9b From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists (Part 2: Molecular Testing)
|
|
|
- Claud Bryan
- 6 years ago
- Views:
Transcription
1 9b From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists (Part 2: Molecular Testing) Songlin Zhang MD, PhD Mary Lowery-Nordberg MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste Chicago, IL 60603
2 9b From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists (Part 2: Molecular Testing) This presentation will illustrate how to apply molecular testing in cytology specimens. Lesions include lymphoproliferative disorders, soft tissue tumors, and other non-gyn lesions. We will present a discussion of molecular pathology, including basic molecular testing knowledge, how to select the appropriate tests, and how to interpret the molecular test results in conjunction with the cytology findings. The most common molecular tests will be covered. Integrate the various genetic test results with morphologic, clinical, and other relevant laboratory data to arrive at a single interpretation for diagnostic and prognostic purposes. Review how laboratories are using molecular diagnostics, particularly fluorescence in situ hybridization (FISH) technologies and outline key advantages and challenges of oncologic molecular testing relative to more traditional diagnostic methods. Recognize the advantages and limitations of the different testing modalities such that they are able to help physicians to prioritize test requests and eliminate redundant testing. FACULTY: Songlin Zhang MD, PhD Mary Lowery-Nordberg MD Practicing Pathologists Cytopathology Cytopathology (Non-Gynecologic) 1.0 CME/CMLE Credit Accreditation Statement: The American Society for Clinical Pathology (ASCP) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education (CME) for physicians. This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME). Credit Designation: The ASCP designates this enduring material for a maximum of 1 AMA PRA Category 1 Credits. Physicians should only claim credit commensurate with the extent of their participation in the activity. ASCP continuing education activities are accepted by California, Florida, and many other states for relicensure of clinical laboratory personnel. ASCP designates these activities for the indicated number of Continuing Medical Laboratory Education (CMLE) credit hours. ASCP CMLE credit hours are acceptable to meet the continuing education requirements for the ASCP Board of Registry Certification Maintenance Program. All ASCP CMLE programs are conducted at intermediate to advanced levels of learning. Continuing medical education (CME) activities offered by ASCP are acceptable for the American Board of Pathology s Maintenance of Certification Program.
3 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 2 Molecular Pathology Mary Lowery Nordberg, PhD Feist-Weiller Cancer Center LSUHSC-S
4 I have no Conflict of Interest
5 Acknowledgements Questions adapted from: Lefkowitch 2006: Anatomic Pathology Board Review, Saunders Mais and Nordberg, 2008: Quick Compendium of Molecular Pathology, ASCP Press.
6 The corresponding figure shows a karyotype of a CD20, CD10, PAX5 and BCL6 positive lymphoid neoplasm. Which of the following statements about this type of tumor is TRUE? Question 1
7 (A) This tumor harbors a t(14;18)(q32;q21) translocation which causes overexpression of cyclin D1. (B) Polymerase chain reaction (PCR) detects this translocation in a greater proportion of cases than do fluorescence in situ hybridization (FISH) or Southern blotting. (C) Immunostaining for BCL2 in B cells is diagnostic of follicular lymphoma. (D) Overexpression of BCL2 is associated with reduced apoptosis and resistance to chemotherapy. (E) Detection of the BCL2 translocation by PCR is diagnostic of follicular lymphoma.

8 BCL2 protein expression non-diagnostic (although not present in non-neoplastic follicular center cells) Flow cytometry Immunohistochemistry Normal mantle cells B-cells in hyperplastic marginal zones Normal plasma cells T-cells Follicular lymphomas MALT lymphomas Mantle cell lymphomas Lymphocytic leukemias ALL

9 Antiapoptotic


10 BCL2 FISH

11 t(11;14)(q13;q32) BCL1/CCND1 Diagnostic of mantle cell lymphoma
12 Oncogene t(11;14)(q13;q32)

13 PCR for BCL2/IGH Wide variability of BCL2 breakpoints Standard primers for MBR and mbr Detects only 35-65% of cases Can be seen at a low level in some reactive lymphoid proliferations
14 The corresponding figure is a fluorescence in situ hybridization (FISH) image of cells from a CSF sediment stained with probes for 15q22 and 17q21. Which of the following statements is TRUE? Question 2
15 (A)Acute promyelocytic leukemia (APL) is characterized by t(15;17)(q22;q21), which results in a fusion transcript incorporating portions of the PML from chromosome 17 and the gene for retinoic acid receptor alpha (RARalpha) from chromosome 15. (B)APL cases with t(11;17)(q23;q21) (PLZF-RARalpha fusion) are resistant to treatment with retinoic acid derivatives (C) The optimal method for demonstrating these translocations is DNA PCR. (D) Treatment with retinoic acid derivatives consistently results in complete loss of detectable transcript in the blood. (E) Real-time reverse transcription (RT)-PCR is not a reliable method for detecting fusion transcripts.
-")
16 FISH for t(15;17)- Fusion probe

17 All-trans-retinoic acid (ATRA) t(15;17) inhibits PML and RARa function Binds to recruit HDAC to RA response genes Chromatin condensation Maturation arrest ATRA inhibits binding Restores trascription of RAresponsive genes Differentiation
 vs RARA")
18 t(11;17) PLZF-RARA Resistance to treatment with ATRA t(15;17) vs RARA variant
19 RT-PCR for t(15;17) Monitoring for treatment response Minimal residual disease
20 REQUIREMENT OF MOLECULAR CYTOGENETIC STUDIES I. Mandatory for diagnosis CML: BCR-ABL; t(9;22) Burkitt Lymphoma: C-MYC/IgH; t(8;14), t(14;22), t(2;14) AML with AML1/ETO; t(8:21) AML with CBF /MYH11; inv(16) or t(16;16) II. Integral part for treatment and prognosis Anaplastic large cell lymphoma: ALK/NPM; t(2;5) Acute promyelocytic leukemia: PML-RAR t(15;17) III. Definitive diagnosis but not mandatory Mantle cell lymphoma: BCL1/IgH; t(11;14) Lymphoplasmacytic lymphoma: PAX/IgH; t(9;14) Diffuse large cell lymphoma/high grade follicular: BCL6 IV. Prognostic predictor Plasma cell myeloma V. No specific cytogenetic abnormality Natural killer cell lymphoma/leukemia

21 This polyacrylamide gel electrophoresis image shows a clonal control and a polyclonal sample product obtained after PCR with immunoglobulin heavy-chain joining region and framework region 3 primers. Which of the following statements about antigen receptor gene rearrangement analysis for detection of lymphoid clonality is TRUE? Question 3
22 (A) PCR detects a larger proportion of rearrangements than does Southern blotting. (B) Unlike Southern blotting, which can be performed on paraffin-embedded tissue, PCR requires frozen tissue, because formalin inhibits DNA polymerases. (C) PCR is especially sensitive for the detection of clonal rearrangements among follicular lymphomas. (D) Use of PCR- either standard PCR or sequence-specific PCR- to detect residual disease in ALL is complicated by ongoing rearrangements. (E) If a sample fails to show a clonal rearrangement by PCR, then Southern blotting will be of little value.

23 VDJ/VJ rearrangements of antigen receptor genes Normal response for immunologic competency Clonal rearrangements targeted for lymphoid proliferations

24 PCR for clonality (IGH/JH) Somatic hypermutations Deletions Failure of consensus primers to amplify different V families Detects on 50-75% of all rearrangements Good for minimal residual disease
25 Southern blot for B-cell clonality Targets broader region of genome Laborious Requires more tissue Unreliable with paraffin
. Which of the following statements about EGFR and tumors of this type is TRUE? Question 4")
26 Direct epithelial growth factor receptor gene sequencing of paraffin-embedded lung tumor showed a 15-bp, inframe deletion in exon 19 (shown here), which leads to a five amino acid deletion within the catalytic kinase domain of EGFR (dele746- A750). Which of the following statements about EGFR and tumors of this type is TRUE? Question 4
27 (A) Given the function of EGFR- a tyrosine kinase-this is likely to be an inactivating mutation and associated with sensitivity to gefitinib (Iressa), an EGFR inhibitor. (B) This lung tumor is likely to be a small cell carcinoma. (C) The patient from whom this sample was obtained is most likely a smoker. (D) This carcinoma is likely to have an activating k-ras mutation. (E) This lung tumor is most likely an adenocarcinoma, and the patient more likely to be a nonsmoker and female.

28


29 Clinical management and EGFR status


30 Molecularly targeted therapy

31 FISH analysis for EGFR copy number

32 EGFR amplification

33

34

35 This image shows results of MYCN FISH performed on a tumor sample from an 11-month-old child with neuroblastoma metastatic to the liver. An FNA of the lesion shows these cells. Which of the following statements is TRUE? Question 5
36 (A) This tumor is likely to have a hyperdiploid content and to be associated with a poor prognosis. (B) This tumor is likely to show duplication of the short arm of chromosome 1 (1p), which is associated with a poor prognosis. (C) This tumor is likely to express the TrkA neurotrophin receptor, which is associated with a poor prognosis. (D) Amplification of the n-myc gene (MYCN) is not relevant in this case, because the patient has metastatic disease and is therefore a highrisk patient. (E) MYCN amplification defines this patient as having high-risk disease.
37 Neuroblastoma Good prognosis Hyperdiploid DNA content No structural chromosomal abnormalities gains of whole chromosomes Expression of TrkA neutrophin receptor Poor prognosis Diploid DNA content Structural aberrations 1p deletions 11q 17q gain MYCN amplification Survival drops from 93% to 10%

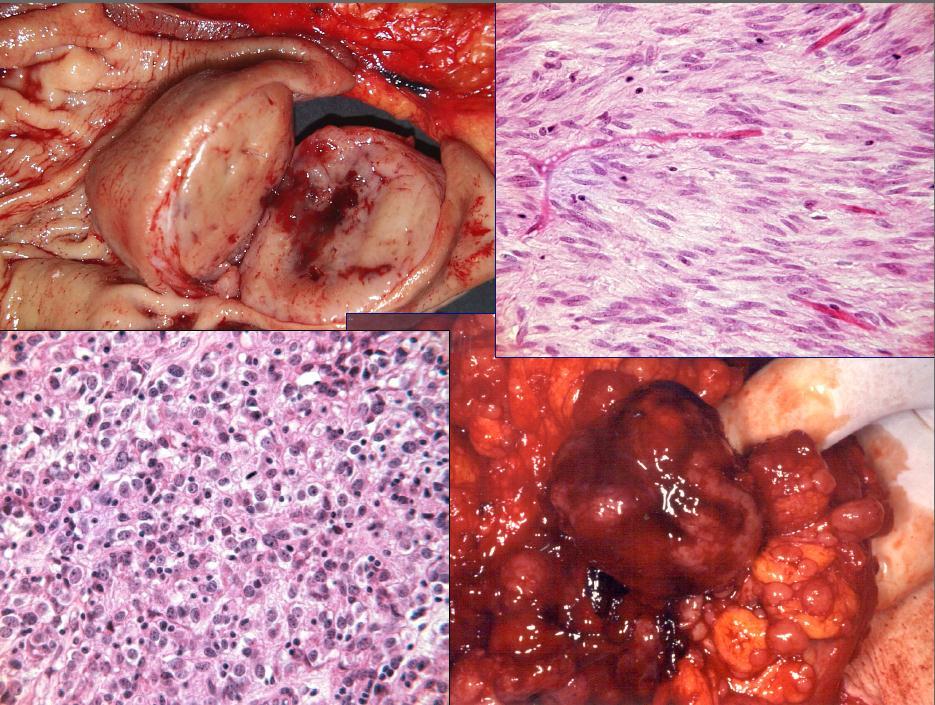
38 This image shows a spindle cell neoplasm in the leg of a 33-year-old woman. The tumor strongly expressed epithelial membrane antigen, BCL2 and CD99, and was focally positive for pancytokeratin. The following statements about this tumor are true EXCEPT: Question 6
39 (A) t(x;18)(p11;q11) is likely to be present in the above tumor. (B) The above translocation results in a fusion encoding a protein incorporating the transactivation domain of SYT encoded on chromosome 18 and the C-terminal portion of SSX1, SSX3, or SSX4 encoded on the X chromosome. (C) Immunohistochemistry for SYT protein, although not diagnostic, can help in the diagnosis of tumors of this type. (D) Cases with the different molecular forms (SYT-SSX1, SYT- SSX2, SYT-SSX4) appear identical by classic karyotyping and by FISH. (E) SYT-SSX2 is rarely seen in biphasic tumors of this type (tumors with distinct gland formation), and might be associated with a better prognosis.

40 18q/SYT- Xp/SSX

41 SYT-SSX

42 FISH Technology

43 This lesion was seen in the cecum of a 40-year-old man who underwent screening colonoscopy because of endometrial carcinoma in a 43- year-old sister. His mother had a history of a pelvic cancer in her 40s, for which she had a total abdominal hysterectomy with bilateral salpingooophorectomy. Immunohistochemistry of the lesion showed complete loss of expression of MSH2 and very weak expression of MSH6. This lesion is LIKELY to: Question 7
44 (A) Exhibit microsatellite instability (MSI) (B) Be associated with a germline mutation in MSH2 (C) Be associated with normal germline MSH6 (D) Be associated with impaired mismatch repair (E) All of the above
45
46

47
48

49

50

51

52 MLH

53

54

55
 translocation (C).")
56 Karyotyping of a renal cortical tumor (A and B) from a 61-year-old man demonstrated a t(x;1) (p11.2;q23) translocation (C). The following statements about tumors of this type are true EXCEPT: Question 8
57 Renal cortical tumors Children and adolescents T(X;1) Xp11.2 ASPL-TFE3 fusion product can be seen in alveolar soft part sarcoma
58 (A) They are more common in older individuals. (B) They may show positive immunohistochemical staining for TFE3 protein. (C) They may contain papillary and solid areas with clear and eosinophilic cells. (D) They stain variably with antibodies to cytokeratin. (E) They share molecular similarities with alveolar soft part sarcoma.
 showed a t(11;22)(q24;q12), which was confirmed by FISH (C).")
59 This small round blue cell tumor (A) in the chest wall of a 14-year-old child showed strong immunohistochemical staining for CD99 and Fli-1, and was negative for desmin, smooth muscle actin, HHF-35, cytokeratin, CD45, CD3, CD20, MyoD1, myogenin, S-100, WT1 and epithelial membrane antigen. Classic cytogenetics (B) showed a t(11;22)(q24;q12), which was confirmed by FISH (C). Which of the following statements is FALSE? Question 9
60 (A) This tumor belongs to the Ewing s sarcoma/primitive neuroectodermal tumor (ES/PNET) family. (B) RT-PCR can be performed on paraffin-embedded tissue, and in this tumor would be likely to demonstrate an EWS-FLI1 fusion (C) When cytogenetics cannot be performed, a negative result for the EWS-FLI1 and EWS-ERG, using a properly designed RT-PCR assay to include all EWS-FLI1 fusion variants, rules out a diagnosis of ES/PNET. (D) Demonstration of split signals with a break-apart EWS probe would have strong evidence in favor of a diagnosis of ES/PNET in this case, had karyotyping been unsuccessful. (E) In addition to ES/PNET, other tumors with fusion transcripts involving the EWS gene include clear cell sarcoma ( malignant melanoma ) of soft parts, desmoplastic small round cell tumors, extraskeletal myxoid chrondrosarcoma and, rarely, myxoid liposarcoma.

61


62

63
 (q35;q14).")
64 This tumor from the leg of an 8-year-old girl was positive for HHF-35, MyoD1 and myogenin. The tumor was negative for cytokeratin, CD45, S-100 and epithelial membrane antigen. Classic cytogenetics showed a t(2;13) (q35;q14). The following are true EXCEPT: Question 10

65

66 The following statements about BCR-ABL translocations are true EXCEPT: Question 11
67 (A) They may be seen in chronic myelocytic leukemia (CML), during a blast crisis, and de novo (ALL). (B) The 190-kilodalton fusion protein, resulting from a translocation within the minor cluster region of BCR, is most often associated with ALL. (C) The oncogenic properties of the fusion protein are the result of constitutive activation of the serine-threonine kinase activity of BCR. (D) Imatinib mesylate, which inhibits ABL kinase activity, is a specific treatment for chronic myelogenous leukemia. (E) The BCR-ABL transcript continues to be detectable by RT-PCR in most patients on imatinib treatment.


68 Amplification of HER 2/ Neu in breast cancer: Question 12
69 (A) Correlates with increased estrogen and/or progesterone (ER/PR) receptor expression (B) Is not an independent predictor of prognosis, because it is related to ER/PR expression (C) Is best detected by immunohistochemistry using the Herceptest kit (D) Results in increased HER2 protein expression, which helps tumors overcome the blocking effect of trastuzumab (Herceptin ), and causes resistance to this form of therapy. (E) Is associated with response to treatment with trastuzumab, but this response is blunted or lost in tumors that lose PTEN expression.
 are true")
70 Question 13 The following statements about KIT and PDGFRA mutations in gastrointestinal stromal tumors (GISTs) are true EXCEPT:
71 (A) GISTs characteristically contain mutations of exons 9, 11, 13 or 17 of c-kit, or exon 12 or 18 of PDGFRA. (B) These mutations cause constitutive activation of the KIT or platelet-derived growth factor receptor alpha (PDGFRA) tyrosine kinases, produced by the above genes. (C) Tumors with PDGFRA mutations tend to be negative for KIT expression by immunohistochemistry. (D) Studies have shown a correlation between specific c-kit and PDGFRA mutations and response to therapy with the tyrosine kinase inhibitor imatinib (Gleevec ). (E) KIT mutations identify GIST as high risk or malignant.

72
73
74
75
76

77
78
 and/or MSI are true EXCEPT: Question")
79 The following statements regarding hereditary nonpolyposis colon cancer (HNPCC) and/or MSI are true EXCEPT: Question 14
80 (A) HNPCC has been associated with mutations in MLH1, MSH2, MSH6, PMS1 and MLH3 genes. (B) According to the modified Bethesda criteria, MSI testing should be performed in carcinomas occurring before the age of 50. (C) HNPCC is associated with a high frequency of somatic mutations of the BRAF gene (D) Other tumors in the spectrum of HNPCC include endometrial carcinoma, urothelial carcinoma, and carcinoma of the small intestine, stomach and hepatobiliary ducts. (E) High MSI in colon cancers is associated with a reduced likelihood of metastatic disease, and better overall survival.
81 Which of the following statements about FISH, using the Urovysion assay to detect bladder cancer, is TRUE? Question 15
82 (A) FISH is more specific but less sensitive than cytologic examination. (B) Loss of at least one copy of any two of chromosomes 3, 7 or 17 identified by centromeric probes, and amplification of chromosome 9p21 with a sequence-specific probe, are the most important markers of urothelial carcinoma. (C) The probe set is chosen to evaluate for polysomy of chromosome 3, 7 and 17, and/or homozygous loss of 9p21. (D) Evaluation of 100 successive cells is more sensitive than evaluating 25 morphologically abnormal cells. (E) Papillary urothelial carcinoma is more likely to be FISH positive than is carcinoma in situ.




83 UroVysion (p16 gene)

84



85 Normal Cell Malignant Cell
(q35;q14).")
86 This tumor from the leg of an 8-year-old girl was positive for HHF-35, MyoD1, and myogenin. This tumor was negative for cytokeratin, CD45, S- 100 and epithelial membrane antigen. Classic cytogenetics showed a t(2;13)(q35;q14). The following are true EXCEPT: Question 16
87 (A)This tumor is an alveolar rhabdomyosarcoma (ARMS). (B)RT-PCR is likely to show a fusion transcript involving the 5 portion of PAX3 and the 3 portion of FOXOA1 (FKHR). (C)A more common translocation in alveolar rhabdomyosarcoma is t(1;13) (p36;q14), which results in a PAX7- FOXOA1 fusion. (D)This transcript is associated with a higher rate of bone marrow involvement than the PAX7-FOXOA1 transcript. (E)The PAX7-FOXOA1 translocation is more likely to be amplified as double minutes (dmin).

88 Which of the following statements about gene expression analysis of lymphomas using microarrays is/are TRUE? Question 17
89 (A) Gene expression analysis of diffuse large B-cell lymphomas using cdna microarrays differentiates a germinal center B cell-like group with a good prognosis, an activated B cell-like group with a poor prognosis and a third, heterogeneous, group with a poor prognosis. (B) Immunohistochemistry with CD10, BCL6 and MUM1 can approximate this separation into germinal center-like and nongerminal center-like groups. (C) The prognosis of follicular lymphomas is related to gene expression patterns of non-neoplastic cells in the microenvironment. (D) It has demonstrated a unique gene expression pattern in primary mediastinal B-cell lymphoma, distinct from that of other diffuse large B-cell lymphomas. (E) All of the above.
90 Which of the following statements about genetic alterations in thyroid neoplasms is/are TRUE? Question 18
91 (A) RET/PTC translocations are common among papillary thyroid carcinomas seen in younger individuals, and in those following radiation exposure. (B) BRAF mutations occur more commonly in papillary thyroid carcinomas in older individuals, and are associated with an increased likelihood of late-stage disease and anaplastic carcinoma. (C) BRAF mutations, RAS mutations and RET/PTC rearrangements rarely occur together in papillary thyroid carcinoma. (D) PAX8-PPARgamma translocations are frequent in follicular thyroid carcinomas and less frequent in follicular adenomas. (E) All of the above.
92 When performing tests on RNA from paraffinembedded tissue, which one of the following factors should be considered? Question 19
93 (A) The amount of RNA retrieved depends on the type of fixative used, time prior to fixation and duration of fixation. (B) The larger the amplicon, the greater the likelihood of successful amplification. (C) Formalin is a better fixative for RNA preservation than is ethanol. (D) RNA integrity in routinely processed, paraffin-embedded tissue is best assessed by gel electrophoresis to determine the ratio of 18S and 28S rrna. (E) RNA extraction from paraffin-embedded tissue is fiction.
94 Which of the following statements about gliomas is TRUE? Question 20
95 (A)Oligodendrogliomas are characterized by the loss of the short arm of chromosome 1 (1p) and the long arm of chromosome 19 (19q) in the majority of cases. (B)Oligodendrogliomas are characterized by the loss of the long arm of chromosome 1 (1q) and the short arm of chromosome 19 (19p) in the majority of the cases. (C)LOH at chromosome 1 is associated with resistance to chemotherapy. (D)Activating mutations in the ATP binding region of EGFR are common in gliomas and are associated with increased sensitivity to gefitinib. (E)Loss of expression of methylguanine methyltransferase (MGMT) is associated with resistance to chemotherapy.
96 Which of the following statements about controls for PCR or RT-PCR is FALSE? Question 21
97 (A) When setting up a PCR, one should always add template to the no DNA control first, to avoid accidentally contaminating it. (B) When setting up a PCR, one should add template to test samples first, followed by the positive control and the negative/no DNA controls. (C)When setting up a RT-PCR, in addition to a no template (no RNA control) one should set up a no RT control for each RNA sample being tested. (D) When setting up a PCR following a RT reaction, one should set up a separate no template control, in addition to the product of the no RNA RT reaction. (E) RT-PCR can be performed in a single tube.
98 A thyroid tumor from a 9- year-old girl shows an insular growth pattern, and is immunoreactive for thyroid transcription factor 1 (TTF-1), carcinoembryonic antigen and chromogranin. There is no history of thyroid cancer in the family. Which of the following statements is TRUE? Question 22
99 (A)This patient is likely to harbor an inactivating germline mutation of the RET tumor suppressor gene. (B)The majority of patients with this type of tumor, even in the absence of a family history, have a germline activating mutation of the RET protooncogene. (C)A significant proportion of tumors of this type harbor a translocation involving the RET protooncogene (PTC1, PTC2 or PTC3). (D)Activating somatic mutations of the RET protooncogene may be seen in at least 25-35% of sporadic cases of this tumor type, and may be associated with an increased likelihood of recurrence. (E)Germline testing for RET mutations is not indicated in this patient, in the absence of a family history.
100 Which of the following statements about loss of imprinting (LOI) of IGF2 in Wilms tumor is TRUE? Question 23
101 (A)IGF2 LOI is more common in older children with Wilms tumors. (B)IGF2 LOI is seen predominantly in perilobar nephrogenic rest-like tumors. (C)IGF2 LOI is present in Wilms tumors that develop in Beckwith-Weidemann syndrome (BWS). (D)IGF2 LOI is absent in tumors with LOH of 11p15 or WT1 mutations. (E)All of the above.
102 Question 24 Pheochromocytoma is associated with germline mutations in:
103 (A)RET proto-oncogene (B)Neurofibromin (C)VHL (D)Succinate dehydrogenase subunit D (E)All of the above.
104 Which of the following statements about alterations of tumor suppressor genes and oncogenes in cancers is TRUE? Question 25
105 (A)Oncogenic mutations of tumor suppressor genes invariably occur at hot spots, allowing one to test only for specific mutations. (B)Because cancer-associated mutations of tumor suppressor genes involve loss of function, they can occur throughout the gene, and never involve hot spots. (C)Activating mutations of receptor tyrosine kinases occur at a limited number of sites. (D)Direct sequencing of the entire coding region of a tumor suppressor gene should detect all significant alterations-barring technical error. (E)Tests for hypermethylation of tumor suppressor gene promoters require pure tumor, and can be performed only on microdissected samples.
106 Which of the following statements about fibroblast growth factor receptor 3 (FGFR3) and p53 (TP53) mutations in bladder cancer is TRUE? Question 26
107 (A)FGFR3 mutations act synergistically with p53 mutations in aggressive bladder cancer. (B)FGFR3 and p53 mutations are independent markers of poor prognosis in bladder cancer. (C)Both FGFR3 and p53 mutations are associated with a poor prognosis, but are not independent predictors of prognosis. (D)FGFR3 and p53 mutations are almost mutually exclusive, and are both associated with high-grade bladder cancer. (E)FGFR3 mutations are more common in low grade and low-stage urothelial carcinomas with a low rate of grade and stage progression.
108 Which of the following statements about gene expression profiling of node-negative, tamoxifentreated breast cancer are TRUE? Question 27
109 (A)A recurrence score based on the normalized quantitative expression of 16 genes predicts longterm distant recurrence-free survival. (B)The test requires frozen tissue, as quantitative analysis of RNA from paraffin-embedded tissue is unreliable. (C)Elevated expression of genes involved in the ER signaling pathway is associated with an increased likelihood of recurrence. (D)HER2 expression is not used in this profile, as it requires evaluation of gene amplification using DNA. (E)Elevated expression of genes involved in proliferation is associated with a reduced likelihood of recurrence.
110 Which of the following associations of tumor/genetic alteration is TRUE? Question 28
111 (A)t(17;22), COL1A1-PDGFB with dermatofibrosaroma protuberans, giant cell fibroblastoma and Bednar tumor (B)t(12;15)(p13;q25), ETV6-NTRK3 with infantile fibrosarcoma and cellular congenital mesoblastic nephroma (C)t(X;17)(q11.2;q25), ASPL-TFE3 with alveolar soft part sarcoma (D)t(7;17)(p15;q21), JAZF1-JJAF1 with endometrial stromal sarcoma (E)All of the above.
Nucleic Acid Testing - Oncology. Molecular Diagnosis. Gain/Loss of Nucleic Acid. Objectives. MYCN and Neuroblastoma. Molecular Diagnosis
 Nucleic Acid Testing - Oncology Molecular Diagnosis Nucleic acid based testing in Oncology Gross alterations in DNA content of tumors (ploidy) Gain/Loss of nucleic acids Markers of Clonality Oncogene/Tumor
Nucleic Acid Testing - Oncology Molecular Diagnosis Nucleic acid based testing in Oncology Gross alterations in DNA content of tumors (ploidy) Gain/Loss of nucleic acids Markers of Clonality Oncogene/Tumor
Molecular Diagnosis. Nucleic acid based testing in Oncology
 Molecular Diagnosis Nucleic acid based testing in Oncology Objectives Describe uses of NAT in Oncology Diagnosis, Prediction, monitoring. Genetics Screening, presymptomatic testing, diagnostic testing,
Molecular Diagnosis Nucleic acid based testing in Oncology Objectives Describe uses of NAT in Oncology Diagnosis, Prediction, monitoring. Genetics Screening, presymptomatic testing, diagnostic testing,
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Current and future applications of Molecular Pathology. Kathy Walsh Clinical Scientist NHS Lothian
 Current and future applications of Molecular Pathology Kathy Walsh Clinical Scientist NHS Lothian Molecular Pathology in Solid tumours Cancer type Genes tested Purpose Associated treatments Non small cell
Current and future applications of Molecular Pathology Kathy Walsh Clinical Scientist NHS Lothian Molecular Pathology in Solid tumours Cancer type Genes tested Purpose Associated treatments Non small cell
GENETIC MARKERS IN LYMPHOMA a practical overview. P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute
 GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
Klinisch belang van chromosomale translocatie detectie in sarcomen
 Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
American Society of Cytopathology Core Curriculum in Molecular Biology
 American Society of Cytopathology Core Curriculum in Molecular Biology American Society of Cytopathology Core Curriculum in Molecular Biology Chapter 1 Molecular Basis of Cancer Molecular Oncology Keisha
American Society of Cytopathology Core Curriculum in Molecular Biology American Society of Cytopathology Core Curriculum in Molecular Biology Chapter 1 Molecular Basis of Cancer Molecular Oncology Keisha
Your single-source laboratory solution. FISH Probe Library
 Your single-source laboratory solution. FISH Probe Library Alphabetical List by Probe with Clinical Indication Probe Clinical Indication 1p36 (TP73)/19q13 (GLTSCR) 1q21 (CKS1B) 5q (CSF1R/RPS14) 7q (MDFIC)
Your single-source laboratory solution. FISH Probe Library Alphabetical List by Probe with Clinical Indication Probe Clinical Indication 1p36 (TP73)/19q13 (GLTSCR) 1q21 (CKS1B) 5q (CSF1R/RPS14) 7q (MDFIC)
Molecular Hematopathology Leukemias I. January 14, 2005
 Molecular Hematopathology Leukemias I January 14, 2005 Chronic Myelogenous Leukemia Diagnosis requires presence of Philadelphia chromosome t(9;22)(q34;q11) translocation BCR-ABL is the result BCR on chr
Molecular Hematopathology Leukemias I January 14, 2005 Chronic Myelogenous Leukemia Diagnosis requires presence of Philadelphia chromosome t(9;22)(q34;q11) translocation BCR-ABL is the result BCR on chr
Objectives. Morphology and IHC. Flow and Cyto FISH. Testing for Heme Malignancies 3/20/2013
 Molecular Markers in Hematologic Malignancy: Ways to locate the needle in the haystack. Objectives Review the types of testing for hematologic malignancies Understand rationale for molecular testing Marcie
Molecular Markers in Hematologic Malignancy: Ways to locate the needle in the haystack. Objectives Review the types of testing for hematologic malignancies Understand rationale for molecular testing Marcie
Neoplasia 2018 lecture 11. Dr H Awad FRCPath
 Neoplasia 2018 lecture 11 Dr H Awad FRCPath Clinical aspects of neoplasia Tumors affect patients by: 1. their location 2. hormonal secretions 3. paraneoplastic syndromes 4. cachexia Tumor location Even
Neoplasia 2018 lecture 11 Dr H Awad FRCPath Clinical aspects of neoplasia Tumors affect patients by: 1. their location 2. hormonal secretions 3. paraneoplastic syndromes 4. cachexia Tumor location Even
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Activation of cellular proto-oncogenes to oncogenes. How was active Ras identified?
 Dominant Acting Oncogenes Eugene E. Marcantonio, M.D. Ph.D. Oncogenes are altered forms of normal cellular genes called proto-oncogenes that are involved in pathways regulating cell growth, differentiation,
Dominant Acting Oncogenes Eugene E. Marcantonio, M.D. Ph.D. Oncogenes are altered forms of normal cellular genes called proto-oncogenes that are involved in pathways regulating cell growth, differentiation,
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
ACMG/CAP Cytogenetics CY
 www.cap.org Cytogenetics Analytes/procedures in bold type are regulated for proficiency testing by the Centers for Medicare & Medicaid Services ACMG/CAP Cytogenetics CY Analyte CY Challenges per Shipment
www.cap.org Cytogenetics Analytes/procedures in bold type are regulated for proficiency testing by the Centers for Medicare & Medicaid Services ACMG/CAP Cytogenetics CY Analyte CY Challenges per Shipment
Test Name Results Units Bio. Ref. Interval. Positive
 LL - LL-ROHINI (NATIONAL REFERENCE 135091534 Age 36 Years Gender Female 1/9/2017 120000AM 1/9/2017 105316AM 2/9/2017 104147AM Ref By Final LEUKEMIA GENETIC ROFILE ANY SIX MARKERS, CR QUALITATIVE AML ETO
LL - LL-ROHINI (NATIONAL REFERENCE 135091534 Age 36 Years Gender Female 1/9/2017 120000AM 1/9/2017 105316AM 2/9/2017 104147AM Ref By Final LEUKEMIA GENETIC ROFILE ANY SIX MARKERS, CR QUALITATIVE AML ETO
Role of FISH in Hematological Cancers
 Role of FISH in Hematological Cancers Thomas S.K. Wan PhD,FRCPath,FFSc(RCPA) Honorary Professor, Department of Pathology & Clinical Biochemistry, Queen Mary Hospital, University of Hong Kong. e-mail: wantsk@hku.hk
Role of FISH in Hematological Cancers Thomas S.K. Wan PhD,FRCPath,FFSc(RCPA) Honorary Professor, Department of Pathology & Clinical Biochemistry, Queen Mary Hospital, University of Hong Kong. e-mail: wantsk@hku.hk
Mohammed El-Khateeb. Tumor Genetics. MGL-12 July 21 st 2013 台大農藝系遺傳學 Chapter 22 slide 1
 Mohammed El-Khateeb Tumor Genetics MGL-12 July 21 st 2013 台大農藝系遺傳學 601 20000 Chapter 22 slide 1 Cellular Basis of Cancer Cancer is a collection of diseases characterized by abnormal and uncontrolled growth
Mohammed El-Khateeb Tumor Genetics MGL-12 July 21 st 2013 台大農藝系遺傳學 601 20000 Chapter 22 slide 1 Cellular Basis of Cancer Cancer is a collection of diseases characterized by abnormal and uncontrolled growth
oncogenes-and- tumour-suppressor-genes)
") Special topics in tumor biochemistry oncogenes-and- tumour-suppressor-genes) Speaker: Prof. Jiunn-Jye Chuu E-Mail: jjchuu@mail.stust.edu.tw Genetic Basis of Cancer Cancer-causing mutations Disease of aging
Special topics in tumor biochemistry oncogenes-and- tumour-suppressor-genes) Speaker: Prof. Jiunn-Jye Chuu E-Mail: jjchuu@mail.stust.edu.tw Genetic Basis of Cancer Cancer-causing mutations Disease of aging
Chapter 4 Cellular Oncogenes ~ 4.6 -
 Chapter 4 Cellular Oncogenes - 4.2 ~ 4.6 - Many retroviruses carrying oncogenes have been found in chickens and mice However, attempts undertaken during the 1970s to isolate viruses from most types of
Chapter 4 Cellular Oncogenes - 4.2 ~ 4.6 - Many retroviruses carrying oncogenes have been found in chickens and mice However, attempts undertaken during the 1970s to isolate viruses from most types of
Molecular. Oncology & Pathology. Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine. Liquid Biopsy.
 Molecular Oncology & Pathology Hereditary Cancer Somatic Cancer Liquid Biopsy Next-Gen Sequencing qpcr Sanger Sequencing Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine
Molecular Oncology & Pathology Hereditary Cancer Somatic Cancer Liquid Biopsy Next-Gen Sequencing qpcr Sanger Sequencing Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine
TARGETED THERAPY FOR CHILDHOOD CANCERS
 TARGETED THERAPY FOR CHILDHOOD CANCERS AZIZA SHAD, MD AMEY DISTINGUISHED PROFESSOR OF PEDIATRIC HEMATOLOGY ONCOLOGY, BLOOD AND MARROW TRANSPLANTATION LOMBARDI CANCER CENTER GEORGETOWN UNIVERSITY HOSPITAL
TARGETED THERAPY FOR CHILDHOOD CANCERS AZIZA SHAD, MD AMEY DISTINGUISHED PROFESSOR OF PEDIATRIC HEMATOLOGY ONCOLOGY, BLOOD AND MARROW TRANSPLANTATION LOMBARDI CANCER CENTER GEORGETOWN UNIVERSITY HOSPITAL
Out-Patient Billing CPT Codes
 Out-Patient Billing CPT Codes Updated Date: August 3, 08 Client Billed Molecular Tests HPV DNA Tissue Testing 8764 No Medicare Billed - Molecular Tests NeoARRAY NeoARRAY SNP/Cytogenetic No 89 NeoLAB NeoLAB
Out-Patient Billing CPT Codes Updated Date: August 3, 08 Client Billed Molecular Tests HPV DNA Tissue Testing 8764 No Medicare Billed - Molecular Tests NeoARRAY NeoARRAY SNP/Cytogenetic No 89 NeoLAB NeoLAB
Mohammed El-Khateeb. Tumor Genetics. MGL-12 May 13 th Chapter 22 slide 1 台大農藝系遺傳學
 Mohammed El-Khateeb Tumor Genetics MGL-12 May 13 th 2014 台大農藝系遺傳學 601 20000 Chapter 22 slide 1 Cancer Genetics Types of Genetic Alterations in Cancer Evidence that Mutations Cause Cancer Multistage Model
Mohammed El-Khateeb Tumor Genetics MGL-12 May 13 th 2014 台大農藝系遺傳學 601 20000 Chapter 22 slide 1 Cancer Genetics Types of Genetic Alterations in Cancer Evidence that Mutations Cause Cancer Multistage Model
Test Bank for Robbins and Cotran Pathologic Basis of Disease 9th Edition by Kumar
 Link full download:https://getbooksolutions.com/download/test-bank-for-robbinsand-cotran-pathologic-basis-of-disease-9th-edition-by-kumar Test Bank for Robbins and Cotran Pathologic Basis of Disease 9th
Link full download:https://getbooksolutions.com/download/test-bank-for-robbinsand-cotran-pathologic-basis-of-disease-9th-edition-by-kumar Test Bank for Robbins and Cotran Pathologic Basis of Disease 9th
Test Bank for Robbins and Cotran Pathologic Basis of Disease 9th Edition by Kumar
 Link full download: http://testbankair.com/download/test-bank-for-robbins-cotran-pathologic-basis-of-disease-9th-edition-bykumar-abbas-and-aster Test Bank for Robbins and Cotran Pathologic Basis of Disease
Link full download: http://testbankair.com/download/test-bank-for-robbins-cotran-pathologic-basis-of-disease-9th-edition-bykumar-abbas-and-aster Test Bank for Robbins and Cotran Pathologic Basis of Disease
TEST MENU TEST CPT CODES TAT. Chromosome Analysis Bone Marrow x 2, 88264, x 3, Days
 TEST MENU CANCER/LEUKEMIA CHROMOSOME ANALYSIS Chromosome Analysis Bone Marrow 88237 x 2, 88264, 88280 x 3, 88291 4 Days Chromosome Analysis Bone Marrow Core 88237 x 2, 88264, 88280 x 3, 88291 4 Days Chromosome
TEST MENU CANCER/LEUKEMIA CHROMOSOME ANALYSIS Chromosome Analysis Bone Marrow 88237 x 2, 88264, 88280 x 3, 88291 4 Days Chromosome Analysis Bone Marrow Core 88237 x 2, 88264, 88280 x 3, 88291 4 Days Chromosome
Bihong Zhao, M.D, Ph.D Department of Pathology
 Bihong Zhao, M.D, Ph.D Department of Pathology 04-28-2009 Is tumor self or non-self? How are tumor antigens generated? What are they? How does immune system respond? Introduction Tumor Antigens/Categories
Bihong Zhao, M.D, Ph.D Department of Pathology 04-28-2009 Is tumor self or non-self? How are tumor antigens generated? What are they? How does immune system respond? Introduction Tumor Antigens/Categories
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Molecular Genetics of Paediatric Tumours. Gino Somers MBBS, BMedSci, PhD, FRCPA Pathologist-in-Chief Hospital for Sick Children, Toronto, ON, CANADA
 Molecular Genetics of Paediatric Tumours Gino Somers MBBS, BMedSci, PhD, FRCPA Pathologist-in-Chief Hospital for Sick Children, Toronto, ON, CANADA Financial Disclosure NanoString - conference costs for
Molecular Genetics of Paediatric Tumours Gino Somers MBBS, BMedSci, PhD, FRCPA Pathologist-in-Chief Hospital for Sick Children, Toronto, ON, CANADA Financial Disclosure NanoString - conference costs for
Oncology Cytogenetics Diagnostic Service - User Guide 2014
 Oncology Cytogenetics Diagnostic Service - User Guide 2014 Contact details Address: Cytogenetics Department 5 th Floor Tower Wing Guy s Hospital Great Maze Pond London SE1 9RT General enquiries 0207 188
Oncology Cytogenetics Diagnostic Service - User Guide 2014 Contact details Address: Cytogenetics Department 5 th Floor Tower Wing Guy s Hospital Great Maze Pond London SE1 9RT General enquiries 0207 188
Significance of Chromosome Changes in Hematological Disorders and Solid Tumors
 Significance of Chromosome Changes in Hematological Disorders and Solid Tumors Size of Components of Human Genome Size of haploid genome 3.3 X 10 9 DNA basepairs Estimated genetic constitution 30,000
Significance of Chromosome Changes in Hematological Disorders and Solid Tumors Size of Components of Human Genome Size of haploid genome 3.3 X 10 9 DNA basepairs Estimated genetic constitution 30,000
Significance of Chromosome Changes in Hematological Disorders and Solid Tumors
 Significance of Chromosome Changes in Hematological Disorders and Solid Tumors Size of Components of Human Genome Size of haploid genome! Estimated genetic constitution! Size of average chromosome
Significance of Chromosome Changes in Hematological Disorders and Solid Tumors Size of Components of Human Genome Size of haploid genome! Estimated genetic constitution! Size of average chromosome
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Cancer Genetics. What is Cancer? Cancer Classification. Medical Genetics. Uncontrolled growth of cells. Not all tumors are cancerous
 Session8 Medical Genetics Cancer Genetics J avad Jamshidi F a s a U n i v e r s i t y o f M e d i c a l S c i e n c e s, N o v e m b e r 2 0 1 7 What is Cancer? Uncontrolled growth of cells Not all tumors
Session8 Medical Genetics Cancer Genetics J avad Jamshidi F a s a U n i v e r s i t y o f M e d i c a l S c i e n c e s, N o v e m b e r 2 0 1 7 What is Cancer? Uncontrolled growth of cells Not all tumors
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia
 Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
molecular oncology services
 Molecular Oncology molecular oncology services ATIENTS.ANSWERS.RESULTS. www.aruplab.com/oncology MARCH 2018 Information in this brochure is current as of March 2018. All content is subject to change. lease
Molecular Oncology molecular oncology services ATIENTS.ANSWERS.RESULTS. www.aruplab.com/oncology MARCH 2018 Information in this brochure is current as of March 2018. All content is subject to change. lease
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Financial disclosures
 An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
Cancer genetics
 Cancer genetics General information about tumorogenesis. Cancer induced by viruses. The role of somatic mutations in cancer production. Oncogenes and Tumor Suppressor Genes (TSG). Hereditary cancer. 1
Cancer genetics General information about tumorogenesis. Cancer induced by viruses. The role of somatic mutations in cancer production. Oncogenes and Tumor Suppressor Genes (TSG). Hereditary cancer. 1
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Anatomic Molecular Pathology: An Emerging Field
 Anatomic Molecular Pathology: An Emerging Field Antonia R. Sepulveda M.D., Ph.D. University of Pennsylvania asepu@mail.med.upenn.edu 2008 ASIP Annual Meeting Anatomic pathology (U.S.) is a medical specialty
Anatomic Molecular Pathology: An Emerging Field Antonia R. Sepulveda M.D., Ph.D. University of Pennsylvania asepu@mail.med.upenn.edu 2008 ASIP Annual Meeting Anatomic pathology (U.S.) is a medical specialty
Test Name Results Units Bio. Ref. Interval. Positive
 LL - LL-ROHINI (NATIONAL REFERENCE 135091533 Age 28 Years Gender Male 1/9/2017 120000AM 1/9/2017 105415AM 4/9/2017 23858M Ref By Final LEUKEMIA DIAGNOSTIC COMREHENSIVE ROFILE, ANY 6 MARKERS t (1;19) (q23
LL - LL-ROHINI (NATIONAL REFERENCE 135091533 Age 28 Years Gender Male 1/9/2017 120000AM 1/9/2017 105415AM 4/9/2017 23858M Ref By Final LEUKEMIA DIAGNOSTIC COMREHENSIVE ROFILE, ANY 6 MARKERS t (1;19) (q23
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Financial disclosures
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Lynch Syndrome Screening for Endometrial Cancer: Basic Concepts 1/16/2017
 1 Hi, my name is Sarah Kerr. I m a pathologist at Mayo Clinic, where I participate in our high volume Lynch syndrome tumor testing practice. Today I hope to cover some of the basics needed to understand
1 Hi, my name is Sarah Kerr. I m a pathologist at Mayo Clinic, where I participate in our high volume Lynch syndrome tumor testing practice. Today I hope to cover some of the basics needed to understand
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328
 Rearrangement Following Therapy for APL Case 0328") Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328 Kenneth N. Holder, Leslie J. Greebon, Gopalrao Velagaleti, Hongxin Fan, Russell A. Higgins Initial Case: Clinical
Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328 Kenneth N. Holder, Leslie J. Greebon, Gopalrao Velagaleti, Hongxin Fan, Russell A. Higgins Initial Case: Clinical
Cost-Effective Strategies in the Workup of Hematologic Neoplasm. Karl S. Theil, Claudiu V. Cotta Cleveland Clinic
 Cost-Effective Strategies in the Workup of Hematologic Neoplasm Karl S. Theil, Claudiu V. Cotta Cleveland Clinic In the past 12 months, we have not had a significant financial interest or other relationship
Cost-Effective Strategies in the Workup of Hematologic Neoplasm Karl S. Theil, Claudiu V. Cotta Cleveland Clinic In the past 12 months, we have not had a significant financial interest or other relationship
KREATECH DIAGNOSTICS SOLID TUMORS
 KREATECH DIAGNOSTICS SOLID TUMORS RF POSEIDON SOLUTIONS FOR SOLID TUMOR FISH DIAGNOSTICS TABLE OF CONTENTS Breast Cancer 3 Bladder Cancer 4 Cervical Cancer 4 Lung Cancer 5 Prostate Cancer 6 Thyroid Carcinoma
KREATECH DIAGNOSTICS SOLID TUMORS RF POSEIDON SOLUTIONS FOR SOLID TUMOR FISH DIAGNOSTICS TABLE OF CONTENTS Breast Cancer 3 Bladder Cancer 4 Cervical Cancer 4 Lung Cancer 5 Prostate Cancer 6 Thyroid Carcinoma
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Molecular Markers in Acute Leukemia. Dr Muhd Zanapiah Zakaria Hospital Ampang
 Molecular Markers in Acute Leukemia Dr Muhd Zanapiah Zakaria Hospital Ampang Molecular Markers Useful at diagnosis Classify groups and prognosis Development of more specific therapies Application of risk-adjusted
Molecular Markers in Acute Leukemia Dr Muhd Zanapiah Zakaria Hospital Ampang Molecular Markers Useful at diagnosis Classify groups and prognosis Development of more specific therapies Application of risk-adjusted
THYROID TUMOR DIAGNOSIS: MARKER OF THE MONTH CLUB
 THYROID TUMOR DIAGNOSIS: MARKER OF THE MONTH CLUB CHARACTERISTIC OF THE IDEAL TUMOR MARKER Specific Sensitive Easy to perform Easy to interpret Adaptable to FNA Reasonable cost (CHEAP) THYROID TUMOR MARKERS
THYROID TUMOR DIAGNOSIS: MARKER OF THE MONTH CLUB CHARACTERISTIC OF THE IDEAL TUMOR MARKER Specific Sensitive Easy to perform Easy to interpret Adaptable to FNA Reasonable cost (CHEAP) THYROID TUMOR MARKERS
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the author to give readers additional information about his work. Supplement to: Croce CM. Oncogenes and cancer. N Engl J Med 2008;358:502-11.
Supplementary Appendix This appendix has been provided by the author to give readers additional information about his work. Supplement to: Croce CM. Oncogenes and cancer. N Engl J Med 2008;358:502-11.
Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San
 Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San Francisco Lung Cancer Classification Pathological Classification
Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San Francisco Lung Cancer Classification Pathological Classification
609G: Concepts of Cancer Genetics and Treatments (3 credits)
") Master of Chemical and Life Sciences Program College of Computer, Mathematical, and Natural Sciences 609G: Concepts of Cancer Genetics and Treatments (3 credits) Text books: Principles of Cancer Genetics,
Master of Chemical and Life Sciences Program College of Computer, Mathematical, and Natural Sciences 609G: Concepts of Cancer Genetics and Treatments (3 credits) Text books: Principles of Cancer Genetics,
78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP)
 Gene Gulati PhD, SH(ASCP)") 78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP) 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste. 1600 Chicago,
78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP) 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste. 1600 Chicago,
Molecular Markers. Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC
 Molecular Markers Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC Overview Testing methods Rationale for molecular testing
Molecular Markers Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC Overview Testing methods Rationale for molecular testing
August 17, Dear Valued Client:
 August 7, 08 Re: CMS Announces 6-Month Period of Enforcement Discretion for Laboratory Date of Service Exception Policy Under the Medicare Clinical Laboratory Fee Schedule (the 4 Day Rule ) Dear Valued
August 7, 08 Re: CMS Announces 6-Month Period of Enforcement Discretion for Laboratory Date of Service Exception Policy Under the Medicare Clinical Laboratory Fee Schedule (the 4 Day Rule ) Dear Valued
Chapt 15: Molecular Genetics of Cell Cycle and Cancer
 Chapt 15: Molecular Genetics of Cell Cycle and Cancer Student Learning Outcomes: Describe the cell cycle: steps taken by a cell to duplicate itself = cell division; Interphase (G1, S and G2), Mitosis.
Chapt 15: Molecular Genetics of Cell Cycle and Cancer Student Learning Outcomes: Describe the cell cycle: steps taken by a cell to duplicate itself = cell division; Interphase (G1, S and G2), Mitosis.
Molecular Oncology, oncology parameters see each test
 Molecular Oncology, oncology parameters see each test DPD deficiency Dihydropyrimidine dehydrogenase deficiency (DPD deficiency) is an autosomal recessive metabolic disorder in which there is absent or
Molecular Oncology, oncology parameters see each test DPD deficiency Dihydropyrimidine dehydrogenase deficiency (DPD deficiency) is an autosomal recessive metabolic disorder in which there is absent or
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities
 Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities Sujana Movva 1, Wenhsiang Wen 2, Wangjuh Chen 2, Sherri Z. Millis 2, Margaret von Mehren 1, Zoran
Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities Sujana Movva 1, Wenhsiang Wen 2, Wangjuh Chen 2, Sherri Z. Millis 2, Margaret von Mehren 1, Zoran
Technology from Abcam
 CD2 (EP222) CD2 is one of the earliest T-cell lineage restricted antigens to appear during T-cell differentiation and only rare CD2+ cells can be found in the bone marrow. Anti-CD2 is a pan-t-cell antigen
CD2 (EP222) CD2 is one of the earliest T-cell lineage restricted antigens to appear during T-cell differentiation and only rare CD2+ cells can be found in the bone marrow. Anti-CD2 is a pan-t-cell antigen
Multistep nature of cancer development. Cancer genes
 Multistep nature of cancer development Phenotypic progression loss of control over cell growth/death (neoplasm) invasiveness (carcinoma) distal spread (metastatic tumor) Genetic progression multiple genetic
Multistep nature of cancer development Phenotypic progression loss of control over cell growth/death (neoplasm) invasiveness (carcinoma) distal spread (metastatic tumor) Genetic progression multiple genetic
Personalized Medicine: Lung Biopsy and Tumor
 Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Development of Carcinoma Pathways
 The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
HSL-Advanced Diagnostics 2018 / 19 Test & Service List
 HSL-Advanced Diagnostics 2018 / 19 Test & Service List 2018/19 TEST & SERVICE LIST Haematoxylin & Eosin H&E H&E per slide Routine Immunohistochemistry Immunohistochemical demonstration of an antigen in
HSL-Advanced Diagnostics 2018 / 19 Test & Service List 2018/19 TEST & SERVICE LIST Haematoxylin & Eosin H&E H&E per slide Routine Immunohistochemistry Immunohistochemical demonstration of an antigen in
Policy Specific Section: Medical Necessity and Investigational / Experimental. October 14, 1998 March 28, 2014
 Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory. Dr Paula Waits Bristol Genetics Laboratory
 The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
Evolution of Pathology
 1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
of 20 to 80 and subsequently declines [2].
![of 20 to 80 and subsequently declines [2].](/thumbs/80/81450506.jpg "of 20 to 80 and subsequently declines [2].") - - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
- - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Haematology Probes for Multiple Myeloma
 Haematology Probes for Multiple Myeloma MULTIPLE MYELOMA Multiple myeloma (MM) is a plasma cell neoplasm, characterised by the accumulation of clonal plasma cells in the bone marrow and by very complex
Haematology Probes for Multiple Myeloma MULTIPLE MYELOMA Multiple myeloma (MM) is a plasma cell neoplasm, characterised by the accumulation of clonal plasma cells in the bone marrow and by very complex
Molecular Cell Biology. Prof. D. Karunagaran. Department of Biotechnology. Indian Institute of Technology Madras
 Molecular Cell Biology Prof. D. Karunagaran Department of Biotechnology Indian Institute of Technology Madras Module 9 Molecular Basis of Cancer, Oncogenes and Tumor Suppressor Genes Lecture 2 Genes Associated
Molecular Cell Biology Prof. D. Karunagaran Department of Biotechnology Indian Institute of Technology Madras Module 9 Molecular Basis of Cancer, Oncogenes and Tumor Suppressor Genes Lecture 2 Genes Associated
Malignant lymphomas are neoplasms that arise from B
 Overview of the Role of Molecular Methods in the Diagnosis of Malignant Lymphomas L. Jeffrey Medeiros, MD; Jeanne Carr, PhD Objective. To review the role of molecular genetics in the diagnosis of malignant
Overview of the Role of Molecular Methods in the Diagnosis of Malignant Lymphomas L. Jeffrey Medeiros, MD; Jeanne Carr, PhD Objective. To review the role of molecular genetics in the diagnosis of malignant
Follicular Lymphoma: the WHO
 Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Tumor Markers & Cytopathology
 Tumor Markers & Cytopathology Objectives: After learning, student should be able to 1. Describe the basic concepts of tumor markers and Asst. Prof. Prasit Suwannalert, Ph.D. (Email: prasit.suw@mahidol.ac.th)
Tumor Markers & Cytopathology Objectives: After learning, student should be able to 1. Describe the basic concepts of tumor markers and Asst. Prof. Prasit Suwannalert, Ph.D. (Email: prasit.suw@mahidol.ac.th)
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Fluorescence in-situ Hybridization (FISH) ETO(RUNX1T1)/AML1(RUNX1) or t(8;21)(q21.3;q22)
 ETO(RUNX1T1)/AML1(RUNX1) or t(8;21)(q21.3;q22)") PML/RARA t(15;17) Translocation Assay Result : nuc ish(pml 2)(RARA 2)[200] : 200/200(100%) interphase nuclei show normal 2O 2G signals for PML/RARA : is Negative for t(15;17)(q22;q21.1) 2 Orange 2 Green
PML/RARA t(15;17) Translocation Assay Result : nuc ish(pml 2)(RARA 2)[200] : 200/200(100%) interphase nuclei show normal 2O 2G signals for PML/RARA : is Negative for t(15;17)(q22;q21.1) 2 Orange 2 Green
Cancer. The fundamental defect is. unregulated cell division. Properties of Cancerous Cells. Causes of Cancer. Altered growth and proliferation
 Cancer The fundamental defect is unregulated cell division. Properties of Cancerous Cells Altered growth and proliferation Loss of growth factor dependence Loss of contact inhibition Immortalization Alterated
Cancer The fundamental defect is unregulated cell division. Properties of Cancerous Cells Altered growth and proliferation Loss of growth factor dependence Loss of contact inhibition Immortalization Alterated
Application. Application of molecular biology methods in hematology and oncology. Oncogenes are involved in:
 Application Application of molecular biology methods in hematology and oncology Research on the etiology of cancer Diagnostics / Differential diagnostics Stratifying for treatment Prognosing the outcome
Application Application of molecular biology methods in hematology and oncology Research on the etiology of cancer Diagnostics / Differential diagnostics Stratifying for treatment Prognosing the outcome
Case 1. Disclosure. Imaging. Clinical history 5/10/2016. USCAP 2016 Annual Meeting Evening Specialty Conference Bone and Soft tissue Pathology
 Disclosure Dr. Agaram has nothing to disclose Case 1 Narsi Agaram, MBBS USCAP 2016 Annual Meeting Evening Specialty Conference Bone and Soft tissue Pathology Clinical history Imaging 1998 A three month
Disclosure Dr. Agaram has nothing to disclose Case 1 Narsi Agaram, MBBS USCAP 2016 Annual Meeting Evening Specialty Conference Bone and Soft tissue Pathology Clinical history Imaging 1998 A three month
Template for Reporting Results of Monitoring Tests for Patients With Chronic Myelogenous Leukemia (BCR-ABL1+)
") Template for Reporting Results of Monitoring Tests for Patients With Chronic Myelogenous Leukemia (BCR-ABL1+) Version: CMLBiomarkers 1.0.0.2 Protocol Posting Date: June 2017 This biomarker template is
Template for Reporting Results of Monitoring Tests for Patients With Chronic Myelogenous Leukemia (BCR-ABL1+) Version: CMLBiomarkers 1.0.0.2 Protocol Posting Date: June 2017 This biomarker template is
number Done by Corrected by Doctor Maha Shomaf
 number 19 Done by Waseem Abo-Obeida Corrected by Abdullah Zreiqat Doctor Maha Shomaf Carcinogenesis: the molecular basis of cancer. Non-lethal genetic damage lies at the heart of carcinogenesis and leads
number 19 Done by Waseem Abo-Obeida Corrected by Abdullah Zreiqat Doctor Maha Shomaf Carcinogenesis: the molecular basis of cancer. Non-lethal genetic damage lies at the heart of carcinogenesis and leads
Clonal evolution of human cancers
 Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Karyotype analysis reveals transloction of chromosome 22 to 9 in CML chronic myelogenous leukemia has fusion protein Bcr-Abl
 Chapt. 18 Cancer Molecular Biology of Cancer Student Learning Outcomes: Describe cancer diseases in which cells no longer respond Describe how cancers come from genomic mutations (inherited or somatic)
Chapt. 18 Cancer Molecular Biology of Cancer Student Learning Outcomes: Describe cancer diseases in which cells no longer respond Describe how cancers come from genomic mutations (inherited or somatic)
Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making
 Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making November 20, 2014 Capturing Value in Next Generation Sequencing Symposium Douglas Johnson MD, MSCI Vanderbilt-Ingram
Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making November 20, 2014 Capturing Value in Next Generation Sequencing Symposium Douglas Johnson MD, MSCI Vanderbilt-Ingram
Tumor Markers Yesterday, Today & Tomorrow. Steven E. Zimmerman M.D. Vice President & Chief Medical Director
 Tumor Markers Yesterday, Today & Tomorrow Steven E. Zimmerman M.D. Vice President & Chief Medical Director Tumor Marker - Definition Substances produced by cancer cells or other cells in response to cancer
Tumor Markers Yesterday, Today & Tomorrow Steven E. Zimmerman M.D. Vice President & Chief Medical Director Tumor Marker - Definition Substances produced by cancer cells or other cells in response to cancer
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION CYTOPATHOLOGY Monday, April 26, 2013 FACULTY COPY
 GOAL: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION CYTOPATHOLOGY Monday, April 26, 2013 FACULTY COPY 1. Understated the role of cytopathology in the clinical management of the patient and recognize
GOAL: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION CYTOPATHOLOGY Monday, April 26, 2013 FACULTY COPY 1. Understated the role of cytopathology in the clinical management of the patient and recognize
Dr C K Kwan. Associate Consultant, Queen Elizabeth Hospital, HKSAR Honorary member, Targeted Therapy Team, ICR, UK
 HA Convention 2013 Dr C K Kwan MBChB, FRCR, FHKCR, FHKAM, MPM, CPI, MAppMgt(Hlth) Associate Consultant, Queen Elizabeth Hospital, HKSAR Honorary member, Targeted Therapy Team, ICR, UK To personalize cancer
HA Convention 2013 Dr C K Kwan MBChB, FRCR, FHKCR, FHKAM, MPM, CPI, MAppMgt(Hlth) Associate Consultant, Queen Elizabeth Hospital, HKSAR Honorary member, Targeted Therapy Team, ICR, UK To personalize cancer
Surgical Pathology Evening Specialty Conference USCAP 2015
 Surgical Pathology Evening Specialty Conference USCAP 2015 John R. Goldblum, M.D. Chairman, Department of Pathology, Cleveland Clinic Professor of Pathology, Cleveland Clinic Lerner College of Medicine
Surgical Pathology Evening Specialty Conference USCAP 2015 John R. Goldblum, M.D. Chairman, Department of Pathology, Cleveland Clinic Professor of Pathology, Cleveland Clinic Lerner College of Medicine