ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits
|
|
|
- Hester Parsons
- 5 years ago
- Views:
Transcription
1 ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits Charitini Salla, MD Head of Cytopathology Department, Hygeia Hospital, Athens, Greece
2 There is no conflict of interest
3 Methods of cytological material collection by FNA CT-guided FNA Transabdominal US-guided FNA Transgastric or transduodenal EUS-FNA Intraoperative FNA is a also a possibility
4 Indications for FNA Most of the times, presence of a mass lesion: solid solid and cystic cystic Organ-specific lesions non-organ-specific lesions (lymphomas, metastases, mesenchymal neoplasms) Sometimes, a diffuse lesion can be sampled

5 EUS-FNA
6 ROSE in Cytology is the equivalent of Frozen section in Pathology
7 Why is ROSE necessary? Decreases: number of non-diagnostic samples number of passes in the lesion patient discomfort cost for health care system
8 PANCREATIC LESIONS SOLID CYSTIC
9 ROSE Recommended for solid lesions: Obtain adequate lesional sampling for a definite diagnosis, taking into account the endoscopist s sonographic impression Prepare the sample for ancillary studies: histochemical, immunohistochemical, biochemical, flow cytometry, molecular (as NGS) and cytogenetic (as FISH) The adequacy of the specimen depends on: size of the lesion nature of the lesion Non-cellular smears in: cystic lesions desmoplasia or necrosis number of passes experience of the endoscopist
10 Valuable information before ROSE Demographic data (gender, age) Clinical data Patient history with emphasis on: alcoholism obesity cigarette smoking pancreatic injury medications toxins infections (toxoplasmosis, adenovirus, TB) malnutrition metabolic disorders IgG4-related diseases polyarteritis nodosa family history of cancer cystic fibrosis other cancer diseases of the biliary tract hyperparathyroidism Signs: Courvoisier Virchow Cullen Grey Turner Symptoms: malaise, fatigue anorexia, weight loss abdominal or back pain recurrent acute pancreatitis nausea and vomiting diarrhea fever and chills ascites / pleural effusion malabsorption new-onset diabetes hyperbilirubinemia (jaundice, pruritus, dark urine, pale colored stools) Syndromes VHL MEN I Peutz-Jeghers FAMMM Beckwith-Wiedemann Trousseau syndrome (hypercoagulability) lipase hypersecrection syndrome clinical syndrome due to hormone production Before ROSE, the cytopathologist should be informed about the most striking features concerning the examined patient
11 Valuable information before ROSE Serum biochemical tests: CEA, Ca19-9 IgG4 amylase, lipase, bilirubin Imaging findings other than EUS* CT/MRI: solid/cystic lesion size and borders of the lesion when cystic: presence of capsule, pattern of calcification location in the pancreas invasion of the adjacent organs probable metastasis in the liver or peripancreatic lymph nodes structural abnormalities, such as pancreas divisum ERCP/MRCP: dilation of ductal system detection of stones or mural nodules in the ductal system communication with the pancreatic ductal system Previous cytological examination Transgastric or transduodenal approach Before ROSE, the cytopathologist should be informed about the most striking features concerning the examined patient

12 Diagnostic approach of the pancreatic lesion Normal vs. lesional tissue Lesional tissue vs. gastrointestinal and pancreatic contamination IF POSSIBLE, allocation of the lesion into one of the diagnostic categories proposed by The Papanicolaou Society of Cytopathology System for Reporting Pancreatobiliary Cytology (Nondiagnostic) Negative Atypical Neoplastic: benign / other Suspicious Positive During the ROSE, most of the times we try to classify the lesion as positive, negative or belonging in the grey zone Identification of the lesion The grey zone includes both: premalignant lesions specimens with various degrees of reactive atypia
 Second step Glandular smear pattern Other lymphoma sarcoma non-aca met Solid")
 metastatic adenocarcinoma Differential diagnosis: PanNET SPN acinar cell")
13 ROSE of solid lesions First step Solid lesions Luminal border formation and columnar configuration Exclude: gastrointestinal contamination metastasis (if compatible with other cancer s morphology) Second step Glandular smear pattern Other lymphoma sarcoma non-aca met Solid cellular smear pattern Cell-rich, stroma-poor Exclude: pancreatic contamination (normal or injured acini) Differential diagnosis: chronic pancreatitis PDA (well, moderately, poorly differentiated) metastatic adenocarcinoma Differential diagnosis: PanNET SPN acinar cell carcinoma PBL
14 EUS findings Chronic pancreatitis Autoimmune pancreatitis Solid cellular lesions PDA Visible side branches Cysts Lobularity MPD: irregular dilated with hyperechoic margins Hypoechoic foci and strands +/- stones Diffuse pancreatic swelling: sausage-like with halo effect Mass lesion Hypoechoic mass Homogeneous Well defined (distinct borders, pushing rather than infiltrating) +/- cystic degeneration Hypoechoic mass Irregular borders Double duct sign : dual dilatation of biliary and pancreatic ducts due to a neoplasm of the pancreatic head: pathognomonic for PDA +/- cystic degeneration EUS features are the most important data for the cytopathologist, as they reflect the endoscopist s impression about the lesion
15 Gastrointestinal contamination: epithelial Gastric epithelium Foveolar cells and mucus neck cells: Sheets Seen on surface: of variable size, with a uniform honeycomb pattern Seen on edge: with apical mucinous cups (occupying the upper 1/3 of the cytoplasm) Nuclei: naked nuclei in a mucoid background, slightly elongated, some with nuclear grooves No goblet cells, no lymphocytes, no brush border Chief cells: Abundant blue granules in the cytoplasm Parietal cells: Abundant dense cytoplasm


16
17 Gastrointestinal contamination: epithelial Duodenal epithelium Enterocytes: large folded sheets of evenly spaced glandular cells studded by goblet cells (fried egg appearance) microvillous border sometimes luminal, sometimes brush border consisting of enterocytes with nonmucinous cytoplasm Intraepithelial lymphocytes: Paneth cells: Coarse, eosinophilic granules in their apical cytoplasm

18
 In immediate proximity with non-degenerated benign glandular cells Colloid-type mucin: suggestive of mucin-producing cystic")
19 Gastrointestinal contamination: mucinous Thin or focally thick, never colloid type Cellular or inflammatory debris are not entrapped within the mucin (clear mucin) In immediate proximity with non-degenerated benign glandular cells Colloid-type mucin: suggestive of mucin-producing cystic neoplasm
20 Pancreatic contamination (in the appropriate clinical setting) Acinar epithelium grape-like acinar structures few naked nuclei Ductal epithelium honeycomb sheets of non-mucinous glandular cells orderly polarized picket-fence cells Islet cells generally not recognized

21 Normal acini
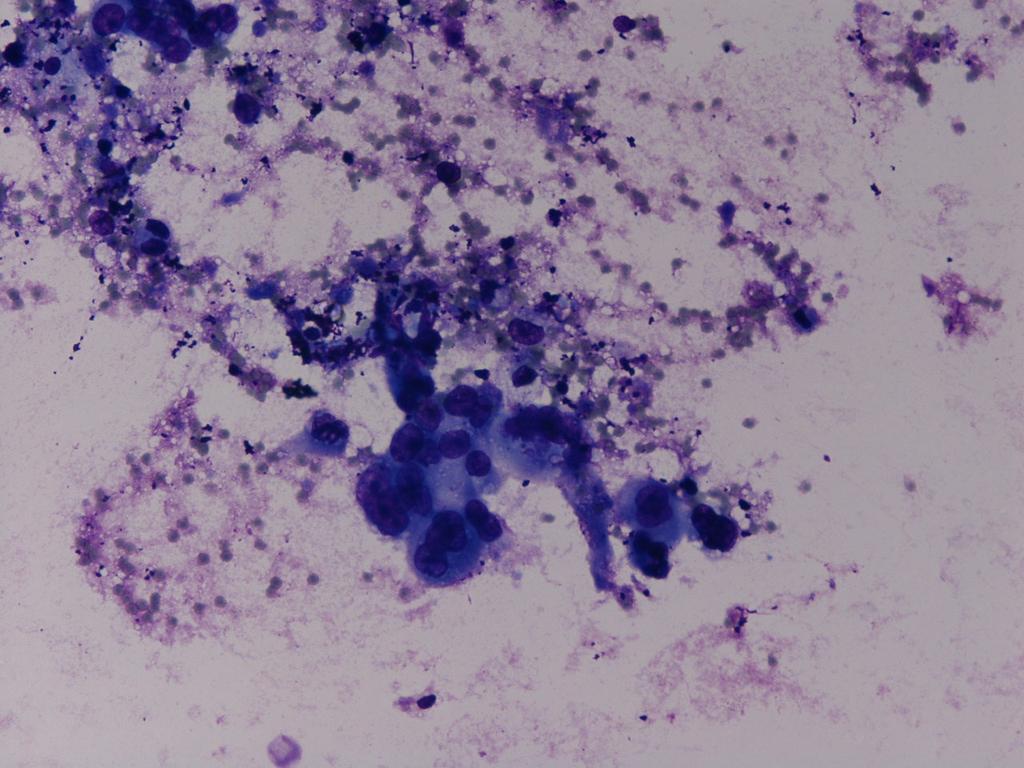
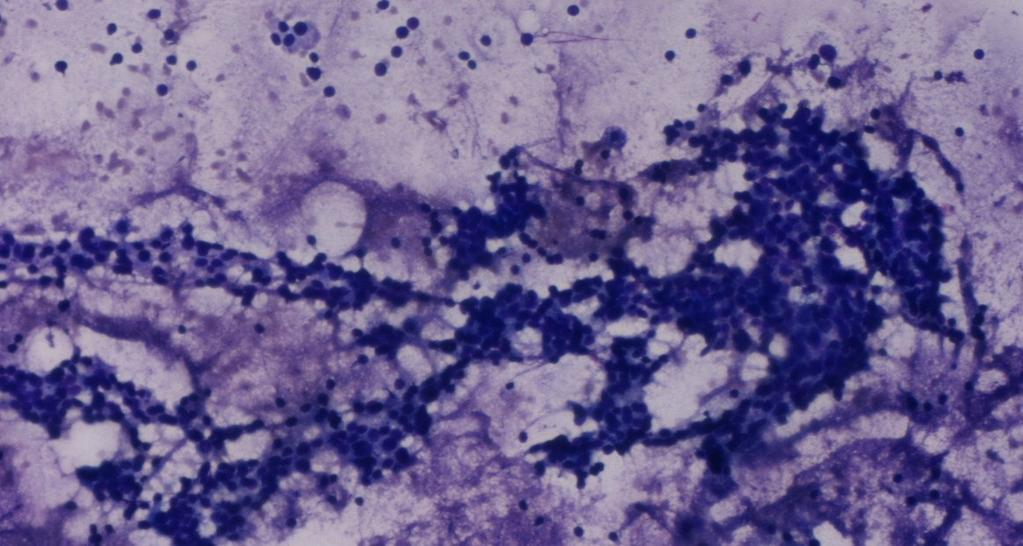
22 Chronic pancreatitis (30%: mass lesion) Mixed population Ductal cells: reactive changes, loss of honeycomb pattern, squamous metaplasia Acinar cells: decrease in late stages Islet cells: single or intact islets Fibrous tissue with spindle cells in interlacing groups Fat but no coagulative necrosis and calcifications Chronic inflammatory cells IgG4-related disease Autoimmune pancreatitis Often not possible diagnosis by cytology alone ROSE: chronic pancreatitis with cellular, fibrous stroma significant atypia of the ductal cells

23 Chronic pancreatitis

24 Chronic pancreatitis

25 Chronic pancreatitis
26 Cellularity Steps in the assessment of PDA Smear pattern (cohesive or loose tissue fragments and dispersed cells) Background (clean or necrotic) Cellular composition (mix of ductal and acinar cells or pure population of ductal cells) Architectural features Nuclear and cytoplasmic features
27 PDA Architectural abnormalities (low power view) Loss of polarity / uneven distribution of cells in the sheet or drunken honeycomb in case of mucinous cytoplasm Crowding / overlapping Cell-in-cell Balls Papillary fragments Nuclear molding Stratification of nuclei when seen on edge More single cells, as dedifferentation occurs +/- tumor diathesis Nuclear abnormalities (high power view) Anisonucleosis (>4:1 nuclear variability in the same cell group) Prominent nucleoli / macronucleoli Chromatin clumping and coarsening Chromatin clearing Nuclear membrane irregularities Nuclear enlargement (>1.5 xrbc) N/C ratio increased +/- Mitoses and karyorrhexis Differential diagnosis between reactive changes in GI epithelium and well-differentiated PDA is based on: nuclear membrane irregularities anisonucleosis 4:1 variation in nuclear size within the same fragment

28 Drunken honeycomb

29 PDA

30 PDA

31 PDA

32 PDA
33 Variants of PDA Colloid carcinoma Undifferentiated carcinoma with osteoclast-like giant cells Undifferentiated/anaplastic carcinoma Adenosquamous carcinoma Medullary carcinoma Hepatoid carcinoma

34 Colloid carcinoma

35 Anaplastic
36 Osteoclastic


37 Adenosquamous carcinoma, squamous component Adenosquamous carcinoma, glandular component
38 ROSE of solid cellular lesions: dd Ar N C PanNET SPN Acinar cell carcinoma PBL (Biphasic and trilineage neoplasm) Small groups Rosettes Clusters Single cells Stripped nuclei Salt & pepper Round nuclei Bland and uniform / endocrine atypia Eccentric Nucleoli inconspicuous (ST: prominent) Branching, papillary-like groups with central fibrovascular core, covered with myxoid stroma, with a third layer of epithelial cells Single cells Naked nuclei Balls of myxoid stroma +/- surrounding thick layer of neoplastic cells (pathognomonic) Round to oval Finely granular chromatin Indentations and grooves Inconspicuous nucleoli Naked nuclei Single cells Cellular fragments Acinar formations Rare syncytia Round to oval Nuclear membrane irregularity (poorly differentiated) Eccentrically placed Single prominent nucleolus Coarsely clumped chromatin Focal anisonucleosis N/C ratio slightly increased Acinar Endocrine Ductal Squamous nests or corpuscles Mesenchymal elements Indistinguishable from acinar cell carcinoma, when squamoid corpuscles and mesenchymal elements are absent, as acinar elements predominate. Cy Scant Dense Variants: clear or oncocytic Basophilic Varying in shape and quantity Perinuclear vacuole Hyaline globules Cytoplasmic tails Mi No No Yes Ne No Yes Rare Granular / vacuolated / dense Often basophilic Bg +/- vascular network Clean or cyst debris Clean or granular
39 Rule of thumb in ROSE ROSE: identification of the solid cellular pattern Definite diagnosis: a matter of immunohistochemistry

40 Acinar cell carcinoma


41 Acinar cell carcinoma

42 Acinar cell carcinoma

43 SPN

44 SPN

45 SPN

46 SPN

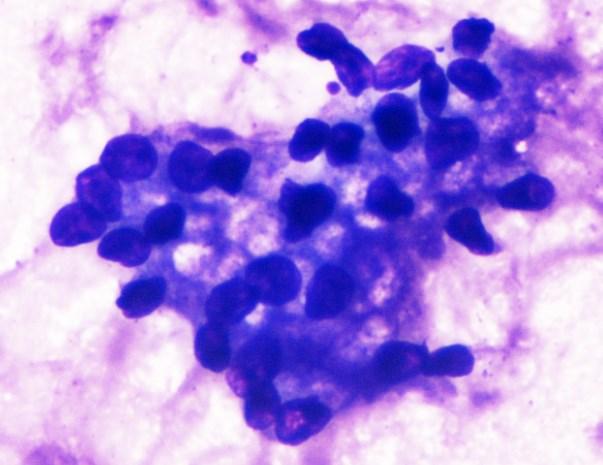
47 Neuroendocrine tumor
48 Neuroendocrine tumor

49 Neuroendocrine tumor
50 Metastatic disease Most common sites of origin in clinical series Lung (23%) Kidney (15%) Breast (8%) Melanoma (5%)


51 Metastasis from colon carcinoma

52 Metastasis from small cell lung carcinoma

53 Metastatic squamous cell carcinoma of the lung

54 Metastatic renal cell carcinoma, clear cell

55 Metastatic urothelial carcinoma

56 Metastatic leiomyosarcoma
57 ROSE is not recommended for cystic lesions However, in our Institution ROSE is performed to identify whether we deal with a mucin-producing neoplasm and the aspirated mucin is lesional or not. Characteristics of lesional mucin: Thick, colloid-type mucin Cellular or inflammatory debris within the mucin, either thick or thin
58 Gold standard Intra-laboratory: concordance between ROSE and final cytologic diagnosis Inter-laboratory: concordance between final cytologic diagnosis and pathology report

59 The battle hymn of the endoscopist Dr. Scott Boerner MD, FRCPC Assoc. Prof., University of Toronto I m in!!! Thank you for your attention!
60 Molecular panel for dd between benign and malignant ductal groups K-ras (expressed also in PanIN grade 1) P53 (loss of expression in adenoca) DPC4 (loss of expression in adenoca in only 55% of all PDAs) Chhieng DC, Stelow EB. Pancreatic Cytopathology Molecular mutations: -activation of oncogenes(k-ras, Her2-neu) -inactivation of tumor suppressor genes (p53, p16, DPC4) PCR identified numerous genes implicated in pancreatic carcinogenesis, such as mesothelin, prostate stem cell antigen, S100P, maspin, IMP3 Promising immunohistochemical panel: pvhl(-), maspin(+), S100P(+), IMP3(+) Distinct pattern of mirnas expression in PDAs, applicable in FNA samples
61 Evaluation of cystic lesions EUS features Location Size Wall thickness Unilocular/ oligolocular /multilocular Single / multiple Communication with the larger pancreatic ducts Margins (sharp/nondescript) Calcifications and their location Presence of mural nodules, papillary projections, thick septa, internal debris Gross features of the fluid Viscosity Colour Volume (quantity) Biochemical assessment CEA and amylase: can be assessed on the neat fluid or the supernatant dilution of saline in case of scant samples 1 ml volume is adequate for both CEA and amylase analyses Molecular assessment +/- molecular mutations (KRAS, GNAS) 0.3 ml of the neat fluid after vortexing is adequate
62 Criteria for presence of mucinous cysts Mucin production Thick, colloid-type mucin Cellular or inflammatory debris within the mucin, either thick or thin or Elevated CEA of the cyst fluid 192 ng/ml: accuracy 80% or KRAS/GNAS mutation and/or Neoplastic epithelial cells present Low grade atypia (low and intermediate grade dysplasia) High grade atypia (at least high grade dysplasia, carcinoma in situ) Mucinous cysts are heterogeneous neoplasms and the cytology sample may not reflect the highest grade of the lesion Low CEA / absence of KRAS or GNAS mutations do not preclude a neoplastic mucinous cyst
63 Genetic mutations in neoplastic mucinous cysts IPMNs KRAS (% of cases) Gastric Intestinal Pancreatobiliary Oncocytic Rare Rare GNAS mutation in codon 201 (% of cases) MCNs Only KRAS mutations The KRAS-GNAS combination cannot predict the grade of dysplasia or invasion Next generation sequencing (NGS) can identify genetic mutations that occurs in high grade dysplasia and invasive carcinoma (TP53, SMAD4, CDKN2A)
64 Targeted therapies in pancreatic adenocarcinoma K-Ras, MAP2K and MEK pathway > MAP2K MEK inhibitors Tyrosine kinase receptor pathway > EGFR, VEGFR, IGFR-1, PDFR inhibitors Molecular targets RET pathway > RET, GDNF inhibitors TP53 tumors suppressor pathway PI3K/Akt pathway > PI3K, Akt inhibitors Stromal compartment > Sonic hedgehog (SHH) pathway inhibitors, Hyaluronidase inhibitors, Matrix Metalloproteinases inhibitors mtor signaling pathway > mtor inhibitors JAK/STAT signaling pathway > JAK1/2, STAT3 inhibitors Cancer stem cells (Notch, Wnt and SHH pathways) > Notch 2/3 inhibitors Autophagy Poly (ADP-ribose)polymerase pathway > PARP inhibitors Mosquera C et al. Molecular targeted therapy for pancreatic adenocarcinoma: A review of completed and ongoing late phase clinical trials. Cancer Genet Aug 2. pii: S (16)30223-X. Chadha AS et al. Recent Advances and Prospects for Multimodality Therapy in Pancreatic Cancer. Semin Radiat Oncol Oct;26(4):
 Greater one year survival (23% vs 17%), p = 0.")
65 EGFR pathway inhibition Erlotinib / Tarceva FDA approval in advanced stage disease Phase III trial conducted by National Cancer Institute of Canada showed: Improved overall survival (OS) (HR 0.82; 95% CI ; p = 0.038) Greater one year survival (23% vs 17%), p = in the erlotinib plus gemcitabine group vs gemcitabine only group Phase II trial by ESMO (Pantar Study) also showed survival improvement Currently, this is the only FDA approved targeted therapeutic option for PDA Karandish F and Mallik S. Biomarkers and Targeted Therapy in Pancreatic Cancer. Biomark Cancer Apr 26;8(Suppl 1): Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the national cancer institute of canada clinical trials group. J Clin Oncol 2007;25:
66 Future perspectives Radiotherapy + targeted therapies Immunotherapy (checkpoint inhibitors, cancer vaccines, adoptive T-cell transfer) + targeted therapies Biomarkers of response (such as serum biomarkers, surface markers of cancer cells, mirnas) Gene therapy Nanotechnology Personalized cancer treatment Not all people are the same Not all tumors are the same
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Video Microscopy Tutorial 19
 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT
 CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Standardization of Nomenclature
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Biliary Tract Neoplasia: A Cyto-histologic Review. Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital
 Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital
 Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Conflicts of Interest
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
LGM International, Inc.
 Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Pancreatobiliary Frozen Section Nightmares
 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Pancreatic Cancer: The ABCs of the AJCC and WHO
 Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
EUS-guided FNAB. Differential Diagnosis 5/1/2017. EUS-FNA of Solid and Cystic Lesions:
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION CYTOPATHOLOGY Monday, April 26, 2013 FACULTY COPY
 GOAL: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION CYTOPATHOLOGY Monday, April 26, 2013 FACULTY COPY 1. Understated the role of cytopathology in the clinical management of the patient and recognize
GOAL: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION CYTOPATHOLOGY Monday, April 26, 2013 FACULTY COPY 1. Understated the role of cytopathology in the clinical management of the patient and recognize
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo. Case Discussions. 60 year old woman Routine gynecologic control LBC
 BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
Objectives. Pancreatic Cysts. Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses
 Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Abid Irshad, MD Director Breast Imaging. Medical University of South Carolina Charleston
 Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Almost any suspected tumor can be aspirated easily and safely. Some masses are more risky to aspirate including:
 DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
INTRODUCTION TO PATHOLOGICAL TECHNIQUES. 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH)
") INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
ROSE in EUS guided FNA of Pancreatic Lesions
 ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
Introduction. 23 rd Annual Seminar in Pathology. FLUIDS, Part 1. Pittsburgh, PA Gladwyn Leiman UVMMC, VT
 23 rd Annual Seminar in Pathology Pittsburgh, PA Gladwyn Leiman UVMMC, VT FLUIDS, Part 1 "Blue walls", Claudia Hansen, 2009 Introduction o Challenging to everyone o Almost any benign or malignant process
23 rd Annual Seminar in Pathology Pittsburgh, PA Gladwyn Leiman UVMMC, VT FLUIDS, Part 1 "Blue walls", Claudia Hansen, 2009 Introduction o Challenging to everyone o Almost any benign or malignant process
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Pancreatic Cysts. Darius C. Desai, MD FACS St. Luke s University Health Network
 Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Diagnostic Cytology of Cancer Cases
 Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS
 ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY. F ZAHRA ALY, MD, PhD
 ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Pancreatic malignant tumors are the fifth leading cause of cancerrelated
 44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
EUS-guided FNAB. Differential Diagnosis 3/14/2018. EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Pancreas. Atrophy, acinar cell. Pathogenesis: Diagnostic key features:
 Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
Normal Morphology. Anatomic Considerations. Normal Urothelial Histology and Cytology
 1 Normal Morphology Anatomic Considerations The urinary tract can be divided into three regions: the kidney; the calyces, pelves and ureters (upper collecting system or upper tract); and the bladder and
1 Normal Morphology Anatomic Considerations The urinary tract can be divided into three regions: the kidney; the calyces, pelves and ureters (upper collecting system or upper tract); and the bladder and
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS
 Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
of Thyroid Lesions Comet Tail Crystals
 2 Ultrasound Features of Thyroid Lesions There are many different features indicating a certain benign or malignant tumor type, but many of these are overlapping signs. Combining several features is considered
2 Ultrasound Features of Thyroid Lesions There are many different features indicating a certain benign or malignant tumor type, but many of these are overlapping signs. Combining several features is considered
XIII CONGRESSO NAZIONALE Roma, 7-9 novembre NODULO TIROIDEO: Agoaspirato o Core Needle Biopsy?
 XIII CONGRESSO NAZIONALE NODULO TIROIDEO: Agoaspirato o Core Needle Biopsy? Anna Crescenzi Policlinico Universitario Campus Bio-Medico Roma Indeterminate lesions are heterogeneous The gray zone CONSERVATIVE
XIII CONGRESSO NAZIONALE NODULO TIROIDEO: Agoaspirato o Core Needle Biopsy? Anna Crescenzi Policlinico Universitario Campus Bio-Medico Roma Indeterminate lesions are heterogeneous The gray zone CONSERVATIVE
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
NEOPLASIA-I CANCER. Nam Deuk Kim, Ph.D.
 NEOPLASIA-I CANCER Nam Deuk Kim, Ph.D. 1 2 Tumor in the hieroglyphics of the Edwin Smith papyrus (1,600 B.C., Breasted s translation 1930) 3 War on Cancer (National Cancer Act, 1971) 4 Cancer Acts in Korea
NEOPLASIA-I CANCER Nam Deuk Kim, Ph.D. 1 2 Tumor in the hieroglyphics of the Edwin Smith papyrus (1,600 B.C., Breasted s translation 1930) 3 War on Cancer (National Cancer Act, 1971) 4 Cancer Acts in Korea
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas
 Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview