The FRCPath Exam. How to pass the short surgicals on the first go By someone who didn t. Plus some tips on frozen sections!
|
|
|
- Sharleen Cross
- 5 years ago
- Views:
Transcription
1 The FRCPath Exam How to pass the short surgicals on the first go By someone who didn t Plus some tips on frozen sections! Dr Paul Bennett
2 Overview Reminder of the exam format How to format your answer for the short surgicals Discussion of cases Brief discussion of frozen sections Mandatory viewing of holiday photos throughout talk
3 Exam Overview Short Surgicals 20 cases Given in pairs, 20 minutes per pair When they re gone, they re gone Can be anything Long Cases 4 cases, 20 minutes per case Special stains / immuno / FISH / EM
4 Exam Overview Frozens 6 cases, 20 minutes per three cases Scribble notes in the answer book Viva at the end OSPEs Two stations, one manned A) Management issue B) Data set and short answers
5 Exam Overview Non-gynae cytology - 8 cases, 20 minutes per pair - Often benign vs. malignant cases - Macros - 4 cases, each with a photograph - Draw blocks on photograph - Answer short questions in Viva
6 Exam Overview Archaic marking system Scored out of 5 1 or 1.5 = fail 2 = bare fail 2.5 = pass 3 = good answer 3.5 = excellent answer 4+ =? Possible Overall pass mark 50%
7 Why focus on the short surgicals? Obviously, each component of the exam requires preparation However, surgicals often cause problems Largest single component of exam Large variety of cases Lots of writing A well-practised approach works

8
9 Approaching the Questions Use a tried and tested format that you are familiar with Answer every question the same way I ed my preferred format to you a 6 point approach (credit to Dr D Scott) This format will allow you to maximise marks for each question
10 Approaching the Questions 1. Description 2. Interpretation 3. Differential diagnosis 4. Extra investigations 5. Clinico-pathological correlation 6. Bottom line diagnosis
11 Approach to a Case Description Keep it brief Include description of type of lesion (eg neoplasm, inflammatory process) Brief description of architecture and morphology if it s a lesion Mention dataset items if a tumour (margin involvement, necrosis, vascular invasion, etc) Don t forget to grade any neoplasms May be appropriate to comment on the background tissue briefly
12 Approach to a Case Interpretation Should immediately follow description and summarise your thoughts on the H+E slide State diagnosis if you re sure This is a malignant melanoma - If you re not sure, go as far as you can This is a malignant epithelioid neoplasm If you re really struggling This is an epithelioid neoplasm
13 Approach to a Case Differential Diagnosis One or two questions may require a differential Will be unnecessary in most questions For example, a malignant epithelioid neoplasm: Carcinoma Melanoma Large cell lymphoma Mesothelioma
14 Approach to a Case Extra investigations (if appropriate) - Start from the bottom - Levels (usually unnecessary but demonstrates safety if uncertain) - Special stains - Immunocytochemistry - IMF - Useful to incorporate immunostains into differential diagnosis - Cytogenetics - EM
15 Approach to a Case If the diagnosis is already established on morphology, mentioning extra investigations still adds extra value to your answer, eg: - Signet ring carcinoma: PAS +ve inclusions - Glomus tumour: SMA +ve - Pemphigus vulgaris: Reticular IgG/C3 on IMF - Well differentiated liposarcoma: MDM-2/CDK4 amplification on cytogenetics - Langerhan s cell histiocytosis: Birbeck granules on EM
16 Approach to a Case Clinicopathological correlation Chance to earn extra credit All malignant cases to relevant MDT Classical histories COCP use in liver adenoma Epithelioid sarcoma peripheral sites, young patients Mention any classical symptoms Painful ANGEL skin lesions Typical imaging features DCIS: Calcification on plain X-Ray
17 Approach to a Case Clinico-pathological correlation (continued) Treatment Melanomas wider excisions +/- sentinel nodes Adenocarcinoma of lung EGFR inhibitors GISTs Tyrosine kinase inhibitors Prognosis Good Nodular lymphocyte predominant Hodgkin s Poor Anaplastic large T cell lymphoma Stage If you can remember! Mention it regardless
18 Approach to a Case Bottom line diagnosis One line only This may be the first bit of your answer the examiner looks at. If it s right, you re off to a good start and the examiner can look for extra marks in the rest of your answer
19 Case 1 29M, testicular mass

20

21
22 Case 1 Description Nested tumour separated by broad, lymphocyte-rich fibrous bands. The tumour cells show large nuclei, prominent nucleoli and delicate cytoplasm. There is focal rete testis involvement There is no evidence of vascular invasion or intratubular germ cell neoplasia
23 Case 1 Interpretation This is a classical seminoma This is a malignant germ cell tumour This is a malignant epithelioid neoplasm The further down the list, the less likely you are to pick up any marks
24 Case 1 Differential Shouldn t really need one H+E spot diagnosis Some other germ cell tumours (spermatocytic seminoma) lymphoma and melanoma are perhaps reasonable to suggest if you don t know Either way.. To the immuno!
25 Case 1 Extra investigations Not necessary if you ve got the diagnosis on H+E BUT, you can still mention classic staining pattern for possible extra points: Classical seminoma: C-Kit, PLAP, Oct 3/4 positive If working on differentials: Spermatocytic Seminoma: C-kit & OCT 3/4 +ve; PLAP -ve Lymphoma: CD45 +ve; germ cell markers -ve Melanoma: Melan-A & S100 +ve; germ cell markers ve
26 Case 1 Clinico-pathological correlation Needs staging and discussion at MDT Commoner in young men Associated with history of undescended testes Treatment orchidectomy Chemo if recurrent or advanced disease Good prognosis in many cases pt1 on this slide
27 Case 1 Testicular mass - Classical seminoma
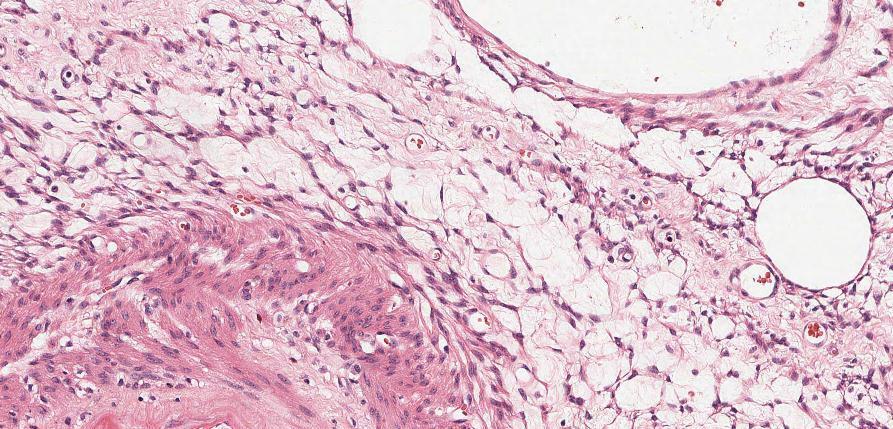
28 Case 2 67F, retroperitoneal mass
29
30 Case 2 Description Diffuse tumour composed of admixture of fat, blood vessels and smooth muscle. The smooth muscle component emanates from the vessel walls No obvious renal tissue in sections No evidence of atypia, necrosis or increased mitotic activity
31 Case 2 Interpretation This is an angiomyolipoma (PEComa) This is a mesenchymal tumour of uncertain malignant potential This is a neoplasm
32 Case 2 Differential Very few no real features of any other tumours expected at this site (RCC, adrenal tumours, well-diff liposarcomas) Fat predominant or muscle predominant variants occur in these cases a differential is reasonable I wouldn t include a differential in this case it s classical
33 Case 2 Extra investigations Positive immunoreactivity for HMB-45 + Melan-A
34 Case 2 Clinico-pathological correlation Discuss at sarcoma MDT Variable malignant potential Excision usually curative, though necrosis, increased mitoses and atypia increase risk of metastasis Many (up to a third) associated with tuberous sclerosis May co-exist with other PEComas Clear cell tumours of the lung Lymphangiomyomatosis
35 Case 2 Retroperitoneal mass - Angiomyolipoma
36 Case 3 38M, lesion on arm

37

38
39 Case 3 Description This is skin with a normal epidermis. The dermis contains a symmetrical proliferation of pigmented, spindled melanocytes. There is no evidence of atypia or mitotic activity. There is no evidence of a junctional component This lesion appears completely excised
40 Case 3 Interpretation This is a blue naevus This is a benign melanocytic proliferation This is a melanocytic proliferation
41 Case 3 Differential Again, only necessary if you re not sure Malignant melanoma (primary / metastatic) If going down this line explain how you d sort it out Check history Levels for junctional component / regression Pigmented DFSP Sort out on immuno if you re worried about this
42 Case 3 Extra investigations Pigment is Masson-Fontana positive, Perl s negative Lesion is S100, HMB45, Melan-A positive SMA and CD34 negative
43 Case 3 Clinico-pathological correlation Benign lesions Small and blue macroscopically Excision curative BRAF / RAS mutations absent
44 Case 3 Skin, arm - Blue naevus
45 Case 4 52F, lesions on lower legs

46

47
48 Case 4 Description This is a punch biopsy of skin and subcutaneous fat. The fat shows septal inflammation composed of histiocytes, lymphocytes and plasma cells. There is no evidence of vasculitis, necrosis or neoplasia. The overlying skin shows mild venous stasisrelated features only
49 Case 4 Interpretation This is erythema nodosum This is a septal panniculitis This is panniculitis This is an inflammatory process
50 Case 4 Differential Only if you re not sure Lobular panniculitis Secondary to pancreatitis Could suggest serum amylase
51 Case 4 Extra investigations Fungal / ZN stains reasonable as granulomatous inflammation
52 Case 4 Clinico-pathological correlation F>M Lots of causes Drugs (COCP) check history Infections (TB, Strep) Malignancies (usu. haematological) Crohn s Sarcoid recent chest X-Ray? EN is often reactive and self-limiting
53 Case 4 Skin, lower leg Erythema Nodosum
54 Case 5 M16, multiple skin lesions excision of one from arm

55

56
57 Case 5 Description This is skin with a normal epidermis. The dermis contains a well-circumscribed proliferation of spindle cells with bland buckled nuclei and admixed mast cells. There are no features of atypia, mitotic activity or necrosis This lesion is incompletely excised at the deep margin
58 Case 5 Interpretation This is a neurofibroma This is a benign neural lesion This is a benign mesenchymal / spindle cell tumour This is a benign neoplasm
59 Case 5 Differential diagnosis If not sure: Dermatofibroma not an unreasonable suggestion, but unlikely to do you much good in a simple case like this
60 Case 5 Extra investigations Not necessary in reality, but could state that neurofibromas are S100 positive (patchy)
61 Case 5 Clinico-pathological correlation History of multiple lesions! NF-1 must be considered Café au lait spots, Lisch nodules Increased risk of MPNST Be firm that this case is benign (no mitoses etc) Otherwise excision is curative
62 Case 5 Skin, arm - Neurofibroma
63 Case 6 M66, testicular mass

64

65
66 Case 6 Description This is a tumour composed of nests and sheets of cells with round nuclei, prominent nucleoli and delicate cytoplasm. There is no evidence of a prominent lymphocytic component. The tumour appears confined to the testis and vascular invasion is not seen. There is no evidence of IGCN.
67 Case 6 Interpretation This is a spermatocytic seminoma This is a malignant germ cell tumour This is a malignant epithelioid neoplasm
68 Case 6 Differential diagnosis Main one is classical seminoma Spermatocytic seminomas lack lymphocyte-rich fibrous bands and usually affect older men They are also not associated with IGCN Can sort out on immuno if unsure
69 Case 6 Extra investigations Immuno Spermatocytic seminoma C-KIT & OCT 3/4 +ve PLAP ve Classical seminoma C-KIT, OCT 3/4, PLAP +ve
70 Case 6 Clinico-pathological correlation Older men Excellent prognosis Excision curative Stage and discuss at Urological MDT
71 Case 6 Testicular mass Spermatocytic seminoma
72 Case 7 M18, diarrhoea, colorectal biopsies

73
74 Case 7 Description Biopsies of large intestinal mucosa showing mild crypt distortion, non-caeseating granulomas within the lamina propria and a mild increase in lamina propria cellularity No evidence of active inflammation, ulceration, dysplasia or malignancy
75 Case 7 Interpretation This is a granulomatous colitis
76 Case 7 Differential diagnosis Necessary in this case Crohn s disease Mycobacterial infection Fungal infection Sarcoidosis Reaction to tumour
77 Case 7 Extra investigations ZN / fungal stains Mycobacterial PCR
78 Case 7 Clinico-pathological correlation Needs examination of targeted colorectal and ileal biopsies to investigate IBD Crohn s disease associated with skip lesions, fissuring
79 Case 7 Colorectal biopsies Granulomatous colitis
80 Case 8 F42, lesion on arm

81

82
83 Case 8 Description This is a well-circumscribed, vascular, dermal lesion composed of small basaloid cells admixed with larger pale epithelial cells and lymphocytes. There is no epidermal connection. There are no features of malignancy. This lesion appears excised in the plane of section examined
84 Case 8 Interpretation This is an eccrine spiradenoma This is a benign eccrine tumour This is a benign adnexal tumour This is a benign tumour
85 Case 8 Differential diagnosis Reasonable to include some other adnexal tumours if you re not sure Cylindroma Acrospiroma (Dermal duct tumour)
86 Case 8 Extra investigations No relevant that I can think of
87 Case 8 Clinico-pathological correlation Usually solitary lesions Classically painful (ANGEL) Malignant transformation rare Excision curative Multiple tumours associated with Brooke- Spiegler syndrome
88 Case 8 Lesion on arm Eccrine spiradenoma
89 Case 9 M38, nausea and vomiting, gastric biopsies

90
91 Case 9 Description These are biopsies of fundic-type gastric mucosa showing diffuse infiltration of the lamina propria by malignant tumour cells The cells show displaced nuclei and occasional cytoplasmic vacuolation ( signetring morphology) No vascular invasion identified No evidence of background dysplasia
92 Case 9 Interpretation This is poorly-differentiated (signet-ring) adenocarcinoma This is a malignant epithelioid neoplasm
93 Case 9 Differential diagnosis Poorly differentiated adenocarcinoma Lymphoma Melanoma
94 Case 9 Extra investigations PAS stain - +ve in vacuoles Immuno Cytokeratin (CK 7) and CEA positive CK20, CD45, S100 and Melan-A negative
95 Case 9 Clinico-pathological correlation Requires MDT correlation Classical linitis plastica picture at endoscopy May be resectable depending on extent of spread Overall poor prognosis New evidence of role of Trastuzumab in Her-2 positive gastric cancer
96 Case 9 Gastric biopsies Poorly differentiated (signet ring) adenocarcinoma
97 Case 10 F28, haematuria and pelvic pain, bladder biopsies

98
99 Case 10 Description Bundles of smooth muscle infiltrated by endometrial glands and stroma Foci of extravasated red blood cells and pigment-laden macrophages No evidence of atypia or necrosis No in-situ disease
100 Case 10 Interpretation This is endometriosis
101 Case 10 Differential diagnosis No others of note
102 Case 10 Extra investigations Not necessary, but can state that endometrial foci would be CD10 and ER positive
103 Case 10 Clinico-pathological correlation Endometriosis often multifocal (cervix, Pouch of Douglas, ovaries) Increased risk of infertility Treatment involves hormones (COCP, coil) or surgical Usually disappears post-menopause
104 Case 10 Bladder biopsies - Endometriosis
105 Case 11 F61, hysterectomy. Lesion in anterior myometrium

106

107
108 Case 11 Description Well-circumscribed cellular lesion composed of spindle cells with cigar-shaped nuclei Minimal nuclear atypia, no increase in mitotic activity and no necrosis Smooth, regular interface with surrounding tissue
109 Case 11 Interpretation This is a cellular leiomyoma This is a leiomyoma This is a benign smooth muscle tumour This is a smooth muscle tumour
110 Case 11 Differential diagnosis Cellular leiomyoma Leiomyosarcoma STUMP
111 Case 11 Extra investigations Correlate with macroscopic appearance Needs extensive sampling, particularly around the edges of the lesion Search for areas of increased mitotic activity, necrosis, infiltrative border Can confirm smooth muscle origin with SMA, desmin, H-caldesmon Ki67 may be useful
112 Case 11 Clinico-pathological correlation Correlate with imaging any suspicious ultrasound features? Cellular leiomyomas are benign Excision curative
113 Case 11 Uterus Cellular leiomyoma
114 Case 12 F30, rash on arms. IgA positive on immunofluorescence studies

115

116
117 Case 12 Description Skin with subepidermal clefting and effacement of the dermal papillae Blister filled with blood, proteinaceous fluid, inflammatory cells Fibrin on base of blister No evidence of neoplasia
118 Case 12 Interpretation This is an inflammatory blistering process
119 Case 12 Differential diagnosis Dermatitis herpetiformis Linear IgA disease Bullous SLE Bullous pemphigoid / EBA These are NOT supported by the IMF Only possible DDs if IMF not present
120 Case 12 Extra investigations IMF main one, already provided Usually patchy and granular along BM in DH Deposits may also be seen in the dermis (in DH)
121 Case 12 Clinico-pathological correlation Essential in this case Discuss history with clinicians? Coeliac disease (Dermatitis Herpetiformis)? Medication history (Linear IgA disease)? Previous history of SLE or autoimmune disease
122 Case 12 Skin, arm Favour dermatitis herpetiformis, see text
123 Summary Short Surgicals Stick to a standard format Practise it, over and over again, on any case Work on degree of certainty If you re prepared, you ll be certain on around 75% of the questions If uncertain take a step back, and keep to the structured answer All this of course depends on good background microscopy skills
124 Frozen Sections
125 Key tips Don t panic The frozen sections are often very straightforward You have plenty of time Your first impression is usually the right one The Viva is usually quick and straightforward You can probably only get away with deferring to paraffin once Show initiative if unsure, ask BMS to cut extra levels, show colleague
126 Common Cases Peritoneal nodules Metastatic tumour Ovarian GI Endometriosis Ureteric resection margins CIS vs normal
127 Common Cases Granulomatous inflammation Differentials Clean the cryostat Resection margins Skin Bone Pancreas Liver nodules Met Ca Von Meyenburg complex
128 Common Cases Lymph nodes Benign / reactive Don t diagnose lymphoma Beware the non-diagnosable cases Spindle cell lesions
129 Finally. Prepare well Reading and slide exposure Practise over and over again Have a few days off before the exam Get a comfortable hotel Take chocolate and water into the exam Not crisps Don t dwell on things, at least until both days are over Go on holiday immediately afterwards
130 THANKS FOR LISTENING Please give feedback
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
SMOOTH MUSCLE TUMOURS
 SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency
 Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
Updates in Urologic Pathology WHO Made Those Changes?! Peyman Tavassoli Pathology Department BC Cancer Agency World Health Organization Available in Feb 2016 Frame work for reporting Major contributing
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
FRCPath Part 2 in Histopathology Spring 2012 Surgical Pathology. Answers
 FRCPath Part 2 in Histopathology Spring 2012 Surgical Pathology Answers One route to examination success is to read the question and then attempt to answer it. The question is: You should provide a written
FRCPath Part 2 in Histopathology Spring 2012 Surgical Pathology Answers One route to examination success is to read the question and then attempt to answer it. The question is: You should provide a written
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Endometrial Stromal Tumors
 Endometrial Stromal Tumors WHO Categories: Endometrial Stromal Nodule (ESN) Endometrial Stromal Sarcoma, low grade (LGESS) Endometrial Stromal Sarcoma, high grade (HGESS) Undifferentiated Uterine Sarcoma
Endometrial Stromal Tumors WHO Categories: Endometrial Stromal Nodule (ESN) Endometrial Stromal Sarcoma, low grade (LGESS) Endometrial Stromal Sarcoma, high grade (HGESS) Undifferentiated Uterine Sarcoma
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Diagnostic problems in uterine smooth muscle tumors
 Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Bladder Case 1 SURGICAL PATHOLOGY REPORT. Procedure: Cystoscopy, transurethral resection of bladder tumor (TURBT)
") Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
INTRODUCTION TO PATHOLOGICAL TECHNIQUES. 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH)
") INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
Circulation: X Case number: 501 Number of responses: 84 Date: 4 MAY 12
 Circulation: X Case number: 500 Number of responses: 81 Date: 4 MAY 12 Female, aged 65 TAH and BSO for G1 endometrioid adenocarcinoma. Tumour positive with inhibin, vimentin, CD56 and SMA. Negative with
Circulation: X Case number: 500 Number of responses: 81 Date: 4 MAY 12 Female, aged 65 TAH and BSO for G1 endometrioid adenocarcinoma. Tumour positive with inhibin, vimentin, CD56 and SMA. Negative with
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
What really matters When and Why. Pathology of Uterine Mesenchymal Lesions. Nafisa Wilkinson London
 What really matters When and Why Pathology of Uterine Mesenchymal Lesions Nafisa Wilkinson London Patient centred approach immunohistochemistry Histological diagnosis Next generation sequencing Genetic
What really matters When and Why Pathology of Uterine Mesenchymal Lesions Nafisa Wilkinson London Patient centred approach immunohistochemistry Histological diagnosis Next generation sequencing Genetic
Classification (1) Classification (3) Classification (2) Spindle cell lesions. Spindle cell lesions of bladder (Mills et al.
 Classification (3) Classification (2) Spindle cell lesions. Spindle cell lesions of bladder (Mills et al.") Non-epithelial tumours and nonepithelial tumour-like lesions of the bladder Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Classification (1) Myofibroblastic proliferations and
Non-epithelial tumours and nonepithelial tumour-like lesions of the bladder Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Classification (1) Myofibroblastic proliferations and
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on
 Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
Review of the AP Part II Practical Examination. Dr David Clift Co Chief Examiner
 Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Diploma Examination. Dermatopathology: First paper. Tuesday 20 March Candidates must answer FOUR questions. Time allowed: 3 hours
 Dermatopathology: First paper Tuesday 20 March 2018 Candidates must answer FOUR questions Time allowed: 3 hours 1. Give an account of the genetic aberrations encountered in Spitzoid neoplasms and how these
Dermatopathology: First paper Tuesday 20 March 2018 Candidates must answer FOUR questions Time allowed: 3 hours 1. Give an account of the genetic aberrations encountered in Spitzoid neoplasms and how these
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
Case E1. Female aged 63 years Right Nephrectomy Two separate tumours Section of each tumour
 Case E1 Female aged 63 years Right Nephrectomy Two separate tumours Section of each tumour Tumour 1 Upper pole tumour 28mm macro diameter Circumscribed Friable cut surface Tumour 2 Middle pole Part solid
Case E1 Female aged 63 years Right Nephrectomy Two separate tumours Section of each tumour Tumour 1 Upper pole tumour 28mm macro diameter Circumscribed Friable cut surface Tumour 2 Middle pole Part solid
Uropathology January Jon Oxley
 Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Five Most Common Problems in Surgical Neuropathology
 Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Tinh hoàn
 Tinh hoàn Tinh hoàn Tinh hoàn Tiền liệt tuyến Tiền liệt tuyến Mào tinh hoàn Mào tinh hoàn Túi tinh Túi tinh Túi tinh Túi tinh So-called cystadenoma of seminal vesicle. Gross appearance of granulomatous
Tinh hoàn Tinh hoàn Tinh hoàn Tiền liệt tuyến Tiền liệt tuyến Mào tinh hoàn Mào tinh hoàn Túi tinh Túi tinh Túi tinh Túi tinh So-called cystadenoma of seminal vesicle. Gross appearance of granulomatous
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
SEBACEOUS NEOPLASMS. Dr. Prachi Saraogi Clinical Fellow in Dermatology
 SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain
 December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Mesenchymal neoplasms of the gastrointestinal tract what s new? Newton ACS Wong Department of Histopathology Bristol Royal Infirmary
 Mesenchymal neoplasms of the gastrointestinal tract what s new? Newton ACS Wong Department of Histopathology Bristol Royal Infirmary Talk plan Summary from 2010 talk. What s happened since 2010. GISTs
Mesenchymal neoplasms of the gastrointestinal tract what s new? Newton ACS Wong Department of Histopathology Bristol Royal Infirmary Talk plan Summary from 2010 talk. What s happened since 2010. GISTs
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
An Overview of Genital Stromal Tumors
 An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Male Genital Cancers in the US in Frequency of Types
 Germ Cell Tumors of the Testis Pathology, Immunohistochemistry, and the Often Confusing Appearance of Their Metastases Charles Zaloudek, MD Department of Pathology UCSF Male Genital Cancers in the US in
Germ Cell Tumors of the Testis Pathology, Immunohistochemistry, and the Often Confusing Appearance of Their Metastases Charles Zaloudek, MD Department of Pathology UCSF Male Genital Cancers in the US in
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
This is the second learning component (Learning Component 2) in our first learning module (Learning Module 1). In this component we review a very
 in our first learning module (Learning Module 1). In this component we review a very") This is the second learning component (Learning Component 2) in our first learning module (Learning Module 1). In this component we review a very basic response to injury inflammation. We ll look at examples
This is the second learning component (Learning Component 2) in our first learning module (Learning Module 1). In this component we review a very basic response to injury inflammation. We ll look at examples
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Circulation: V Case number: 301 Number of responses: 83 Date: 3 MAY 11
 Circulation: V Case number: 300 Number of responses: 73 Date: 3 MAY 11 Male, 58 years Right Renal Cell Carcinoma. Negative for Vimentin and Hales' Colloidal Iron Right Nephrectomry Right nephrectomy 432.0g
Circulation: V Case number: 300 Number of responses: 73 Date: 3 MAY 11 Male, 58 years Right Renal Cell Carcinoma. Negative for Vimentin and Hales' Colloidal Iron Right Nephrectomry Right nephrectomy 432.0g
Myxo-inflammatory Fibroblastic sarcoma
 AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Almost any suspected tumor can be aspirated easily and safely. Some masses are more risky to aspirate including:
 DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
Tumour Markers. For these reasons, only a handful of tumour markers are commonly used by most doctors.
 Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Differential diagnosis of HCC
 Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig
 Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is:
 Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
TUMOR,NEOPLASM. Pathology Department, Zhejiang University School of Medicine,
 TUMOR,NEOPLASM Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn The points in this chapter What is a neoplasm (conception) Morphology of neoplasm Macroscopy of Neoplasm
TUMOR,NEOPLASM Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn The points in this chapter What is a neoplasm (conception) Morphology of neoplasm Macroscopy of Neoplasm
Diploma examination. Dermatopathology: First paper. Tuesday 21 March Candidates must answer FOUR questions ONLY. Time allowed: Three hours
 Dermatopathology: First paper Tuesday 21 March 2017 1. Discuss the role of fluorescent in-situ hybridization (FISH) and emerging molecular techniques in the diagnosis of cutaneous melanocytic lesions,
Dermatopathology: First paper Tuesday 21 March 2017 1. Discuss the role of fluorescent in-situ hybridization (FISH) and emerging molecular techniques in the diagnosis of cutaneous melanocytic lesions,
CASE year old male with a PET avid nodule in the left adrenal gland
 CASE 1 55 year old male with a PET avid nodule in the left adrenal gland Case 1 Adrenal gland parenchyma partly replaced by a spindle cell tumour with mild nuclear pleomorphism Atypical mitoses present
CASE 1 55 year old male with a PET avid nodule in the left adrenal gland Case 1 Adrenal gland parenchyma partly replaced by a spindle cell tumour with mild nuclear pleomorphism Atypical mitoses present
Journal of International Academy of Forensic Science & Pathology (JIAFP)
") Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Gross appearance of peritoneal cysts. They have a thin, translucent wall and contain a clear fluid.
 Gross appearance of peritoneal cysts. They have a thin, translucent wall and contain a clear fluid. So-called multicystic benign mesothelioma. A, Gross appearance. So-called multicystic benign mesothelioma.
Gross appearance of peritoneal cysts. They have a thin, translucent wall and contain a clear fluid. So-called multicystic benign mesothelioma. A, Gross appearance. So-called multicystic benign mesothelioma.
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Solitary Fibrous Tumor of the Kidney with Massive Retroperitoneal Recurrence. A Case Presentation
 246) Prague Medical Report / Vol. 113 (2012) No. 3, p. 246 250 Solitary Fibrous Tumor of the Kidney with Massive Retroperitoneal Recurrence. A Case Presentation Sfoungaristos S., Papatheodorou M., Kavouras
246) Prague Medical Report / Vol. 113 (2012) No. 3, p. 246 250 Solitary Fibrous Tumor of the Kidney with Massive Retroperitoneal Recurrence. A Case Presentation Sfoungaristos S., Papatheodorou M., Kavouras
List of Available TMAs in the PRN
 TMA RPCI_BrainCa01 RPCI_BrCa03 RPCI_BrCa04 RPCI_BrCa05 RPCI_BrCa0 RPCI_BrCa07 RPCI_BrCa08 RPCI_BrCa15 RPCI_BrCa1 RPCI_BrCa17 RPCI_BrCa18 RPCI_BrCa19 RPCI_BrCa20 RPCI_BrCa21 RPCI_BrCa24 RPCI_BrCa25 RPCI_BrCa2
TMA RPCI_BrainCa01 RPCI_BrCa03 RPCI_BrCa04 RPCI_BrCa05 RPCI_BrCa0 RPCI_BrCa07 RPCI_BrCa08 RPCI_BrCa15 RPCI_BrCa1 RPCI_BrCa17 RPCI_BrCa18 RPCI_BrCa19 RPCI_BrCa20 RPCI_BrCa21 RPCI_BrCa24 RPCI_BrCa25 RPCI_BrCa2
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Cutaneous Adnexal Tumors
 Cutaneous Adnexal Tumors Lesions with Predominant Follicular Differentiation Special Emphasis on Basal Cell Carcinoma 2014-04-01 Prof. Dr. med. Katharina Glatz Pathologie Cutaneous Adnexal Tumors Hair
Cutaneous Adnexal Tumors Lesions with Predominant Follicular Differentiation Special Emphasis on Basal Cell Carcinoma 2014-04-01 Prof. Dr. med. Katharina Glatz Pathologie Cutaneous Adnexal Tumors Hair
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
Pancreas. Atrophy, acinar cell. Pathogenesis: Diagnostic key features:
 Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation