The Case of the Adrenal Mass
|
|
|
- Brianne Kennedy
- 5 years ago
- Views:
Transcription

1 The Case of the Adrenal Mass Functional Adrenal Tumors Patricia Leung Kings County Hospital
2 Case presentation 62 year old F PMH: HTN, DM, arthritis PSH: none Meds: Metoprolol, Nifedipine, Losartan, Chlorthalidone, ASA, Metformin, Glipizide NKDA No EtOH/drug/tobacco use
3 July 2012 c/o palpitations VS: BP 152/60 HR 116 RR 16 Afebrile Exam: Gen: obese, nad, A+Ox3 CV: tachycardic, regular rhythm Skin: multiple hyperpigmented macules, no striae, bruising, or abnormal hair growth Abd: obese, soft, nontender to palpation
4 EKG: sinus tachycardia, LVH Labs: Na 139 K 3.1 BUN/Cr 29/1.36 Gluc 175 Imaging: Albumin 4.4 TSH 0.6 T Troponin negative x3 ECHO EF 50-55%, LVH CTA C/A/P

5

6
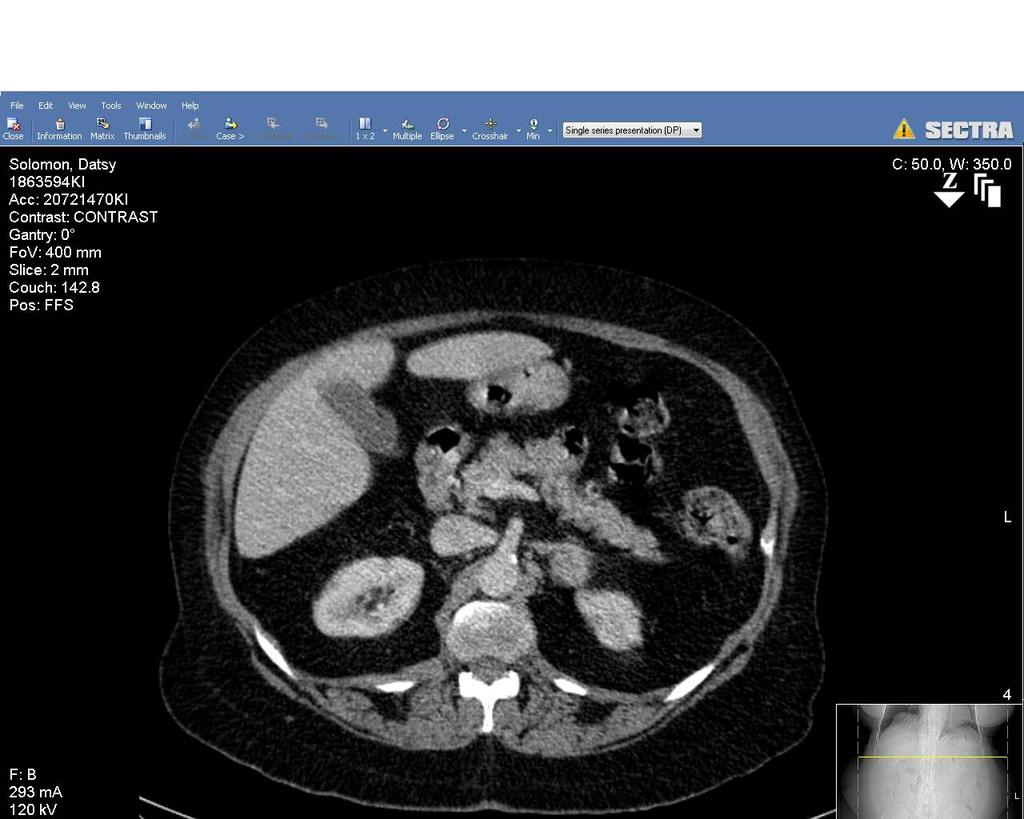
7
8 Lab workup Test Value Normal range Aldosterone 5 <28 (ng/dl) Renin (ng/ml/h) ACTH (pg/ml) Urine catecholamine WNL Serum cortisol (ug/dl) Urine cortisol (ug/24hr) Dexamethasone suppression test (mcg/dl)

9 Surgery clinic appointments July October 2013 February 2014 March 2014 May 2014 scheduled for surgery cancelled by patient for personal reasons


