VENTANA PD-L1 (SP263) Assay Staining in Urothelial Carcinoma Interpretation Guide
|
|
|
- Baldwin Phillips
- 5 years ago
- Views:
Transcription
1 VENTANA PD-L1 (SP263) Assay Staining in Urothelial Carcinoma Interpretation Guide
2 2 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
3 Table of Contents Introduction 4 Intended Use of Product 4 Purpose of Interpretation Guide 4 Clinical Evaluation 5 Evaluating Staining Patterns and Intensities 5 Tissue Requirements 10 Morphology and Background Acceptability Criteria 10 Positive Tissue Control 11 VENTANA PD-L1 (SP263) Assay Scoring Algorithm for Urothelial Carcinoma Tissue 12 Overview of PD-L1 (SP263) Scoring Algorithm for Urothelial Carcinoma 14 Evaluation of Immune Cell Staining 16 PD-L1 Expression Atlas in Urothelial Carcinoma 25 Tumor Cell Cases 25 Immune Cell Cases 31 Challenging Cases 39 Challenging cases: Weak Tumor Membrane vs Cytoplasmic Staining 40 Challenging cases: Strong Immune Cell Staining Overlapping with Tumor Cell Staining 42 Challenging cases: Cases with Multiple Tissue Fragments 44 Challenging cases: Borderline PD-L1 Status 45 Challenging cases: Obscuring Endogenous Material 48 Impact of Pre-Analytical Conditions on VENTANA PD-L1 (SP263) Assay Staining 50 Fixative Recommendations to Achieve Optimal Staining Results with the VENTANA PD-L1 (SP263) Assay 50 Impact of Tissue Thickness on Assay Staining 51 Cut Slide Stability 51 References 51 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 3
4 Introduction Urothelial carcinoma (also known as urothelial cell carcinoma, transitional cell carcinoma of the urinary tract, or urothelial bladder cancer) is the most common cancer of the urinary system worldwide. The majority of urothelial tumors arise in the bladder with the remainder originating in the renal pelvis, urethra, or ureter. Transitional cell carcinoma (TCC) is the most common histologic subtype associated with bladder cancer and accounts for greater than 90% of all urothelial carcinoma cases in the industrialized world; non-urothelial subtypes (e.g., squamous cell, adenocarcinoma, small cell carcinoma) are more frequent in other areas of the world. 1 Globally, there were an estimated 429,793 new cases of bladder cancer and 165,084 deaths in In Europe alone, for 2012, there were an estimated 151,297 new cases of bladder cancer and 52,411 deaths. In 2015, it was estimated that there would be 74,000 new cases of bladder cancer and 16,000 deaths in the United States. 3 Urothelial carcinoma presents as non-muscle-invasive, muscleinvasive, or metastatic disease. The overall 5-year survival rate for metastatic urothelial carcinoma (muc) is approximately 5.4%. 4 PD-L1 is a transmembrane protein that downregulates immune responses through binding to its two receptors programmed death-1 (PD-1) and B7-1 (CD80). 5 PD-1 is an inhibitory receptor expressed on T cells following T-cell activation, which is sustained in states of chronic stimulation such as in chronic infection or cancer. 6 Binding of PD-L1 with PD-1 inhibits T cell proliferation, cytokine production, and cytolytic activity, leading to the functional inactivation or exhaustion of T cells. CD80 is a molecule expressed on antigen presenting cells and activated T cells. PD-L1 binding to CD80 on T cells and antigen presenting cells can mediate downregulation of immune responses, including inhibition of T-cell activation and cytokine production. 7 PD- L1 expression has been observed in immune cells and tumor cells. 8,9 Aberrant expression of PD-L1 on tumor cells and or tumor-associated immune cells has been reported to impede anti-tumor immunity, resulting in immune evasion. 6,9 Therefore, interruption of the PD-L1/ PD-1 pathway represents an attractive strategy to reinvigorate tumorspecific T cell immunity suppressed by the expression of PD-L1 in the tumor microenvironment. PD-L1 is expressed in a broad range of cancers including lung, melanoma, urothelial, ovarian, and colorectal cancer. Prevalence of PD-L1 expression has been reported from 12% to 100% depending on the tumor type, anti PD-L1 clone and cutoff for positivity. 10 Intended Use of Product VENTANA PD-L1 (SP263) Assay is a qualitative immunohistochemical assay using rabbit monoclonal anti-pd-l1 clone SP263 intended for use in the assessment of the PD-L1 protein in formalin-fixed, paraffin-embedded (FFPE) urothelial carcinoma tissue stained with OptiView DAB IHC Detection Kit on a VENTANA BenchMark ULTRA instrument. PD-L1 status is determined by the percentage of tumor cells with any membrane staining above background or by the percentage of tumor-associated immune cells with staining (IC+) at any intensity above background. The percent of tumor area occupied by any tumor-associated immune cells (Immune Cells Present, ICP) is used to determine IC+, which is the percent area of ICP exhibiting PD-L1 positive immune cell staining. PD-L1 status is considered High if any of the following are met: 25% of tumor cells exhibit membrane staining; or, ICP > 1% and IC+ 25%; or, ICP = 1% and IC+ = 100%. PD-L1 High status as determined by VENTANA PD-L1 (SP263) Assay was associated with increased objective response rate (ORR) in a single arm study of IMFINZI (durvalumab). This product is intended for in vitro diagnostic (IVD) use. Purpose of Interpretation Guide This guide is intended to aid pathologists in the clinical evaluation of formalin-fixed, paraffin-embedded (FFPE) urothelial carcinoma sections stained with the Assay using the Assay Scoring Algorithms in accordance with the proposed product labeling. Specifically, this guide: Provides pathologists with a tool to facilitate the evaluation of formalin-fixed, paraffin-embedded (FFPE) urothelial carcinoma sections stained with the Assay using the Assay Scoring Algorithms in accordance with the proposed product labeling. Provides photographic images that illustrate the staining patterns and intensities that may result from staining of urothelial carcinoma tissue samples with the Assay. Provides guidance in the use of placenta tissue as a system-level control when stained with the Assay. Provides photographic images of internal controls. Provides a reference for relating staining patterns to specific PD-L1 scores. Provides example images of challenging cases to provide guidance in their evaluation. 4 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide






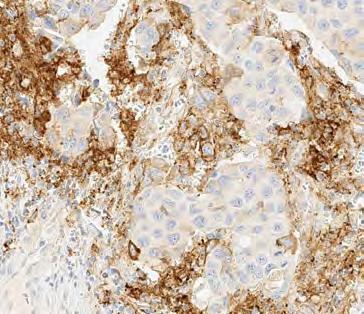
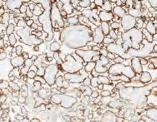
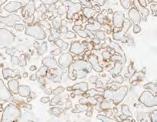
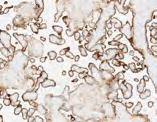
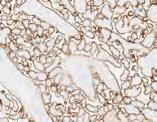
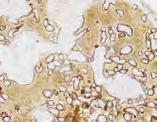
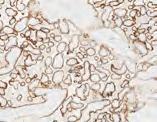
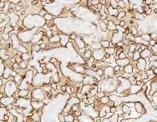
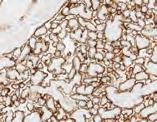
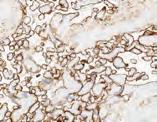
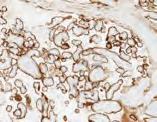
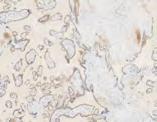
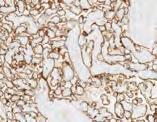
5 Clinical Evaluation Evaluating Staining Patterns and Intensities Urothelial carcinoma cases stained with the Assay are assessed for both the percentage of tumor cells with membrane staining and the percentage of tumor-associated immune cells with membrane, cytoplasm, or punctate staining. Tumor Cell Staining: Urothelial carcinoma neoplastic cells labeled with the Assay are evaluated for the percent of the tumor cells with membrane staining at any intensity of the diaminobenzidine (DAB) signal. The immunohistochemical staining in urothelial carcinoma is membranous and/or cytoplasmic, and may be expressed homogeneously or heterogeneously throughout the neoplasm. Membrane staining can have a partial or complete circumferential pattern. Cytoplasmic staining is generally diffuse with some cases displaying a finely granular quality. Tumor cell cytoplasmic staining is disregarded for determining PD-L1 expression. The total percentage of membrane signal intensities is visually estimated and used to generate the PD-L1 expression level. An isotype-matched negative control antibody is used to evaluate the presence of background in test samples and establish a staining intensity baseline. Urothelial carcinoma, H&E and Assay: Various cases demonstrating the range of membrane and cytoplasmic staining in tumor cells (10X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 5

 membrane")
 membrane staining pattern")

 Assay in")

6 Urothelial carcinoma, H&E and Assay: Tumor cells with circumferential (black arrow) and partial (blue arrow) membrane staining pattern (20X) Urothelial carcinoma, H&E and Assay: Tumor cells with weak (blue arrow) membrane staining pattern (20X) Urothelial carcinoma, H&E and Assay: Tumor cells show membranous and weak granular cytoplasmic staining (40X) 6 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide



.")
.")

7 Tumor-Associated Immune Cell Staining: Immune cells exhibit a range of staining intensities and patterns: negative to weak diffuse cytoplasmic and/or weak to strong membranous signal. A punctate pattern of staining may be seen in association with lymphocytes. PD-L1 expression has been observed in lymphocytes, macrophages, histiocytes, plasma cells, and neutrophils. staining. Immune cell staining is assessed by initially reviewing the entire tumor area and determining the percentage of the tumor area occupied by immune cells (ICP). Next the percentage of immune cells demonstrating any pattern of PD-L1 expression within the tumor area is visually estimated (IC+). The percentage of tumor-associated immune cells with staining in urothelial carcinoma cases is evaluated in addition to tumor cell Urothelial carcinoma, H&E and Assay: Various cases demonstrating the range and patterns of immune cells staining (10X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 7


 and membranous (black")
 Assay: Scattered")

 (20X)")

8 Urothelial carcinoma, H&E and Assay: Positive macrophage staining (blue outline) with adjacent PD-L1 negative tumor (20X) Urothelial carcinoma, H&E and Assay: Punctate (blue outline) and membranous (black arrow) immune cell staining with adjacent PD-L1 negative tumor (20X) Urothelial carcinoma, H&E and Assay: Scattered immune cells with punctate staining infiltrating throughout tumor (single example circled in blue) (20X) 8 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
 within the tumor demonstrating PD-L1 staining.")
 Assay in Urothelial Carcinoma")
9 NSCLC, H&E and Assay: Case with rare neutrophil-only infiltrate (blue arrow) within the tumor demonstrating PD-L1 staining. Tumor cell membrane staining also present (black arrow) (40X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 9
10 Tissue Requirements The VENTANA PD-L1 (SP263) Assay requires one serial tissue section for hematoxylin and eosin (H&E) staining, a second serial tissue section for negative control antibody staining, and a third serial tissue section for staining with the VENTANA PD-L1 (SP263) Assay. In addition, normal human term placenta tissue can be used as a control for the PD-L1 (SP263) Assay. This tissue shows moderate to strong uniform staining of the membrane and weak to strong uniform staining of the cytoplasm of trophoblast-lineage cells. Placental stromal tissue and vasculature can be used for assessment of any background staining. If H&E evaluation indicates that the patient specimen is inadequate then a new specimen should be obtained. Repeat staining of a specimen should be carried out on unstained slides if (1) the tissue run control slide does not exhibit acceptable staining; (2) the negative control case slide does not exhibit acceptable staining; or (3) the VENTANA PD-L1 (SP263) Assay stained case slide (the PD-L1 IHC slide) is not evaluable. If the last of these slides is not interpretable due to artifacts, edge effects, necrosis, lack of tissue, or any other reason, then the slide cannot be used for clinical evaluation. If controls are acceptable and the VENTANA PD-L1 (SP263) Assay stained slide is evaluable, the slide can be evaluated by a trained pathologist as described in the Scoring Criteria. Morphology and Background Acceptability Criteria Tissue morphology and background acceptability are assessed for each patient case using the criteria described in Tables 1 and 2. Table 1: Morphology Acceptability Criteria Interpretation Microscope Observation Acceptable Not Acceptable Cellular elements of interest are visualized allowing interpretation of the stain. Cellular elements of interest are not visualized compromising interpretation of the stain. Table 2: Background Acceptability Criteria Interpretation Microscope Observation Acceptable Not Acceptable Non-specific staining that is not obtrusive to interpretation of specific staining. Non-specific staining that is obtrusive to interpretation of specific staining. 10 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
 Assay staining procedure performed.")

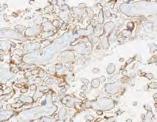
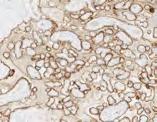
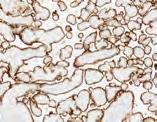
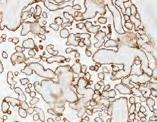
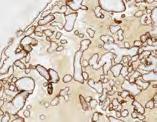
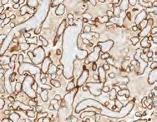
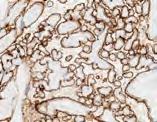
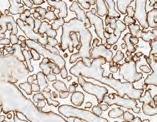
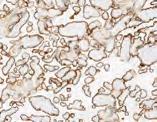
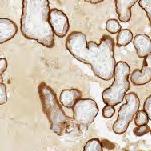
11 Positive Tissue Control A known positive control tissue fixed and processed in the same manner as the patient specimens should be run for each set of test conditions and with every VENTANA PD-L1 (SP263) Assay staining procedure performed. The control tissue (an index case) should be a fresh autopsy, biopsy, surgical specimen prepared and fixed as soon as possible in a manner identical to patient specimens. This tissue may be used to monitor all steps of specimen processing and staining. A tissue section fixed or processed differently from the test specimen can be used as a control for reagents and staining but not for fixation or tissue preparation. A positive urothelial carcinoma case with moderate staining is more suitable for quality control than one that stains strongly; it can be used to detect minor levels of reagent degradation or out-of-specification issues that might be instrumentrelated. Positive membrane staining of neoplastic cells in the control tissue confirms that the VENTANA PD-L1 (SP263) antibody was applied and the instrument functioned properly. The positive tissue control should be used only to monitor performance; it should not be used to aid the clinical diagnosis of patient samples. Additionally, the VENTANA PD-L1 (SP263) Assay can utilize as a positive control human term placental tissue, which shows moderate to strong uniform staining of the membrane and weak to strong uniform staining of the cytoplasm of trophoblast-lineage cells. Placental stromal tissue and vasculature can be used for assessment of any background staining. Please refer to Table 3. Placenta, VENTANA PD-L1 (SP263) Assay: Strong uniform membrane staining and moderate cytoplasmic staining of trophoblast-lineage cells (10X) Placenta, VENTANA PD-L1 (SP263) Assay: Stroma and vasculature within villi show no PD-L1 staining (20X) Table 3: Placenta Tissue Control Evaluation Criteria for the Ventana PD-L1 (SP263) Assay Acceptable Not Acceptable Moderate to strong uniform membrane staining of trophoblast-lineage cells, and placental stroma and vasculature with no staining. No to weak uniform membrane staining of trophoblast lineage cells and/or specific staining within placental stromal and vascular tissue. VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 11



12 VENTANA PD-L1 (SP263) Assay Scoring Algorithm for Urothelial Carcinoma Tissue PD-L1 status and expression level is assigned by a trained pathologist based on their evaluation of the percentage of specific staining for both tumor and tumor-associated immune cells. PD-L1 status is based on the total percent of tumor cells with membrane staining or the total percent of tumor-associated immune cells with staining (IC+) at any intensity. Specifically, this guide highlights an expression level of greater than or equal to 25% of tumor cells with membrane staining or of tumor-associated immune cells with staining. In cases where the percent of tumor-associated immune cells in the tumor area (ICP) is 1%, IC+ is scored as either 0%, <100% or 100% due to the difficulties in estimating the percent staining in small volumes of immune cells in low measures. The small amount of PD-L1 staining observed in cases with < 100% IC+, should be considered as < 25% PD-L1 expression. Please refer to Table 4. Interpretation of urothelial carcinoma cases stained with the Assay is based on the criteria noted in the table below. Images of various expression level staining patterns are provided in the subsequent sections. Please refer to Table 4. Table 4: VENTANA PD-L1 (SP263) Assay Scoring Algorithm for Urothelial Carcinoma PD-L1 Interpretation Staining Description PD-L1 status is determined by the percentage of tumor cells with any membrane staining above background or by the percentage of tumor-associated immune cells with staining (IC+) at any intensity above background. Percent of tumor area occupied by any tumor-associated immune cells (ICP) is used to determine IC+, which is the percent area of ICP exhibiting PD-L1 positive immune cell staining. High PD-L1 Status is considered high if any of the following are met: 25% of tumor cells exhibit membrane staining; or, ICP > 1% and IC+ 25%; or, ICP = 1% and IC+ = 100%. Low/negative PD-L1 Status is considered low/negative if: none of the criteria for PD-L1 High Status are met. PD-L1 LOW/NEGATIVE STATUS: TUMOR CELL EXPRESSION < 25% 0% 5% 10% 12 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide








13 PD-L1 HIGH STATUS: TUMOR CELL EXPRESSION 25% 25% 50% 100% PD-L1 LOW/NEGATIVE STATUS: TUMOR-ASSOCIATED IMMUNE CELL EXPRESSION < 25% 0% IC+ 10% IC+ 20% IC+ PD-L1 HIGH STATUS: TUMOR-ASSOCIATED IMMUNE CELL EXPRESSION 25% 30% IC+ 60% IC+ 80% IC+ VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 13
14 Overview of PD-L1 (SP263) Scoring Algorithm for Urothelial Carcinoma 1. H&E slide is reviewed for viable tumor, tumor-associated immune cells and tumor area. a. Tumor area encompasses the tumor proper, associated desmoplastic stroma and immune cells infiltrating the tumor and contained within the desmoplasia. 2. Visually, tumor-associated immune cells are densely aggregated (with no intervening stroma) within the tumor area when estimating Immune Cells Present (ICP). a. Tumor associated immune cells include those present within the tumor reactive stroma, between the tumor islands and those invading the tumor proper. 3. The ICP percentage is scored as 0%, 1%, 5%, and deciles and quartiles (10, 20, 25, 30, 40, 50, 60, 70, 75, 80, 90, 100). a. If a raw percentage falls between a decile or quartile, standard mathematical rounding is used to score to the nearest decile or quartile. b. When differentiating between 1% and 5% ICP, a raw percentage estimate of 2% is rounded to 1% and an estimate of 3% to 4% is rounded to 5%. 4. PD-L1 stained slide is reviewed for tumor cell and immune cell staining. 5. Estimate the percentage of tumor cells with partial or complete membrane staining at any intensity. 6. The percentage of immune cells (within the ICP) expressing PD- L1 (IC+) is estimated. a. Immune cells with any staining (membranous, cytoplasmic, or punctate) at any intensity are visually aggregated within the ICP to estimate IC+. b. IC+ is scored as deciles and quartiles (0, 10, 20, 25, 30, 40, 50, 60, 70, 75, 80, 90, 100). 7. For cases with 1% ICP, the percentage estimate for IC+ is reported as 0%, <100%, or 100%. 14 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
.")



15 Overview of PD-L1 (SP263) Scoring Algorithm for Urothelial Carcinoma Evaluate H&E for viable tumor, and tumor area (red). Review tumor area for immune cells (black) at 10X and visually aggregate immune cells at 2X or 4X to determine ICP. Tumor cells Immune cells Review PD-L1 stained slide at 10X or 20X to distinguish tumor cell and immune cell staining. Review tumor cells at 10X or 20X to evaluate for membrane staining at any intensity. Determine percentage of tumor cells with membrane staining by reviewing at 2X or 4X, if needed. Review immune cells at 10X or 20X to evaluate for any staining at any intensity. Visually aggregate staining immune cells (blue) at 2X or 4X and compare to ICP to estimate IC+. VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 15


16 Evaluation of Immune Cell Staining A variety of immune cells display staining with the Assay, and include lymphocytes, macrophages, histiocytes, reticular dendritic cells, plasma cells and neutrophils. The H&E-stained slide is initially examined to determine the total percentage of the tumor area (tumor cells and any desmoplastic stroma) involved by immune cells with no intervening stroma (ICP). Areas not considered part of the tumor area include non-viable tumor such as those with cautery or crush artifacts, and extensive necrosis. Normal lymphoid tissue uninvolved by the neoplasm, as seen in lymph nodes with metastatic tumor, is not considered as a part of the tumor area or immune cells involving the tumor. The PD-L1 IHC slide is then scored for the percentage of tumorassociated immune cells staining for PD-L1 (IC+). Membranous, cytoplasmic, and punctate PD-L1 immune cell staining are all included in the estimation. In cases where positively-staining immune cells are intermixed with positively-staining tumor cells, it can be difficult to quantify the amount of staining for each component. Examples of immune cell interpretation are given in the following photo sets. The following steps describe the estimation of tumor-associated immune cell staining percentage. Tumor-associated immune cell staining percentage estimation: 1. Review case H&E to assess viable tumor with attached desmoplastic stroma containing tumor-associated immune cells. Tumor associated immune cells include those present within the tumor reactive stroma, between the tumor islands and those invading the tumor proper. Tumor within lymphatics is not included within the tumor area. Immune Cell scoring 1: Tumor-associated immune cells (black arrows) within the tumor area (blue outline) are present at the leading edge of the tumor and are included in ICP estimation. A separate aggregate of lymphocytes is not within the tumor area (black outline) (4X) 16 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
.")




17 2. Lower magnification review is recommended to perform the percentage estimate of immune cells within and adjacent to the tumor area (ICP). Immune cells located within blood vessels and lymphatics are disregarded. Immune Cell scoring 2: Tumor area containing tumor cells, desmoplastic stroma and tumor-associated immune cells is outlined in blue, which includes immune cell aggregates identified by black arrows. Immune cells outside of the tumor area are also present (black outlines) (1X) 3. Exclude non-neoplastic areas not involved by tumor, areas with necrotic tumor, crush and cautery artifacts. Immune Cell scoring 3: Tumor area consists of only viable areas of tumor and desmoplasia (areas outlined in blue). Any necrosis, cautery artifact, crush artifact or large areas of non-neoplastic tissue are disregarded (3X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 17



18 4. If tumor islands are separated by muscle or stroma, they are included as part of the tumor area if the tumor borders on both sides within a 10X field. NOT included in tumor area INCLUDED in tumor area 10X 10X Immune Cell scoring 4: The circled areas show large areas of fibromuscular stroma uninvolved by tumor. When viewed at higher power (10X), the stroma with tumor on both sides within a single field of view (blue) is included in the overall tumor area. When the large bundle of fibromuscular stroma is not bordered by tumor within a single 10X field (black), it is not included in the overall tumor area. (1X) 18 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide

 shows base of")
.")
 (5X) are included in estimation of ICP")
19 5. For noninvasive urothelial carcinoma (papillary carcinoma), include the immune cells within the fibrovascular cores as well as within the immediately adjacent base of the frond/stalk. A B A B Immune Cell scoring 5: Double sided arrow (black) shows base of papillary tumor with the tumor area for this noninvasive urothelial carcinoma outlined (blue). Immune cells from the intratumoral fibrovascular core (A) (10X) and adjacent base of the stalk (B) (5X) are included in estimation of ICP (0.8X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 19
.")
 and then densely aggregated (illustrated by the smaller black areas) in order to estimate the percentage of the tumor area with immune cells, or")
20 6. Visually estimate the area occupied by the tumor-associated immune cells relative to the total tumor area (ICP = percent of tumor area occupied by immune cells). Immune Cell scoring 6: The regions occupied by immune cells within the tumor area in the upper image (blue outlines) are identified in the lower image (gray outlines) and then densely aggregated (illustrated by the smaller black areas) in order to estimate the percentage of the tumor area with immune cells, or ICP in this example 10% (black areas together relative to the tumor area) (5X) 20 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
 in order to estimate the percentage of the tumor area")

21 Immune Cell scoring 7: The stromal regions occupied by widely dispersed immune cells (blue outlines) are identified. When the immune cells are densely aggregated (represented by the black area) in order to estimate the percentage of the tumor area with immune cells, the ICP in this example is 5% (10X) Immune Cell scoring 8: The immune cell infiltrates with neutrophils and eosinophils, are included in the ICP estimation. The ICP in this example is 25% (10X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 21
 Immune Cell")
 22 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma")
22 Immune Cell scoring 9: In this field of view, the ICP for the small amount of immune cells in the upper right corner is 1% (10X) Immune Cell scoring 10: The ICP for this field of view when densely aggregated is 5% (10X) 22 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide


 and can be seen densely aggregated")
 are highlighted in red")
 (5X).")
23 7. Review PD-L1-stained slide and estimate the percentage of tumor-associated immune cells which demonstrate PD-L1 expression (IC+) including diffuse cytoplasmic, linear membrane and punctate immune cell staining. Immune Cell scoring 11: The immune cells comprising ICP are outlined in blue (upper image) and can be seen densely aggregated in the lower image. The immune cells with PD- L1 staining (IC+) are highlighted in red (upper image) and when aggregated constitute 25% of the ICP (lower image) (5X). Please refer to the associated H&E image contained within this guide, Immune Cell scoring 6. VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 23

.")
). 9.")
24 8. When evaluating lymph node metastases the reactive stroma generated by the tumor is included as part of the tumor area when determining ICP. In cases where the tumor does not generate a stromal response, the tumor area is limited to the tumor nests and adjacent immune cells in direct contact with the tumor only. Any immune cells part of the uninvolved lymphoid tissue are disregarded for ICP. Immune Cell scoring 12: In this metastatic tumor to a lymph node, the tumor area containing tumor cells, desmoplastic stroma and immune cells is outlined in blue (4X). Higher power shows immune cells that are included as part of ICP within the reactive stroma (inset A (20X)). Along the periphery of the metastatic nodule only immune cells immediately adjacent to the tumor cells outlined in blue are included as part of ICP (inset B (20X)). 9. Only in cases where the ICP equals 1%, the IC+ is only scored as 0%, <100% or 100% due to the difficult nature of quantifying expression is such small amounts of cells. 10. If the PD-L1-stained slide shows more immune cell staining than the initial ICP estimation from the H&E slide, refer back to the H&E slide and revise the ICP percentage, if necessary. 24 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide

 (Top row H&E 10X, PD-L1 20X.")
 VENTANA PD-L1 (SP263) Assay in Urothelial")
25 PD-L1 Expression Atlas in Urothelial Carcinoma Tumor Cell Cases Tumor Cell Case 1: Tumor cells with 0% staining, Immune cells with 0% staining. (IC+) (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 25

 (Top row H&E 10X, PD-L1 20X.")
 26 VENTANA PD-L1 (SP263) Assay in")
26 Tumor Cell Case 2: Tumor cells with 0% staining, Immune cells with 80% staining. (IC+) (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) 26 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide


27 Tumor Cell Case 3: Tumor cells with 10% staining, Immune cells with 40% staining (IC+) (10X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 27


28 Tumor Cell Case 4: Tumor cells with 25% staining, Immune cells with 10% staining (IC+) (10X) 28 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
 (10X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation")
29 Tumor Cell Case 5: Tumor cells with 50% staining, Immune cells with 20% staining (IC+) (10X) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 29

 (Top row H&E 10X, PD-L1 20X.")
 30 VENTANA PD-L1 (SP263) Assay in")
30 Tumor Cell Case 6: Tumor cells with 100% staining, Immune cells with 20% staining. (IC+) (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) 30 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
,")

 VENTANA PD-L1 (SP263) Assay in")
31 Immune Cell Cases Immune Cell Case 1: Immune cells with 0% staining (IC+), Tumor cells with 0% staining. (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 31
, Tumor")

 32 VENTANA PD-L1 (SP263) Assay in")
32 Immune Cell Case 2: Immune cells with 10% staining (IC+), Tumor cells with 80% staining. (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) 32 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
, Tumor")

 VENTANA PD-L1 (SP263) Assay in")
33 Immune Cell Case 3: Immune cells with 30% staining (IC+), Tumor cells with 10% staining. (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 33
, Tumor cells")

 34 VENTANA PD-L1 (SP263) Assay in")
34 Immune Cell Case 4: Immune cells with 25% staining (IC+), Tumor cells with 100% staining. (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) 34 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
, Tumor")

 VENTANA PD-L1 (SP263) Assay in")
35 Immune Cell Case 5: Immune cells with 40% staining (IC+), Tumor cells with 10% staining. (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 35
, Tumor cells")

 36 VENTANA PD-L1 (SP263) Assay in")
36 Immune Cell Case 6: Immune cells with 50% staining (IC+), Tumor cells with 100% staining. (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) 36 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
, Tumor")

 VENTANA PD-L1 (SP263) Assay in")
37 Immune Cell Case 7: Immune cells with 60% staining (IC+), Tumor cells with 0% staining. (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 37
, Tumor cells")

 38 VENTANA PD-L1 (SP263) Assay in")
38 Immune Cell Case 8: Immune cells with 90% staining (IC+), Tumor cells with 100% staining. (Top row H&E 10X, PD-L1 20X. Bottom row PD-L1 10X.) 38 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
39 Challenging Cases Cases are given a PD-L1 score according to percentage of tumor cells with membrane staining and tumor-associated immune cells. Various staining patterns and morphologic features may make interpretation and quantification of tumor membrane staining difficult. Some cases may be particularly challenging due to the following issues: Weak Tumor Cell Membrane vs Weak Tumor Cell Cytoplasmic Staining Some specimens may exhibit weak cytoplasmic staining of the tumor cells that may be confused at low power with weak tumor cell membrane staining. For this reason when evaluating PD-L1 IHC stained slides, weak staining should be confirmed with examination at higher powers to distinguish between tumor cell membranous and cytoplasmic staining. Obscuring Endogenous Material Occasionally in urothelial carcinoma samples endogenous material, such as melanin pigment or hemosiderin, may obscure and interfere with interpretation of PD-L1 IHC staining of tumor and immune cells. Comparison of the negative isotype control slide with the PD-L1 stained slide can aid in differentiating between biomarker staining and endogenous material. Non-specific staining can also be seen on the PD-L1 stained slide in areas of necrosis. Some challenging cases are shown. Strong Immune Cell Staining Overlapping with Tumor Cell Staining Some tumors may contain an extensive inflammatory component both surrounding the tumor and infiltrating within the tumor. In instances when significant staining is seen for both tumor and immune cells, it can be challenging to differentiate and quantify the PD-L1 IHC staining between the two cell populations. The presence of immune cells infiltrating the tumor should be confirmed using the H&E slide. The pattern of PD-L1 staining and nuclear morphology are utilized to help attribute expression to immune cells (punctate staining, small uniform nucleus) and tumor cells (linear membrane staining, large irregular nucleus). Borderline PD-L1 (SP263) Status Some cases are near the cut-off between a PD-L1 High and Low/negative status. These cases are particularly challenging to estimate the percent of target cells with staining. For these borderline cases it may be helpful to view the case at a magnification that enables the entire tumor area to be assessed. Consultation with a trained colleague may also be helpful. Cases with Multiple Tissue Fragments Urothelial carcinoma samples resulting from transurethral resections of the bladder (TURB) can result in challenging cases complicated by multiple fragments of tissue scattered across the slide with varying amounts of necrosis, crush/cautery artifact, viable tumor cells and/or tumor-associated immune cells. A fragment-by-fragment examination approach with individual percent staining estimates followed by an overall average can help in the evaluation. VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 39



 (Top row H&E 10X, PD-L1 10X.")
40 Challenging cases: Weak Tumor Membrane vs Cytoplasmic Staining Challenging Case 1: The area outlined in blue (10X PD-L1 image, upper right) contains weak tumor cell staining that is difficult to distinguish. Examination at higher power (20X) shows there is scattered weak tumor membrane staining. For 10X image: Tumor cells with 40% staining, Immune cells with 80% staining. (IC+) (Top row H&E 10X, PD-L1 10X. Bottom row PD-L1 20X.) 40 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide

 that should also be counted towards the total percentage of membrane staining.")
41 Challenging Case 2: Tumor cells with moderate or stronger membrane staining are readily identified within the right half of this field. Careful examination of the tumor demonstrates cells with weak membrane expression (blue outlines) that should also be counted towards the total percentage of membrane staining. VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 41


 as well as")


42 Challenging cases: Strong Immune Cell Staining Overlapping with Tumor Cell Staining Challenging Case 3: TC and IC intermixed together with both expressing PD-L1. In areas with strong TC staining, IC can only be evaluated where discernible from tumor cell staining. The different patterns of IC staining (punctate pattern) as well as nuclear morphology can be used to identify PD-L1 expression. The blue outlines contain areas with discernible immune cell staining with the green outlined area having scattered punctate immune cell staining. Tumor cells with 100% staining, Immune cells with 25% staining (IC+) (Top row H&E 10X, PD-L1 10X. Bottom row PD-L1 20X.) 42 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide


 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma")
43 Challenging Case 4: TC and IC intermixed together with TC membrane staining more distinct and IC difficult to evaluate and can only be scored along the periphery of the tumor. Tumor cells with 100% staining. (Top row H&E 10X, PD-L1 10X. Bottom row PD-L1 20X.) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 43

 Assay in Urothelial Carcinoma Interpretation")
44 Challenging cases: Cases with Multiple Tissue Fragments Challenging Case 5: TURB specimen contains multiple pieces with crush artifact, blood clot and necrosis which shows non-specific staining on the IHC slide(1x). 44 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide


 Assay")
45 Challenging cases: Borderline PD-L1 Status Challenging Case 6: Weak tumor cell staining seen at 10X magnification is difficult to distinguish between membrane and cytoplasmic staining. Examination at higher power (20X) reveals tumor cells with 20% weak, delicate membranous staining. VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 45


46 Challenging Case 7: Borderline TC PD-L1 expression with 25% tumor cell membrane staining (10X) 46 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide


 VENTANA PD-L1 (SP263) Assay in")
47 Challenging Case 8: Borderline IC PD-L1 expression with an IC+ of 20% (20X). (Top row H&E 10X, PD-L1 10X. Bottom row PD-L1 20X.) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 47


 (20X).")

48 Challenging cases: Obscuring Endogenous Material Challenging Case 9: Case contains anthracotic pigment (red arrow) overlapping with punctate immune cell staining (blue arrow) as well as tumor cell membrane staining (black arrow) (20X). (Top row H&E 10X, Neg Rb 10X. Bottom row PD-L1 10X.) 48 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide


 VENTANA PD-L1 (SP263) Assay in")
49 Challenging Case 10: Large necrotic areas can have non-specific DAB staining which may be confused with immune cell staining. (Top row H&E 10X, PD-L1 10X. Bottom row PD-L1 20X.) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 49

















50 Impact of Pre-Analytical Conditions on VENTANA PD-L1 (SP263) Assay Staining Fixative Recommendations to Achieve Optimal Staining Results with the VENTANA PD-L1 (SP263) Assay Ventana recommends fixation in 10% NBF for 6-72 hours. Acceptable fixatives and fixation times are outlined in blue. VENTANA PD-L1 (SP263) Assay Staining of Placenta Tissue Across Fixatives and Fixation Times Time Fixative Point (Hrs) 10% NBF Zinc Formalin PREFER fixative** AFA** Alcoholic Formalin** 95% Ethanol** 1* NOTES *One hour fixation time is not recommended for all fixative types **Use of PREFER fixative and 95% Ethanol (weaker staining) or alcoholic fixatives (high background) is not recommended. See additional higher magnification images to the right. 50 VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide
51 Impact of Tissue Thickness on Assay Staining Ventana recommends tissue thickness of 4-5 microns for use with the Assay. Cut Slide Stability Sections approximately 4-5 microns in thickness should be cut and mounted on positively charged glass slides. Slides should be stained within 6 months of sectioning. References 1. Chalasani V, Chin JL, Izawa JI. Histologic variants of urothelial bladder cancer and nonurothelial histology in bladder cancer. Can Urol Assoc J. 2009;3(6 Suppl 4):S Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0. Cancer Incidence and Mortality Worldwide: IARC CancerBase No Published Updated Accessed American Cancer Society. Cancer Facts & Figures Atlanta: American Cancer Society; Howlader N, Noone AM, Krapcho M, et al. (eds). SEER Cancer Statistics Review (CSR), National Cancer Institute. Published Updated Accessed Keir ME, Butte MJ, Freeman GJ, et al. PD-1 and its ligands in tolerance and immunity. Annu Rev Immunol 2008;26: Blank C, Mackensen A. Contribution of the PD-L1/PD-1 pathway to T-cell exhaustion: an update on implications for chronic infections and tumor evasion. Cancer Immunol Immunother. 2007;56(5): Butte MJ, Keir ME, Phamduy TB, et al. Programmed death-1 ligand 1 interacts specifically with the B7-1 costimulatory molecule to inhibit T cell responses. Immunity. 2007;27(1): Dong H, Zhu G, Tamada K, Chen L. B7-H1, a third member of the B7 family, co-stimulates T-cell proliferation and interleukin-10 secretion. Nat Med. 1999;5(12): Massard C, Gordon MS, Sharma S, et al. Safety and efficacy of durvalumab (MEDI4736), an anti-programmed cell death ligand-1 immune checkpoint inhibitor, in patients with advanced urothelial bladder cancer. J Clin Oncol. 2016; 34(26): Patel SP, Kurzrock R. PD-L1 Expression as a Predictive Biomarker in Cancer Immunotherapy. Mol Cancer Ther. 2015;14(4) VENTANA PD-L1 (SP263) Assay in Urothelial Carcinoma Interpretation Guide 51

52 Ventana Medical Systems, Inc E. Innovation Park Drive Tucson, Arizona USA (USA) Ventana Medical Systems, Inc. All rights reserved. VENTANA, BENCHMARK, OPTIVIEW, and the VENTANA logo are trademarks of Roche. All other trademarks are the property of their respective owners US Rev A VENTANA Empowering Innovation
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy
 Assay Guiding immunotherapy") VENTANA PD-L1 (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA PD-L1 (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA PD-L1 (SP142) Assay Identify patients most
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA PD-L1 (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA PD-L1 (SP142) Assay Identify patients most
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy in NSCLC
 Assay Guiding immunotherapy in NSCLC") VENTANA (SP142) Assay Guiding immunotherapy in NSCLC Hiker s path: VENTANA (SP142) Assay on non-small cell lung cancer tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess NSCLC patient benefit
VENTANA (SP142) Assay Guiding immunotherapy in NSCLC Hiker s path: VENTANA (SP142) Assay on non-small cell lung cancer tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess NSCLC patient benefit
VENTANA PD-L1 (SP142) Assay
 Assay") VENTANA (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess UC patient benefit from TECENTRIQ
VENTANA (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess UC patient benefit from TECENTRIQ
VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue
 VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue VENTANA anti-mlh1 (M1) Mouse Monoclonal Primary Antibody VENTANA anti-pms2 (A16-4) Mouse Monoclonal Primary Antibody VENTANA
VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue VENTANA anti-mlh1 (M1) Mouse Monoclonal Primary Antibody VENTANA anti-pms2 (A16-4) Mouse Monoclonal Primary Antibody VENTANA
Immunotherapy in NSCLC Pathologist role
 Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Digital Pathology and CAP Guidelines
 Digital Pathology and CAP Guidelines Frequently asked questions The VENTANA family of digital pathology products empowers you with the convenience of a comprehensive image and workflow solution. When used
Digital Pathology and CAP Guidelines Frequently asked questions The VENTANA family of digital pathology products empowers you with the convenience of a comprehensive image and workflow solution. When used
Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma. PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use
 Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use For countries outside of the United States, see the local
Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use For countries outside of the United States, see the local
Bladder Case 1 SURGICAL PATHOLOGY REPORT. Procedure: Cystoscopy, transurethral resection of bladder tumor (TURBT)
") Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Supplemental materials
 Supplemental materials 1 Supplemental Fig. 1 Immunogram This immunogram summarizes patient clinical data and immune parameters at corresponding time points for Patient IMF-32. The top panel illustrates
Supplemental materials 1 Supplemental Fig. 1 Immunogram This immunogram summarizes patient clinical data and immune parameters at corresponding time points for Patient IMF-32. The top panel illustrates
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Anti-PD-L1 antibody [28-8] ab205921
![Anti-PD-L1 antibody [28-8] ab205921](/thumbs/84/91196262.jpg "Anti-PD-L1 antibody [28-8] ab205921") Anti-PD-L1 antibody [28-8] ab205921 2 Abreviews 16 References 15 Images Overview Product name Anti-PD-L1 antibody [28-8] Description Tested applications Species reactivity Immunogen Rabbit monoclonal [28-8]
Anti-PD-L1 antibody [28-8] ab205921 2 Abreviews 16 References 15 Images Overview Product name Anti-PD-L1 antibody [28-8] Description Tested applications Species reactivity Immunogen Rabbit monoclonal [28-8]
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Predictive Biomarkers for Pembrolizumab. Eric H. Rubin, M.D.
 Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
PD-L1 and Immunotherapy of GI cancers: What do you need to know
 None. PD-L1 and Immunotherapy of GI cancers: What do you need to know Rondell P. Graham September 3, 2017 2017 MFMER slide-2 Disclosure No conflicts of interest to disclose 2017 MFMER slide-3 Objectives
None. PD-L1 and Immunotherapy of GI cancers: What do you need to know Rondell P. Graham September 3, 2017 2017 MFMER slide-2 Disclosure No conflicts of interest to disclose 2017 MFMER slide-3 Objectives
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al -
 Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Interpretation guide. Abnormal cytology can t hide anymore
 Interpretation guide Abnormal cytology can t hide anymore Unique dual-biomarker technology makes you certain about the presence of transforming HPV infection. The science that creates certainty. Table
Interpretation guide Abnormal cytology can t hide anymore Unique dual-biomarker technology makes you certain about the presence of transforming HPV infection. The science that creates certainty. Table
CINtec PLUS Cytology. Interpretation training
 CINtec PLUS Cytology Interpretation training Objectives After reviewing this learning module, you will have a basic understanding of how to interpret CINtec PLUS Cytology, including: The mechanism of action
CINtec PLUS Cytology Interpretation training Objectives After reviewing this learning module, you will have a basic understanding of how to interpret CINtec PLUS Cytology, including: The mechanism of action
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
International Society of Breast Pathology. Immune Targeting in Breast Cancer. USCAP 2017 Annual Meeting
 International Society of Breast Pathology USCAP 2017 Annual Meeting Immune Targeting in Breast Cancer Ashley Cimino-Mathews, MD Assistant Professor of Pathology and Oncology The Johns Hopkins Hospital
International Society of Breast Pathology USCAP 2017 Annual Meeting Immune Targeting in Breast Cancer Ashley Cimino-Mathews, MD Assistant Professor of Pathology and Oncology The Johns Hopkins Hospital
Multiple Primary and Histology Site Specific Coding Rules URINARY. FLORIDA CANCER DATA SYSTEM MPH Urinary Site Specific Coding Rules
 Multiple Primary and Histology Site Specific Coding Rules URINARY 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways to view the Multiple l Primary/Histology
Multiple Primary and Histology Site Specific Coding Rules URINARY 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways to view the Multiple l Primary/Histology
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we
 9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Assessment Run C1 2017
 Assessment Run C1 2017 PD-L1 The first assessment in this new NordiQC Companion module C1 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories to identify patients
Assessment Run C1 2017 PD-L1 The first assessment in this new NordiQC Companion module C1 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories to identify patients
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano
 Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano Unit of Pathology Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Foggia,Italy p.graziano@operapadrepio.it Disclosure
Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano Unit of Pathology Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Foggia,Italy p.graziano@operapadrepio.it Disclosure
Identifying ALK+ NSCLC patients for targeted treatment
 VENTANA (D5F3) CDx Assay Identifying + NSCLC patients for targeted treatment VENTANA (D5F3) CDx Assay Identify + NSCLC patients eligible for treatment with XORI, ZYKADIA or ALECENSA NSCLC tissue samples
VENTANA (D5F3) CDx Assay Identifying + NSCLC patients for targeted treatment VENTANA (D5F3) CDx Assay Identify + NSCLC patients eligible for treatment with XORI, ZYKADIA or ALECENSA NSCLC tissue samples
VENTANA ALK (D5F3) CDx Assay
 CDx Assay") VENTANA ALK (D5F3) CDx Assay 790-4796 06687199001 50 Figure 1. VENTANA ALK (D5F3) CDx Assay staining in non-small cell lung carcinoma. INTENDED USE VENTANA ALK (D5F3) CDx Assay is intended for the qualitative
VENTANA ALK (D5F3) CDx Assay 790-4796 06687199001 50 Figure 1. VENTANA ALK (D5F3) CDx Assay staining in non-small cell lung carcinoma. INTENDED USE VENTANA ALK (D5F3) CDx Assay is intended for the qualitative
Emerging Tissue and Serum Markers
 Emerging Tissue and Serum Markers for Immune Checkpoint Inhibitors Kyong Hwa Park MD, PhD Medical Oncology Korea University College of Medicine Contents Immune checkpoint inhibitors in clinical practice
Emerging Tissue and Serum Markers for Immune Checkpoint Inhibitors Kyong Hwa Park MD, PhD Medical Oncology Korea University College of Medicine Contents Immune checkpoint inhibitors in clinical practice
Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma
 Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Interpreting Therapeutic Response on Immune Cell Number and Spatial Distribution within the Tumor Microenvironment. Lorcan Sherry, CSO OracleBio
 Interpreting Therapeutic Response on Immune Cell Number and Spatial Distribution within the Tumor Microenvironment Lorcan Sherry, CSO OracleBio Company Overview OracleBio is a specialised CRO providing
Interpreting Therapeutic Response on Immune Cell Number and Spatial Distribution within the Tumor Microenvironment Lorcan Sherry, CSO OracleBio Company Overview OracleBio is a specialised CRO providing
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Assessment Run C3 2018
 Assessment Run C3 2018 PD-L1 Amended version May 14 th 2018 The third assessment in NordiQC Companion module C3 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories
Assessment Run C3 2018 PD-L1 Amended version May 14 th 2018 The third assessment in NordiQC Companion module C3 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
PD-L1 Analyte Control DR
 Quality in Control PD-L1 Analyte Control DR PD-L1_PI_v2 Product Codes: HCL019, HCL020 and HCL021 Contents PD-L1 Analyte Control DR 2 What is PD-L1? 3 The Role of PD-L1 in Cancer 3 PD-L1 Assessment 4 PD-L1
Quality in Control PD-L1 Analyte Control DR PD-L1_PI_v2 Product Codes: HCL019, HCL020 and HCL021 Contents PD-L1 Analyte Control DR 2 What is PD-L1? 3 The Role of PD-L1 in Cancer 3 PD-L1 Assessment 4 PD-L1
Mucin-producing urothelial-type adenocarcinoma of prostate: report of two cases of a rare and diagnostically challenging entity
 & 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Mucin-producing urothelial-type adenocarcinoma of prostate: report of two cases of a rare and diagnostically challenging
& 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Mucin-producing urothelial-type adenocarcinoma of prostate: report of two cases of a rare and diagnostically challenging
Corporate Medical Policy
 Corporate Medical Policy Microarray-based Gene Expression Testing for Cancers of Unknown File Name: Origination: Last CAP Review: Next CAP Review: Last Review: microarray-based_gene_expression_testing_for_cancers_of_unknown_primary
Corporate Medical Policy Microarray-based Gene Expression Testing for Cancers of Unknown File Name: Origination: Last CAP Review: Next CAP Review: Last Review: microarray-based_gene_expression_testing_for_cancers_of_unknown_primary
Product Introduction. Product Codes: HCL029, HCL030 and HCL031. Issue
 Product Introduction Product Codes: HCL029, HCL030 and HCL031 Issue 1. 180510 Contents Introduction to Estrogen Receptor 2 ER immunohistochemistry 3 Quality control 5 Cell lines as controls 6 Estrogen
Product Introduction Product Codes: HCL029, HCL030 and HCL031 Issue 1. 180510 Contents Introduction to Estrogen Receptor 2 ER immunohistochemistry 3 Quality control 5 Cell lines as controls 6 Estrogen
Mass Histology Service
 Mass Histology Service A complete anatomical pathology laboratory www.masshistology.com Telephone: (877) 286-6004 Report on Pathology A Time Course Study of the Local Effects of Intramuscular XXXXXXX Injection
Mass Histology Service A complete anatomical pathology laboratory www.masshistology.com Telephone: (877) 286-6004 Report on Pathology A Time Course Study of the Local Effects of Intramuscular XXXXXXX Injection
Spectrum of Lesions in Cystoscopic Bladder Biopsies -A Histopathological Study
 AJMS Al Ameen J Med Sci (2 012 )5 (2 ):1 3 2-1 3 6 (A US National Library of Medicine enlisted journal) I S S N 0 9 7 4-1 1 4 3 C O D E N : A A J M B G ORIGI NAL ARTICLE Spectrum of Lesions in Cystoscopic
AJMS Al Ameen J Med Sci (2 012 )5 (2 ):1 3 2-1 3 6 (A US National Library of Medicine enlisted journal) I S S N 0 9 7 4-1 1 4 3 C O D E N : A A J M B G ORIGI NAL ARTICLE Spectrum of Lesions in Cystoscopic
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES COPYRIGHTED MATERIAL SECOND EDITION
 VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Urothelial Carcinoma (UC)
") EDUCATION PD-L1 IHC 28-8 pharmdx Interpretation Manual Urothelial Carcinoma (UC) For In Vitro Diagnostic Use Table of Contents Introduction...5 Intended Use in Urothelial Carcinoma...5 How to Use the
EDUCATION PD-L1 IHC 28-8 pharmdx Interpretation Manual Urothelial Carcinoma (UC) For In Vitro Diagnostic Use Table of Contents Introduction...5 Intended Use in Urothelial Carcinoma...5 How to Use the
Molecular Probes Introducing 14 new probes
 Molecular Probes Introducing 14 new probes Gene and Chromosome Probes Dual Colour ISH INFORM HER2 Dual ISH DNA Probe Cocktail Assay Product Part Number INFORM HER2 Dual ISH DNA Probe Cocktail 800-4422
Molecular Probes Introducing 14 new probes Gene and Chromosome Probes Dual Colour ISH INFORM HER2 Dual ISH DNA Probe Cocktail Assay Product Part Number INFORM HER2 Dual ISH DNA Probe Cocktail 800-4422
Enterprise Interest Lecture 9º Personalized Healthcare in Oncology sponsored by Roche, Lisbon 2017 Bladder Diagnostic Advisory Board Invitation
 Enterprise Interest Lecture 9º Personalized Healthcare in Oncology sponsored by Roche, Lisbon 2017 Bladder Diagnostic Advisory Board Invitation sponsored by Astra-Zeneca, London 2017 SPEC-02 ESP/ESMO PD-L1
Enterprise Interest Lecture 9º Personalized Healthcare in Oncology sponsored by Roche, Lisbon 2017 Bladder Diagnostic Advisory Board Invitation sponsored by Astra-Zeneca, London 2017 SPEC-02 ESP/ESMO PD-L1
ANATOMICAL PATHOLOGY TARIFF
 ANATOMICAL PATHOLOGY TARIFF A GUIDE TO UTILISATION. The following guidelines have been agreed by consensus of Anatomical Pathologists who are members of the Anatomical Pathologist s Group, or the National
ANATOMICAL PATHOLOGY TARIFF A GUIDE TO UTILISATION. The following guidelines have been agreed by consensus of Anatomical Pathologists who are members of the Anatomical Pathologist s Group, or the National
Pathologic Assessment of Invasion in TUR Specimens. A. Lopez-Beltran. T1 (ct1)
") Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
, , 2011 HODGKIN LYMPHOMA
 European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
LYMPH GLAND. By : Group 1
 LYMPH GLAND By : Group 1 ANATOMY LYMPH NODE Lymphatic Organs Red bone marrow Thymus gland Lymph nodes Lymph nodules Spleen Primary organs Secondary organs Lymph Nodes Firm, smooth-surfaced, bean-shaped
LYMPH GLAND By : Group 1 ANATOMY LYMPH NODE Lymphatic Organs Red bone marrow Thymus gland Lymph nodes Lymph nodules Spleen Primary organs Secondary organs Lymph Nodes Firm, smooth-surfaced, bean-shaped
Gastric Carcinoma with Lymphoid Stroma: Association with Epstein Virus Genome demonstrated by PCR
 Gastric Carcinoma with Lymphoid Stroma: Association with Epstein Virus Genome demonstrated by PCR Pages with reference to book, From 305 To 307 Irshad N. Soomro,Samina Noorali,Syed Abdul Aziz,Suhail Muzaffar,Shahid
Gastric Carcinoma with Lymphoid Stroma: Association with Epstein Virus Genome demonstrated by PCR Pages with reference to book, From 305 To 307 Irshad N. Soomro,Samina Noorali,Syed Abdul Aziz,Suhail Muzaffar,Shahid
Prostate Immunohistochemistry. Literature Interpretation: Caveats. Must be aware of staining pattern of antibody in the relevant tissue
 IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Product Introduction
 Product Introduction Product Codes: HCL026, HCL027 and HCL028 Contents Introduction to HER2 2 HER2 immunohistochemistry 3 Cell lines as controls 5 HER2 Analyte Control DR IHC 7 HER2 Analyte Control DR
Product Introduction Product Codes: HCL026, HCL027 and HCL028 Contents Introduction to HER2 2 HER2 immunohistochemistry 3 Cell lines as controls 5 HER2 Analyte Control DR IHC 7 HER2 Analyte Control DR
Pancreatobiliary Frozen Section Nightmares
 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
COMPUTER-AIDED HER-2/neu EVALUATION IN EXTERNAL QUALITY ASSURANCE (EQA) OF BREAST CANCER SCREENING PROGRAMME
 OF BREAST CANCER SCREENING PROGRAMME") COMPUTER-AIDED HER-2/neu EVALUATION IN EXTERNAL QUALITY ASSURANCE (EQA) OF BREAST CANCER SCREENING PROGRAMME Maria Lunardi MD Anatomic Pathology Fracastoro Hospital San Bonifacio, Verona -Italy HER2-neu
COMPUTER-AIDED HER-2/neu EVALUATION IN EXTERNAL QUALITY ASSURANCE (EQA) OF BREAST CANCER SCREENING PROGRAMME Maria Lunardi MD Anatomic Pathology Fracastoro Hospital San Bonifacio, Verona -Italy HER2-neu
Urothelial Carcinoma (UC)
") EDUCATION PD-L1 IHC 28-8 pharmdx Interpretation Manual Urothelial Carcinoma (UC) PD-L1 IHC 28-8 pharmdx is FDA-approved for In Vitro Diagnostic Use Table of Contents Introduction...5 Intended Use in Urothelial
EDUCATION PD-L1 IHC 28-8 pharmdx Interpretation Manual Urothelial Carcinoma (UC) PD-L1 IHC 28-8 pharmdx is FDA-approved for In Vitro Diagnostic Use Table of Contents Introduction...5 Intended Use in Urothelial
Neoplasia part I. Dr. Mohsen Dashti. Clinical Medicine & Pathology nd Lecture
 Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Cancer Immunotherapy Patient Forum. for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015
 Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Immune Cell Phenotyping in Solid Tumors using Quantitative Pathology
 Immune Cell Phenotyping in Solid Tumors using Quantitative Pathology James R. Mansfield Director of Quantitative Pathology Applications 2009 PerkinElmer What is Quantitative Pathology? Quantitative Pathology
Immune Cell Phenotyping in Solid Tumors using Quantitative Pathology James R. Mansfield Director of Quantitative Pathology Applications 2009 PerkinElmer What is Quantitative Pathology? Quantitative Pathology
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Biopsy diagnosis of renal tumors. Current applications Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Czech Republic Dealing
Enterprise Interest Nothing to declare Biopsy diagnosis of renal tumors. Current applications Ondřej Hes Department of Pathology Charles University and University Hospital Plzeň Czech Republic Dealing
Assessment Run GATA3
 Assessment Run 44 2015 GATA3 Material The slide to be stained for GATA3 comprised: 1. Tonsil 2. Kidney, 3. Urothelial carcinoma, 4. Breast ductal carcinoma, 5. Colon adenocarcinoma All tissues were fixed
Assessment Run 44 2015 GATA3 Material The slide to be stained for GATA3 comprised: 1. Tonsil 2. Kidney, 3. Urothelial carcinoma, 4. Breast ductal carcinoma, 5. Colon adenocarcinoma All tissues were fixed
Table of Contents. 1. Overview. 2. Interpretation Guide. 3. Staining Gallery Cases Negative for CINtec PLUS
 Staining Atlas Table of Contents 1. Overview 1.1 Introduction 1.2 Role of p16 INK4a 1.3 Role of Ki-67 1.4 Molecular Pathogenesis 1.5 p16 INK4a Expression in Cervical Dysplasia 1.6 The Concept of CINtec
Staining Atlas Table of Contents 1. Overview 1.1 Introduction 1.2 Role of p16 INK4a 1.3 Role of Ki-67 1.4 Molecular Pathogenesis 1.5 p16 INK4a Expression in Cervical Dysplasia 1.6 The Concept of CINtec
Next-Generation Immunohistochemistry: Multiplex tissue imaging with mass cytometry
 Nat Met, April 2014 Nat Med, April 2014 Next-Generation Immunohistochemistry: Multiplex tissue imaging with mass cytometry Journal Club Timo Böge Overview Introduction Conventional Immunohistochemistry
Nat Met, April 2014 Nat Med, April 2014 Next-Generation Immunohistochemistry: Multiplex tissue imaging with mass cytometry Journal Club Timo Böge Overview Introduction Conventional Immunohistochemistry
Dr. dr. Primariadewi R, SpPA(K)
") Curriculum Vitae Dr. dr. Primariadewi R, SpPA(K) Education : Medical Doctor from UKRIDA Doctoral Degree from Faculty of Medicine University of Indonesia Pathologist Specialist and Consultant from Faculty
Curriculum Vitae Dr. dr. Primariadewi R, SpPA(K) Education : Medical Doctor from UKRIDA Doctoral Degree from Faculty of Medicine University of Indonesia Pathologist Specialist and Consultant from Faculty
Immunohistochemical Evaluation of Necrotic Malignant Melanomas
 Anatomic Pathology / EVALUATION OF NECROTIC MALIGNANT MELANOMAS Immunohistochemical Evaluation of Necrotic Malignant Melanomas Daisuke Nonaka, MD, Jordan Laser, MD, Rachel Tucker, HTL(ASCP), and Jonathan
Anatomic Pathology / EVALUATION OF NECROTIC MALIGNANT MELANOMAS Immunohistochemical Evaluation of Necrotic Malignant Melanomas Daisuke Nonaka, MD, Jordan Laser, MD, Rachel Tucker, HTL(ASCP), and Jonathan
PD-L1 IHC 22C3 pharmdx. SK tests for use with Autostainer Link 48 Table of Contents
 PD-L1 IHC 22C3 pharmdx SK006 50 tests for use with Autostainer Link 48 Table of Contents 1 Intended Use... 2 2 Summary and Explanation... 2 2.1 NSCLC... 2 2.2 Gastric or Gastroesophageal Junction (GEJ)
PD-L1 IHC 22C3 pharmdx SK006 50 tests for use with Autostainer Link 48 Table of Contents 1 Intended Use... 2 2 Summary and Explanation... 2 2.1 NSCLC... 2 2.2 Gastric or Gastroesophageal Junction (GEJ)
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Supplementary Online Content
 Supplementary Online Content Rimm DL, Han G, Taube JM, et al. A prospective, multi-institutional, pathologistbased assessment of 4 immunohistochemistry assays for PD-L1 expression in non small cell lung
Supplementary Online Content Rimm DL, Han G, Taube JM, et al. A prospective, multi-institutional, pathologistbased assessment of 4 immunohistochemistry assays for PD-L1 expression in non small cell lung
NSCLC. Harmonization study 1. Lung cancer and other malignancies -PD-L1 assay, QuIP EQA
 Lung cancer and other malignancies -PD-L1 assay, QuIP EQA Korinna Jöhrens Institute for pathology Carl Gustav Cars Universitätsklinikum Dresden, Germany Medical consultant QuIP 11.05.2018 NSCLC Harmonization
Lung cancer and other malignancies -PD-L1 assay, QuIP EQA Korinna Jöhrens Institute for pathology Carl Gustav Cars Universitätsklinikum Dresden, Germany Medical consultant QuIP 11.05.2018 NSCLC Harmonization
Contributions to Anatomic Pathology, over the years
 Contributions to Anatomic Pathology, over the years Anatomic Pathology, part 1 G.B. Morgagni Xavier Bichat Rudolf Wirchow Anatomic Pathology, part 1 Anatomic pathology materials: morphological samples
Contributions to Anatomic Pathology, over the years Anatomic Pathology, part 1 G.B. Morgagni Xavier Bichat Rudolf Wirchow Anatomic Pathology, part 1 Anatomic pathology materials: morphological samples
Bone Marrow Pathology. Part 1. R.S. Riley, M.D., Ph.D.
 Bone Marrow Pathology Part 1 R.S. Riley, M.D., Ph.D. Bone Marrow Pathology Bone marrow basics Red cell diseases White cell diseases Other diseases Bone Marrow Pathology Bone marrow basics Hematopoiesis
Bone Marrow Pathology Part 1 R.S. Riley, M.D., Ph.D. Bone Marrow Pathology Bone marrow basics Red cell diseases White cell diseases Other diseases Bone Marrow Pathology Bone marrow basics Hematopoiesis
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Cerebral Parenchymal Lesions: I. Metastatic Neoplasms
 Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
VENTANA ALK (D5F3) Rabbit Monoclonal Primary Antibody. ALK IHC Biomarker Testing Aiding in patient diagnosis
 Rabbit Monoclonal Primary Antibody. ALK IHC Biomarker Testing Aiding in patient diagnosis") VENTANA (D5F3) Rabbit Monoclonal Primary Antibody IHC Biomarker Testing Aiding in patient diagnosis 2 IHC Biomarker Testing Lung cancer is the leading cause of death Lung cancer is the most prevalent form
VENTANA (D5F3) Rabbit Monoclonal Primary Antibody IHC Biomarker Testing Aiding in patient diagnosis 2 IHC Biomarker Testing Lung cancer is the leading cause of death Lung cancer is the most prevalent form
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Reviewing Immunotherapy for Bladder Carcinoma In Situ
 Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Tracking skin cancers and melanoma at the microscopic level
 Tracking skin cancers and melanoma at the microscopic level Rosalie Elenitsas, M.D. Professor of Dermatology Director of Dermatopathology Hospital of the University of Pennsylvania May 12, 2017 Outline
Tracking skin cancers and melanoma at the microscopic level Rosalie Elenitsas, M.D. Professor of Dermatology Director of Dermatopathology Hospital of the University of Pennsylvania May 12, 2017 Outline
Biomarkers for Cancer Immunotherapy Debate
 Biomarkers for Cancer Immunotherapy Debate Moderator: Maria Karasarides, PhD AstraZeneca Pro: Daniel S. Chen, MD, PhD Genentech Con: Steve Averbuch, MD Bristol-Myers Squibb Biomarkers to Select Patients
Biomarkers for Cancer Immunotherapy Debate Moderator: Maria Karasarides, PhD AstraZeneca Pro: Daniel S. Chen, MD, PhD Genentech Con: Steve Averbuch, MD Bristol-Myers Squibb Biomarkers to Select Patients
Results you can trust
 PRODUCT I NF OR MAT ION pharmdx Results you can trust The first and only FDA-approved PD-L1 test to assess the magnitude of treatment effect on progression-free survival in melanoma patients from OPDIVO
PRODUCT I NF OR MAT ION pharmdx Results you can trust The first and only FDA-approved PD-L1 test to assess the magnitude of treatment effect on progression-free survival in melanoma patients from OPDIVO
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology
 Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology Ugur Ozerdem, M.D. 1 Abstract Background: There is a paradigm shift in breast biopsy philosophy. In
Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology Ugur Ozerdem, M.D. 1 Abstract Background: There is a paradigm shift in breast biopsy philosophy. In
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Large blocks in prostate and bladder pathology
 Large blocks in prostate and bladder pathology Farkas Sükösd Department of Pathology, University of Szeged The history of the large block technique in radical prostatectomy and cystectomy The first large
Large blocks in prostate and bladder pathology Farkas Sükösd Department of Pathology, University of Szeged The history of the large block technique in radical prostatectomy and cystectomy The first large