Polypoid lesions of the gastrointestinal tract
|
|
|
- Anna Elliott
- 5 years ago
- Views:
Transcription
1 Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015
2 Polypoid lesions of the gastrointestinal tract A polyp is any lesion that is raised above an epithelial surface
3 Polypoid lesions of the gastrointestinal tract polyp = any lesion that is raised above an epithelial surface polypoid = something that looks like something that is raised above an epithelial surface pseudo-polyp = something that looks like something that is raised above an epithelial surface

4

5 Gastric polyps Morson & Dawson s Gastrointestinal Pathology, 2013
6 Colorectal polyps
7 Polypoid lesions of the gastrointestinal tract Case 1
8 Case 1 64M. 96mm polypoid mass in stomach. Wedge resection and second resection of adjacent stomach with thickened area.

9 96mm polypoid lesion

10 Gastric adenoma type 1 intestinal type 2 foveolar others pyloric gland adenoma (rare)
11 Gastric adenoma 34 intestinal-type adenomas (56%) in 31 patients 25 gastric-type adenomas (41%) in 18 patients (but 10 with FAP) intestinal-type adenomas significantly more likely to show: high-grade dysplasia adenocarcinoma within the polyp intestinal metaplasia in the surrounding stomach gastritis in the surrounding stomach separate adenocarcinoma Abraham et al. Am J Surg Pathol 2002; 26:

12 Gastric type 2/foveolar adenoma rarer often large and protuberant lower grades of dysplasia dysplasia subtle often mistaken for hyperplastic polyp of the stomach less carcinoma

13 Second resection of adjacent stomach with thickened area

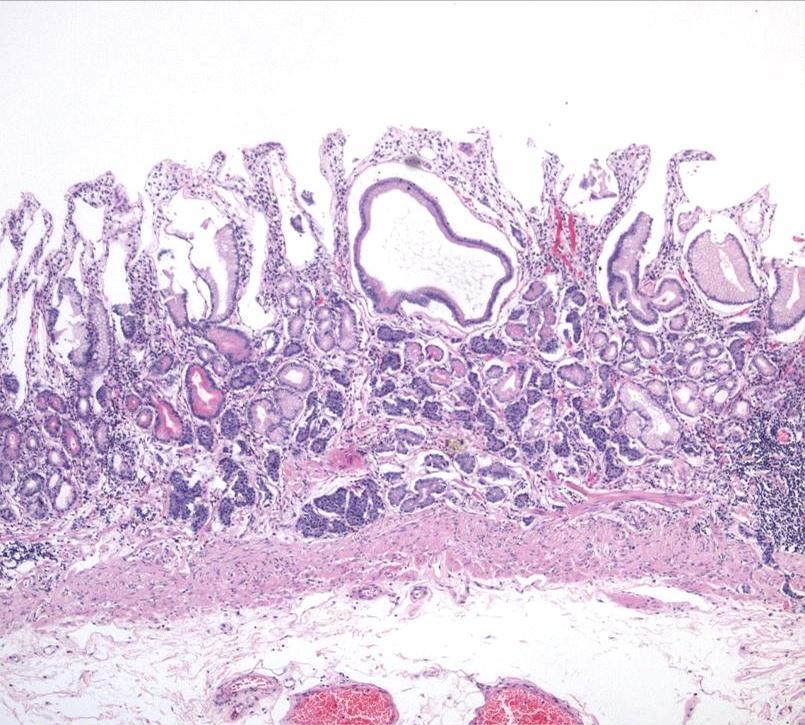
14 The adjacent mucosa..


15 Second resection of adjacent stomach with thickened area


16 Second resection of adjacent stomach with thickened area cytokeratin


17 Second resection of adjacent stomach with thickened area synaptophysin

18 Gastric neuro-endocrine tumour (NET) (formerly carcinoid) Four types of gastric chronic atrophic Zollinger-Ellison syndrome sporadic intrinsic abnormality of parietal cells The first is the commonest, is usually benign and often treated very conservatively (EMR/ER/surveillance only)


19 Context in gastrointestinal neuro-endocrine tumours Rectum Stomach Stomach
20 Case 1 - learning points always look at the background mucosa in any polyp pathology this patient had chronic atrophic gastritis chronic atrophic gastritis predisposes to multiple neuro-endocrine tumours these NETs are mainly small, benign and treated conservatively BUT you also get adenomas, MANECs and frank adenocarcinomas complicating CAG Multiple neuro-endocrine tumours complicating chronic atrophic gastritis: the cloak that hides the dagger Bamford & Shepherd, 2015
21 Polypoid lesions of the gastrointestinal tract Case 1 diagnosis: Foveolar (type 2) adenoma and neuro-endocrine tumours complicating chronic atrophic gastritis
22 Polypoid lesions of the gastrointestinal tract Case 2
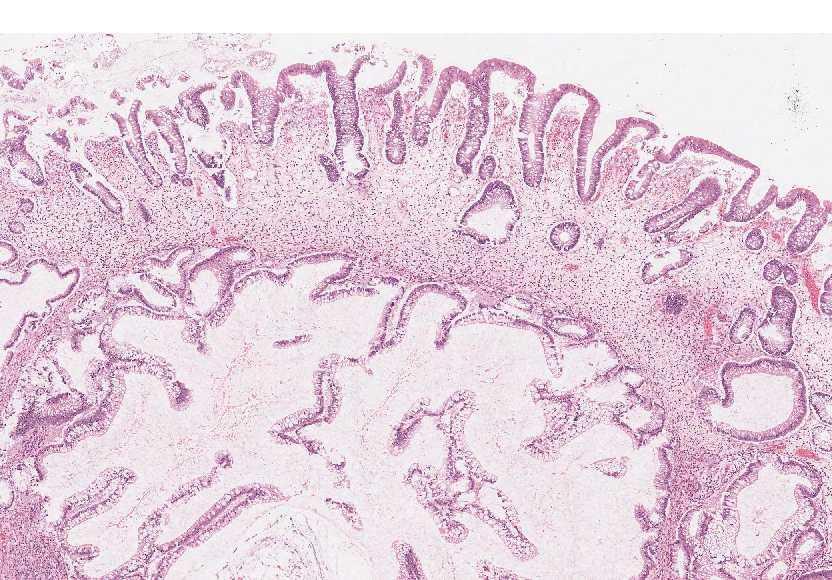
23 Case 2 Female 27 years. Multiple polyps in colon.
24
25