10 9/2/14 Laparoscopic left adrenalectomy Post-operative steroid taper Discharged home POD#3 Pathology: adenoma



11 Introduction 1563 Eustachius first anatomic account 1805 Cuvier described anatomic division of cortex and medulla 1855 Addison described adrenal insufficiency 1885 Frankel identified pheochromocytoma 1897 Adrenaline identified as agent of adrenal medulla elevating BP in dogs 1932 Cushing described 11 patients with moon facies, truncal obesity, hypertension 1952 Aldosterone identified by Conn
12 Anatomy Arterial 3 sources 1. Inferior phrenic 2. Renal artery 3. Aorta Venous Right IVC Left renal vein

13 Pop quiz! Arterial 3 sources 1. Inferior phrenic 2. Renal artery 3. Aorta Venous Right IVC Left renal vein


14 Anatomy
15
16 Aldosterone Major adrenal mineralocorticoid Regulated by the reninangiotensin system Decreased renal blood flow, decreased plasma sodium, increased sympathetic tone renin release Function increase Na reabsorption and K and H+ excretion at renal distal convoluted tubule

17 Cortisol Major adrenal glucocorticoid Hypothalamic-pituitary-adrenal axis Diurnal variation


18 Androgens DHEA, DHEAS Peripheral conversion to testosterone and dihydrotestosterone Fetal development male genitalia Development of secondary sexual characteristics at puberty Androgen excess o Boys - precocious puberty in boys o Girls - acne, and hirsutism, anovulation
19 Catecholamines Norepinephrine, epinephrine, dopamine Adrenal medulla Synthesis from Tyrosine N-methyltransferase present in adrenal glands Metabolism to metanephrines, normetanephrines, VMA
20 Functional Adrenal Tumors
21 Benign Cortisol-producing (Cushing s syndrome) Aldosteronoma (Conn s syndrome) Sex-steroid-producing Pheochromocytoma Malignant Adrenal cortical carcinoma Malignant pheochromocytoma Metastatic disease to adrenal gland
22 Benign

23 Cortisol-producing Adenoma Cushing s syndrome complex of symptoms related to hypersecretion of cortisol regardless of etiology Cushing s disease pituitary tumor


24 Cortisol-producing adenoma: H+P Hypertension, diabetes, osteopenia ROS: Generalized weakness, headaches, weight gain, depression, emotional lability, decreased libido, menstrual irregularities Exam: Central obesity, moon facies, buffalo hump, supraclavicular fat pads, purple striae, acne
25 Cortisol-producing adenoma: Laboratory studies Elevated 24 hour urinary cortisol level OR Low-dose dexamethasone suppression test STEP 1: Determine Hypercortisolism Plasma ACTH levels Suppressed Primary cortisol-secreting adrenal tumors Elevated Adrenal hyperplasia due to pituitary tumor and CRH-secreting tumors; highest in those with ectopic ACTH producing tumors STEP 2: ACTHindependent or dependent High-dose dexamethasone suppression test Failure to suppress urinary cortisol by 50% Ectopic Suppression: pituitary tumor STEP 3: Ectopic or pituitary



26 CT Cortisol-producing adenoma: Imaging Hounsfield unit (HU) <10 Percentage washout - HIGH MRI Better assessment vascular anatomy
27 Cortisol-producing adenoma: Treatment Laparoscopic adrenalectomy Pre and post-operative steroids Duration of treatment ACTH stimulation test

28 Aldosteronoma (Conn s syndrome) Hyperaldosteronism renal artery stenosis, CHF, cirrhosis, b/l adrenal hyperplasia Primary hyperaldosteronism autonomous aldosterone secretion suppression of renin secretion years 1% hypertension Associated with hypokalemia
29 Aldosteronoma (Conn s syndrome) H+P Hypertension Difficult control multiple drug Rx ROS: weakness, fatigue, headaches, polydipsia/polyuria, muscle weakness

30 Aldosteronoma (Conn s syndrome) Laboratory studies Na, K Hypokalemia on diuretic therapy Aldosterone:renin ratio >30 suspect Sodium loading test No suppression

31 Aldosteronoma (Conn s syndrome) Localization/Imaging CT/MRI Equivocal: Adrenal vein sampling Lateralization: aldosteronoma Non-lateralization: bilateral adrenal hyperplasia NP 59 study
32 Aldosteronoma (Conn s syndrome) Treatment Aldosteronoma Pre-op HTN control, correction of K laparoscopic adrenalectomy or posterior open approach unless carcinoma suspected anterior abdominal approach Post-op mineralocorticoid for up to 3 months Bilateral adrenal hyperplasia medical management - spironolactone


33 Sex-steroid producing adenoma Women hirsutism, amenorrhea, infertility, increased muscle mass, deepened voice, temporal balding Men present in advanced stages Children accelerated growth, premature development of facial and pubic hair, acne, genital enlargement, deepening of voice Feminizing tumors least common Men gynecomastia, impotence, testicular atrophy Women irregular menses or dysfunctional uterine bleeding Girls precocious puberty, early menarche

34 Sex-steroid producing adenoma Labs/Treatment Androgen precursor DHEA Measure 17-ketosteroids Adrenalectomy Metastatic disease adrenolytic drugs Mitotane Ketoconazole

35 Pheochromocytoma Chromaffin cells Rare, % Male=Female Rule of 10s: 10% bilateral 10% malignant 10% pediatric patients 10% extra-adrenal 10% familial (MEN2a, MEN2b, VHL) Found in % of hypertensive patients Extra-adrenal 3x more malignant
36 Pheochromocytoma H+P Headaches, palpitations, diaphoresis Classic triad Anxiety, tremulousness, chest pain, SOB, nausea/vomiting Hypertension most common Sudden death in patients with undiagnosed tumors undergoing biopsy or other surgeries

37 Pheochromocytoma Labs


38 Pheochromocytoma Imaging CT 85-95% sensitive Should include diaphragm to aortic bifurcation MRI more sensitive and specific Metaiodobenzylguanidine (MIBG) -
39 Pheochromocytoma Management PREOP 1. Alpha-blockade Phenoxybenzamine Start 1-3 weeks prior to surgery (10 mg BID) Volume repletion 2. Beta-blockade Propanolol mg q6-8 H Must administer after alpha-blockade! SURGERY Laparoscopic adrenalectomy <5cm, o/w open Minimal tumor manipulation/capsule rupture Induction Intraoperative BP control Post-op volume repletion
40 Malignant
41 Adrenocortical carcinoma Incidence 2 in1 million Bimodal age distribution Majority sporadic, some assocation with germline mutations Large tumors (>6cm) at time of Dx Hypersecretory or mixed 50% non-functioning 0-25% of incidentalomas Poor prognosis (median survival 18 months - 35% Mixed - 30% cortisol - 20% androgens - 10% estrogens - 2% aldosterone
42 Adrenocortical carcinoma H+P Functioning tumors often present with Cushing s syndrome + virilizing features Non-functioning Enlarging abdominal mass Abdominal or back pain Weight loss, anorexia, nausea

43 Adrenocortical carcinoma Labs/Imaging CT/MRI Size *** >6cm Tumor heterogeneity, irregular margins, presence of hemorrhage, adjacent lymphadenopathy, liver metastases

44 Adrenocortical carcinoma Treatment Most important predictor of survival adequacy of resection Complete resection 32-48% 5 year survival Incomplete excision median survival <1 year
45 Adrenal metastases Common site of metastasis Breast, lung, GI tract, melanoma, kidney Autopsy review, metastases found in 27% of 1,000 patients Most asymptomatic, incidental finding Imaging delayed contrast washout FNA after r/o pheochromocytoma Surgical resection if solitary Improved survival 31 months vs. 8.5 months
46 Adrenal Incidentaloma Definition % incidence on CT Autopsies: 1.4-9%

47 Size does matter? Risk of malignancy <2% in <4cm 6% 4-6 cm >25% in >6cm

48 Adrenal Incidentalomas 2 questions: Is it functional Is it malignant surgery
49 Question 1 A 45 year old woman with a hx of HTN undergoes CT A/P after presenting to the ER with RLQ pain. The study is negative except for an incidentally found 3 cm mass in the R adrenal. Evaluation reveals elevated urine metanephrines. Based on this result the lesion is most likely located in the: A. Zona glomerulosa B. Zona fasciculate C. Zona reticularis D. Medulla E. Para-adrenal tissues
50 Question 1 A 45 year old woman with a hx of HTN undergoes CT A/P after presenting to the ER with RLQ pain. The study is negative except for an incidentally found 3 cm mass in the R adrenal. Evalution reveals elevated urine metanephrines. Based on this result the lesion is most likely located in the: A. Zona glomerulosa B. Zona fasciculate C. Zona reticularis D. Medulla E. Para-adrenal tissues
51 Question 2 A 47 year old female has recent onset headaches, palpitations, sweating and heat intolerance. On PE her BP 190/100 and her HR 110. Biochemical evaluation revealed an elevated plasma metanephrine level and elevated 24 hr urinary metanephrine level. A CT A/P demonstrates 3 cm left adrenal mass. Which of the following should be the next most appropriate step? A. MIBG scan B. Somatostatin scintigraphy C. MRI D. PET E. No further imaging needed
52 Question 2 A 47 year old female has recent onset headaches, palpitations, sweating and heat intolerance. On PE her BP 190/100 and her HR 110. Biochemical evaluation revealed an elevated plasma metanephrine level and elevated 24 hr urinary metanephrine level. A CT A/P demonstrates 3 cm left adrenal mass. Which of the following should be the next most appropriate step? A. MIBG scan B. Somatostatin scintigraphy C. MRI D. PET E. No further imaging needed
53 Question 3 A 51 year old female reports significant weight gain over the past 6 months. In this period she had 2 episodes of UTI and noticed that she bruised more easily. On PE her BP 150/95. She is 68 inches tall and weighs 250 lbs. She has a characteristic bulge of fat on her back and striae on her abdomen. Which of the following statements about the disease is TRUE? A. Ectopic ACTH secretion is most often caused by medullary thyroid cancer B. Cushing disease is the most common cause of endogenous Cushing s syndrome C. An elevated spot urinary free cortisol is diagnostic for Cushing s syndrome D. Cushing s syndrome can be excluded by measuring a C-peptide level E. An adrenal adenoma causes ACTH-dependent Cushing s syndrome
54 Question 3 A 51 year old female reports significant weight gain over the past 6 months. In this period she had 2 episodes of UTI and noticed that she bruised more easily. On PE her BP 150/95. She is 68 inches tall and weighs 250 lbs. She has a characteristic bulge of fat on her back and striae on her abdomen. Which of the following statements about the disease is TRUE? A. Ectopic ACTH secretion is most often caused by medullary thyroid cancer B. Cushing disease is the most common cause of endogenous Cushing s syndrome C. An elevated spot urinary free cortisol is diagnostic for Cushing s syndrome D. Cushing s syndrome can be excluded by measuring a C-peptide level E. An adrenal adenoma causes ACTH-dependent Cushing s syndrome
55 References Brian J. Gallay, MD PhD a, b, c, Suhail Ahmad, MD a, b, c, Lei Xu, PhD a, b, c, Bert Toivola, PhD a, b, c, Robert C. Davidson, MD, a, b, c, Screening for primary aldosteronism without discontinuing hypertensive medications: Plasma aldosterone-renin ratio American Journal of Kidney Diseases, Volume 37, Issue 4, April 2001, Pages Paolo Mulatero, Franco Rabbia, Alberto Milan, Cristina Paglieri, Fulvio Morello,Livio Chiandussi, Franco Veglio Drug Effects on Aldosterone/Plasma Renin Activity Ratio in Primary Aldosteronism Hypertension.2002; 40: William F. Young* and Anthony W. Stanson, What are the keys to successful adrenal venous sampling (AVS) in patients with primary aldosteronism? Clinical Endocrinology (2009) 70, Paul R. Gittens Jr., Surgical management of metastatic disease to the adrenal gland Jefferson Digital Commons April 2008 Schwartz Chapter 38: Thyroid, Parathyroid, and Adrenal Terzolo, M; Subclinical Cushing s syndrome: Definition and Management; Clinical Endocrinology, :12-18 Luketich JD, Burt ME. Does resection of adrenal metastases from non-small cell lung cancer improve survival? Ann Thorac Surg. 1996;62: Williams Textbook of Endocrinology: Adrenal adenomas, incidentalomas, and carcinomas
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Adrenal Incidentalomas. G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine
 Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Adrenal and retropetionium
 Adrenal and retropetionium Disorders of the Adrenal Cortex Hyperaldosteronism: Hyperaldosteronism may be secondary to stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow
Adrenal and retropetionium Disorders of the Adrenal Cortex Hyperaldosteronism: Hyperaldosteronism may be secondary to stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Morbidity & Mortality. Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005
 Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
PHEOCHROMOCYTOMA. Anita Chiu, MD Kings County Hospital Center January 13, 2011
 PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
The Adrenal Glands. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement. II.
 The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
ENDOCRINOLOGY 3. R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice
 Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
RECURRENT ADRENAL DISEASE. Megan Applewhite Endorama 2/19/2015 SR , SC
 RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pathophysiology of Adrenal Disorders
 Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
ADRENAL GLAND. Introduction 4/21/2009. Among most important and vital endocrine organ. Small bilateral yellowish retroperitoneal organ
 Introduction Among most important and vital endocrine organ ADRENAL GLAND D.Hammoudi.MD Small bilateral yellowish retroperitoneal organ Lies just above kidney in gerota s fascia 2 1 The Adrenal Gland Anatomy
Introduction Among most important and vital endocrine organ ADRENAL GLAND D.Hammoudi.MD Small bilateral yellowish retroperitoneal organ Lies just above kidney in gerota s fascia 2 1 The Adrenal Gland Anatomy
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
Read the following article and answer the questions that follow. Refer to the Keys section to check your answers.
 ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
ADRENAL LESIONS 10/09/2012. Adrenal + lesion. Introduction. Common causes. Anatomy. Financial disclosure. Dr. Boraiah Sreeharsha. Nothing to declare
 ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia
 Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Case Presentation. Gordon Callender, MD Department of Surgery PGY-4
 Case Presentation Gordon Callender, MD Department of Surgery PGY-4 History Chief Complaint: Abdominal pain History of Present Illness: 43 y.o. black female with multiple medical problems presented to the
Case Presentation Gordon Callender, MD Department of Surgery PGY-4 History Chief Complaint: Abdominal pain History of Present Illness: 43 y.o. black female with multiple medical problems presented to the
Where in the adrenal cortex is cortisol produced? How do glucocorticoids inhibit prostaglandin production?
 CASE 35 A 36-year-old woman presents to her gynecologist with complaints of amenorrhea and hirsutism. She has also noticed an increase in her weight (especially in the trunk region) and easy fatigability.
CASE 35 A 36-year-old woman presents to her gynecologist with complaints of amenorrhea and hirsutism. She has also noticed an increase in her weight (especially in the trunk region) and easy fatigability.
adrenal and parathyroid glands Done by jehad abdel aziz
 15-11-09 prof. muhammed khammash adrenal and parathyroid glands Done by jehad abdel aziz The adrenal glands:- Anatomy:- The adrenal glands are flattened, yellowish structures that weigh less than 10g in
15-11-09 prof. muhammed khammash adrenal and parathyroid glands Done by jehad abdel aziz The adrenal glands:- Anatomy:- The adrenal glands are flattened, yellowish structures that weigh less than 10g in
ADRENAL GLANDS. G M Kellerman. Hunter Area Pathology Service
 ADRENAL GLANDS G M Kellerman Hunter Area Pathology Service ADRENAL FUNCTIONS THE ADRENAL GLANDS ACTUALLY HAVE 4 QUITE SEPARATE FUNCTIONS 1. MINERALOCORTICOID SECRETION BY THE ZONA GLOMERULOSA OF THE CORTEX
ADRENAL GLANDS G M Kellerman Hunter Area Pathology Service ADRENAL FUNCTIONS THE ADRENAL GLANDS ACTUALLY HAVE 4 QUITE SEPARATE FUNCTIONS 1. MINERALOCORTICOID SECRETION BY THE ZONA GLOMERULOSA OF THE CORTEX
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Ch 8: Endocrine Physiology
 Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa Qiao.Li@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa Qiao.Li@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases. The Pathological Basis of Disease
 Endocrine Diseases The Pathological Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Management of adrenal incidentalomas
 31 Management of adrenal incidentalomas KEVIN MURTAGH, NANA MUHAMMAD AND MAREK MILLER The return of a scan result with reference to an incidental finding of an adrenal mass is a common scenario. 1 The
31 Management of adrenal incidentalomas KEVIN MURTAGH, NANA MUHAMMAD AND MAREK MILLER The return of a scan result with reference to an incidental finding of an adrenal mass is a common scenario. 1 The
