNATIVE AIRWAY IS ASSURED
30 Anesthesia for Laser Endoscopy Assure patient and staff protection Have a fire plan of action Minimize FiO2 Avoid adding fuel to the fire when possible Endotracheal tubes/packs Apneic ventilation Relaxant extends working time, accuracy
31 Anatomic Classification Supraglottic Nose Choanal atresia NOWCA Craniofacial Dysmorphology Pierre Robin Syndrome Treacher collins Aperts Crouzons Moebius Macroglossia Beckwith Wiedemann Syndrome Down s Syndrome Tumors Hemangioma Neuroblastoma Laryngomalacia Glottic Vocal cord paralysis Tumors and cysts Laryngoceles Papillomatosis Cystic hygroma Laryngoceles Atresia Webs Subglottic Stenosis Webs Atresia Tumors Hemangioma Cystic Hygroma Cysts Trachea Tracheomalacia Stenosis Cyst Atresia Extrinsic Goiter Vascular Ring Hemangioma Cystic hygroma Teratoma Mediastinal masses



32 Nasal Disorders Choanal Atresia Obstruction in posterior nasal cavity 90% bony, 10% membraneous Bilateral in 40%; other congenital anomalies in 50% Failure to pass #6 catheter Unilateral- observe Bilateral Oral airway; gavage; repair; tracheostomy



33 Nasal Disorders Pyriform Aperture Stenosis Hairy polyp Encephalocele/Glioma

34 Craniofacial disorders Pierre Robin Syndrome Micrognathia, cleft palate, glossoptosis Respiratory distress worst with feeding Nasopharyngeal airway Improvement with mandibular growth Distraction osteogenesis

35 Craniofacial Disorders Treacher Collins Sydrome Autosomal Dominant Findings Antimongoloid slant lower lid coloboma auricular malformation Malar/mandibular hypoplasia

36 Craniofacial Disorders Crouzon s Syndrome Midfacial hypoplasia Glossoptosis, posterior pharyngeal compromise

37 Break time!

38 Laryngeal Disorders
39 Laryngomalacia Most common cause of stridor in neonate Etiology: collapse of supraglottic structures into airway lumen, creating turbulent flow and obstruction Idiopathic--Anatomy vs. innervation GERD relationship (suck swallow dyscoordination) Coarse, non musical inspiratory stridor during first few weeks of life Accentuated by supine position, feeding Cry is normal Evaluation: Flexible laryngoscopy, airway flouro, BS Treatment Spontaneous resolution by 2 years in vast majority of patients Epiglottoplasty Tracheostomy


40 Vocal Cord Paralysis 2 nd most common cause of congenital stridor Bilateral Etiology Idiopathic, CNS lesions, birth trauma Presentation Progressive stridor, voice may be normal High risk for aspiration Unilateral Etiology Mediastinal anomalies, idiopathic(heart, TEF surgery), trauma Presentation Hoarse cry,feeding difficulties, aspiration Evaluation Endoscopy Imaging MR or CT of Brain, Neck and Mediastinum Laryngeal EMG Management Tracheotomy: spontaneous recovery in >50% within 2 years Vocal cord lateralization: arytenoidectomy vs. transverse cordotomy
 Rx: Observation-> surgery->tracheotomy Laryngeal Atresia Acute airway obstruction TE fistula may allow some ventilation Tracheostomy is lifesaving Polyhydramnios may provide a clue,")
41 Congenital laryngeal webs Incomplete recanalization of laryngotracheal anlage Sx: Mild dysphonia to airway obstruction 1/3 have associated anomalies, most often subglottic stenosis Chromosome 22q11.2 deletion (VCFS) Rx: Observation-> surgery->tracheotomy Laryngeal Atresia Acute airway obstruction TE fistula may allow some ventilation Tracheostomy is lifesaving Polyhydramnios may provide a clue, allow for preoperative preparation



42 Laryngeal Cyst Congenital saccular cyst 25% of laryngeal cysts Obstruction of saccule with accumulation of mucus Vallecular cyst Subglottic cyst

43 Subglottic hemangioma 1.5% of congenital airway anomalies Female 2:1 Male. ½ with cutaneous hemangiomata Usually asymptomatic at birth, rapid growth after 2 months through 12 months Symptoms mimic recurrent croup Treatment options Observation, tracheostomy, steroids (systemic and local), interferon, surgical excision

44 Recurrent Respiratory Papillomatosis HPV 6,11 Entire respiratory tract Infancy through adult No cure Surgical therapy, medical adjunct Vaccine holds promise

45 Subglottic stenosis Congenital Rare Incomplete recanalization More mild Elliptical cricoid Acquired Most common 1-8% of intubated neonates Other causes Trauma Burns Neoplasms Infection Collagen vascular disorders

46 Pathogenesis of acquired subglottic stenosis intubation Circumferential scarring Pressure injury Mucosal edema Ulceration Perichondrial injury Cartilage necrosis Fibroblasts & Granulation tissue

47 Subglottic Stenosis the recipe Congenital subglottic stenosis GERD Infection Nasogastric tube ETT size and properties Movement of ETT Reintubations Duration?


48 Staging Classification from to Grade I No obstruction 50% Grade II 51% 70% Grade III 71% 99% Grade IV No lumen
49 Evaluation: GER/GERD, GLPR/GLPRD GER is common in children with subglottic stenosis and usually asymptomatic GER/GLPR likely exacerbates SGS and compromises repair No gold standard to differentiate GER and GERD Dual ph probe: 50% of candidates have upper probe ph<4 more than 1% of the time Majority had no symptoms
50 Evaluation: Swallowing Dysfunction Increased risk of aspiration postoperatively Rely on history Videoflouroscopic examination Limited in patients with food aversion or congenital aerodigestive anomalies FEES

51 Management Observation Tracheostomy Endoscopic techniques Cricoid split Augmentation Laryngoplasty Partial cricotracheal resection
52 Observation Non tracheotomized Grade I or mild grade II Occasional symptoms infrequent hospitalizations No retractions No feeding difficulties Tracheotomized patients reactive larynx Age/weight/pulmonary status/neurologic disease/aspiration potential/craniofacial or systemic abnormalities
53 Endoscopic Management Mild SGS May be required following open repair techniques Techniques Dilation CO2 laser wedge resections
54 Tracheotomy Temporizing measure Allows for growth prior to definitive procedure Time for improvement of BPD Facilitates discharge Gold Standard? Mortality rate varies with degree of obstruction above stoma Impairment of speech and language skills Nursing/childcare issues
55 History of airway reconstruction 193O s Chevalier Jackson recognizes that many children with laryngeal stenosis do not outgrow their obstruction permanent tracheotomy was treatment of choice 1960 s McDonald and Stocks: long term intubation for the management of prolonged ventilatory support in newborns Greater survival potential of premature newborns Shift of subglottic stenosis from older children and adults to premature infants
56 History of airway reconstruction Increased incidence of subglottic stenosis recognized Treatment consisted of repeated dilations Dogma was never divide the larynx to avoid growth disturbance 1956 Rethi Expansion of larynx and trachea with long term stent 1970 s Fearon and Cotton: Pedicled thyroid cartilage grafts 1980 s Free cartilage grafts allow for posterior and anterior grafting 1993 First series of successful cricotracheal resections reported
57 Cricoid Split Overview Indications Acquired subglottic stenosis in neonate (>1500g) without significant coincidental airway or pulmonary disease <30%FiO2, <35mm Pressure, no vent support Surgical technique Outcome Complications
58

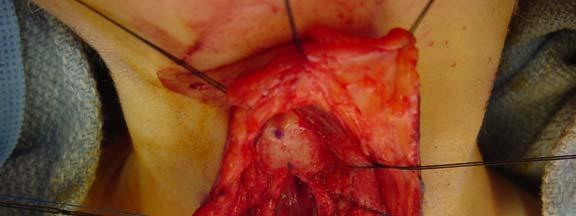
59 Augmentation Laryngotracheoplasty Overview Indications Surgical technique Single stage vs. 2 stage Source of donor cartilage Autologous materials Outcome Complications
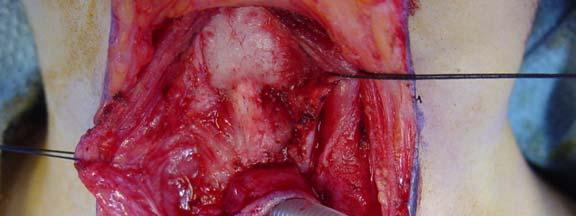
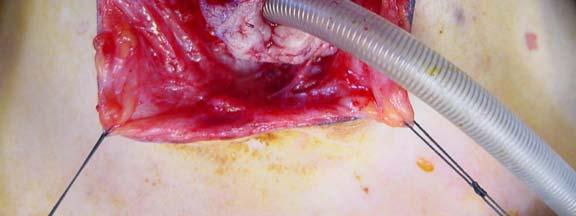
60 Single Stage LTR Uses cartilage grafts for expansion and a short phase of stenting with ETT Stoma is grafted and closed Postoperatively 0-14 days of intubation in ICU +/-Paralysis and sedation Bronchoscopy and downsize prior to extubation





61

62 Results >90% success rates in most series Success is dependent upon degree of stenosis <50% in severe grade III and IV stenosis
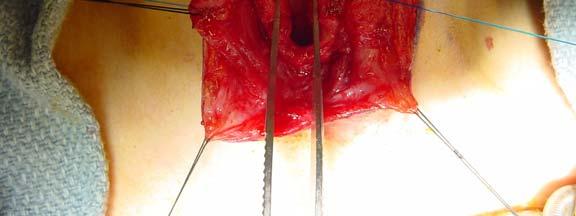
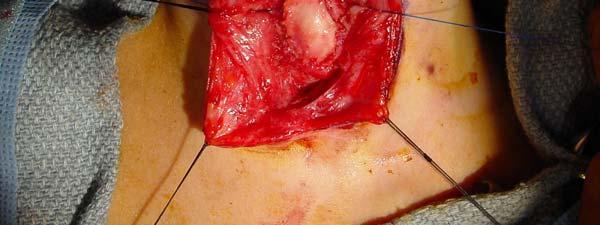
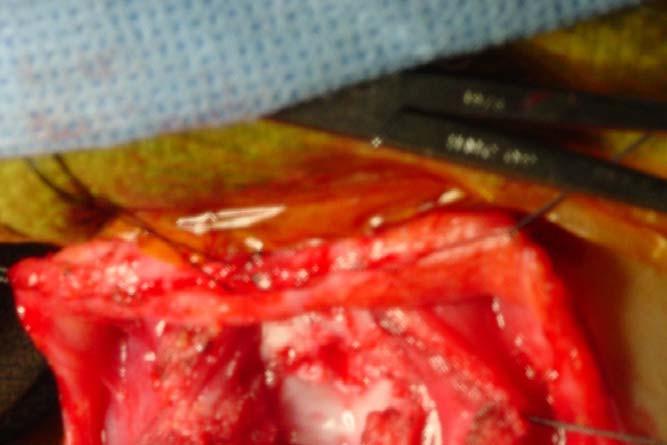
63 Partial Cricotracheal resection Overview Indications Surgical technique Outcome Complications

64
65 Adjunctive measures Stenting Useful for areas of stenosis beyond subglottis (posterior glottic stenosis) result in addition granulation tissue and scarring, Mitomycin C Antineoplastic antibiotic inhibits fibroblast formation Fibrin glue Holds mucosal flaps, produces an airtight seal
66 Postoperative care PICU Intubation for 0 14 days for single stage Sedation minimal paralysis Bronchoscopy/downsizing/extubation
67 Complications of Airway Reconstruction Intraoperative Hypoxia Pneumothorax Pneumomediastinum Vocal cord paralysis Early Postoperative SQ emphysema Seroma Hematoma Single Stage ETT obstruction Unplanned extubation Narcotic withdrawl Pulmonary problems Nasal alar ulceration Failed extubation Intermediate postoperative Granulations Restenosis Graft displacement Graft resorption Chonditis Suprastomal/ posterior glottic stenosis Late Postoperative Voice problems Epiglottic/arytenoid collapse Web Tracheocutaneous fistula
 Primary vs secondary MRI Rarely occurs with")
 Segmental resection Cartilage")
68 Tracheal Anomalies Tracheomalacia Abnormal flaccidity of trachea leading to collapse on expiration Collapse of greater than 20% on endoscopy (spontaneous ventilation) Primary vs secondary MRI Rarely occurs with laryngomalacia Rx: Mild- typically improves within 1-2 years Reflux therapy Severe tracheostomy with PPV Surgical correction varying success Stent placement (internal or external) Segmental resection Cartilage grafting



69 Tracheal Disorders Tracheal Stenosis Congenital vs. acquired Symptoms depend upon severity and length Complete tracheal rings Biphasic or expiratory stridor, wheezing, failure to thrive, bronchiolitis, cough recurrent croup Very gentle endoscopy! Rx: conservative for mild cases; resolution with growth Severe cases: segmental resection vs. anterior split with perichondrial grafting vs slide tracheoplasty or homograft tracheal transplantation Complications: granulation tissue at anastamotic site

70 Tracheal Disorders Vascular Compression 3% of population with anomalies of great vessels Rarely result in airway obstruction Rings vs slings Double aortic arch most common ring Innominate artery most common sling Right aortic arch with aberrant left subclavian Barium swallow and MR are essential
71 Conclusions Diagnosis of airway disorders in the neonate requires a comprehensive and systematic approach Stridor is not a diagnosis, but a symptom: the characteristics will help localize the source Twenty five years ago once a trach, always a trach Now, almost all tracheotomy dependent children with airway obstruction can eventually be decannulated Important to have a bag of tricks, as different approach works in different patients list of options for restoration of the pediatric airway continues to expand
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Complex Airway problems - Paediatric Perspective
 Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Aetiology. Poor tube management. Small cricoid (acquired on congenital) Reflux Poor general status. Size of tube (leak) Duration of intubation
 Reflux Poor general status. Size of tube (leak) Duration of intubation") Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Subject Index. Bacterial infection, see Suppurative lung disease, Tuberculosis
 Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Basic Science Review Wound Healing
 Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center
 Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center Children s Hospital of New Orleans Assistant Professor, Otolaryngology-Head & Neck Surgery, Louisiana State University. I do not have any
Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center Children s Hospital of New Orleans Assistant Professor, Otolaryngology-Head & Neck Surgery, Louisiana State University. I do not have any
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction. Nathan Page, MD Pediatrics in the Red Rocks June?
 Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Neonatal Stridor. Neonatology Roy Rajan, MD. Assistant Professor, Pediatric Otolaryngology Emory University
 Neonatal Stridor Neonatology 2015 Roy Rajan, MD Assistant Professor, Pediatric Otolaryngology Emory University Disclosures None 2 Goals/Objectives Describe embryology related to laryngeal development Define
Neonatal Stridor Neonatology 2015 Roy Rajan, MD Assistant Professor, Pediatric Otolaryngology Emory University Disclosures None 2 Goals/Objectives Describe embryology related to laryngeal development Define
Pediatric Airway Disorders Speaker Disclosure Outline
 Pediatric Airway Disorders G. Paul Digoy, M.D. Director of Pediatric Otolaryngology OU Health Sciences Center Paul-Digoy@ouhsc.edu Office: 405 271-5504 Speaker Disclosure Speakers, moderators, or panelists
Pediatric Airway Disorders G. Paul Digoy, M.D. Director of Pediatric Otolaryngology OU Health Sciences Center Paul-Digoy@ouhsc.edu Office: 405 271-5504 Speaker Disclosure Speakers, moderators, or panelists
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
Dundee Focused FRCS ENT Viva Course
 Dundee Focused FRCS ENT Viva Course Choanal atresia Nasal masses Craniofacial Micrognathia Glossomegaly IM Retropharyngeal abscess Caustics Vascular compression FB Bacterial tracheitis TOF Bronchiolitis
Dundee Focused FRCS ENT Viva Course Choanal atresia Nasal masses Craniofacial Micrognathia Glossomegaly IM Retropharyngeal abscess Caustics Vascular compression FB Bacterial tracheitis TOF Bronchiolitis
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant. Tara Brennan, MD 2,3
 Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Management of Pediatric Tracheostomy
 Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Evaluation and Management of Pediatric Stridor
 Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Pediatric Airway Emergencies
 Pediatric Airway Emergencies The University of Texas Medical Branch Department of Otolaryngology, Grand Rounds Presentation November 23, 2005 Steven T. Wright, M.D. Faculty Advisor: Seckin Ulualp, M.D.
Pediatric Airway Emergencies The University of Texas Medical Branch Department of Otolaryngology, Grand Rounds Presentation November 23, 2005 Steven T. Wright, M.D. Faculty Advisor: Seckin Ulualp, M.D.
External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other
 Internal trauma (Endotracheal intubation, tracheostomy) Other") Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Contents. Part A Clinical Evaluation of Laryngeal Disorders. 3 Videostroboscopy and Dynamic Voice Evaluation with Flexible Laryngoscopy...
 Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
THE DIFFICULT PEDIATRIC AIRWAY. Learning Objectives. The Pediatric Airway 6/7/18. Jason W. Gatling, MD Department of Anesthesiology June 7, 2018
 THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
4. Neoplastic: benign & malignant. 5. Allergic rhinitis & nasal polyp. 6. hypertrophied tonsils or adenoids. L 5
 L 5 Stertor& Stridor Stertor& stridor are both auditory manifestation of disordered respiratory function. Stertor: Is a low pitched snoring or snuffly sound caused by obstruction of the airway above the
L 5 Stertor& Stridor Stertor& stridor are both auditory manifestation of disordered respiratory function. Stertor: Is a low pitched snoring or snuffly sound caused by obstruction of the airway above the
Section 4.1 Paediatric Tracheostomy Introduction
 Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Unilateral Supraglottoplasty for Severe Laryngomalacia in Children. Nasser A Fageeh, MD, FRCSC, FACS*
 Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
PANELISTS. Controversial Issues In Common Interventions In ORL 4/10/2014
 Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
CASE PRIMERS. Pediatric Anesthesia Fellowship Program. Laryngotracheal Reconstruction (LTR) Tufts Medical Center
 Tufts Medical Center") CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications
 A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications Moderators: Marcellene Franzen, MD Fellow in Pediatric Anesthesiology Medical College
A case of a neonate with a congenital laryngeal web: management of a difficult airway and intra-operative complications Moderators: Marcellene Franzen, MD Fellow in Pediatric Anesthesiology Medical College
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction
 The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
Anesthetic consideration in Clefts & Craniofacial surgery
 Anesthetic consideration in Clefts & Craniofacial surgery พญ.เด อนเพ ญ ห อร ตนาเร อง ภาคว ชาว ส ญญ ว ทยา คณะแพทย แพทยศาสตร มหาว ทยาล ยขอนแก น Preoperative evaluation Cleft lip & Cleft palate reconstruction
Anesthetic consideration in Clefts & Craniofacial surgery พญ.เด อนเพ ญ ห อร ตนาเร อง ภาคว ชาว ส ญญ ว ทยา คณะแพทย แพทยศาสตร มหาว ทยาล ยขอนแก น Preoperative evaluation Cleft lip & Cleft palate reconstruction
Pediatrics Grand Rounds 25 October University of Texas Health Science Center at San Antonio, Texas
 PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
Chapter 124: Congenital Disorders of the Trachea. Bruce Benjamin
 Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
Chapter 124: Congenital Disorders of the Trachea Bruce Benjamin Investigation of the larynx and pharynx may be incomplete in infants and children with congenital abnormalities without investigation of
Airway Concerns. Trouble Breathing. Anywhere from nose to lungs. Neonates are obligate nasal breathers. Nasal symptoms:
 Pediatric Airway Naren Venkatesan, MD Mentor: Harold Pine, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology Head & Neck Surgery Grand Rounds Presentation April 26, 2013
Pediatric Airway Naren Venkatesan, MD Mentor: Harold Pine, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology Head & Neck Surgery Grand Rounds Presentation April 26, 2013
Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children
 Case Reports in Otolaryngology, Article ID 304593, 4 pages http://dx.doi.org/10.1155/2014/304593 Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children Aliye Filiz
Case Reports in Otolaryngology, Article ID 304593, 4 pages http://dx.doi.org/10.1155/2014/304593 Case Report Long-Term Outcomes of Balloon Dilation for Acquired Subglottic Stenosis in Children Aliye Filiz
Wheeze. Dr Jo Harrison
 Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
What are the Challenges? Spreading the Word in NICU. Need for NICU Care: Impact. Baby Trachs: Use of the Passy Muir Valve in the NICU to
 What are the Challenges? Baby Trachs: Use of the Passy Muir Valve in the NICU to Optimize Swallowing and Feeding Catherine S Shaker, MS/CCC SLP, BRS S and Cari Mutnick, MS/CCC SLP Florida Hospital for
What are the Challenges? Baby Trachs: Use of the Passy Muir Valve in the NICU to Optimize Swallowing and Feeding Catherine S Shaker, MS/CCC SLP, BRS S and Cari Mutnick, MS/CCC SLP Florida Hospital for
Review of literature suggests that there are three basic theories that attempt to explain the development of laryngomalacia.
 TITLE: Current Concepts in Diagnosis and Management of Laryngomalacia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 FACULTY PHYSICIANS: Shraddha Mukerji, MD and
TITLE: Current Concepts in Diagnosis and Management of Laryngomalacia SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 FACULTY PHYSICIANS: Shraddha Mukerji, MD and
Preface... Contributors... 1 Embryology... 3
 Contents Preface... Contributors... vii xvii I. Pediatrics 1 Embryology... 3 Pearls... 3 Branchial Arch Derivatives... 3 Branchial Arch Anomalies: Cysts, Sinus, Fistulae... 4 Otologic Development... 4
Contents Preface... Contributors... vii xvii I. Pediatrics 1 Embryology... 3 Pearls... 3 Branchial Arch Derivatives... 3 Branchial Arch Anomalies: Cysts, Sinus, Fistulae... 4 Otologic Development... 4
Disclosure Statement The Squeaky Baby
 Disclosure Statement The Squeaky Baby A Pediatric Provider s Guide to Stridor in the Young Child I have no actual or potential conflict of interest in relation to this program. Daniel Jensen, MD Assistant
Disclosure Statement The Squeaky Baby A Pediatric Provider s Guide to Stridor in the Young Child I have no actual or potential conflict of interest in relation to this program. Daniel Jensen, MD Assistant
I enjoy open airway surgery In 2010: LTRs 28 CTRs 6 Clefts 4 Slides 20
 Michael J. Rutter, FRACS Department of Pediatric Otolaryngology- Head & Neck Surgery Aerodigestive and Esophageal Center Cincinnati Children s Hospital Medical Center Cincinnati, Ohio IPSA Denver, CO June
Michael J. Rutter, FRACS Department of Pediatric Otolaryngology- Head & Neck Surgery Aerodigestive and Esophageal Center Cincinnati Children s Hospital Medical Center Cincinnati, Ohio IPSA Denver, CO June
Congenital Laryngeal Anomalies
 Congenital Laryngeal Anomalies Prof. Hesham Abd Al-Fattah Alexandria - Egypt Embryology Resp primordium 3 rd wk Resp primordium separated by tracheoesophageal folds Fuse to form septum (4-5 wks) Larynx
Congenital Laryngeal Anomalies Prof. Hesham Abd Al-Fattah Alexandria - Egypt Embryology Resp primordium 3 rd wk Resp primordium separated by tracheoesophageal folds Fuse to form septum (4-5 wks) Larynx
CHAPTER 7 Procedures on Respiratory System
 CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Airway Endoscopy The Basics Neonatal Progressive Acute Quiz
 Endoscopy of the Airway Dave Albert Airway Endoscopy The Basics Neonatal Progressive Acute Quiz The laws of Poiseuille and Bernoulli French physician,physicist mathemetician and Dutch Swiss mathemetician
Endoscopy of the Airway Dave Albert Airway Endoscopy The Basics Neonatal Progressive Acute Quiz The laws of Poiseuille and Bernoulli French physician,physicist mathemetician and Dutch Swiss mathemetician
Subspecialty Rotation: Otolaryngology
 Subspecialty Rotation: Otolaryngology Faculty: Evelyn Kluka, M.D. GOAL: Hearing Loss. Understand the morbidity of hearing loss, intervention strategies, and the pediatrician's and other specialists' roles
Subspecialty Rotation: Otolaryngology Faculty: Evelyn Kluka, M.D. GOAL: Hearing Loss. Understand the morbidity of hearing loss, intervention strategies, and the pediatrician's and other specialists' roles
Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic Pause: Experience in 5 Children
 BioMed Research International, Article ID 397295, 4 pages http://dx.doi.org/10.1155/2014/397295 Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic
BioMed Research International, Article ID 397295, 4 pages http://dx.doi.org/10.1155/2014/397295 Research Article Balloon Dilatation of Pediatric Subglottic Laryngeal Stenosis during the Artificial Apneic
Congenital Laryngeal Anomalies November 2002
 TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 20, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, M.D. FACULTY ADVISOR: Ronald W. Deskin,
TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 20, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, M.D. FACULTY ADVISOR: Ronald W. Deskin,
ORIGINAL ARTICLE. Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty
 ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy
 An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
The surgical management of subglottic stenosis (SGS)
") Original Research Pediatric Otolaryngology Short- versus Long-term Stenting in Children with Subglottic Stenosis Undergoing Laryngotracheal Reconstruction Otolaryngology Head and Neck Surgery 2018, Vol.
Original Research Pediatric Otolaryngology Short- versus Long-term Stenting in Children with Subglottic Stenosis Undergoing Laryngotracheal Reconstruction Otolaryngology Head and Neck Surgery 2018, Vol.
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis
 Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Paediatric Otolaryngology
 Paediatric Otolaryngology Antony A Narula MA FRCS FRCS Ed Consultant St Mary s & Ealing Hospitals Hon. Professor, Middlesex University 17 th July 2004 Otology Acute Otitis Media Otitis Media with Effusion
Paediatric Otolaryngology Antony A Narula MA FRCS FRCS Ed Consultant St Mary s & Ealing Hospitals Hon. Professor, Middlesex University 17 th July 2004 Otology Acute Otitis Media Otitis Media with Effusion
Congenital Laryngeal Anomalies November 2005
 TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 2, 2005 RESIDENT PHYSICIAN: Jean P. Font M.D. FACULTY: ADVISOR: Seckin Ulualp, M.D.
TITLE: Congenital Laryngeal Anomalies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 2, 2005 RESIDENT PHYSICIAN: Jean P. Font M.D. FACULTY: ADVISOR: Seckin Ulualp, M.D.
Day 2 Pulmonary Breakout Interventional Pulmonology
 Day 2 Pulmonary Breakout Interventional Pulmonology R. Paul Boesch, DO, MS Assistant Professor, Pulmonary Medicine Mayo Clinic Children s Center Interventional Pediatric Pulmonology or Pulm/ENT airway
Day 2 Pulmonary Breakout Interventional Pulmonology R. Paul Boesch, DO, MS Assistant Professor, Pulmonary Medicine Mayo Clinic Children s Center Interventional Pediatric Pulmonology or Pulm/ENT airway
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
Stridor in Children. Agrício Nubiato Crespo and Rodrigo Cesar e Silva
 Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Idiopathic laryngotracheal stenosis
 Surgical Technique Idiopathic laryngotracheal stenosis Christina L. Costantino, Douglas J. Mathisen Massachusetts General Hospital, Boston, MA 02114, USA Correspondence to: Douglas J. Mathisen, MD. Massachusetts
Surgical Technique Idiopathic laryngotracheal stenosis Christina L. Costantino, Douglas J. Mathisen Massachusetts General Hospital, Boston, MA 02114, USA Correspondence to: Douglas J. Mathisen, MD. Massachusetts
There are four general types of congenital lung disorders:
 Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Pediatric Pulmonology Conditions Evaluated and Treated As a parent, watching a child suffer from a respiratory disorder can be frightening and worrisome. Our respiratory specialists provide compassionate
Tracheal stenosis in infants and children is typically characterized
 Slide Tracheoplasty for Congenital Tracheal Stenosis Peter B. Manning, MD Tracheal stenosis in infants and children is typically characterized by the presence of complete cartilaginous tracheal rings and
Slide Tracheoplasty for Congenital Tracheal Stenosis Peter B. Manning, MD Tracheal stenosis in infants and children is typically characterized by the presence of complete cartilaginous tracheal rings and
-Discussed in the Ebers Papyrus and the Rig Veda BC
 Tracheotomy History -Discussed in the Ebers Papyrus and the Rig Veda -1500 BC History -Treatment obstructive diseases (Antyllus, 2 nd century AD) -Discussed in the writings of Braassarolo (1546) -Considered
Tracheotomy History -Discussed in the Ebers Papyrus and the Rig Veda -1500 BC History -Treatment obstructive diseases (Antyllus, 2 nd century AD) -Discussed in the writings of Braassarolo (1546) -Considered
Airway Management in the ICU
 Airway Management in the ICU New developments in management of epistaxis. April 28, 2008 Methods of airway control Non surgical BIPAP CPAP Mask ventilation Laryngeal Mask Intubation Surgical Cricothyrotomy
Airway Management in the ICU New developments in management of epistaxis. April 28, 2008 Methods of airway control Non surgical BIPAP CPAP Mask ventilation Laryngeal Mask Intubation Surgical Cricothyrotomy
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy
 Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Clinical Practice Guideline: Tonsillectomy in Children, Baugh et al Otolaryngology Head and Neck Surgery, 2011 J and: 144 (1 supplement) S1 30.
 S1 30.") Pediatric ENT Guidelines Jane Cooper, FNP, CORLN References: Clinical Practice Guideline: Tympanostomy tubes in children, Rosenfeld et al., American Academy of Otolaryngology Head and Neck Surgery Foundation
Pediatric ENT Guidelines Jane Cooper, FNP, CORLN References: Clinical Practice Guideline: Tympanostomy tubes in children, Rosenfeld et al., American Academy of Otolaryngology Head and Neck Surgery Foundation
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience
 1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
Disclosures. Learning Objectives. Coeditor/author. Associate Science Editor, American Heart Association
 Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005
 Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Surgery
Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Surgery
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September ISSN
 International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
Airway Emergencies: Pearls for the Anesthesiologist
 Airway Emergencies: Pearls for the Anesthesiologist Pavan S. Mallur, MD, FACS Division of Otolaryngology, Department of Surgery Beth Israel Deaconess Medical Center Department of Otology and Laryngology
Airway Emergencies: Pearls for the Anesthesiologist Pavan S. Mallur, MD, FACS Division of Otolaryngology, Department of Surgery Beth Israel Deaconess Medical Center Department of Otology and Laryngology
Laryngotracheal stenosis in children
 Eur Arch Otorhinolaryngol (1998) 255 : 12 17 Springer-Verlag 1998 LARYNGOLOGY M. M. Lesperance G. H. Zalzal Laryngotracheal stenosis in children Received: 8 March 1977 / Accepted: 31 July 1997 Abstract
Eur Arch Otorhinolaryngol (1998) 255 : 12 17 Springer-Verlag 1998 LARYNGOLOGY M. M. Lesperance G. H. Zalzal Laryngotracheal stenosis in children Received: 8 March 1977 / Accepted: 31 July 1997 Abstract
ORIGINAL ARTICLE. Office-Based Lower Airway Endoscopy in Pediatric Patients. airway symptoms is an integral part of the otolaryngology practice.
 ORIGINAL ARTICLE Office-Based Lower Airway Endoscopy in Pediatric Patients D. Richard Lindstrom III, MD; David T. Book, MD; Stephen F. Conley, MD; Valerie A. Flanary, MD; Joseph E. Kerschner, MD Background:
ORIGINAL ARTICLE Office-Based Lower Airway Endoscopy in Pediatric Patients D. Richard Lindstrom III, MD; David T. Book, MD; Stephen F. Conley, MD; Valerie A. Flanary, MD; Joseph E. Kerschner, MD Background:
Objectives. Module A2: Upper Airway Anatomy & Physiology. Function of the Lungs/Heart. The lung is for gas exchange. Failure of the Lungs/Heart
 Module A2: Upper Airway Anatomy & Physiology Objectives Classify epithelial tissue based on cell type and tissue layers. Identify location of tissue epithelium in the respiratory system. Describe the major
Module A2: Upper Airway Anatomy & Physiology Objectives Classify epithelial tissue based on cell type and tissue layers. Identify location of tissue epithelium in the respiratory system. Describe the major
ORIGINAL ARTICLE. Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy
 ORIGINAL ARTICLE Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy Shyan Vijayasekaran, FRACS; David R. White, MD; Benjamin E. J. Hartley, FRCS(ORL); Michael J. Rutter, FRACS; Ravindhra G.
ORIGINAL ARTICLE Open Excision of Subglottic Hemangiomas to Avoid Tracheostomy Shyan Vijayasekaran, FRACS; David R. White, MD; Benjamin E. J. Hartley, FRCS(ORL); Michael J. Rutter, FRACS; Ravindhra G.
A study on paediatric stridor causes and management: case series
 International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Varied Presentation and Management of Tracheal Polyps in Children Vinod M Raj 1, Varun Hathiramani 2, Swathi
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Varied Presentation and Management of Tracheal Polyps in Children Vinod M Raj 1, Varun Hathiramani 2, Swathi
Microdebrider. Microdebrider. Mohamed Hesham,MD. The Management of Different Laryngeal Lesions. Dr. Ahmad Yassin 4/11/2013
 Microdebrider In The Management of Different Laryngeal Lesions Mohamed Hesham,MD Dr. Ahmad Yassin Otolaryngology Head&Neck Surgery Alexandria Faculty of Medicine Microdebrider The microdebrider is a powered
Microdebrider In The Management of Different Laryngeal Lesions Mohamed Hesham,MD Dr. Ahmad Yassin Otolaryngology Head&Neck Surgery Alexandria Faculty of Medicine Microdebrider The microdebrider is a powered
Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis
 Journal of Voice Vol. 14, No. 2, pp. 282-286 2000 Singular Publishing Group Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis *Reza Rahbar,
Journal of Voice Vol. 14, No. 2, pp. 282-286 2000 Singular Publishing Group Preliminary Results of Intraoperative Mitomycin-C in the Treatment and Prevention of Glottic and Subglottic Stenosis *Reza Rahbar,
Subglottic stenosis in infants and children
 Original Article Singapore Med J 010; 51(1 1) : 88 Subglottic stenosis in infants and children Choo K K M, Tan H K K, Balakrishnan A Yong Loo Lin School of Medicine, National University of Singapore, 10
Original Article Singapore Med J 010; 51(1 1) : 88 Subglottic stenosis in infants and children Choo K K M, Tan H K K, Balakrishnan A Yong Loo Lin School of Medicine, National University of Singapore, 10
Tracheal Trauma: Management and Treatment. Kosmas Iliadis, MD, PhD, FECTS
 Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Chronic Stridor in Children These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Chronic Stridor in Children These podcasts are designed to give medical students an overview of key topics in pediatrics.
Therapeutic Bronchoscopy Etiology - Benign Stenosis Post - intubation Trauma Post - operative Inflammatory Idiopathic
 Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Pediatric upper airway and congenital anomalies
 Anesthesiology Clin N Am 20 (2002) 747 766 Pediatric upper airway and congenital anomalies Andrew Infosino, MD Department of Anesthesia and Perioperative Care, University of California at San Francisco,
Anesthesiology Clin N Am 20 (2002) 747 766 Pediatric upper airway and congenital anomalies Andrew Infosino, MD Department of Anesthesia and Perioperative Care, University of California at San Francisco,
Audra Fuller MD, Mark Sigler MD, Shrinivas Kambali MD, Raed Alalawi MD
 Clinical Series Successful treatment of post-intubation tracheal stenosis with balloon dilation, argon plasma coagulation, electrocautery and application of mitomycin C Audra Fuller MD, Mark Sigler MD,
Clinical Series Successful treatment of post-intubation tracheal stenosis with balloon dilation, argon plasma coagulation, electrocautery and application of mitomycin C Audra Fuller MD, Mark Sigler MD,
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Otolaryngology
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Otolaryngology 1. GOAL: Hearing Loss. Understand the morbidity of hearing loss, intervention strategies, and the pediatrician's
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Otolaryngology 1. GOAL: Hearing Loss. Understand the morbidity of hearing loss, intervention strategies, and the pediatrician's
Subglottic stenosis, with involvement of the lower larynx
 Laryngotracheal Resection and Reconstruction John D. Mitchell, MD n, Subglottic stenosis is being recognized with increasing frequency in adults, and may be the most frequent indication for airway intervention
Laryngotracheal Resection and Reconstruction John D. Mitchell, MD n, Subglottic stenosis is being recognized with increasing frequency in adults, and may be the most frequent indication for airway intervention
Pediatric Difficult Airway Management. R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee
 Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee The pediatric difficult airway is associated with a high risk for complications during
Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee The pediatric difficult airway is associated with a high risk for complications during
Surgical Treatment of Benign Subglottic Stenosis. JLKasperbauer MD Mayo Clinic Rochester, MN USA
 Surgical Treatment of Benign Subglottic Stenosis JLKasperbauer MD Mayo Clinic Rochester, MN USA Goals Review Subglottic Stenosis Anatomy, Airway Dynamics, Etiology Idiopathic Subglottic Stenosis Definition,
Surgical Treatment of Benign Subglottic Stenosis JLKasperbauer MD Mayo Clinic Rochester, MN USA Goals Review Subglottic Stenosis Anatomy, Airway Dynamics, Etiology Idiopathic Subglottic Stenosis Definition,
Conflict of Interest: none. Neonatal Airway Masses. Neonatal Respiratory Papillomatosis. Paul J. Samuels, MD
 Paul J. Samuels, MD Professor of Anesthesiology and Pediatrics Director of Education Cincinnati Children s Hospital Cincinnati, Ohio Conflict of Interest: none Neonatal Respiratory Papillomatosis Caused
Paul J. Samuels, MD Professor of Anesthesiology and Pediatrics Director of Education Cincinnati Children s Hospital Cincinnati, Ohio Conflict of Interest: none Neonatal Respiratory Papillomatosis Caused
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY LARYNGOMALACIA Laryngomalacia is characterised by collapse of the supraglottic tissues on inspiration, and is the most common cause of
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY LARYNGOMALACIA Laryngomalacia is characterised by collapse of the supraglottic tissues on inspiration, and is the most common cause of
Use of the Silicone T-tube to Treat Tracheal Stenosis or Tracheal Injury
 Use of the Silicone T-tube to Treat Stenosis or Injury Chang-Jer Huang MD Backgound: stenosis or tracheal is a troublesome disease. Traditional temporary tracheostomy and reconstruction can resolve some
Use of the Silicone T-tube to Treat Stenosis or Injury Chang-Jer Huang MD Backgound: stenosis or tracheal is a troublesome disease. Traditional temporary tracheostomy and reconstruction can resolve some
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
Recognizing the Difficult Airway in Pediatric Patients. Nancy L. Glass, MD, MBA,
 Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Emergency ENT Anaesthesia. Richard Semenov
 Emergency ENT Anaesthesia Richard Semenov Emergency ENT Anaesthesia Dr Richard Semenov MBBS (Adel) FRCA (UK) FANZCA Dept of Anaesthesia Royal Adelaide Hospital My Experience in Emergency ENT Anaesthesia
Emergency ENT Anaesthesia Richard Semenov Emergency ENT Anaesthesia Dr Richard Semenov MBBS (Adel) FRCA (UK) FANZCA Dept of Anaesthesia Royal Adelaide Hospital My Experience in Emergency ENT Anaesthesia
Subglottic Stenosis November 2002
 TITLE: Subglottic Stenosis SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 13, 2002 RESIDENT PHYSICIAN: Christopher D. Muller, M.D. FACULTY PHYSICIAN: Anna M. Pou, M.D.
TITLE: Subglottic Stenosis SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 13, 2002 RESIDENT PHYSICIAN: Christopher D. Muller, M.D. FACULTY PHYSICIAN: Anna M. Pou, M.D.
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation
 Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Anna & John J. Sie Center for Down Syndrome Affiliates
 Anna & John J. Sie Center for Down Syndrome Affiliates Types of Medical Research Bench or basic research: done in a controlled laboratory setting using nonhuman subjects Clinical research: answer questions
Anna & John J. Sie Center for Down Syndrome Affiliates Types of Medical Research Bench or basic research: done in a controlled laboratory setting using nonhuman subjects Clinical research: answer questions
Disclosures. Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia. Case Presentation. Case Presentation.
 Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant