Pitfalls in Shortness of Breath
|
|
|
- Nancy Montgomery
- 6 years ago
- Views:
Transcription






1 Pitfalls in Shortness of Breath Stuart Swadron, MD FRCPC FACEP Vice-Chair of Education and Program Director Department of Emergency Medicine Los Angeles County-University of Southern California Medical Center Massive Hemoptysis WHERE ARE YOUR FRIENDS?



2 Pitfalls in Shortness of Breath Agenda Tricky Aspirations Pitfalls in Shortness of Breath 1 Crashing Asthmatic Sweaty Can t Talk Tachypneic Tripoding THE LOOK OF DOOM Maximal O 2 (NRB) Inhaled Albuterol Inhaled Atrovent IV Steroids IV Magnesium SC Terbutaline THE KITCHEN SINK Maximal Rx


3 Theophylline Leukotriene Inhibitors Long Acting β2 agonists Heliox (maybe a bit harsh!) BiPAP CPAP THE GARBAGE BIN Not Indicated NON-INVASIVE VENTILATION Too Early Too Late KEEP IT SIMPLE! Etomidate Succinylcholine OPTIONS... Lidocaine Ketamine GO FAST! WHEN TO INTUBATE HOW TO INTUBATE





4 Reason #1 Mucous Plugs STILL TRYING TO DIE? BIG ET TUBE AGGRESSIVE TOILET Reason #2 Dehydration yekaterina yushmanaova 2003 STILL TRYING TO DIE? IV FLUID BOLUS





5 Reason #3 Breath Stacking STILL TRYING TO DIE? Squeeze Chest Low Vent Settings Reason #4 Barotrauma STILL TRYING TO DIE? Chest Tubes



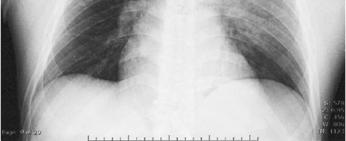
6 1 Disconnect ventilator 2 Squeeze chest 3 Bilateral chest tubes 4 Fluid bolus Asthma Arrest Anesthetic Gases ECMO Summary DISPO TO THE OR! Pitfalls in Shortness of Breath Upright PA View 2 New News on Pneumos Typical Pneumothorax Visceral pleural line No vessels past line Density equal to other lung

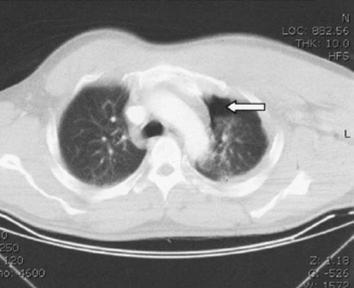


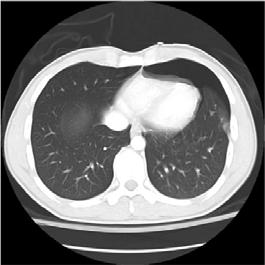
7 Do You See A Pneumothorax? CT Shows Large Pneumothorax The Deep Sulcus Sign CT



8 The Deep Sulcus Sign The Deep Sulcus Sign The Deep Sulcus Sign Sharp Diaphragm Sign


: 541-46 Some")
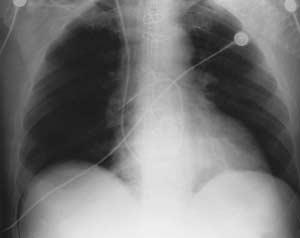
9 Sharp Diaphragm Sign Double Diaphragm Sign 761 patients 103 pneumothoracies 57 were not seen on initial supine AP film! Ball CG et al. Am J Surg 189 (2005): Some Recent Literature Some Recent Literature


10 Pneumothorax in the supine patient Often missed on portable film Seeing vessels out to edges does not rule out Anterior in the lower thorax Signs: Deep sulcus Sharp Diaphragm Double diaphragm Summary I ve learned everything I know by screwing something up - S. Swadron

11 71 o with COPD Exacerbation Assault with a Deadly Weapon Before After Oops! Small (but real!) Septations


12 Before After More Oops! Another Septation Bulla vs. Pneumothorax Bullae are common in asthma and COPD Beware of a pneumothorax with non-anatomic contours Check an old chest x-ray if available Don t be afraid to ask for help! One You Wouldn t Miss Summary



13 Pitfalls in Shortness of Breath 3 NORMAL PNEUMOTHORAX Will Ultrasound be the Answer? The Great Masquerader Syphilis Endocarditis Tuberculosis Lupus Lyme Disease HIV Candidate Diseases Pneumonia? Candidate Diseases


14 57o smoker c cough, CP and SOB x 3d 57o smoker c cough, CP and SOB x 3d Pulmonary Embolus and the CXR Usually an abnormal x-ray but non-specific (e.g. elevated hemidiaphragm) Common abnormalities often attributed to pneumonia or simple atelectasis An infiltrate may be a Hampton s hump! Westermark s sign does exist! Multiple Pulmonary Emboli Summary



15 47o IVDU c SOB and Fever x 1d Multiple Cannonballs When you diagnose pneumonia, briefly consider Pulmonary Embolus Endocarditis Septic Emboli Tuberculosis Diffuse Alveolar Hemorrhage 67o with severe COPD exacerbation Summary
 Pulmonary embolus Lobar collapse D-Dimer BNP Troponin Summary The SOB Blood Panel Causes Of SOB D")

16 In COPD exacerbation, briefly consider Pneumothorax (but beware the bulla!) Pulmonary embolus Lobar collapse D-Dimer BNP Troponin Summary The SOB Blood Panel Causes Of SOB D Dimer BNP Troponin COPD PNA PE ACS CHF Others The Utopian Scenario Will the D-Dimer Save You? False positive with pneumonia/ sepsis COPD increases risk of PE Pitfalls of Biomarkers in SOB
 COPD and CHF frequently co-exist A very low BNP rules out CHF but intermediate values may only raise more")
17 How about the troponin? False positives with severe COPD False positives with PE (e.g. Doesn t indicate ACS) Does predict a poor outcome Pitfalls of Biomarkers in SOB How about the BNP? False positives with severe COPD False positives with PE (2º to right ventricular strain) COPD and CHF frequently co-exist A very low BNP rules out CHF but intermediate values may only raise more questions Pitfalls of Biomarkers in SOB CLINICAL FINDING Initial clinical judgment History Heart failure Myocardial infarction Symptoms Paroxysmal nocturnal dyspnea Edema Physical examination LR LR Chest radiograph Interstitial edema Alveolar edema Cardiomegaly ECG Atrial fibrillation Any abnormal finding BNP alone (pg/ml) Don t throw away your stethoscope Third heart sound Rales Lower-extremity edema Wang CS et al JAMA :1944 Predictors of CHF Pitfalls of Biomarkers in SOB


18 Pitfalls in Shortness of Breath Tricky Aspirations 4 Tricky Aspirations Yikes! Tricky Aspirations Tricky Aspirations Major Hemoptysis Major Chest Tubes Major Pneumothorax One Nail in the Coffin Tracheobronchial Tear




19 Tricky Aspirations Improvement with antibiotics & bronchodilators Tricky Aspirations 17 month old boy, sudden onset coughing Pneumonia seen on the X-ray Negative X-rays Failure to consider in adults Why Do We Miss the Diagnosis? Plain Film Series Tricky Aspirations Tricky Aspirations Right Lateral Decubitus Lateral Neck Plain Film Series Expiratory film Plain Film Series





:353-60 A")


20 Tricky Aspirations Tricky Aspirations Allan JS et al. Chest Surg Clin N Am 13 (2003) A Swallowed Coin in an Adult? Kavanagh et al. Clin Radiol (6): A Swallowed Coin in an Adult? LAC+USC Medical Center LEVEL 1 COCAINE ASPIRATION CENTER

21 Pitfalls in Shortness of Breath Agenda Thank you! 4 Tricky Aspirations
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
DIASTOLOGY DON T BE SUCH A STIFF
 DIASTOLOGY DON T BE SUCH A STIFF Michael Mallin, MD University of Utah Director Emergency Ultrasound www.ultrasoundpodcast.com Warning: The education found within this presentation is not approved by anyone
DIASTOLOGY DON T BE SUCH A STIFF Michael Mallin, MD University of Utah Director Emergency Ultrasound www.ultrasoundpodcast.com Warning: The education found within this presentation is not approved by anyone
For more information about how to cite these materials visit
 Project: Ghana Emergency Medicine Collaborative Document Title: Approach to the Dyspenic Adult Patient Author(s): Randall Ellis, MD MPH (Vanderbilt University) License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: Approach to the Dyspenic Adult Patient Author(s): Randall Ellis, MD MPH (Vanderbilt University) License: Unless otherwise noted, this material
Bronchoconstriction is also treated with medications that inhibit bronchiolar constriction such as: Ipratropium (Atrovent)
") Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis?
. What is the diagnosis?") 1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
HOSPITAL RECORD ABSTRACTION FORM
 HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Author(s): Frank Madore (Hennepin County Medical Center), MD 2012
: Frank Madore (Hennepin County Medical Center), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Objectives. What is a Chest X Ray? CXR Workshop. Definition (diagnostic tool/internal PE) Types. Cost
 Types. Cost") Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Chronic Obstructive Pulmonary Disease
 Scope of Problem Chronic Obstructive Pulmonary Disease Marianne J. Davies, RN, MSN, APRN Yale University School of Medicine Yale Comprehensive Cancer Center Nevada Cancer Institute 2005 Hospitalizations
Scope of Problem Chronic Obstructive Pulmonary Disease Marianne J. Davies, RN, MSN, APRN Yale University School of Medicine Yale Comprehensive Cancer Center Nevada Cancer Institute 2005 Hospitalizations
THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS. 1. Cardiovascular Disease
 THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS 1. Cardiovascular Disease Cardiovascular disease is considered to have developed if there was a definite manifestation
THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS 1. Cardiovascular Disease Cardiovascular disease is considered to have developed if there was a definite manifestation
Introduction to Chest Radiography
 Introduction to Chest Radiography RSTH 366: DIAGNOSTIC TECHNIQUES Alan Alipoon BS, RCP, RRT Instructor Department of Cardiopulmonary Sciences 1 Introduction Discovered in 1895 by Wilhelm Roentgen Terminology
Introduction to Chest Radiography RSTH 366: DIAGNOSTIC TECHNIQUES Alan Alipoon BS, RCP, RRT Instructor Department of Cardiopulmonary Sciences 1 Introduction Discovered in 1895 by Wilhelm Roentgen Terminology
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
Interactive Lecture. Lecture 7 - Interactive. Radiology of cardiorespiratory disease. Editing File. Done By. Color Coding Important Notes Extra
 Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
FAILURE. Matt Beecroft, MD
 FAILURE Matt Beecroft, MD 64 yo male with no real PMH Sitting on couch when sudden onset SOB Says he s been sweaty FIRST PATIENT OF THE WEEKEND HR 131, RR 28, 132/96, 93% RE-EXAM BP 229/130, HR 180s
FAILURE Matt Beecroft, MD 64 yo male with no real PMH Sitting on couch when sudden onset SOB Says he s been sweaty FIRST PATIENT OF THE WEEKEND HR 131, RR 28, 132/96, 93% RE-EXAM BP 229/130, HR 180s
Alexander A Schult, M.D., FCCP. October 21, 2017 Revised 1/10/18
 Alexander A Schult, M.D., FCCP October 21, 2017 Revised 1/10/18 Identifying normal anatomy Identifying various pathologic states Identifying placement of hardware Identifying limitations of portable CXR
Alexander A Schult, M.D., FCCP October 21, 2017 Revised 1/10/18 Identifying normal anatomy Identifying various pathologic states Identifying placement of hardware Identifying limitations of portable CXR
ACUTE HEART FAILURE in the ED. Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia
 ACUTE HEART FAILURE in the ED Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia ACUTE HEART FAILURE 80% Acute Heart Failure Syndrome Sensitivity Specificity
ACUTE HEART FAILURE in the ED Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia ACUTE HEART FAILURE 80% Acute Heart Failure Syndrome Sensitivity Specificity
EMS Subspecialty Certification Review Course
 EMS Subspecialty Certification Review Course 1.3.1 1.3.1.1 Shortness of Breath 1.3.1.1.1 Use of portable non invasive ventilation devices 1.3.1.1.2 Field Identification of COPD 1.3.1.1.3 Assisted Ventilation
EMS Subspecialty Certification Review Course 1.3.1 1.3.1.1 Shortness of Breath 1.3.1.1.1 Use of portable non invasive ventilation devices 1.3.1.1.2 Field Identification of COPD 1.3.1.1.3 Assisted Ventilation
Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous structures - Significant thoracic inj
 PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
Management of Pleural Effusion
 Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient
 Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Children s Hospital Discuss when foreign body aspiration
Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Children s Hospital Discuss when foreign body aspiration
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD)
 Instructions for the Pulmonary Diagnosis Form (PLD)") Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
POCUS for the Internist: Lungs & Pericardial Effusions
 POCUS for the Internist: Lungs & Pericardial Effusions Jeremy S. Boyd, MD, FACEP Asst. Professor of Emergency Medicine Vanderbilt University Medical Illustrations courtesy of Robinson Ferre, MD, FACEP
POCUS for the Internist: Lungs & Pericardial Effusions Jeremy S. Boyd, MD, FACEP Asst. Professor of Emergency Medicine Vanderbilt University Medical Illustrations courtesy of Robinson Ferre, MD, FACEP
Pulmonary Emergencies. Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012
 Pulmonary Emergencies Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012 Learning Objectives Review commonly encountered pulmonary emergencies
Pulmonary Emergencies Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012 Learning Objectives Review commonly encountered pulmonary emergencies
Core Content In Urgent Care Medicine Release Date: December 1, 2009 Review Date: January 31, 2011 Expiration Date: November 30, 2014
 Posttest and CME Instructions To receive a statement of credit for CME you must: 1. Print out the handouts and posttest files prior to reviewing the presentations. You can find the handouts by clicking
Posttest and CME Instructions To receive a statement of credit for CME you must: 1. Print out the handouts and posttest files prior to reviewing the presentations. You can find the handouts by clicking
Palliative Sedation An ICU Perspective. William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC
 Department of Critical Care Thunder Bay Regional HSC") Palliative Sedation An ICU Perspective William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC Conflict Disclosure Information: Presenter: Dr. Will Anderson I have no financial
Palliative Sedation An ICU Perspective William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC Conflict Disclosure Information: Presenter: Dr. Will Anderson I have no financial
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Asthma. No financial relationships with a commercial interest to disclose
 Asthma in the ED Emily Rose, MD FAAP FAAEM FACEP Assistant Professor of Clinical Emergency Medicine Keck School of Medicine of USC LA County + USC Medical Center No financial relationships with a commercial
Asthma in the ED Emily Rose, MD FAAP FAAEM FACEP Assistant Professor of Clinical Emergency Medicine Keck School of Medicine of USC LA County + USC Medical Center No financial relationships with a commercial
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS
 RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
buteykobreathing.co.nz Melanie Kalmanowicz, MD Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center
 buteykobreathing.co.nz Melanie Kalmanowicz, MD Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center PMH: hypertension, hyperlipidemia, asthma, hypothyroidism
buteykobreathing.co.nz Melanie Kalmanowicz, MD Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center PMH: hypertension, hyperlipidemia, asthma, hypothyroidism
A Practical Approach to Ultrasound Assessment of Respiratory Distress
 A Practical Approach to Ultrasound Assessment of Respiratory Distress Yanick Beaulieu, MD, FRCPC Director, Bedside Ultrasound Curriculum Division of Cardiology and Critical Care Hôpital du Sacré-Coeur
A Practical Approach to Ultrasound Assessment of Respiratory Distress Yanick Beaulieu, MD, FRCPC Director, Bedside Ultrasound Curriculum Division of Cardiology and Critical Care Hôpital du Sacré-Coeur
Radiologic Features of The Pulmonary Embolus
 January 2003 Radiologic Features of The Pulmonary Embolus Travis McGlothin HMSIII Mr. J is a 51 y.o. male who presented to the BIDMC ED w/ acute onset of: Lft. Hemiparesis slurred speech mild dyspnea mild
January 2003 Radiologic Features of The Pulmonary Embolus Travis McGlothin HMSIII Mr. J is a 51 y.o. male who presented to the BIDMC ED w/ acute onset of: Lft. Hemiparesis slurred speech mild dyspnea mild
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES
 PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES Robert Harwood, MSA, RRT-NPS Objectives At the end of this presentation the student should be able to: Describe the indications of a chest radiograph.
PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES Robert Harwood, MSA, RRT-NPS Objectives At the end of this presentation the student should be able to: Describe the indications of a chest radiograph.
April 2011 CE. Site code # E The Patient With Heart Failure; CPAP as an Intervention
 April 2011 CE Site code # 107200E-1211 The Patient With Heart Failure; CPAP as an Intervention Prepared by: Lt. Bill Hoover, Medical Officer Wauconda Fire District Reviewed/revised by Sharon Hopkins, RN,
April 2011 CE Site code # 107200E-1211 The Patient With Heart Failure; CPAP as an Intervention Prepared by: Lt. Bill Hoover, Medical Officer Wauconda Fire District Reviewed/revised by Sharon Hopkins, RN,
Jeffrey Tabas, MD. sf g h. Risk Assessment Do we understand risk stratification? Are we limiting radiation /contrast with the PERC rule and D-Dimers?
 Pulmonary Embolism Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital Disclosure No Financial Relationships to Disclose No significant investments
Pulmonary Embolism Update Jeffrey Tabas, MD Professor UCSF School of Medicine Emergency Department San Francisco General Hospital Disclosure No Financial Relationships to Disclose No significant investments
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
Airway Foreign Body in Children
 Joseph E. Dohar, M.D., M.S. Dr. Dohar Financial Disclosures Alcon consultant Incusmed consultant Otonomy consultant OrbiMed consultant Learning Objectives Identify clinical situations that may require
Joseph E. Dohar, M.D., M.S. Dr. Dohar Financial Disclosures Alcon consultant Incusmed consultant Otonomy consultant OrbiMed consultant Learning Objectives Identify clinical situations that may require
Signs in Chest Radiology
 Signs in Chest Radiology Jonathan H. Chung, MD Disclosures No pertinent disclosures Jonathan H. Chung, MD Assistant Professor Institute t of fadvanced d Biomedical Imaging National Jewish Health Denver,
Signs in Chest Radiology Jonathan H. Chung, MD Disclosures No pertinent disclosures Jonathan H. Chung, MD Assistant Professor Institute t of fadvanced d Biomedical Imaging National Jewish Health Denver,
10/17/16. Acute Respiratory Failure in the Acute Care Setting. Margaret Rosales, APRN-CNP, FNP
 Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Chest Radiology: A Systematic Approach. Objectives. Basic Principles 10/2/2014
 Chest Radiology: A Systematic Approach Brian Wetzel ACNP Senior Instructor OHSU School of Medicine Department of Emergency Medicine Objectives A systematic approach to evaluating CXRs Identifying common
Chest Radiology: A Systematic Approach Brian Wetzel ACNP Senior Instructor OHSU School of Medicine Department of Emergency Medicine Objectives A systematic approach to evaluating CXRs Identifying common
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 4/7/2012 Radiology Quiz of the Week # 67 Page 1 CLINICAL PRESENTATION AND RADIOLOGY QUIZ
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 4/7/2012 Radiology Quiz of the Week # 67 Page 1 CLINICAL PRESENTATION AND RADIOLOGY QUIZ
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
The Future of EMS as Revealed through Research. A Window into the Near Future
 The Future of EMS as Revealed through Research A Window into the Near Future Raymond L. Fowler, M.D., FACEP Co-Principal Investigator National Institutes of Health Resuscitation Outcomes Consortium --------------------
The Future of EMS as Revealed through Research A Window into the Near Future Raymond L. Fowler, M.D., FACEP Co-Principal Investigator National Institutes of Health Resuscitation Outcomes Consortium --------------------
Radiology of the respiratory disease
 Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
The diagnosis and management of pneumothorax
 Respiratory 131 The diagnosis and management of pneumothorax Pneumothorax is a relatively common presentation in patients under the age of 40 years (approximately, 85% of patients are younger than 40 years).
Respiratory 131 The diagnosis and management of pneumothorax Pneumothorax is a relatively common presentation in patients under the age of 40 years (approximately, 85% of patients are younger than 40 years).
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
Pulmonary Emergencies. Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs
 Pulmonary Emergencies Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs Pulmonary Surfactant Thin film that coats alveoli Prevents alveoli from
Pulmonary Emergencies Lower Airway Structures Trachea Bronchial tree Primary bronchi Secondary bronchi Bronchioles Alveoli Lungs Pulmonary Surfactant Thin film that coats alveoli Prevents alveoli from
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
And Then There is Failure
 Heart Failure And Then There is Failure Heart Failure Brenda Phipps BSN Nurse Educator Minneapolis VA Tina Wright MSN Clinical Nurse Leader Minneapolis VA Symptoms SOB, use of accessory muscles Crackles,
Heart Failure And Then There is Failure Heart Failure Brenda Phipps BSN Nurse Educator Minneapolis VA Tina Wright MSN Clinical Nurse Leader Minneapolis VA Symptoms SOB, use of accessory muscles Crackles,
Author(s): Rashmi U. Kothari (Michigan State University), MD 2012
: Rashmi U. Kothari (Michigan State University), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Acute Congestive Heart Failure Author(s): Rashmi U. Kothari (Michigan State University), MD 2012 License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: Acute Congestive Heart Failure Author(s): Rashmi U. Kothari (Michigan State University), MD 2012 License: Unless otherwise noted, this material
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
X-rays. Dr Will Dooley
 X-rays Dr Will Dooley Plan Chest X-Rays Abdominal X-Rays Exam approach Presentation skills EMQ EMQ- answers Chest X-Ray - Systematic Approach D R Details RIP Image Quality +/- OBVIOUS ABNORMALITY A B C
X-rays Dr Will Dooley Plan Chest X-Rays Abdominal X-Rays Exam approach Presentation skills EMQ EMQ- answers Chest X-Ray - Systematic Approach D R Details RIP Image Quality +/- OBVIOUS ABNORMALITY A B C
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Interesting Capnography Cases
 Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in