Hyperandrogenism. Dr Jack Biko. MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany)
, MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany)") Hyperandrogenism Dr Jack Biko MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany) 2012 Hyperandrogenism Excessive production of androgens Adrenal glands main source
Hyperandrogenism Dr Jack Biko MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany) 2012 Hyperandrogenism Excessive production of androgens Adrenal glands main source
Case. 24 year old female presented to your office complaining of excess hair growth on her face and abdomen. Questions?
 Hirsutism Case 24 year old female presented to your office complaining of excess hair growth on her face and abdomen Questions? Started around puberty with gradual progression Irregular menstrual cycle
Hirsutism Case 24 year old female presented to your office complaining of excess hair growth on her face and abdomen Questions? Started around puberty with gradual progression Irregular menstrual cycle
Adrenal disease Real and Unreal. Objectives. Real
 Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
3 year old boy with puberty. Katie Stanley, MD August 1, 2013
 3 year old boy with puberty Katie Stanley, MD August 1, 2013 Initial presentation 3 and 11/12 year old boy with signs of puberty Presented to outside endocrinologist in 2002 with: Pubic hair since 2.5
3 year old boy with puberty Katie Stanley, MD August 1, 2013 Initial presentation 3 and 11/12 year old boy with signs of puberty Presented to outside endocrinologist in 2002 with: Pubic hair since 2.5
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
CUSHING S SYNDROME. Chapter 8. Case: A 43-year-old man with delusions
 Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Adrenal gland And Pancreas
 Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Adrenocortical Scan. Quality Control. Adult Dose Range
 chapter 1 Adrenocortical Scan RADIOPHARMACY Radionuclide 131 I t 1/2 : 8.1 days Energies: 364 kev Type: β, γ, fission product Radiopharmaceutical 131 I-6-β-Iodomethyl-19-norcholesterol (NP-59). Available
chapter 1 Adrenocortical Scan RADIOPHARMACY Radionuclide 131 I t 1/2 : 8.1 days Energies: 364 kev Type: β, γ, fission product Radiopharmaceutical 131 I-6-β-Iodomethyl-19-norcholesterol (NP-59). Available
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology
 Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW
 CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
The Endocrine System
 The Endocrine System Glands are modified epithelium which produces certain secretions. TYPES OF GLANDS: Exocrine Gland/Duct Gland Secretions of these Glands are carried to the site of action through fine
The Endocrine System Glands are modified epithelium which produces certain secretions. TYPES OF GLANDS: Exocrine Gland/Duct Gland Secretions of these Glands are carried to the site of action through fine
The Adrenal Glands. Bởi: OpenStaxCollege
 The Adrenal Glands Bởi: OpenStaxCollege The adrenal glands are wedges of glandular and neuroendocrine tissue adhering to the top of the kidneys by a fibrous capsule ([link]). The adrenal glands have a
The Adrenal Glands Bởi: OpenStaxCollege The adrenal glands are wedges of glandular and neuroendocrine tissue adhering to the top of the kidneys by a fibrous capsule ([link]). The adrenal glands have a
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens
 Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Adrenal masses in infancy and childhood: A clinical and radiological overview M. Mearadji
 Adrenal masses in infancy and childhood: A clinical and radiological overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neoplastic adrenal masses usually originate from
Adrenal masses in infancy and childhood: A clinical and radiological overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neoplastic adrenal masses usually originate from
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Current Management of Adrenal Cortical Carcinoma
 Current Management of Adrenal Cortical Carcinoma American Association of Clinical Endocrinologists Texas Chapter of the AACE Annual Meeting And Texas Endocrine Surgery Symposium August 4, 2017 Jeffrey
Current Management of Adrenal Cortical Carcinoma American Association of Clinical Endocrinologists Texas Chapter of the AACE Annual Meeting And Texas Endocrine Surgery Symposium August 4, 2017 Jeffrey
Adrenal Glands. Huiping Wang ( 王会平 ), PhD. Rm C541, Block C, Research Building, School of Medicine Tel:
, PhD. Rm C541, Block C, Research Building, School of Medicine Tel:") Adrenal Glands Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline The Adrenal Glands The adrenal cortex The Adrenal Medulla
Adrenal Glands Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline The Adrenal Glands The adrenal cortex The Adrenal Medulla
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
14 Girl with Cushing s Disease: An Update. Kristen Dillard, MD Endorama October 17, 2013
 14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System
 PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
Il Carcinoma Surrenalico
 Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
ComprehensivePLUS Hormone Profile with hgh
 OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
Pathophysiology of the th E d n ocr i ne S S t ys em B. Marinov, MD, PhD Endocrine system Central: Hypothalamus
 Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
The Metabolic System. Physiologic Integrity and Therapeutic Nursing Interventions for Patients With Endocrine Needs. The Endocrine System
 Physiologic Integrity and Therapeutic Nursing Interventions for Patients With Endocrine Needs Black, J.M. & Hawks, J.H. (2005) Chapters 44, (pp 1154-1189) Baptist Health School of Nursing NSG 4037: Adult
Physiologic Integrity and Therapeutic Nursing Interventions for Patients With Endocrine Needs Black, J.M. & Hawks, J.H. (2005) Chapters 44, (pp 1154-1189) Baptist Health School of Nursing NSG 4037: Adult
Therapeutic Cohort Results
 Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Puberty and Pubertal Disorders Part 2: Precocious Puberty. These podcasts are designed to give medical students an overview
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Puberty and Pubertal Disorders Part 2: Precocious Puberty. These podcasts are designed to give medical students an overview
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Endocrinology and VHL: The adrenal and the pancreas
 Overview Endocrinology and VHL: The adrenal and the pancreas LAUREN FISHBEIN MD, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE DIVISION OF ENDOCRINOLOGY, METABOLISM AND DIABETES DIVISION OF BIOMEDICAL
Overview Endocrinology and VHL: The adrenal and the pancreas LAUREN FISHBEIN MD, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE DIVISION OF ENDOCRINOLOGY, METABOLISM AND DIABETES DIVISION OF BIOMEDICAL
THE ENDOCRINE AND REPRODUCTIVE SYSTEMS
 THE ENDOCRINE AND REPRODUCTIVE SYSTEMS The focus of this week s lab will be pathology of the endocrine and reproductive systems. There are a bunch of tissues and topics that can be covered in these systems,
THE ENDOCRINE AND REPRODUCTIVE SYSTEMS The focus of this week s lab will be pathology of the endocrine and reproductive systems. There are a bunch of tissues and topics that can be covered in these systems,
4.04 Understand the Functions and Disorders of the ENDOCRINE SYSTEM Understand the functions and disorders of the endocrine system
 4.04 Understand the Functions and Disorders of the 4.04 Understand the Functions and Disorders of the What are the functions of the endocrine system? What are some disorders of the endocrine system? How
4.04 Understand the Functions and Disorders of the 4.04 Understand the Functions and Disorders of the What are the functions of the endocrine system? What are some disorders of the endocrine system? How
Adrenal Gland. Zona Glomerulosa (mineralcorticoids) Zona Fasciculata (glucocorticoids) Zona Reticularis (sexual hormones) Adrenaline and noradrenaline
 Zona Fasciculata (glucocorticoids) Zona Reticularis (sexual hormones) Adrenaline and noradrenaline") n Cortex Zona Glomerulosa (mineralcorticoids) Zona Fasciculata (glucocorticoids) Zona Reticularis (sexual hormones) n Medulla Adrenaline and noradrenaline n Adrenocortical Hyperfunction Hyperaldosteronism
n Cortex Zona Glomerulosa (mineralcorticoids) Zona Fasciculata (glucocorticoids) Zona Reticularis (sexual hormones) n Medulla Adrenaline and noradrenaline n Adrenocortical Hyperfunction Hyperaldosteronism
ADRENAL GLANDS HORMONES
 ADRNAL GLANDS HORMONS Glands Cortex 80% mesoderm Mineralococorticoids Glucocorticoids (phenylethanolamine N- methyl transferase) A Sex Hormones Catecholamines Medulla 20% PNMT, N neuroectoderm N PNMT V
ADRNAL GLANDS HORMONS Glands Cortex 80% mesoderm Mineralococorticoids Glucocorticoids (phenylethanolamine N- methyl transferase) A Sex Hormones Catecholamines Medulla 20% PNMT, N neuroectoderm N PNMT V
One Day Hormone Check
 One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
2402 : Anatomy/Physiology
 Dr. Chris Doumen Lecture 4 2402 : Anatomy/Physiology Major Endocrine Organs Calci u m H o me os t asis TextBook Readings Pages 624 through 632. Make use of the figures in your textbook ; a picture is worth
Dr. Chris Doumen Lecture 4 2402 : Anatomy/Physiology Major Endocrine Organs Calci u m H o me os t asis TextBook Readings Pages 624 through 632. Make use of the figures in your textbook ; a picture is worth
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules. Celeste Thomas November 1, 2012
 57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank