Hyponatremia Clinical Significance. Ágnes Haris MD PhD, St. Margit Hospital, Budapest
|
|
|
- Roxanne Gilmore
- 5 years ago
- Views:
Transcription
1 Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1
2 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial pain, poor appetite, body weight decreased by 3 kg When specifically asked: complains of weaknes, dizziness, unsteady gait family doctor arranged an appointment for head CT 2
3 Physical examination RR 148/72 mmhg, P 89/min Some wheezes above the chest Mild epigastrial tenderness No edema Conscious, oriented, no focal neurological abnormality 3
4 Laboratory results on admission Na K Cl Blood sugar CN Creatinine Uric acid Urinary sodium Urinary potassium Urinary osmolality 114 mmol/l 4,7 mmol/l 82 mmol/l 7,1 mmol/l 3,8 mmol/l 52 umol/l 138 umol/l 86 mmol/l 63 mmol/l 577 mosm/kg 4
5 What is your approach? 1) Is this a true hyponatremia? - Can it be pseudohyponatremia? - Measurement of serum osmolality 2) Is this an acute or chronic hyponatremia? 3) What is the most appropriate treatment? 5

6 93% 7% Pseudohyponatremia Clinical practice guideline on diagnosis and treatment of hyponatraemia. NDT *Our pt s serum lipid and protein levels were normal.
7 Hyperglycemia - Role of blood sugar Translocational hyponatremia! Serum osmolality in not low! Corrected serum Na = measured serum Na x actual glucose (mmol/l) / 5.5 mmol/l Quick, approximate calculation: - Each 5 mmol/l increase of blood sugar above normal alters serum sodium concentration by 2 mmol/l - e.g. blood sugar = 25 mmol/l 20 mmol/l increment - serum Na decreases by 20/5x2 = 8 mmol/l 7
8 What do the urinary lab results tell us? Urinary sodium 86 mmol/l Based on the physical examination and the urinary Na concentration he was normovolemic. * He did not get any diuretics Diuretic drugs alter urinary Na excretion, regardless of volume status Uosm: 577 mosm/kg = strong ADH effect - Why??? 8

9 Action of ADH on the tubular water reabsorption - urinary concentration 9 If Uosm > 100 mosm/kg = ADH is acting
10 Other labs to pay attention Blood sugar CN Creatinine Uric acid TSH Cortisol 7,1 mmol/l rules out pseudohypona (also serum lipids, protein levels) 3,8 mmol/l no signs of volume depletion, renal failure 52 umol/l - no sign of renal failure 138 umol/l not enchanced tubular reabsorption (as in volume depletion) 1,155 miu/l - rule out hypothyroidism measure if clinical suspition - rule out hypocorticism 10

11 Acute or chronic? 11
12 Clinical course Chest XR - widening of the left hilus + 2 cm wide mass Suspected pulmonal malignancy - CT scan is suggested Treatment of hyponatremia: fluid restriction (< 750 ml fluid intake/day) and generous amount of salt consumption with meals Serum sodium on the following days: mmol/l 12
 and by internal exchange between Na that is free in solution and Na that is bound to polyanionic proteoglycans in bone,")
13 Internal and External Solute and Water Balance and the Plasma Sodium Concentration Sterns RH. N Engl J Med 2015;372:55-65 Plasma Na concentration: Na and K in the body to total body water. This concentration is altered by net external balances (intake minus output) and by internal exchange between Na that is free in solution and Na that is bound to polyanionic proteoglycans in bone, cartilage, and skin. 13
14 Summary of the basic approach to chronic hyponatremia 1) Differentiate acute and chronic hyponatremia 2) Look for the reason of ADH secretion - determine what the patient volume status is - check urinary electrolytes and osmolality - initiate work up to determine etiology 3) Decide about treatment - in case of chronic hypona be moderate and slow 14
15 HypoNa in euvolemic patients -Medications One of the most frequent cause of hypona Caused very often by thiazides - increased urinary solute excretion - no increase in free water excretion - medullary concentration gradient remains intact - especially risky in elderly patients with low solute intake - ADH stimulation by diuretic caused volume depletion contributes to some extent - volume depletion causes increased thirst, fluid intake Many other drugs associated with hypona: SSRI-s, carbamazepin, narcotics, cyclophosphamide, desmopressin, etc. 15
16 HypoNa in euvolemic patients -SAH Frequently seen in neurosurgical departments Hannon at al. J Clin Endocrinol Metab patients suffered SAH, 49 developed hypona, serum Na <135 mmol/l, 14% < 130 mmol/l ADH, BNP, cortisol were measures, based on these: Etiology of hypona was SIAD in 71% (Rarely other intracranial hemorrhages, infections, or pulmonary infections cause hypona) 16

17 Hyponatremia following mild/moderate SAH Hannon at al. J Clin Endocrinol Metab
18 Hyponatremia following mild/moderate SAH Hannon at al. J Clin Endocrinol Metab
19 HypoNa in euvolemic patients - Malignancy Although this was the original description of SIADH by Schwartz and Bartter in 1957, it is a relatively rare cause of hypona Several tumors can cause:, e.g. lung, oropharynx, GI, genitourinary, carcinomas, lymphomas, sarcomas, neuroblasoma 19
20 Hyponatremia in hyperhydrated patients liver cirrhosis In 15-20% of alcoholic patients High level of vasopressin due to decreased effective circulatory volume (systemic vasodilatation, arteriovenosus shunting) neurohormonal activation, baroreceptor mediated vasopressin release HypoNa means more water than salt Poor prognostic sign Treatment: water restriction, salt restriction, diuretics Potential role of vaptans? 20
21 Hyponatremia in hyperhydrated patients heart failure In 20-30% with NYHA III-IV decreased cardiac output baroreceptor mediated neurohormonal activation High level of vasopressin due to decreased effective circulatory volume HypoNa means more water than salt Poor prognostic sign Treatment: water restriction, salt restriction, loop diuretics; treatment of the cardiac disease Potential role of vaptans (?) Similar 21 situation in nephrotic syndrome
22 Hyponatremia in volume depleted patients Vasopressin secretion is mediated by volume depletion non-osmotic baroreceptor mediated ADH secretion Treatment: In this case isotonic saline infusion will correct serum Na as the stimulus for vasopressin secretion is stopped Do not give hypertonic Na infusion! risk of overcorrection! Watch for dilute urine increased free water excretion! it predicts the serum Na increase 22
23 From: Clinical practice guideline on diagnosis and treatment of hyponatraemia Nephrol Dial Transplant. 2014;29(suppl_2):i1-i39. doi: /ndt/gfu040 Nephrol Dial Transplant European Society of Endocrinology, European Society of Intensive Care Medicine, European Renal Association European Dialysis and Transplant Association (2014). 23
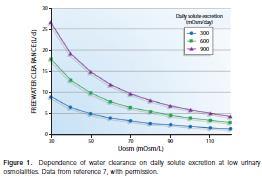
24 Beer potomania or Tea and toast hyponatremia - Impact of solute intake Maximal urinary diluting capacity > 50 moms/kg (We cannot pee tapwater ) Sodium, potassium and protein consumption determines solute excretion (10 g of protein results in 50 mmol urinary urea excretion) Solute excretion determines water excretion Beer potomania minimal solute intake (salt, protein) Treatment: hypertonic saline administriation depens on acuteness and severity; Aim to normalize salt and protein consumption Be carefull with serum osmolality measurement alcohol increases it! calculated osmolality is better 24
25 25
26 Hyponatremia in chronic renal failure Limited diluting capacity: urinary osmolality serum osmolality (isostenuria) On low protein, low salt and low potassium diet Limited solute excretion Treatment: adjust fuid intake to solute intake and renal diluting capacity 26
27 27 Acute hyponatremia
28 Acute hypona is a rare condition You may diagnose it in Postoperative state: excesive ADH secretion due to pain, stress, nausea, narcotics + inappropriate hypotonic fluid administration Recent introduction of a thiazide diuretic Psychogenic polydypsia Endurance exercise Use of ecstasy 28
29 Acute hypona causes severe symptoms Signs of cerebral edema: vomiting, confusion, seizures, stupor, coma, noncardiogenic pulmonary edema (In case the patient does not have such symptoms hyponatremia is very likely chronic!) 29
30 Acute hypona during preparation for colonoscopy 84 years old female, admitted to hospital 12 days earlier because she had had diarrhoea for 3 days On admission she looked volume depleted, had low BP (90/50 mmhg) Laboratory results: Hgb 9,86 g%, serum Na 134 mmol/l, K 3,0 mmol/l, BUN 21,9 mmol/l, creatinine 182 umol/l She got 0,9% NaCl infusion+kcl for 3 days the BP normalized (118/59 mmhg), the labs: Na 141 mmol/l, K 3,6 mmol/l, BUN 4,1 mmol/l, creatinine 86 umol/l The gastroenterology team decided to go on with GI work up in order to look for the cause of anemia 30
31 Acute hypona during preparation for colonoscopy Scheduled for colonoscopy on Monday (plan to preparing her by Fleet enema on Sunday evening) Instruction by the nurse on Sunday morning: no solid food to eat, only fluids to drink On Sunday morning complaints free, ambulating, looked nervous In the afternoon: she suddenly lost her consciousness, had a convulsion, did not respond even to pain, had uncoordinated movements in all her extremities. Vomited repeatedly
32 Acute hypona during preparation for colonoscopy Urgent labwork: serum Na 117 mmol/l, K 2,9 mmol/l, BUN 2,4 mmol/l, creatinine 98 umol/l Urinary osmolality 431 mosm/kg, urinary Na 164 mmol/l, K 44 mmol/l hrs, 900 ml/12 hrs Brain CT: -no major abnormality can be seen 32 32
33 Approach of the case Acute, severe hyponatremia very likely cerebral edema Urine osmolality: 431 mosm/kg - strong influence of ADH (likely due to stress, anxiety, nausea) Lots of fluid intake according to the instructions Urine Na: 164 mmol/l means - no volume depletion Treatment: 3% NaCl infusion 33 33
34 Treatment plan Weight of the patient: 84 kg. Body water: 42 l - To elevate sena by 1mmol/l, she needs 42 mmol Na - To elevate sena by 5 mmol/l, she needs 210 mmol Na - It means 408 ml of 3% NaCl infusion Follow urinary Na loss and replace it Check electrolytes frequently 34 34
35 Treatment on the 12th day She got 300 ml 3% NaCl infusion (154 mmol) + 4 g KCl 4 hours later serum Na 119 mmol/l, K 3,2 mmol/l During Sunday night 300 ml 3% NaCl (154 mmol) + 4 g KCl On Monday morning 300 ml 3% NaCl infusion (154 mmol) (still unconscious) By the afternoon: serum Na 130 mmol/l, K 3,9 mmol/l In summary she got 462 mmol Na in the 1 st 24 hrs Urinary losses in 24 hrs: 230 mmol Na and 62 mmol K 35 35
36 Full recovery Monday Neurological examination: - no primary neurological abnormality, - EEG: diffuse functional cortical abnormality Next day: serum Na 134 mmol/l, she regained consciousness Two days later: serum Na 140 mmol/l 36
37 37 Treatment

38 Consequences of Rapid Changes in the Plasma Sodium Concentration 38 Sterns RH. N Engl J Med 2015;372:55-65
39 Acute, or chronic hypona with severe symptoms Administer 150 ml 3% NaCl bolus infusion over 20 minutes (Na conc. 513 mmol/l) Check serum Na concentration Meanwhile repeate the 150 ml 3% NaCl bolus infusion once or twice Aim to increase serum Na concentration by 5 mmol/l Limite correction in 10 mmol/l in the first 24 hr, and in 8 mmol/l in the next 24 hr Check serum Na concentration in 4-6 hrs until severe symptoms have stopped and serum Na stabilised 39
40 Role of potassium Loss of potassium intracellular depletion sodium is transferred from EC to IC space Therefore in hyponatremic patients potassium administration increases serum Na level - 1 mmol of retained potassium elevates serum Na by 1 mmol 40
41 Watch for urinary Na+K concentration Excretion of hypotonic urine will increase serum Na concentration: lots of free water is excreted Urinary Na+Urinary K/serum Na - if low, eg < 0,5 lots of free water is excreted serum sodium will increase If the electrolyte concentration of urine is higher than serum Na, serum Na is expected Large increase of urine output predicts water diuresis 41
42 Effect of furosemide Increases the volume of the urine Dilute urine is excreted Reduces the risk of the EC volume expansion Increase the speed of serum Na elevation 42
43 Chronic hypona with moderate or mild symptoms Fluid restriction: < ml/day For patients with no edema: increase solute intake (protein, sodium and potassium) Urea may be considered (good effect with 30 g/day in patients with NSIAD) In hyperhydrated patients: fluid + salt restriction! + furosemide Check the medications the patient was taking! 43
44 Vaptans V 2 receptor antagonists Block the effect of ADH on collecting duct May be considered in heart failure, SIADH Contraindicated in acute hypona, volume depletion Potential liver toxicity Very expensive 44
45 In case of overcorrection D5W infusion (adjust dose to urine output) Desmopressin (iv 1-5 ug in 6-8 hours) - consider if too rapid serum Na increase in hypovolemic hypona due to Saline infusion 45
46 Osmotic demyelination In the pons CPM May extend to extrapontin structures Pseudobulbar palsy, hyperreflexia, quadriparesis, cerebellar ataxia, dysarthria, dysphagia, movement disorders or locked-in syndrome, even death Biphasic presentation it develops 1-7 days after overcorrection MRI proves, but only approx 2 weeks later Higher risk in patients with very severe chronic hypona, in alhoholic patiens, in malnutrition, potassium depletion High disability, short and long term mortality rate 46
:i1-i39. doi:10.")
47 Clinical practice guideline on diagnosis and treatment of hyponatraemia Nephrol Dial Transplant. 2014;29(suppl_2):i1-i39. doi: /ndt/gfu040 47
:i1-i39. doi:10.")
48 Clinical practice guideline on diagnosis and treatment of hyponatraemia Nephrol Dial Transplant. 2014;29(suppl_2):i1-i39. doi: /ndt/gfu040 48
49 49 Thank you for your attention!
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Hyponatraemia- Principles, Investigation and Management. Sirazum Choudhury Biochemistry
 Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
SATURDAY PRESENTATIONS
 Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY PRESENTATIONS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY PRESENTATIONS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS Annual Meeting
 Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical education
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical education
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
Hyponatremia FOSPED 2018
 Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Iposodiemia: diagnosi e trattamento
 Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Workshop CME 22 mars Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 Workshop CME 22 mars 2013 Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles Overcorrection of chronic hyponatremia CASE REPORT I (1) Female 71 year Altered
Workshop CME 22 mars 2013 Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles Overcorrection of chronic hyponatremia CASE REPORT I (1) Female 71 year Altered
Hyponatremia and Hypomagnesemia
 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Workshop on Hyponatremia
 Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Pathophysiology of Water and Electrolyte Metabolism. Ágnes Haris MD, PhD Budapest
 Pathophysiology of Water and Electrolyte Metabolism Ágnes Haris MD, PhD Budapest A case of severe hyponatraemia initial steps 75 yrs old female Diabetic, but who refused taking her medications and keeping
Pathophysiology of Water and Electrolyte Metabolism Ágnes Haris MD, PhD Budapest A case of severe hyponatraemia initial steps 75 yrs old female Diabetic, but who refused taking her medications and keeping
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
HYPONATRAEMIA GUIDELINES
 HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
Each tablet contains:
 Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital
 JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
Hyponatraemia. Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals
 Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
Hyponatremia: A Review
 Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Hyponatremia in Heart Failure: why it is important and what should we do about it?
 Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
SAMSCA (tolvaptan) oral tablet
 oral tablet") SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
All but Vaptans. Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 All but Vaptans Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles [ Na ] = Na + e + K + e TBW 60 y BW 66 kg, TBW ± 33 L, SNa 140 meq/l TBW 1 L SNa: 3% (or 4.2
All but Vaptans Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles [ Na ] = Na + e + K + e TBW 60 y BW 66 kg, TBW ± 33 L, SNa 140 meq/l TBW 1 L SNa: 3% (or 4.2
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Supplemental Information
 FROM THE AMERICAN ACADEMY OF PEDIATRICS Supplemental Information SUPPLEMENTAL FIGURE 2 Forest plot of all included RCTs using a random-effects model and M-H statistics with the outcome of hyponatremia
FROM THE AMERICAN ACADEMY OF PEDIATRICS Supplemental Information SUPPLEMENTAL FIGURE 2 Forest plot of all included RCTs using a random-effects model and M-H statistics with the outcome of hyponatremia
Case Report Development of Severe Hyponatremia due to Salt-Losing Nephropathy after Esophagectomy for Esophageal Cancer
 Case Reports in Medicine Volume 009, Article ID 183, pages doi:10.1155/009/183 Case Report Development of Severe Hyponatremia due to Salt-Losing Nephropathy after Esophagectomy for Esophageal Cancer Katsunobu
Case Reports in Medicine Volume 009, Article ID 183, pages doi:10.1155/009/183 Case Report Development of Severe Hyponatremia due to Salt-Losing Nephropathy after Esophagectomy for Esophageal Cancer Katsunobu
Metabolism of water and electrolytes. 2. Special pathophysiology disturbances of intravascular volume and
 Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Cerebral Salt Wasting
 Cerebral Salt Wasting Heather A Martin MSN, RN, CNRN, SCRN Swedish Medical Center 1 Disclosures none 2 2 The problem Hyponatremia is the most common disorder of electrolytes encountered in medical practice
Cerebral Salt Wasting Heather A Martin MSN, RN, CNRN, SCRN Swedish Medical Center 1 Disclosures none 2 2 The problem Hyponatremia is the most common disorder of electrolytes encountered in medical practice
For more information about how to cite these materials visit
 Author(s): Roger Grekin, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Roger Grekin, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Neurohypophysis. AVP Receptors. Hyponatremia in Pituitary Disorders 9/29/2016. Lewis S. Blevins, Jr., M.D.
 in Pituitary Disorders Lewis S. Blevins, Jr., M.D. Neurohypophysis AVP secreting neurons in SON and PVN Osmo- and thirst receptors/centers in anterior hypothalamus Ascending pathways from ANS and brainstem
in Pituitary Disorders Lewis S. Blevins, Jr., M.D. Neurohypophysis AVP secreting neurons in SON and PVN Osmo- and thirst receptors/centers in anterior hypothalamus Ascending pathways from ANS and brainstem
Public Assessment Report. Scientific discussion. Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR
 SE/H/1443/01/MR") Public Assessment Report Scientific discussion Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR This module reflects the scientific discussion for the approval of Natriumklorid Abcur. The procedure
Public Assessment Report Scientific discussion Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR This module reflects the scientific discussion for the approval of Natriumklorid Abcur. The procedure
IX: Electrolytes. Sodium disorders. Specific Learning Objectives: Dan Henry, MD Clerkship Director University of Connecticut School of Medicine
 IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
Disorders o f of water water Detlef Bockenhauer
 Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Disclaimer. Chapter 3 Disorder of Water, Electrolyte and Acid-base Professor A. S. Alhomida. Disorder of Water and Electrolyte
 Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
 Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Extracellular fluid (ECF) compartment volume control
 compartment volume control") Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Faculty version with model answers
 Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Overview. Fluid & Electrolyte Disorders. Water distribution. Introduction 5/10/2014
 Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Correction of hypervolaemic hypernatraemia by inducing negative Na + and K + balance in excess of negative water balance: a new quantitative approach
 Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
Neuroendocrine challenges following hemispherectomy
 Neuroendocrine challenges following hemispherectomy Philip S. Zeitler MD. PhD Professor and Head Section of Endocrinology Children s Hospital Colorado University of Colorado Anschutz Medical Campus I am
Neuroendocrine challenges following hemispherectomy Philip S. Zeitler MD. PhD Professor and Head Section of Endocrinology Children s Hospital Colorado University of Colorado Anschutz Medical Campus I am
Functions of Proximal Convoluted Tubules
 1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017
 CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Hyponatremia 11/4/2010. Learning Objectives
 JAMES S. KALUS, PHARM.D, BCPS (AQ-CARDIOLOGY) Senior Manager, Patient Care Services, Department of Pharmacy Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE ANGELA STEWART, PHARM.D,
JAMES S. KALUS, PHARM.D, BCPS (AQ-CARDIOLOGY) Senior Manager, Patient Care Services, Department of Pharmacy Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE ANGELA STEWART, PHARM.D,
Hyponatremia in Children with Acute Central Nervous System Diseases
 Bahrain Medical Bulletin, Volume 30, No 1, March 2008 Hyponatremia in Children with Acute Central Nervous System Diseases Lamia M Al Naama, PhD* Meaad Kadhum Hassan, CABP** Entisar A. Al Shawi, MSc***
Bahrain Medical Bulletin, Volume 30, No 1, March 2008 Hyponatremia in Children with Acute Central Nervous System Diseases Lamia M Al Naama, PhD* Meaad Kadhum Hassan, CABP** Entisar A. Al Shawi, MSc***
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
Workshop on Hyponatremia. Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 Workshop on Hyponatremia Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles CASE REPORT I A 70-year-old female patient is hospitalized because she fall on the
Workshop on Hyponatremia Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles CASE REPORT I A 70-year-old female patient is hospitalized because she fall on the
For nearly 25 years, the treatment of hyponatremia
 The Treatment of Hyponatremia Richard H. Sterns, MD, Sagar U. Nigwekar, MD, and John Kevin Hix, MD Summary: Virtually all investigators now agree that self-induced water intoxication, symptomatic hospital-acquired
The Treatment of Hyponatremia Richard H. Sterns, MD, Sagar U. Nigwekar, MD, and John Kevin Hix, MD Summary: Virtually all investigators now agree that self-induced water intoxication, symptomatic hospital-acquired
Case Report Severe Hyponatremia due to Phlegmonous Trismus
 Case Reports in Dentistry, Article ID 320438, 4 pages http://dx.doi.org/10.1155/2014/320438 Case Report Severe Hyponatremia due to Phlegmonous Trismus Yoshihiro Momota, 1,2 Tomio Iseki, 3 and Tadashi Ohkubo
Case Reports in Dentistry, Article ID 320438, 4 pages http://dx.doi.org/10.1155/2014/320438 Case Report Severe Hyponatremia due to Phlegmonous Trismus Yoshihiro Momota, 1,2 Tomio Iseki, 3 and Tadashi Ohkubo
Treating the syndrome of inappropriate ADH secretion with isotonic saline
 Q J Med 1998; 91:749 753 Treating the syndrome of inappropriate ADH secretion with isotonic saline W. MUSCH and G. DECAUX1 From the Department of Internal Medicine, Bracops Hospital, Brussels, and 1Department
Q J Med 1998; 91:749 753 Treating the syndrome of inappropriate ADH secretion with isotonic saline W. MUSCH and G. DECAUX1 From the Department of Internal Medicine, Bracops Hospital, Brussels, and 1Department
Pediatric Sodium Disorders
 Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
hyponatremia/hypo-osmolality/hypotonic dehydration
 E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
Sym pt om s of "hyponat rem ia" Serum [Na + ] m Eq/ L: - Asymptomatic
![Sym pt om s of hyponat rem ia Serum [Na + ] m Eq/ L: - Asymptomatic](/thumbs/94/122329913.jpg "Sym pt om s of hyponat rem ia Serum [Na + ] m Eq/ L: - Asymptomatic") Sym pt om s of "" Serum [Na + ] >130 m Eq/ L: - Asymptomatic Serum [Na + ] 120-130 m Eq/ L: - Nausea, vomiting - Fatigue, muscle cramps - Abdominal symptoms - Mild cognitive - Gait disturbances Serum [Na
Sym pt om s of "" Serum [Na + ] >130 m Eq/ L: - Asymptomatic Serum [Na + ] 120-130 m Eq/ L: - Nausea, vomiting - Fatigue, muscle cramps - Abdominal symptoms - Mild cognitive - Gait disturbances Serum [Na
ACID-BASE AND ELECTROLYTE TEACHING CASE Treating Profound Hyponatremia: A Strategy for Controlled Correction
 ACID-BASE AND ELECTROLYTE TEACHING CASE Treating Profound Hyponatremia: A Strategy for Controlled Correction Richard H. Sterns, MD, John Kevin Hix, MD, and Stephen Silver, MD An alcoholic patient presented
ACID-BASE AND ELECTROLYTE TEACHING CASE Treating Profound Hyponatremia: A Strategy for Controlled Correction Richard H. Sterns, MD, John Kevin Hix, MD, and Stephen Silver, MD An alcoholic patient presented
diabetes in adults Metabolic complications of
 Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Taking Tolvaptan with a grain of salt. Jia (Shermaine) Ngo LMPS Pharmacy Resident October 7, 2016
 Ngo LMPS Pharmacy Resident October 7, 2016") Taking Tolvaptan with a grain of salt Jia (Shermaine) Ngo LMPS Pharmacy Resident 2016-2017 October 7, 2016 1 Learning Objectives Define Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Taking Tolvaptan with a grain of salt Jia (Shermaine) Ngo LMPS Pharmacy Resident 2016-2017 October 7, 2016 1 Learning Objectives Define Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Kidney Physiology. Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed
 Kidney Physiology Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed The purpose of tubular secrection To dispose of certain substances that are bound to plasma proteins. To
Kidney Physiology Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed The purpose of tubular secrection To dispose of certain substances that are bound to plasma proteins. To
Empowering Pharmacists to Improve Management of Hyponatremia. Learning Objectives. Diagnostic Algorithm for Hyponatremia
 Empowering Pharmacists to Improve Management of Hyponatremia A Patient-Centric, Process of Care Guide Learning Objectives Discuss the clinical consequences of undertreatment of hyponatremia, including
Empowering Pharmacists to Improve Management of Hyponatremia A Patient-Centric, Process of Care Guide Learning Objectives Discuss the clinical consequences of undertreatment of hyponatremia, including
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Management of hyponatremia: Providing treatment and avoiding harm
 REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will treat hyponatremia appropriately, taking care to avoid overcorrection CHIRAG VAIDYA, MD Tufts University School of Medicine; Renal Division, Baystate
REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will treat hyponatremia appropriately, taking care to avoid overcorrection CHIRAG VAIDYA, MD Tufts University School of Medicine; Renal Division, Baystate
SIMULTANEOUSLY PRESENTATION OF TWO PARANEOPLASTIC SYNDROMES IN A PATIENT WITH LUNG CARCINOMA
 Bulletin of the Transilvania University of Braşov Series VI: Medical Sciences Vol. 6 (55) No. 1-2013 SIMULTANEOUSLY PRESENTATION OF TWO PARANEOPLASTIC SYNDROMES IN A PATIENT WITH LUNG CARCINOMA A. STOICESCU
Bulletin of the Transilvania University of Braşov Series VI: Medical Sciences Vol. 6 (55) No. 1-2013 SIMULTANEOUSLY PRESENTATION OF TWO PARANEOPLASTIC SYNDROMES IN A PATIENT WITH LUNG CARCINOMA A. STOICESCU
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Two Little Water Cravers
 Two Little Water Cravers Baby Mo (5mths/M) Chief complaint Repeated vomiting since 2 months old with poor weight gain PMH Gestation 40+6wks, BW 3.375kg Hx of fracture Rt clavicle at birth HbH disease on
Two Little Water Cravers Baby Mo (5mths/M) Chief complaint Repeated vomiting since 2 months old with poor weight gain PMH Gestation 40+6wks, BW 3.375kg Hx of fracture Rt clavicle at birth HbH disease on
CLINICAL GUIDELINE FOR THE MANAGEMENT OF HYPONATRAEMIA Summary. Start. End. Key: Na + below normal range ( mmol/L) Symptomatic?
 Symptomatic?") CLINICAL GUIDELINE FOR THE MANAGEMENT OF HYPONATRAEMIA Summary Key: General tes ED/MAU/SRU/Acute GP/Amb-Care GP/SWASFT In-patient wards Start Na + below normal range (135 145mmol/L) Refer to endocrinology
CLINICAL GUIDELINE FOR THE MANAGEMENT OF HYPONATRAEMIA Summary Key: General tes ED/MAU/SRU/Acute GP/Amb-Care GP/SWASFT In-patient wards Start Na + below normal range (135 145mmol/L) Refer to endocrinology
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Endocrine Emergencies: Recognition and Management
 Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Regulation of fluid and electrolytes balance
 Regulation of fluid and electrolytes balance Three Compartment Fluid Compartments Intracellular = Cytoplasmic (inside cells) Extracellular compartment is subdivided into Interstitial = Intercellular +
Regulation of fluid and electrolytes balance Three Compartment Fluid Compartments Intracellular = Cytoplasmic (inside cells) Extracellular compartment is subdivided into Interstitial = Intercellular +
Utility and Limitations of the Traditional Diagnostic Approach to Hyponatremia: A Diagnostic Study
 CLINICAL RESEARCH STUDY Utility and Limitations of the Traditional Diagnostic Approach to Hyponatremia: A Diagnostic Study Wiebke Fenske, a Sebastian K. G. Maier, b Anne Blechschmidt, a Bruno Allolio,
CLINICAL RESEARCH STUDY Utility and Limitations of the Traditional Diagnostic Approach to Hyponatremia: A Diagnostic Study Wiebke Fenske, a Sebastian K. G. Maier, b Anne Blechschmidt, a Bruno Allolio,
Caledonian Society Endocrinology & Diabetes, Dunkeld 2014 Hyponatraemia guidelines. an inside view
 Caledonian Society & Diabetes, Dunkeld 2014 Hyponatraemia guidelines an inside view Dr Steve Ball Endocrine Unit, Hospitals NHS Trust & The Medical School Hyponatraemia assessment, management & guidance
Caledonian Society & Diabetes, Dunkeld 2014 Hyponatraemia guidelines an inside view Dr Steve Ball Endocrine Unit, Hospitals NHS Trust & The Medical School Hyponatraemia assessment, management & guidance
SODIUM BALANCE Overview
 SODIUM BALANCE Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS III Seminar VJ Temple 1 How are solute and solvent related to solution?
SODIUM BALANCE Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS III Seminar VJ Temple 1 How are solute and solvent related to solution?
EXCRETION QUESTIONS. Use the following information to answer the next two questions.
 EXCRETION QUESTIONS Use the following information to answer the next two questions. 1. Filtration occurs at the area labeled A. V B. X C. Y D. Z 2. The antidiuretic hormone (vasopressin) acts on the area
EXCRETION QUESTIONS Use the following information to answer the next two questions. 1. Filtration occurs at the area labeled A. V B. X C. Y D. Z 2. The antidiuretic hormone (vasopressin) acts on the area
Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi
 Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi At the end of this lecture student should be able to describe: The loop of Henle is referred to as countercurrent
Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi At the end of this lecture student should be able to describe: The loop of Henle is referred to as countercurrent
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
Disorders of Water Metabolism
 Disorders of Water Metabolism Joshua M. Thurman and Tomas Berl 2 Introduction Disorders of water balance and serum Na ( S Na ) are very common in hospitalized patients [ 1 ]. In health, water balance and
Disorders of Water Metabolism Joshua M. Thurman and Tomas Berl 2 Introduction Disorders of water balance and serum Na ( S Na ) are very common in hospitalized patients [ 1 ]. In health, water balance and
After i.v injection 45% of the amount of desmopressin is found in the urine within 24 hours.
 MINIRIN Tablets 0.1 and 0.2 mg Declaration Tablets 0.1 mg. Each tablet contains desmopressin acetate 0.1 mg and excipients q.s Tablets 0.2 mg. Each tablet contains desmopressin acetate 0.2 mg and excipients
MINIRIN Tablets 0.1 and 0.2 mg Declaration Tablets 0.1 mg. Each tablet contains desmopressin acetate 0.1 mg and excipients q.s Tablets 0.2 mg. Each tablet contains desmopressin acetate 0.2 mg and excipients
Eggplant: The Story of Sodium in Neurocritical Care
 Eggplant: The Story of Sodium in Neurocritical Care Larry Burris, DO Medical Director NCC - Sanford Health Medical Director Renal Transplant - Sanford Health Assistant Professor of Medicine SSOM NaCl Facts
Eggplant: The Story of Sodium in Neurocritical Care Larry Burris, DO Medical Director NCC - Sanford Health Medical Director Renal Transplant - Sanford Health Assistant Professor of Medicine SSOM NaCl Facts