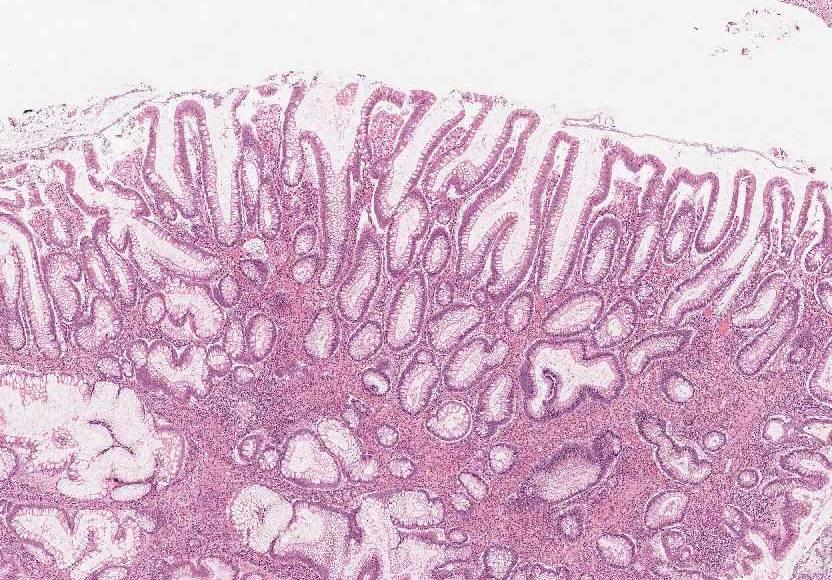
26 Is this dysplasia?

27 Is this dysplasia?
28


29




30 Case 2
31 Case 2
32 Juvenile polyposis 1 in 80,000 genetics becoming clearer but polymorphic: SMAD4 implicated in 25%; BMPR1A in 20% high rates of colorectal cancer: life time risk -? up to 60% dysplasia in atypical juvenile polyps? surveillance? prophylactic colectomy
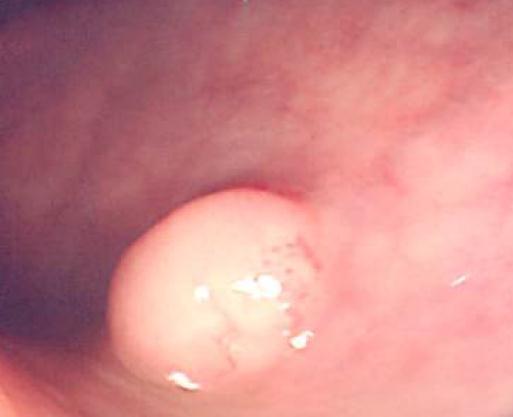
33 SMAD 4 mutation is implicated in about a quarter of cases of juvenile polyposis. What does SMAD stand for? 1. small mothers against decapentaplegia 2. serine-methionine-arginine deletion 3. somatic mutation in Aleutian drosophila
34 SMAD 4 mutation is implicated in about a quarter of cases of juvenile polyposis. What does SMAD stand for? 1. small mothers against decapentaplegia 2. serine-methionine-arginine deletion 3. somatic mutation in Aleutian drosophila
35 Mutations of the gene BMPR1A are implicated in about 20% of cases of juvenile polyposis. What does BMPR stand for? 1. bowel matrix protein regulator? 2. bone morphogenetic protein receptor? 3. biotin muscle protein resorption?
36 Mutations of the gene BMPR1A are implicated in about 20% of cases of juvenile polyposis. What does BMPR stand for? 1. bowel matrix protein regulator? 2. bone morphogenetic protein receptor? 3. biotin muscle protein resorption?
37 Case 2 - learning points juvenile polyps are common commonest polyp in the under 20s and have classic pathology juvenile polyposis causes strange-looking polyps ( atypical juvenile polyps ) which are multiple although not of the number, usually, seen in FAP (often ) atypical juvenile polyps show high levels of dysplasia significant cancer risk for JP and it may affect the whole gut
38 Case 2 Diagnosis: atypical juvenile polyp in juvenile polyposis
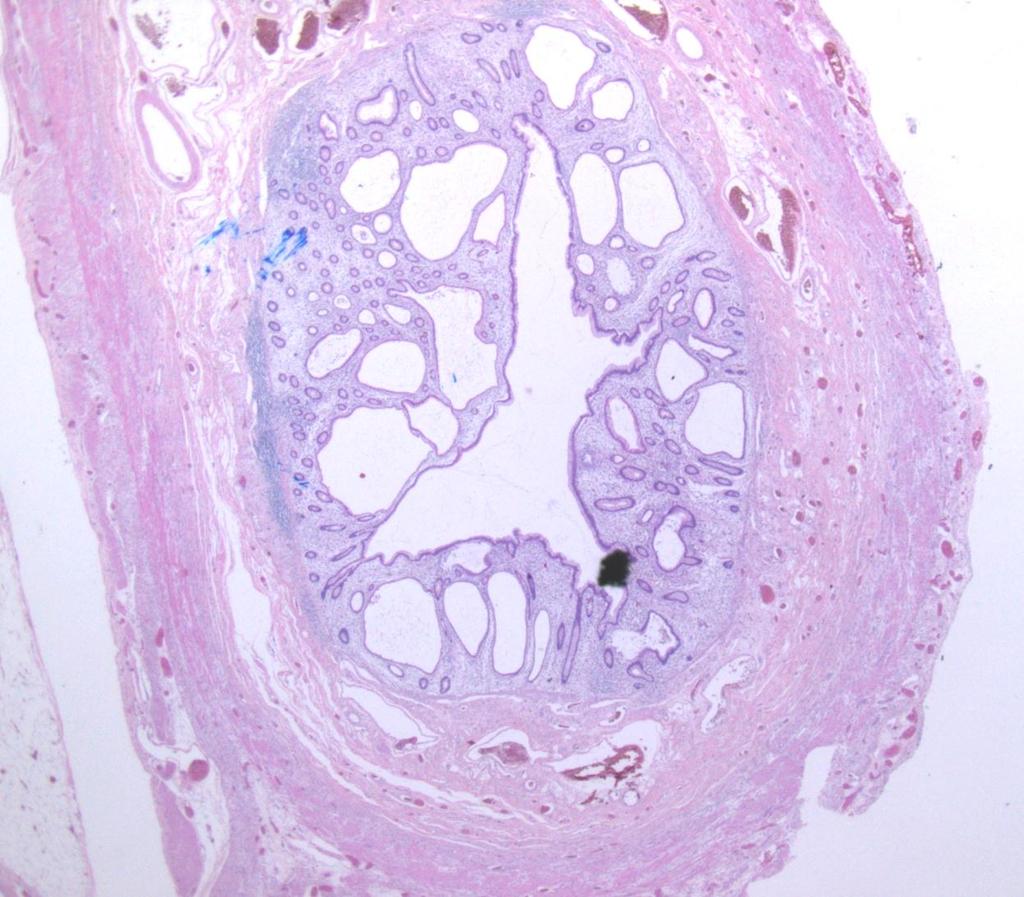
39 Polypoid lesions of the gastrointestinal tract Case 3
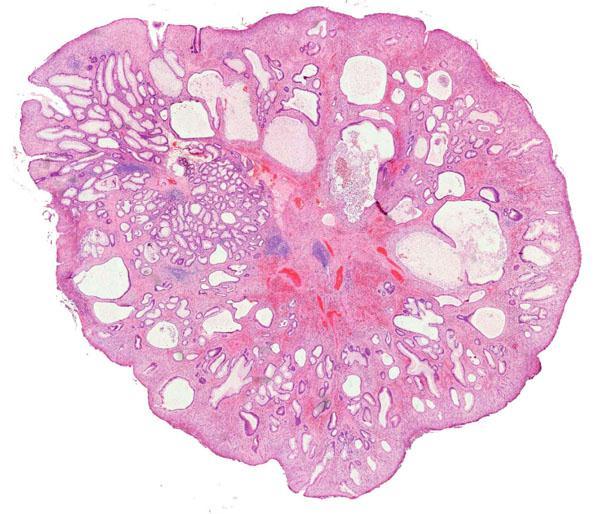
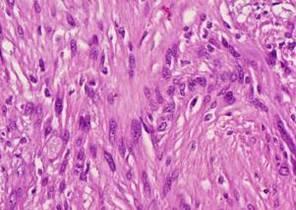
40 Case 3 Female 45 years. 40mm polypoid nodule in ascending colon.

41
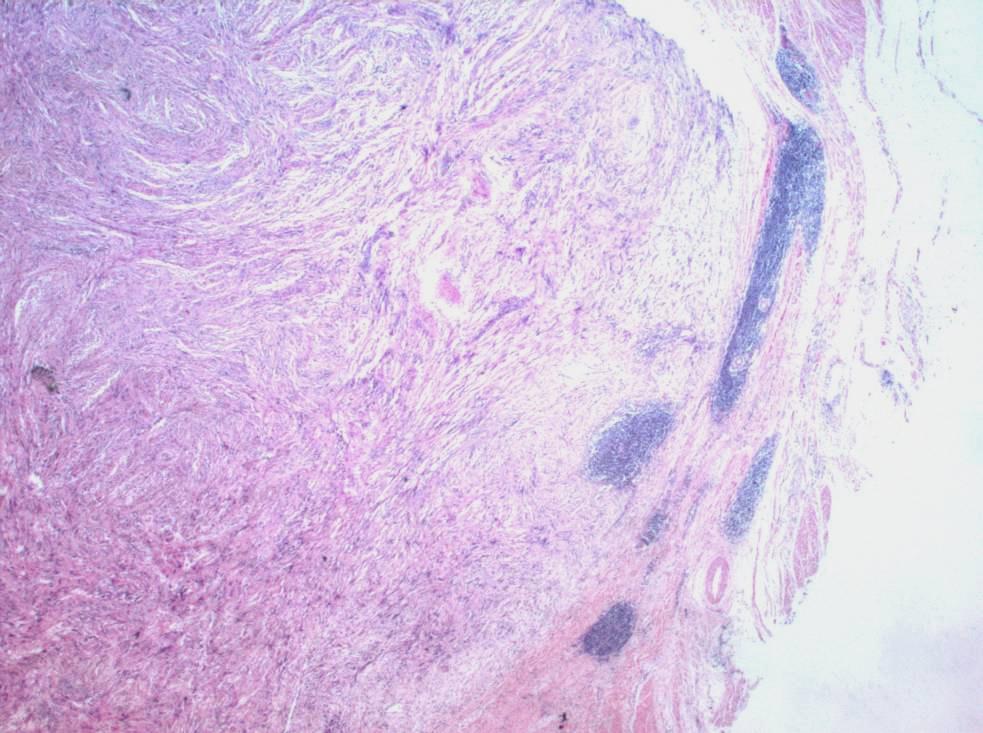
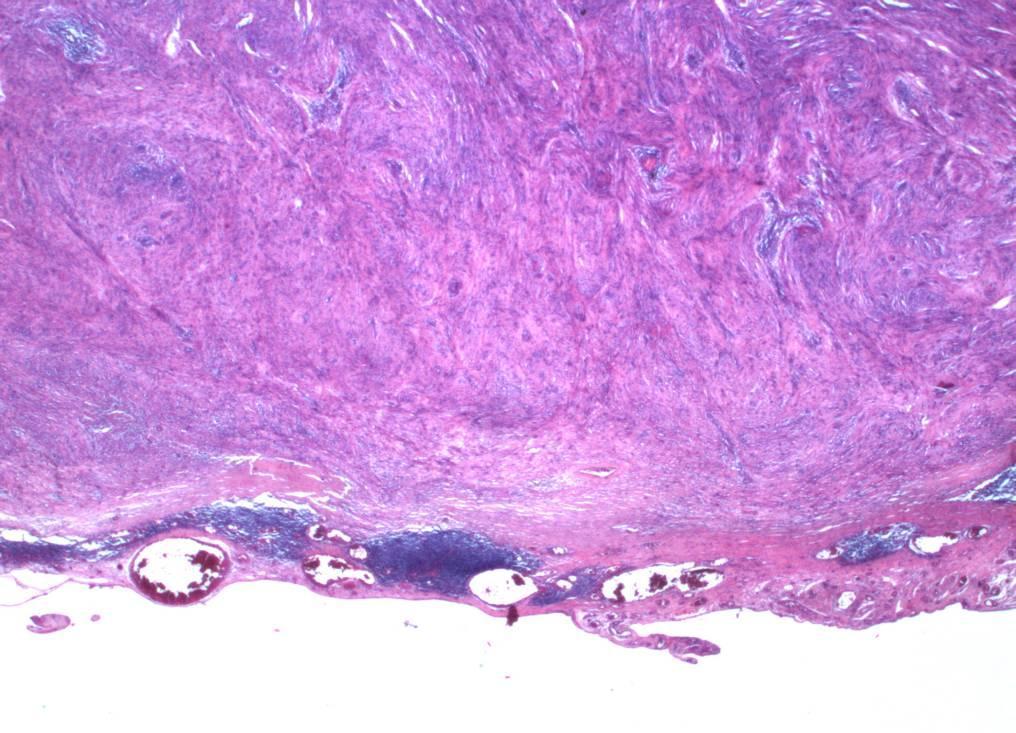
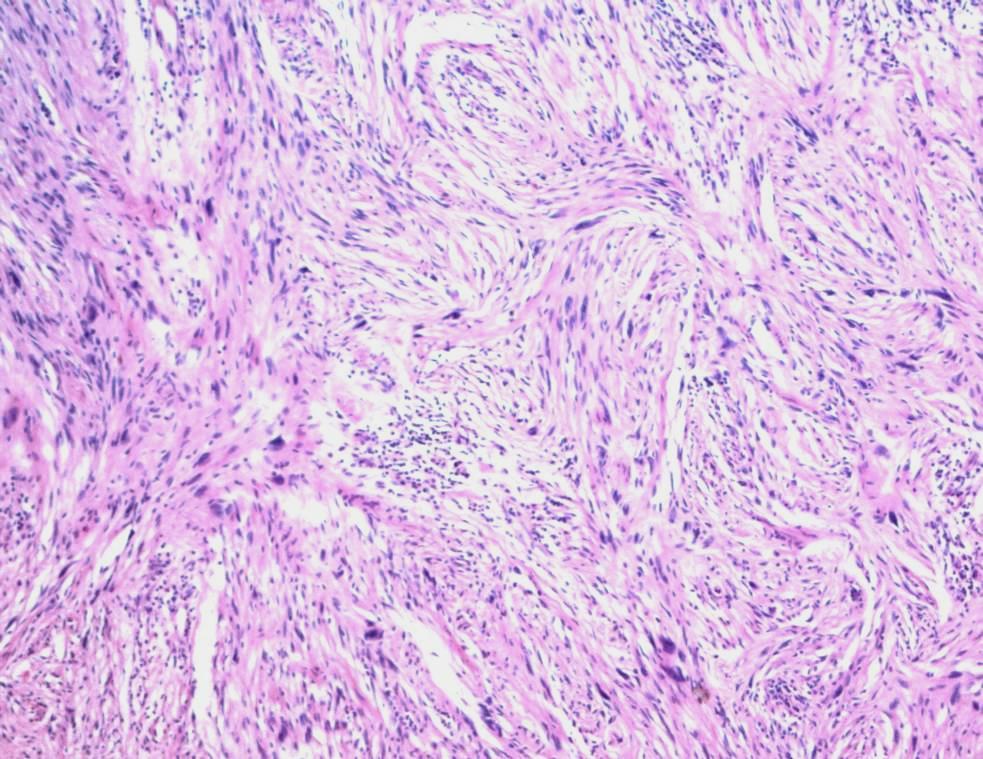
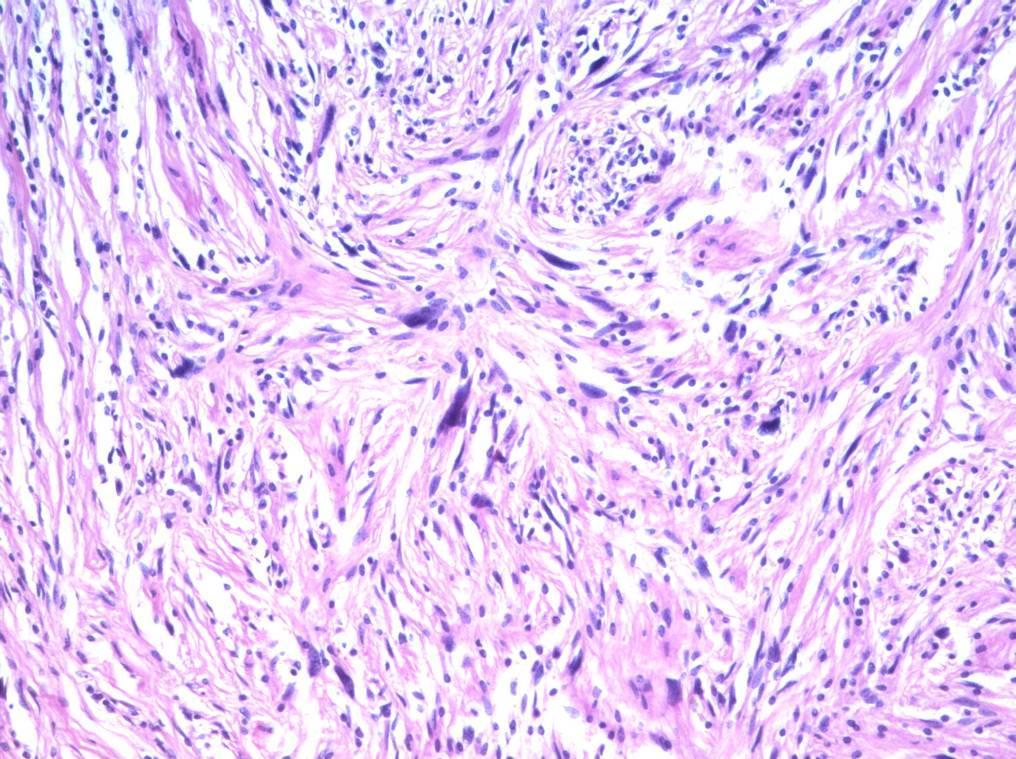
42
43 ? diagnosis? immunohistochemistry



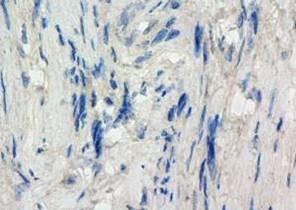
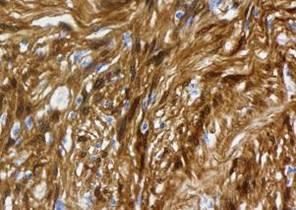
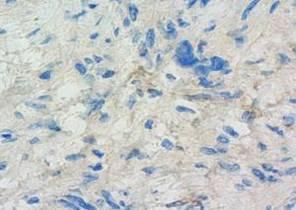
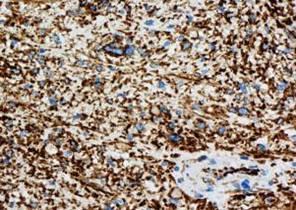
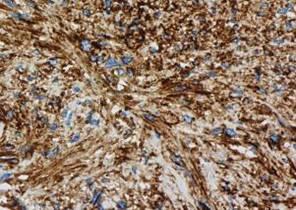
44 CD117 CD34 SMA desmin H&E S100 DOG1 nestin L1


45 Gastrointestinal schwannoma: the peritumoral lymphoid hyperplasia is almost pathognomonic
46 Gastrointestinal schwannoma can occur anywhere in the GI tract, but commonest in the stomach (60-70%), then colorectum microscopic features different from conventional schwannomas lack NF2 gene mutations unlike conventional schwannomas probably different tumours almost always behave in a benign fashion
47 Gastrointestinal schwannoma 33 cases: 4 oesophagus, 24 stomach, 2 colon and 3 rectum mainly within muscularis propria and/or subserosa none encapsulated but all well circumscribed 32/33 cuff of lymphocytes only 12 originally called schwannoma S100 and vimentin positive; CD117, CD34, ASMA, desmin negative all showed some nuclear pleomorphism:? longevity: no mitoses all benign Hou et al, Histopathology 2006

48 Gastric schwannoma showing central ulcer Levy et al. AJR 2005;184:
49 Case 3 - learning points not all spindle cell tumours of the gut are GISTs all larger GISTs are potentially malignant and there are many benign mimics smaller stromal tumours, especially in the stomach and colorectum, often present as polyps in bowel cancer screening, you see any number of unusual small polyps including unusual stromal tumours (perineurioma, epithelioid mucosal neuroma, neurofibroma, leiomyoma of the muscularis mucosae, etc)
50 Case 3 Diagnosis: gastrointestinal schwannoma in colon
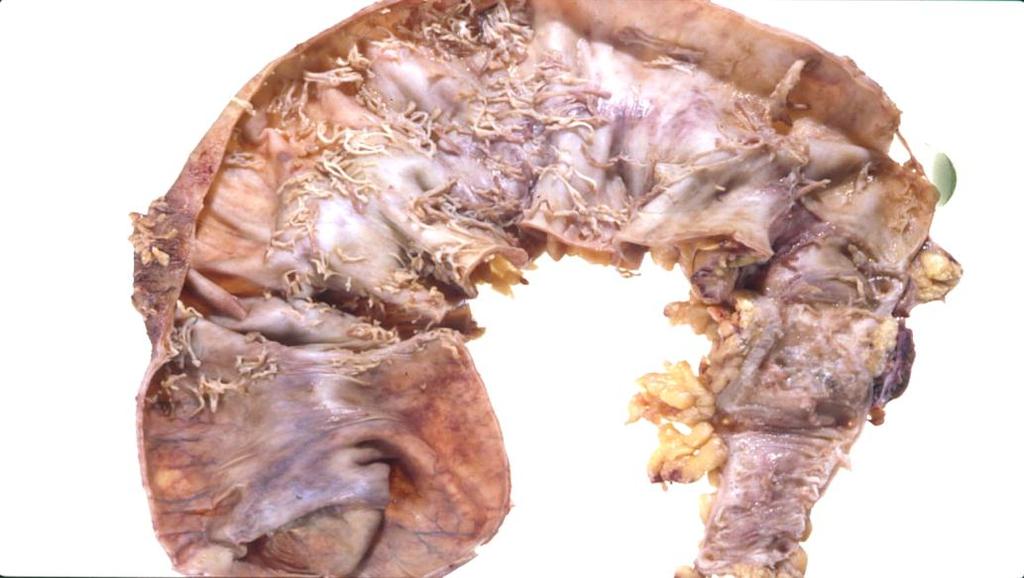
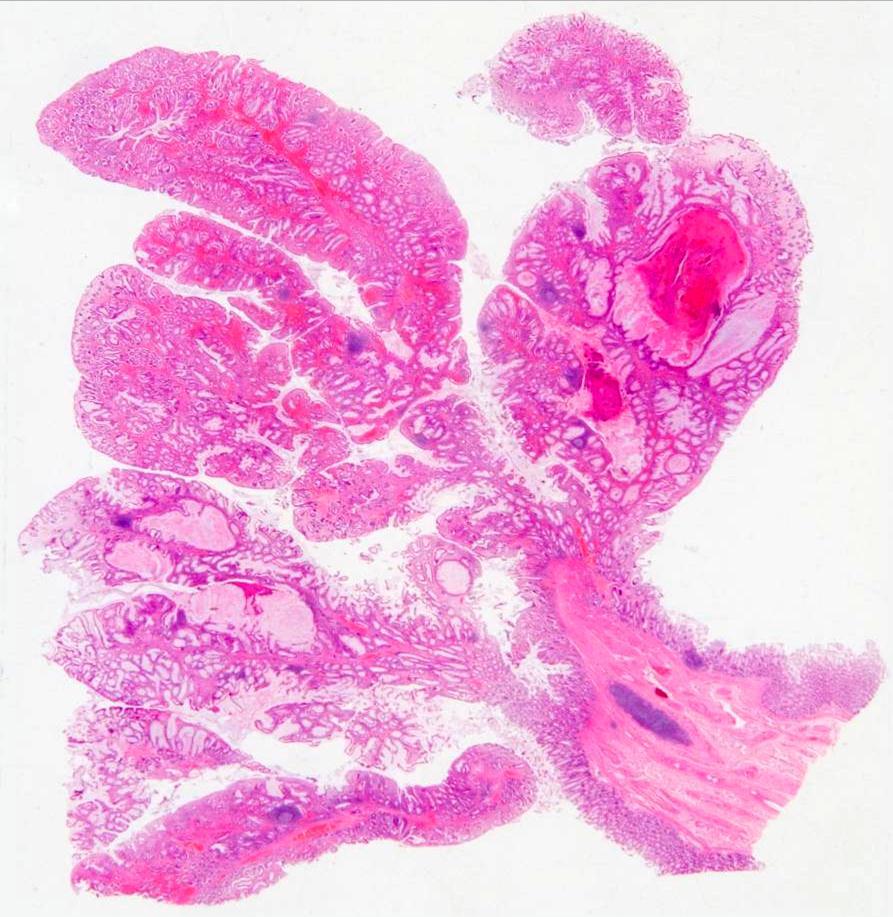
51 Case 4 68M. Three month history of diarrhoea, especially mucus diarrhoea, loss of weight and fatigue. Colonoscopy.
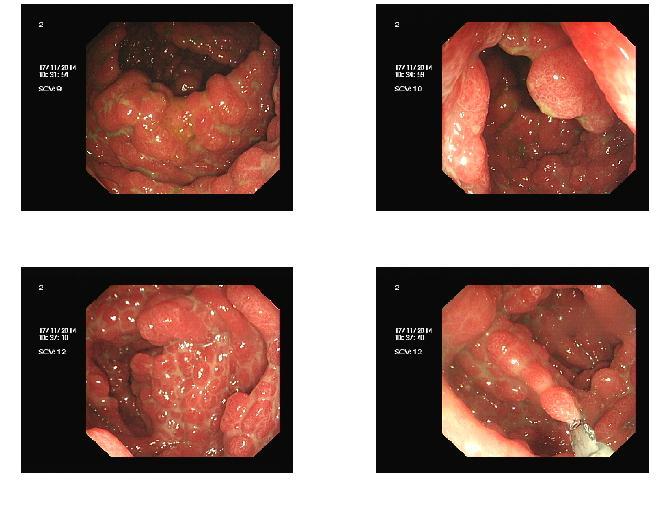
52
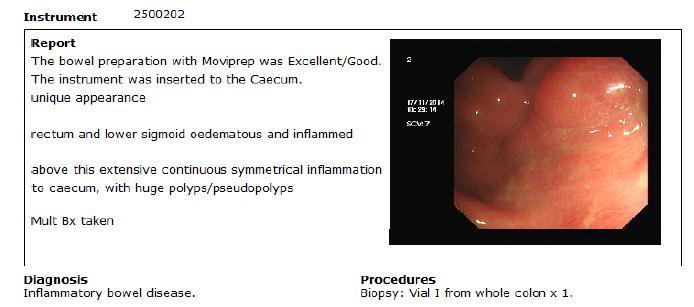
53 Colonoscopy

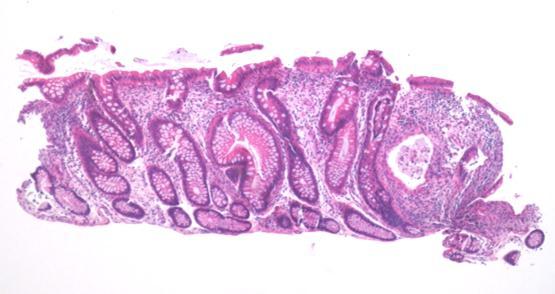
54 Biopsy pathology


55 in keeping with active chronic inflammatory bowel disease of ulcerative colitis type
56 Management working diagnosis: chronic inflammatory bowel disease, probably ulcerative colitis with inflammatory polyp formation treated with mesalazine and high dose steroids with poor response infliximab tried but continued deterioration continuing severe mucus diarrhoea and hypokalaemia subtotal colectomy one month after initial presentation


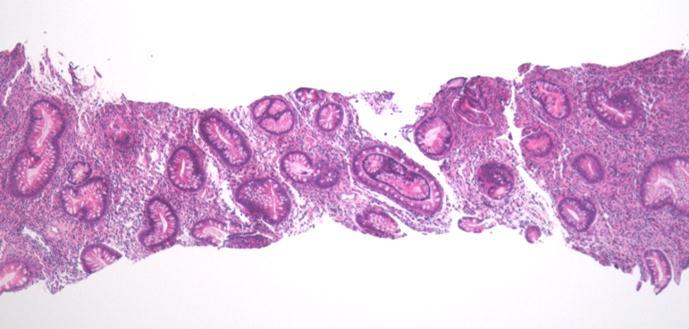
57 Colon - low and high power

58


59 Histology of ileum and typical colon

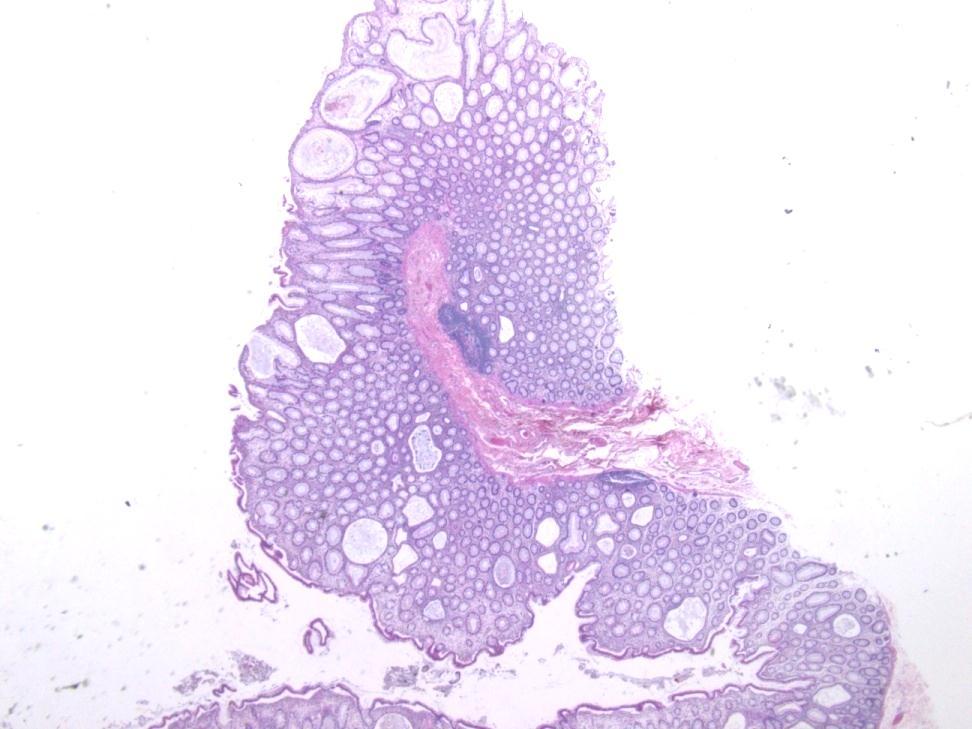
60 Polypoid areas in colon
61 Appendix
62 Further management treated as inflammatory bowel disease of ulcerative colitis type but discussed in MDTM and agreed that a second opinion was required
63 That second opinion guess who by?!? Now, normally, I would be a little hesitant about making dogmatic diagnoses in second opinion practice because this can be dangerous, perhaps particularly in somebody who has already been extensively treated, as in this case. However, I am going to make a dogmatic diagnosis here. I think this is Cronkhite- Canada syndrome. Cronkhite-Canada syndrome is an abnormality of ectodermal tissues, possibly a defect of apoptosis. It is an acquired condition, usually presenting in the 60s and is slightly more common in males. The colon is universally affected but most patients have gastric and small bowel involvement (an upper GI endoscopy in this patient would be interesting). To fully confirm the diagnosis, one requires to confirm the presence of the extra-alimentary manifestations of the disease (alopecia, hyperpigmentation, marked oedema, cataracts and onycholysis). A quick check for the clinician would be to look at this man s fingernails and to make sure he has not got a wig



64
65 Upper GI endoscopy Because of his recent diagnosis of Cronkhite-Canada syndrome, I brought him in for a gastroscopy which revealed extensive polyps in the distal half of his stomach and also his proximal duodenum.
66 Generalized gastrointestinal polyposis an unusual syndrome of polyposis, pigmentation, alopecia and onychotrophia Leonard W. Cronkhite, Jr., M.D., and Wilma Jeanne Canada, M.D. N Engl J Med 1955; 252:
67 Daniel ES, et al. Medicine 1982
68 Daniel ES, et al. Medicine 1982

69 Daniel ES, et al. Medicine 1982

70 Daniel ES, et al. Medicine 1982

71 Daniel ES, et al. Medicine 1982


72 Cronkhite-Canada syndrome a disease of ectoderm polyposis of the GI tract characteristic skin and nail changes 50s to 60s M > F likely a defect of ectodermal apoptosis mucus diarrhoea is a characteristic presentation poor prognosis protein-losing enteropathy and colopathy, electrolyte disturbances colorectal neoplasia markedly increased
73 Polypoid lesions of the gastrointestinal tract Case 4 diagnosis: Cronkhite-Canada syndrome
74 Take home messages: Polypoid lesions of the gastrointestinal tract the term polyp merely describes any lesion raised above an epithelial surface in every part of the GI tract, there are many causes. colonoscopists tend to equate polyp with adenoma and this can be very misleading it is always important to look at the background mucosa because this can give important clues about the diagnosis and pathogenesis (eg neuro-endocrine tumours and chronic atrophic gastritis; polyposis syndromes, etc) in bowel cancer screening, you see any number of unusual small polyps including neuro-endocrine tumours and unusual stromal tumours (perineurioma, epithelioid mucosal neuroma, neurofibroma, leiomyoma of the muscularis mucosae, etc)
75 Thank you for listening!
12/7/2011. Pathological mimics of malignancy in the GI tract. Professor Neil A Shepherd President, British Division of the IAP
 Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
FINAL HISTOLOGICAL DIAGNOSIS: Villo-adenomatous polyp with in-situ-carcinomatous foci (involving both adenomatous and villous component).
.") SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
27
 26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
A rare gastric polyposis: Cronkhite-Canada syndrome
 Diagnostic and Interventional Imaging (2012) 93, 799 803 RADIOLOGIC PATHOLOGIC CORRELATION / Gastrointestinal imaging A rare gastric polyposis: Cronkhite-Canada syndrome C. Sellal a,, C. Lemarié b, F.
Diagnostic and Interventional Imaging (2012) 93, 799 803 RADIOLOGIC PATHOLOGIC CORRELATION / Gastrointestinal imaging A rare gastric polyposis: Cronkhite-Canada syndrome C. Sellal a,, C. Lemarié b, F.
Small Bowel Cases. Introduction. Introduction, Continued 12/7/2011. Lesions Found on endoscopic biopsies Just Like Signing Out
 Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
JOURNAL OF CASE REPORTS 2014;4(2):
:") JOURNAL OF CASE REPORTS 2014;4(2):395-399 Juvenile Polyposis Syndrome -Two Case Reports Samuel Essoun 1, Jonathan CB Dakubo 2, Antoinette A Bediako-Bowan 2 From the Department of Surgery, 1 Korle Bu Teaching
JOURNAL OF CASE REPORTS 2014;4(2):395-399 Juvenile Polyposis Syndrome -Two Case Reports Samuel Essoun 1, Jonathan CB Dakubo 2, Antoinette A Bediako-Bowan 2 From the Department of Surgery, 1 Korle Bu Teaching
Pseudoinvasion and how to deal with it
 Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Gastrointestinal Malignancies. Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline
 Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Pathology perspective of colonic polyposis syndromes
 Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Hereditary Gastric Cancer
 Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
The pathology of neuroendocrine tumours of the gut
 The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The pathology of neuroendocrine tumours (NETs)
The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The pathology of neuroendocrine tumours (NETs)
A 9cm mass was excised from the jejunal wall and mesentery of a 33 year old woman.
 A Few Observations on Gastrointestinal Stromal Tumors and Their Differential Diagnosis E. Montgomery A 9cm mass was excised from the jejunal wall and mesentery of a 33 year old woman. 1 2 3 CD117/c-kit
A Few Observations on Gastrointestinal Stromal Tumors and Their Differential Diagnosis E. Montgomery A 9cm mass was excised from the jejunal wall and mesentery of a 33 year old woman. 1 2 3 CD117/c-kit
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
Rectal biopsy as an aid to cancer control in ulcerative colitis
 Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Primary mucinous adenocarcinoma developing in an ileostomy stoma
 Gut, 1988, 29, 1607-1612 Primary mucinous adenocarcinoma developing in an ileostomy stoma P J SMART, S SASTRY, AND S WELLS From the Departments of Histopathology and Surgery, Bolton General Hospital, Fan
Gut, 1988, 29, 1607-1612 Primary mucinous adenocarcinoma developing in an ileostomy stoma P J SMART, S SASTRY, AND S WELLS From the Departments of Histopathology and Surgery, Bolton General Hospital, Fan
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Commonly Encountered Neuro-Endocrine Tumors of the Gut
 Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Endoscopic Corner CASE 1. Sirimontaporn N Klaikaew N Imraporn B Rerknimitr R
 Endoscopic Corner Sirimontaporn N, et al. THAI J GASTROENTEROL 2010 Vol. 11 No. 3 Sept. - Dec. 2010 171 Sirimontaporn N Klaikaew N Imraporn B Rerknimitr R CASE 1 A 47- year-old female presented to the
Endoscopic Corner Sirimontaporn N, et al. THAI J GASTROENTEROL 2010 Vol. 11 No. 3 Sept. - Dec. 2010 171 Sirimontaporn N Klaikaew N Imraporn B Rerknimitr R CASE 1 A 47- year-old female presented to the
Upper GIT IV Gastric cancer
 Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Unexpected Findings at Endoscopy
 The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
Pancreas. Atrophy, acinar cell. Pathogenesis: Diagnostic key features:
 Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Subepithelial Lesions of the Gut: When Should I Worry?
 Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract
 Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
EDUCATIONAL CASES E1 & E2. Natasha Inglis 20/03/15
 EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
Scholars Journal of Applied Medical Sciences (SJAMS)
") Scholars Journal of Applied Medical Sciences (SJAMS) Abbreviated Key Title: Sch. J. App. Med. Sci. Scholars Academic and Scientific Publisher A Unit of Scholars Academic and Scientific Society, India www.saspublisher.com
Scholars Journal of Applied Medical Sciences (SJAMS) Abbreviated Key Title: Sch. J. App. Med. Sci. Scholars Academic and Scientific Publisher A Unit of Scholars Academic and Scientific Society, India www.saspublisher.com
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
Mesenchymal neoplasms of the gastrointestinal tract what s new? Newton ACS Wong Department of Histopathology Bristol Royal Infirmary
 Mesenchymal neoplasms of the gastrointestinal tract what s new? Newton ACS Wong Department of Histopathology Bristol Royal Infirmary Talk plan Summary from 2010 talk. What s happened since 2010. GISTs
Mesenchymal neoplasms of the gastrointestinal tract what s new? Newton ACS Wong Department of Histopathology Bristol Royal Infirmary Talk plan Summary from 2010 talk. What s happened since 2010. GISTs
GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY
 Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
Neoplasia 18 lecture 6. Dr Heyam Awad MD, FRCPath
 Neoplasia 18 lecture 6 Dr Heyam Awad MD, FRCPath ILOS 1. understand the role of TGF beta, contact inhibition and APC in tumorigenesis. 2. implement the above knowledge in understanding histopathology reports.
Neoplasia 18 lecture 6 Dr Heyam Awad MD, FRCPath ILOS 1. understand the role of TGF beta, contact inhibition and APC in tumorigenesis. 2. implement the above knowledge in understanding histopathology reports.
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on
 Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
Rare GI Malignancies
 Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Case Presentations: Gastric Polyps and The Company They Keep. Elizabeth Montgomery, MD Department of Pathology Johns Hopkins Hospital Baltimore MD
 Case Presentations: Gastric Polyps and The Company They Keep Elizabeth Montgomery, MD Department of Pathology Johns Hopkins Hospital Baltimore MD Case 1 A 68 year old woman with dyspepsia underwent upper
Case Presentations: Gastric Polyps and The Company They Keep Elizabeth Montgomery, MD Department of Pathology Johns Hopkins Hospital Baltimore MD Case 1 A 68 year old woman with dyspepsia underwent upper
Stage 4 gastric adenocarcinoma icd 10
 > Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
> Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Duodenal adenomas Management. Dr Stratis Alexandridis Consultant Gastroenterologist BRI
 Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Proceedings of the 36th World Small Animal Veterinary Congress WSAVA
 www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
Gastrointestinal stromal tumours - clinicopathological study
 Original research article Gastrointestinal stromal tumours - clinicopathological study *Dr. Putrevu Venkata Gurunadha Raju, ** Dr. Kanwaljit Kaur *Professor, **Assistant Professor Department of Pathology,
Original research article Gastrointestinal stromal tumours - clinicopathological study *Dr. Putrevu Venkata Gurunadha Raju, ** Dr. Kanwaljit Kaur *Professor, **Assistant Professor Department of Pathology,
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Pathology of the oesophagus and the stomach. Neil A Shepherd Gloucester, UK. Bristol Pathology 1 st Year Training School, The layers of the GI tract
 Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
In-situ and invasive carcinoma of the colon in patients with ulcerative colitis
 Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease
 Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Gastro Intestinal Pathology
 Duration: 04 weeks (20 days) Gastro Intestinal 3/SBM-4/01 Alimentation in health Topic/ Concept Objectives Time Dept. 1. recall digestion, absorption and metabolism relating to, carbohydrates, proteins,
Duration: 04 weeks (20 days) Gastro Intestinal 3/SBM-4/01 Alimentation in health Topic/ Concept Objectives Time Dept. 1. recall digestion, absorption and metabolism relating to, carbohydrates, proteins,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
Brief History. Identification : Past History : HTN without regular treatment.
 Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
What is your diagnosis? a. Lymphocytic colitis. b. Collagenous colitis. c. Common variable immunodeficiency (CVID) associated colitis
 associated colitis") Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
number Done by Corrected by Doctor مها شوماف
 number 15 Done by Ali Yaghi Corrected by Waseem Alhaj Doctor مها شوماف 1 P a g e Epidemiology Epidemiology is the study of the incidence of a disease. It can give us information about the possible causes
number 15 Done by Ali Yaghi Corrected by Waseem Alhaj Doctor مها شوماف 1 P a g e Epidemiology Epidemiology is the study of the incidence of a disease. It can give us information about the possible causes
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Histo-Meeting
 Histo-Meeting 23.10.2013 Index Cap polyps Crohn s disease Stomach resection Gastric MALT lymphoma Cloacogene polyp of the rectum Histo-Meeting October 23, 2013 2 53 year old male patient 1. Neurofibromatosis
Histo-Meeting 23.10.2013 Index Cap polyps Crohn s disease Stomach resection Gastric MALT lymphoma Cloacogene polyp of the rectum Histo-Meeting October 23, 2013 2 53 year old male patient 1. Neurofibromatosis
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
BowelGene. How do I know if I am at risk? Families with hereditary bowel cancer generally show one or more of the following clues:
 BowelGene BowelGene What is hereditary bowel cancer? Bowel cancer (also known as colorectal cancer) is the fourth most common cancer in the UK. Unfortunately 1 in 19 women and 1 in 14 men will develop
BowelGene BowelGene What is hereditary bowel cancer? Bowel cancer (also known as colorectal cancer) is the fourth most common cancer in the UK. Unfortunately 1 in 19 women and 1 in 14 men will develop
Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum
 Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Endoscopic techniques for surveillance and treatment of FAP
 Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה
 ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
GI Polyp syndromes in children. Screening and surveillance, surgery.
 Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare Objectives Understand
Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare Objectives Understand
Imaging of Gastrointestinal Stromal Tumors (GIST) Amir Reza Radmard, MD Assistant Professor Shariati hospital Tehran University of Medical Sciences
 Amir Reza Radmard, MD Assistant Professor Shariati hospital Tehran University of Medical Sciences") Imaging of Gastrointestinal Stromal Tumors (GIST) Amir Reza Radmard, MD Assistant Professor Shariati hospital Tehran University of Medical Sciences Describe the typical imaging findings of GIST at initial
Imaging of Gastrointestinal Stromal Tumors (GIST) Amir Reza Radmard, MD Assistant Professor Shariati hospital Tehran University of Medical Sciences Describe the typical imaging findings of GIST at initial
polyps of the colon and rectum
 J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
what is the alternative mechanism of histogenesis? Aspects of the morphology of the adenomacarcinoma Morphology of the
 Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Tumors of the Intestines. Malignant Lesion. Adenocarcinoma. sessile Serrated Adenomas
 Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
A 50 year old female with no significant past medical history presented for a routine screening colonoscopy. The patient reported only symptoms of
 A 50 year old female with no significant past medical history presented for a routine screening colonoscopy. The patient reported only symptoms of reflux. She had no family history of colorectal cancer
A 50 year old female with no significant past medical history presented for a routine screening colonoscopy. The patient reported only symptoms of reflux. She had no family history of colorectal cancer
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
Update on the pathological classification of gastritis. Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada
 Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon