The pathology of neuroendocrine tumours of the gut
|
|
|
- Brenda Pope
- 5 years ago
- Views:
Transcription
1 The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May
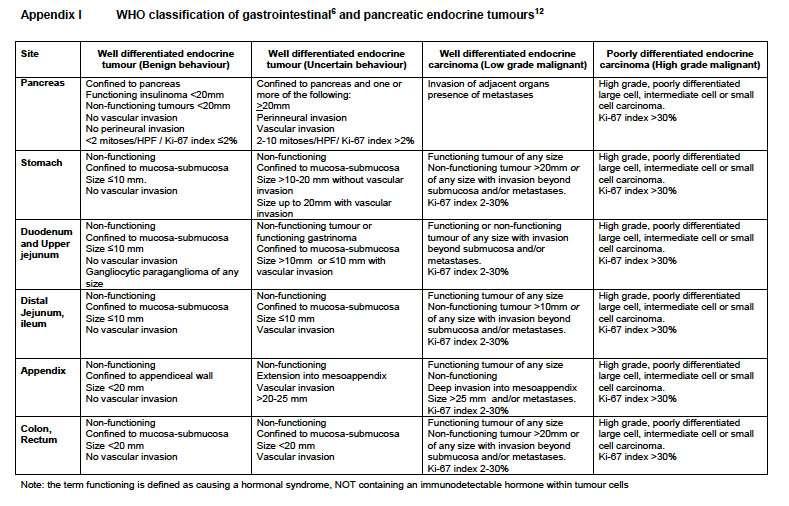
2 The pathology of neuroendocrine tumours (NETs) of the gut: general comments site in the GI tract has a profound influence on the morphology, natural history, hormone elaboration, management & prognosis of NETs grade is an important factor in treatment and prognosis and is an important assessment. This is largely determined by proliferative activity and the Ki67/MIB1 score there is a lack of international conformity about classification with the terms neuroendocrine tumour, endocrine tumour and carcinoid all still being used around the world (WHO and ENETS have different classifications) useful information is available in the Royal College datasets and guidelines at: /G081_DatasetGIEndocrine_Sep12.pdf
3 The clinico-pathological spectrum endocrine cell hyperplasia pure neuro-endocrine cell neoplasms low grade, well differentiated neuro-endocrine tumours (formerly carcinoids) high grade poorly differentiated neuro-endocrine carcinomas (small cell and large cell types) mixed tumours carcinomas of mixed neuro-endocrine and non-endocrine type (MANECs)
4 Markers argentaffin: Masson-Fontana (enterochromaffin cells) argyrophil: Grimelius Churukian-Schenk Sevier-Munger Hellerstrom-Hellman immunohistochemistry in-situ hybridisation
 secretory granule associated")
5 Immunostaining cytosol / cell membrane: neurone specific enolase PGP 9.5 CD56, CD99 small vesicle associated markers: synaptophysin SV2 (synaptic vesicle protein 2) secretory granule associated markers: chromogranins A & B Leu-7 (CD57) peptide hormones
6 Upper GI neuro-endocrine tumours well differentiated neuro-endocrine tumour - benign non-functioning, <1 cm, within mucosa-submucosa no angioinvasion well differentiated neuro-endocrine tumour - borderline non-functioning, 1-2 cm, within mucosa-submucosa no angioinvasion well differentiated neuro-endocrine carcinoma any functioning tumour any tumour with angioinvasion or invading beyond submucosa >2 cm poorly differentiated neuro-endocrine carcinoma intermediate or small cell carcinoma
7 Lower GI neuro-endocrine tumours well differentiated neuro-endocrine tumour - benign non-functioning, <2 cm, within mucosa-submucosa, no angioinvasion well differentiated neuro-endocrine tumour - borderline non-functioning, <2 cm, within mucosa-submucosa with angioinvasion well differentiated neuro-endocrine carcinoma any functioning tumour any tumour >2cm or invading beyond submucosa poorly differentiated neuro-endocrine carcinoma intermediate or small cell carcinoma
8
9 Pape UF et al. Cancer 2008; 113:
10
11

12 Upper GI tumours Pape UF et al. Cancer 2008; 113:
13

 Maru D et al.")
14 Oesophageal neuro-endocrine tumours uncommon, usually in distal oesophagus very rare well differentiated NETs arising in a background of Barrett s oesophagus majority are bulky G3 neuro-endocrine carcinomas of small cell type synaptophysin > chromogranin express TTF-1 some are admixed with in situ or invasive squamous or adenocarcinoma (MANEC) Maru D et al. Am J Surg Pathol 2008; 32:
15 Oesophageal NETs prognosis worse for pure neuroendocrine carcinomas than for mixed tumours no difference in survival of pure small cell and large cell Maru D et al. Am J Surg Pathol 2008; 32:
16 Neuro-endocrine cells of the stomach A ghrelin corpus EC serotonin antrum & corpus D somatostatin antrum & corpus ECL histamine corpus X, D1, P endothelin (X) corpus G gastrin antrum
17 Enterochromaffin-like (ECL) cells ~40% of neuro-endocrine cells of gastric corpus mucosa argyrophil but non-argentaffin chromogranin A-positive vesicular granules on electron microscopy contain histamine histidine decarboxylase vesicular monoamine transporter 2 - VMAT-2 secrete histamine in response to gastrin and PACAP (pituitary adenylyl cyclase activating peptides) proliferation induced by hypergastrinaemia
18 ECL-cell tumours in hypergastrinaemia chronic atrophic gastritis (type I) Zollinger-Ellison syndrome (type II) defective parietal cell function (type IV) sporadic ECL-cell (Type III)
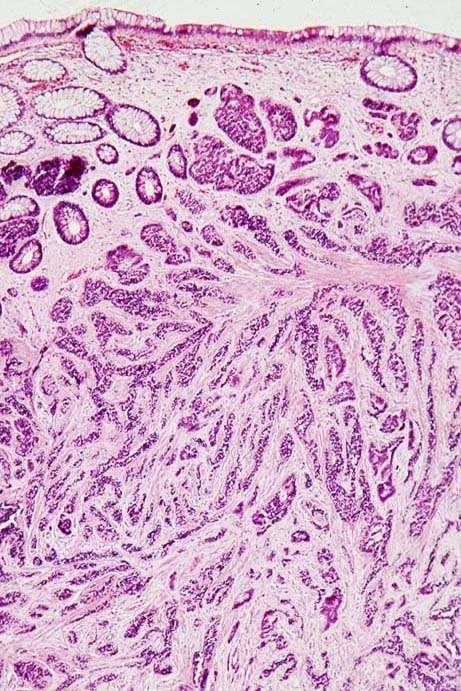
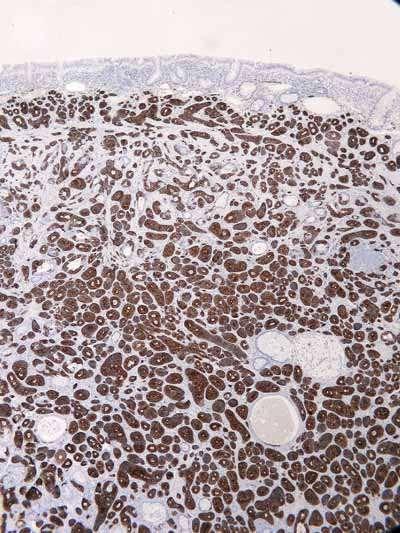
19 chronic atrophic gastritis intragastric hypoacidity antral G cells hypergastrinaemia corpus ECL-cell hyperplasia corpus ECL-cell dysplasia corpus ECL-cell neuro-endocrine tumours
20 ECL cell lesions in the stomach hyperplasia simple linear linear sequences of 5 or more cells micronodular 5 or more in clusters <150 µm dysplasia nodules µm, fusion, stromal response invasive neuro-endocrine tumour >500 µm, submucosal invasion

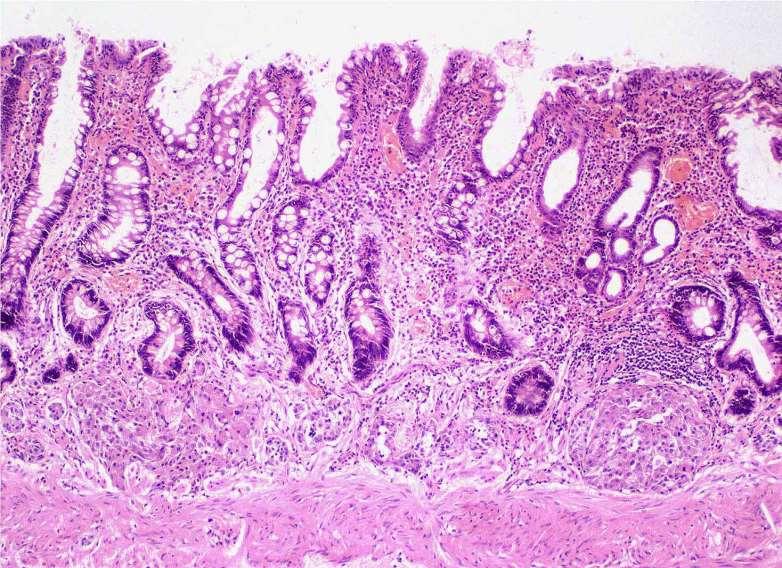
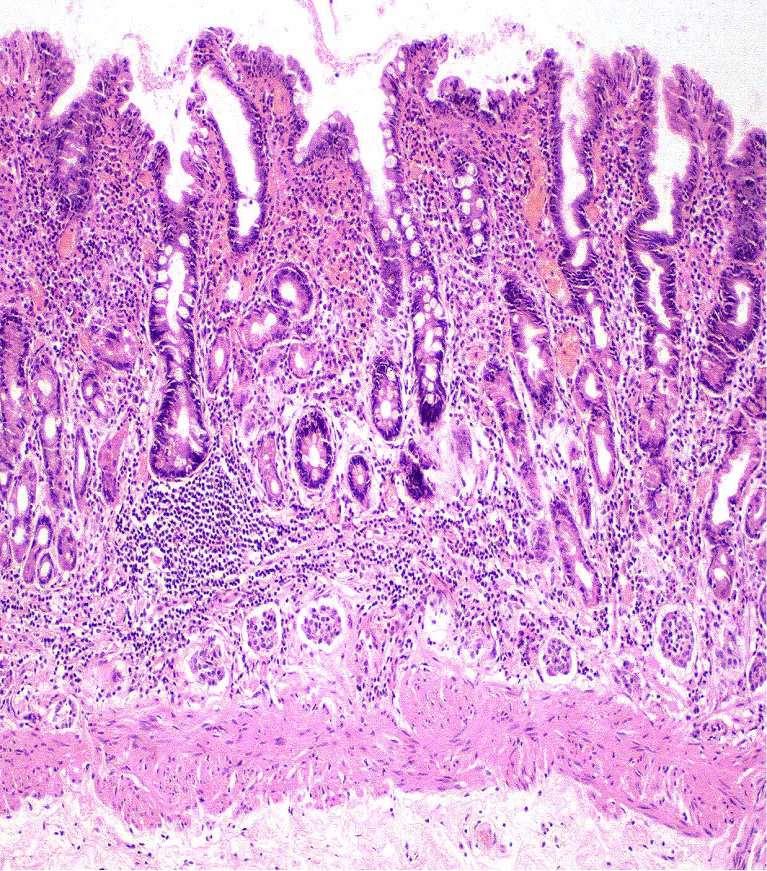
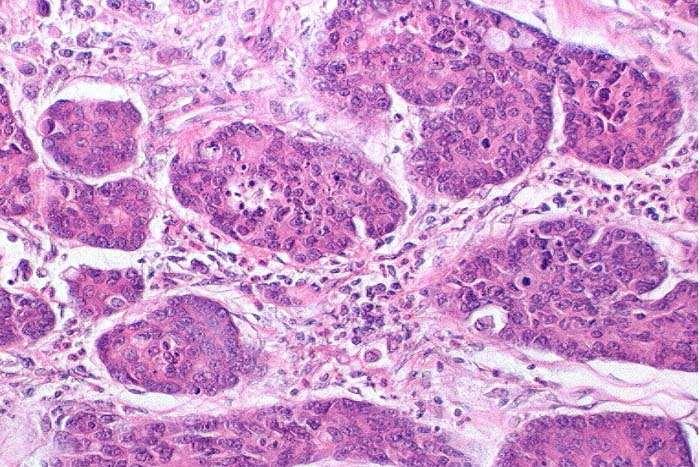
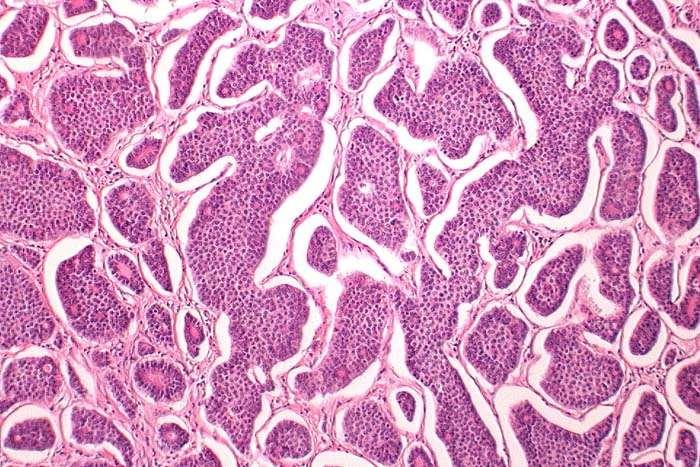
21 Neuroendocrine pathology in chronic atrophic gastritis
22
23
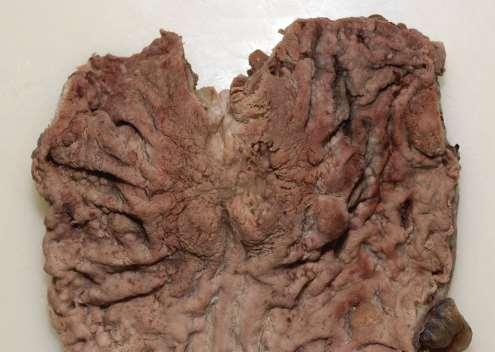
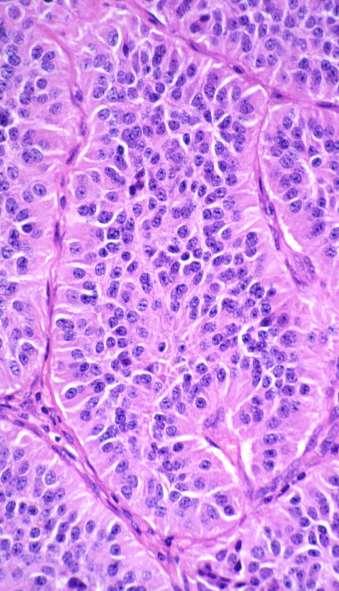
24 Type 1: ECL-cell tumours in chronic atrophic gastritis small (77% <1cm) polypoid multiple grade 1 confined to mucosa/submucosa (93%) slow-growing metastasis uncommon (5% LN) and not fatal
25 Management of type 1 ECL-cell tumours staging (EUS/CT) treat vitamin deficiencies, eradicate HP if present endoscopic polypectomy for raised lesions antrectomy and local excision for large (>1 cm) or numerous tumours gastrectomy only for tumours with clear-cut malignant features endoscopic follow-up ablation of new lesions surveillance for adenocarcinoma completion gastrectomy as last resort?? octreotide Gladdy RA et al. Ann Surg Oncol 2009; 16:

26 Type II ECL-cell tumours in Zollinger-Ellison syndrome hypertrophic oxyntic glands all patients have linear ECL-cell hyperplasia nodular ECL-cell hyperplasia and ECL-cell tumours are virtually confined to those who have underlying MEN-1 Solcia E et al. Am J Surg Pathol 1990; 14:
27 G cell tumour hypergastrinaemia corpus ECL-cell hyperplasia corpus ECL-cell dysplasia corpus ECL-cell neuro-endocrine tumours
28 Type II ECL-cell tumours in MEN 1 present in 13-30% of cases small (75% <1.5 cm) polypoid multiple grade 1 confined to mucosa/submucosa slow-growing metastasis unusual (30% LN) and rarely fatal
29 Management treat primary condition and investigate family eradicate HP if present endoscopic polypectomy for raised lesions local excision for large (>1 cm) or numerous tumours consider gastrectomy only for tumours with clear-cut malignant features endoscopic follow-up and ablation of new lesions completion gastrectomy as last resort?? octreotide
30 Type IV ECL-cell tumours spectacularly rare no gastritis no gastrinoma, ZE syndrome or MEN1 ECL -cell hyperplasia, dysplasia, multiple invasive tumours hypertrophic, distended oxyntic glands containing inspissated eosinophilic material hyperplastic vacuolated parietal cells ciliated metaplasia Ooi A et al (1995) Endocrine Pathol 3: 229 Abraham SC et al (2005) Am J Surg Pathol 29:969-75
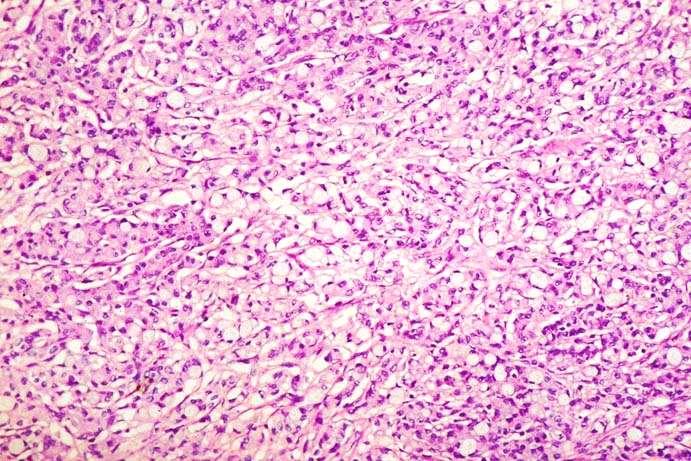
31 Sporadic (type III) gastric NETs 13% of all gastric neuro-endocrine tumours males > females mainly corpus and of ECL-cell or X-cell type (antral G-cell or EC-cell tumours rare) no background ECL-cell hyperplasia usually solitary (but multiple polyps described) often have features of gastric carcinoma may produce a flushing syndrome (histamine) Rindi G et al. Gastroenterology 1993; 104:
32 Sporadic (type III) gastric NETs usually >2cm frequently deeply invasive carcinomas 76% muscularis propria 53% serosa frequently metastatic (LN 71%; distant 69%) significant mortality (27%) mean survival 28 months

33 Sporadic (type III) gastric NETs typically G2 tumours but some are G3 neuro-endocrine carcinomas usually large cell type vesicular nuclei, large nucleoli sometimes atypical mitoses may have a scirrhous pattern >10% Ki67 labelling index necrosis p53 expression Jiang S-X et al. Am J Surg Pathol 2006; 30:
34
35 Management small (<1cm), well differentiated G1 tumours, confined to submucosa without angioinvasion polypectomy confirm favourable histology and complete excision remainder gastrectomy
 are very uncommon endocrine component is usually grade 3 manage as conventional adenocarcinomas (similar prognosis)")
36 Gastric mixed tumours (MANECs) although gastric adenocarcinomas frequently contain neuro-endocrine cells, they rarely account for >30% AB/PAS) MANECs (by WHO criteria) are very uncommon endocrine component is usually grade 3 manage as conventional adenocarcinomas (similar prognosis) chromogranin

37 An important case 64 F. Polyp with superficial ulcer in stomach. not Gloucestershire slides!

38 64 F. Polyp with superficial ulcer in stomach.


39 64 F. Polyp with superficial ulcer in stomach. cytokeratin


40 64 F. Polyp with superficial ulcer in stomach. Here comes the total gastrectomy..


41 64 F. Polyp with superficial ulcer in stomach. Here comes the total gastrectomy.. synaptophysin


42 NET v carcinoma Four types of gastric chronic atrophic Zollinger-Ellison syndrome sporadic intrinsic abnormality of parietal cells The first is the commonest, is benign (unless..) and treated very conservatively (EMR/ER/surveillance)



43 Context in gastrointestinal NETs Rectum Stomach Stomach

44 Beware, though!
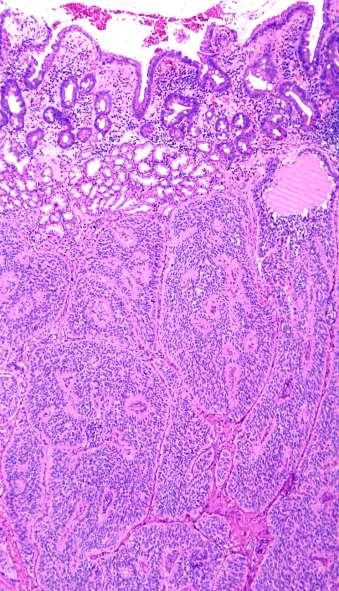
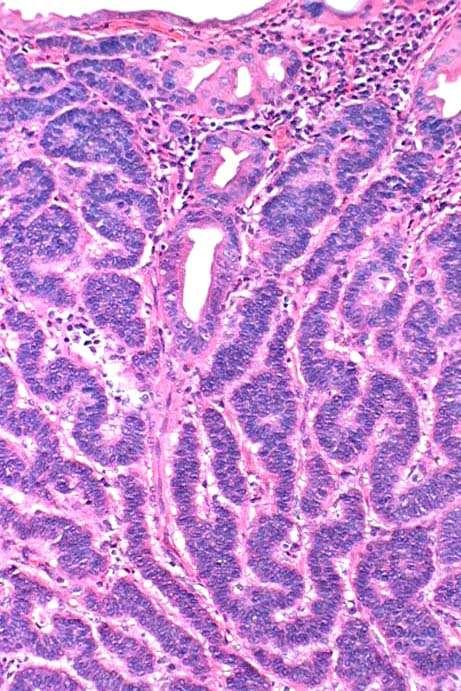
45 Differentiated duodenal neuro-endocrine tumours classical neuro-endocrine cell tumours: G cell, argyrophil, gastrin-containing EC cell, argentaffin, serotonin-containing A and B cell (glucagon and insulin) very rare tumours of unusual morphology: D cell, variably argyrophil, somatostatin-containing gangliocytic paraganglioma
 can be very small and difficult")
46 Duodenal G-cell NET commonest duodenal neuro-endocrine tumours proximal duodenum usually small (<1cm) and G1, occasionally G2 trabecular pattern, may contain amyloid 1/3 functional (ZE syndrome) can be very small and difficult to detect
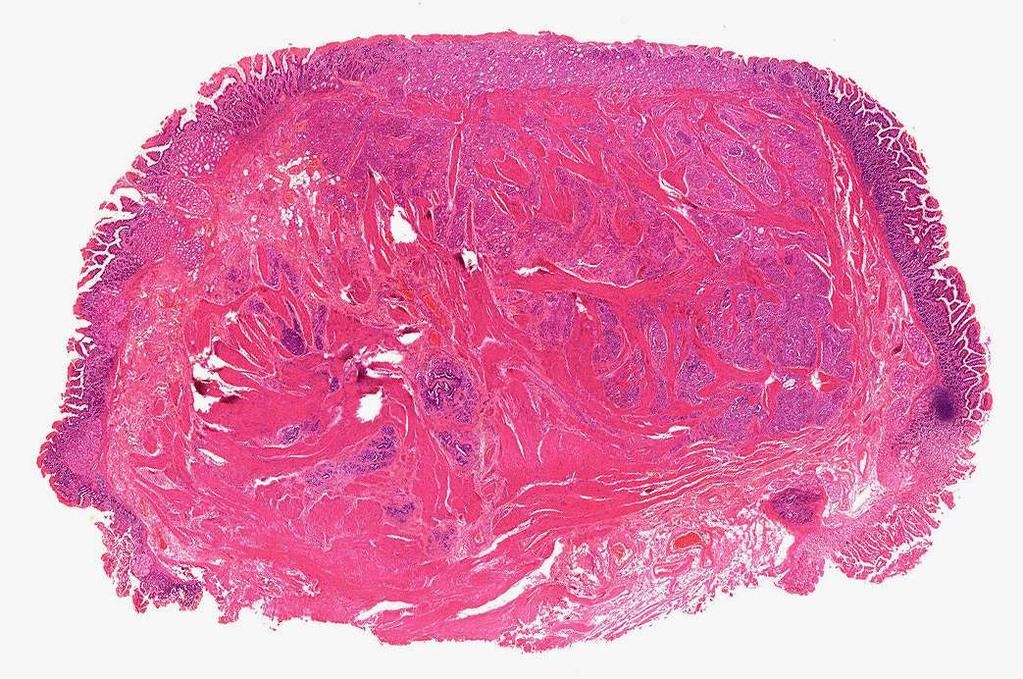
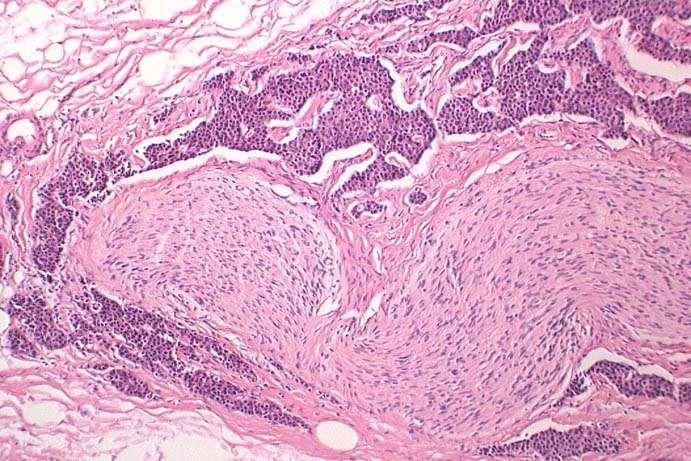
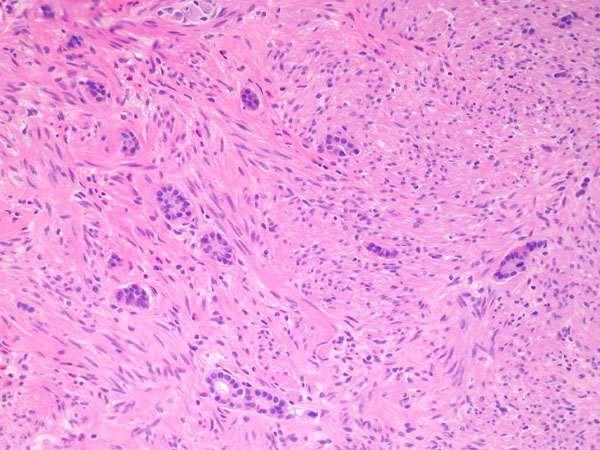
47
48 Duodenal G-cell NETs non-functional tumours usually benign behaving functional tumours have long natural history: lymph node metastases (often larger than primary) common if functional liver metastases late and rare prognosis with metastatic disease good with acid suppression or octreotide

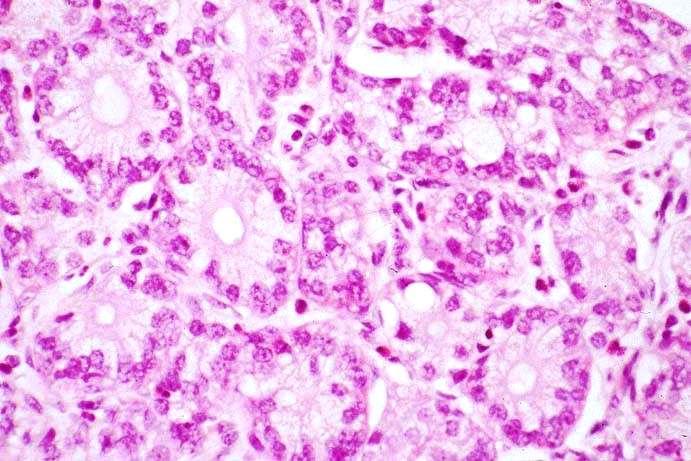
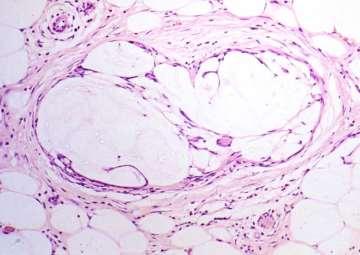
49 Duodenal D-cell tumours 15-20% of duodenal neuro-endocrine tumours periampullary (haemorrhage, jaundice, pancreatitis) small intramural or polypoid tumours contain somatostatin always non-functional ~ 50% have type 1 neurofibromatosis <1% of NF-1 patients have duodenal tumours Garbrecht N et al. Endocr Relat Cancer 2008; 15:
50


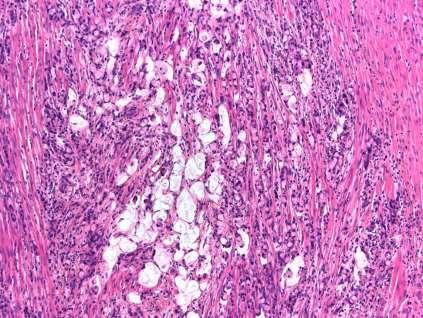
51 Is this pancreatic adenocarcinoma or metastatic prostatic carcinoma?
52 PAS PAS
53

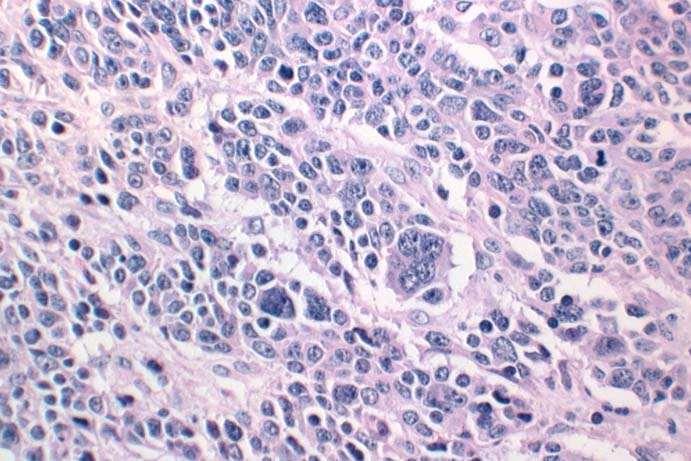
54

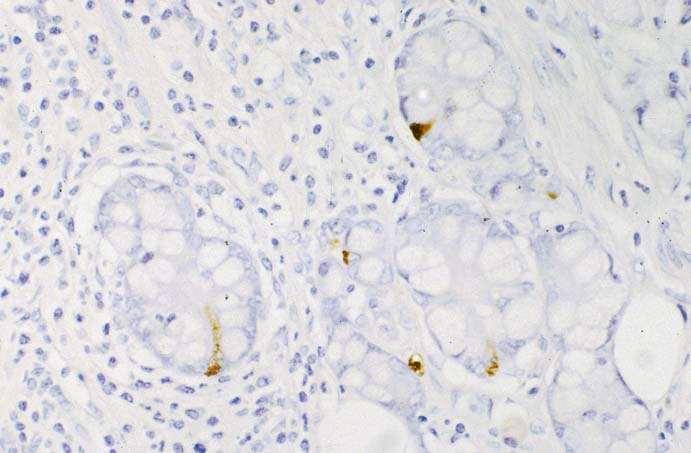
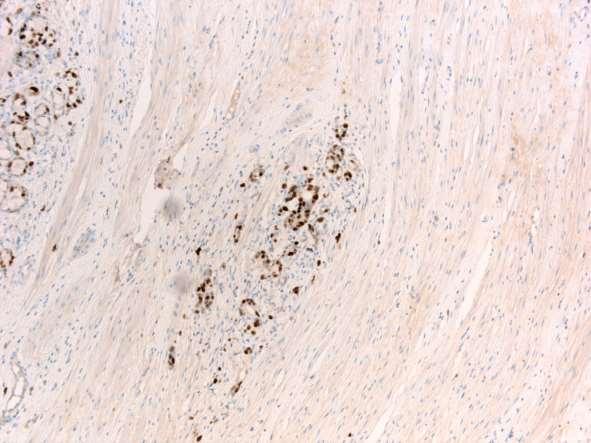
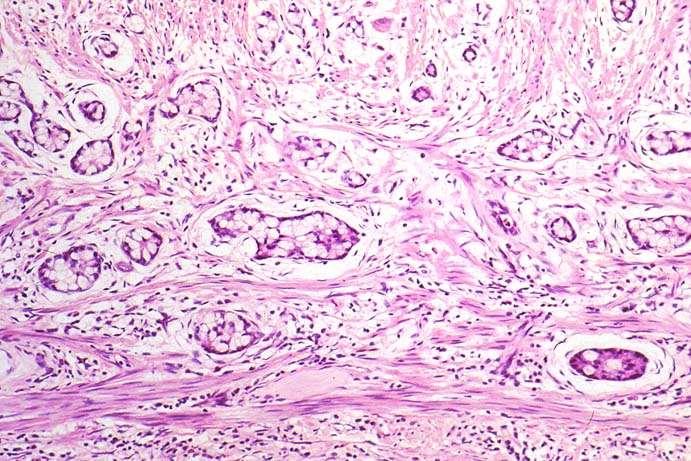
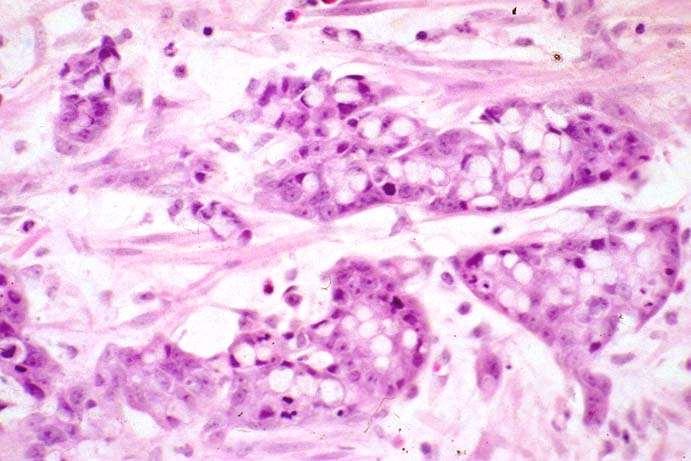
55 ? synaptophysin somatostatin
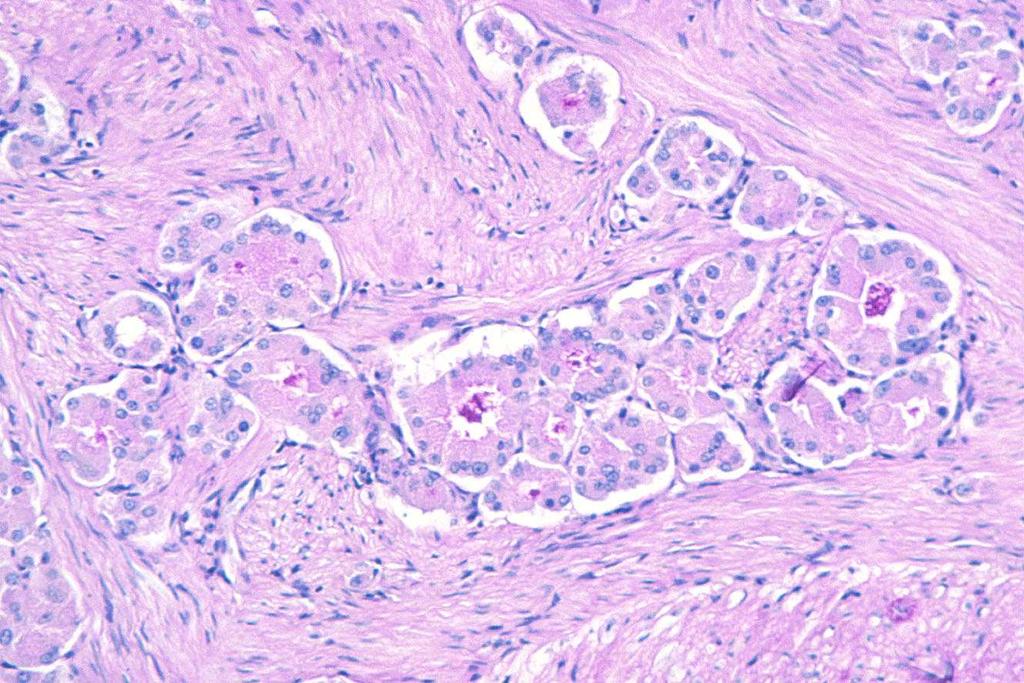
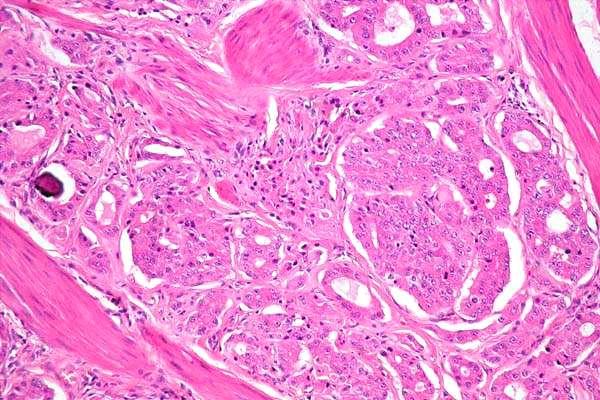
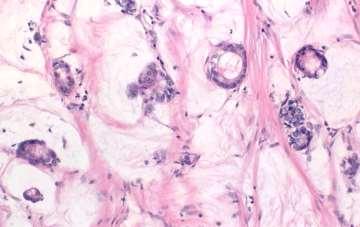
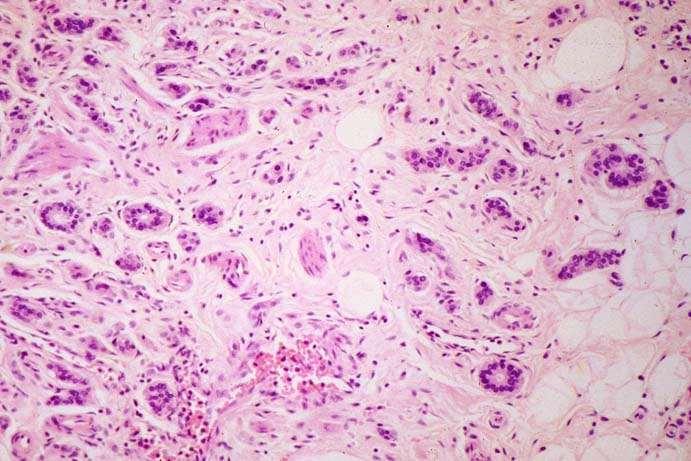
56 Duodenal D-cell NETs glandular architecture PAS-positive luminal cell borders psammoma bodies non-argentaffin non-argyrophil by Grimelius synaptophysin positive usually chromogranin A positive somatostatin positive
 distant metastasis very uncommon very good prognosis after local")
57 Duodenal D-cell NETs tumours of low grade malignancy lymph node metastasis in 25% (usually in larger tumours) distant metastasis very uncommon very good prognosis after local excision
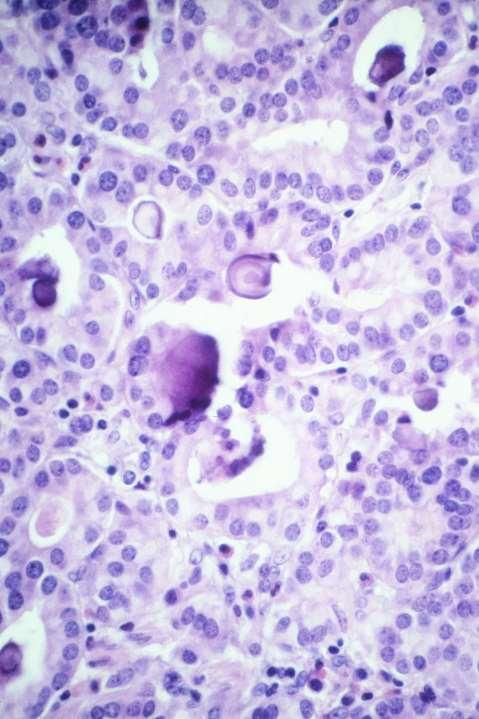
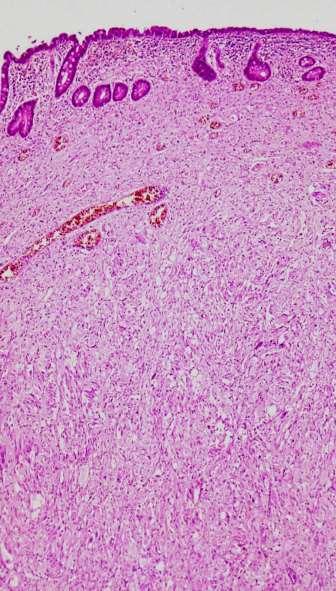
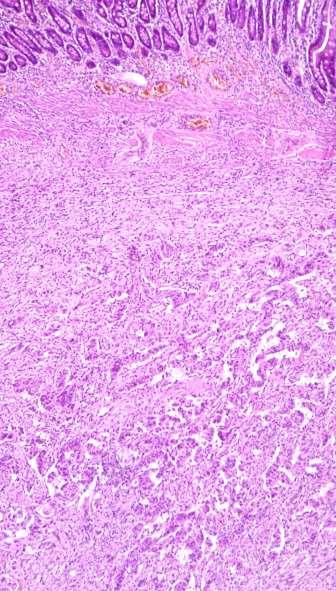
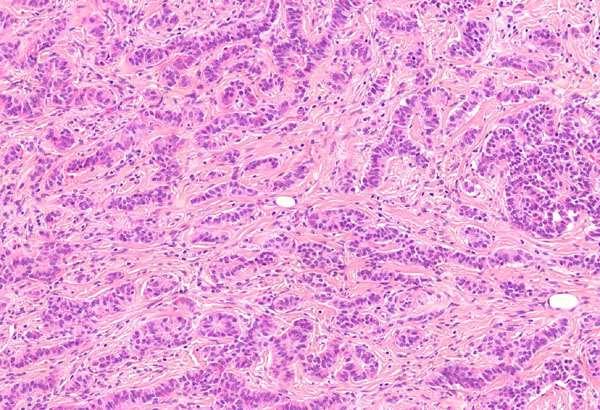
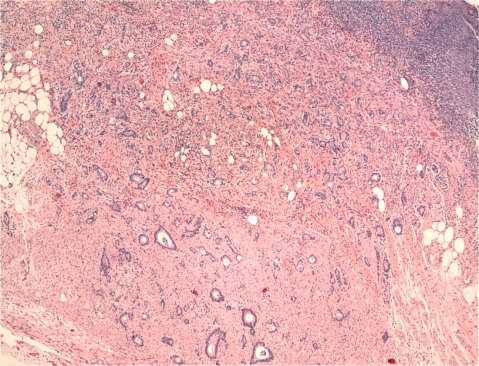
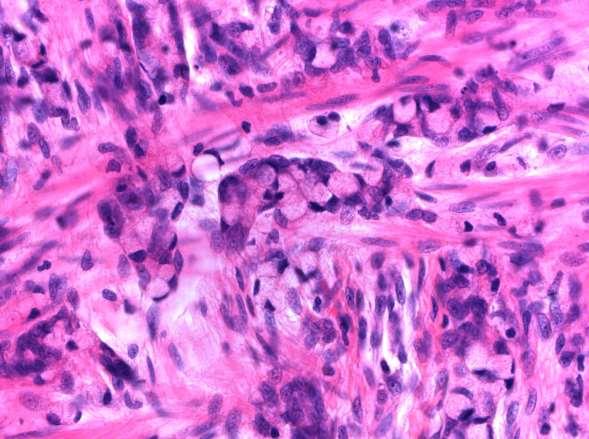
58 Gangliocytic paraganglioma periampullary (haemorrhage, jaundice, pancreatitis) solitary intramural or polypoid tumours Up to 7cm any age always non-functional benign behaving (though rare LN mets) occasionally found in NF-1 patients triphasic histological components Hamid QA et al. Hum Pathol 1986;17:

59
60
61

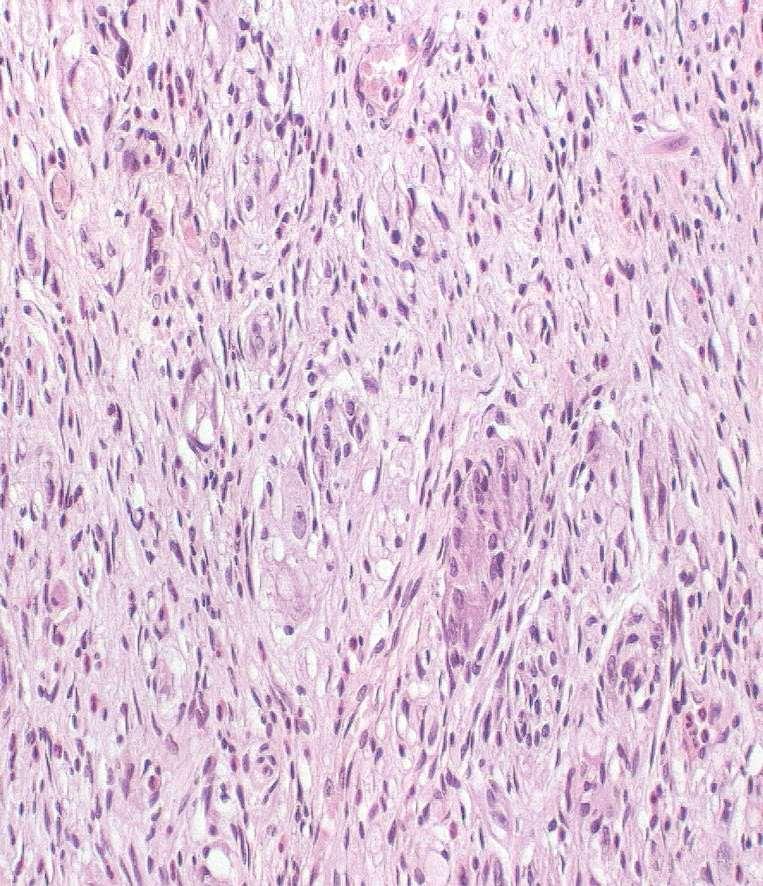
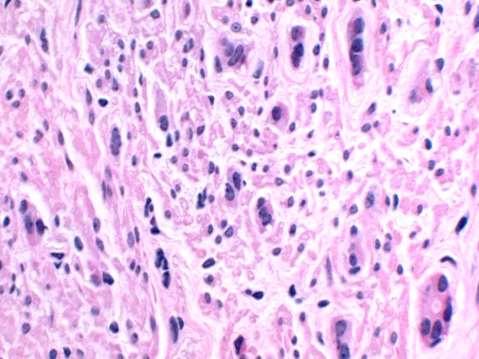
62 Gangliocytic paraganglioma spindle cells interweaving fascicles S-100 and neurofilament-positive

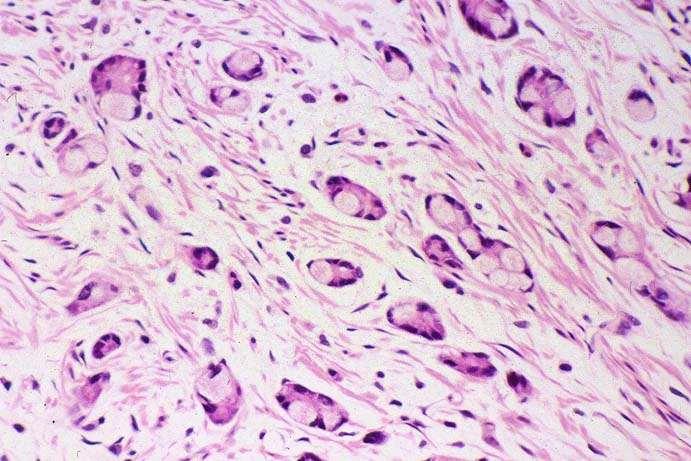
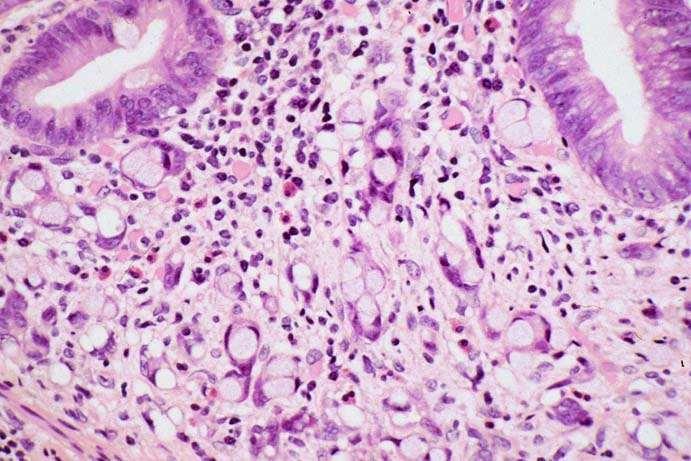
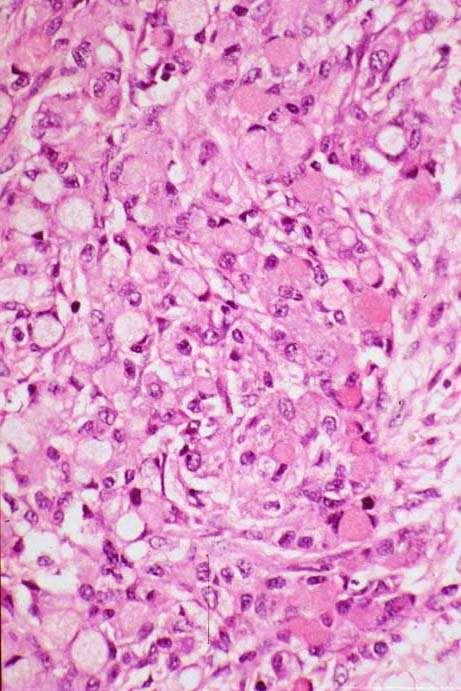
63 Gangliocytic paraganglioma spindle cells epithelioid cells nests and ribbons variably chromogranin + synaptophysin + usually contain PP, somatostatin may be psammoma bodies, amyloid synapto

64 Gangliocytic paraganglioma spindle cells epithelioid cells ganglion cells typical ganglion cells, with satellite cells, GFAP+ some merge with epithelioid cells zellballen-like arrangements



65 Duodenal neuro-endocrine carcinoma & MANEC rare large, bulky, ulcerating periampullary lesions sporadic small cell and large cell extensive necrosis metastases at presentation in 92% mean survival 8 months chromogranin A synaptophysin
66 Jejunal & ileal NETS EC-cell tumours contain serotonin and substance P classical argentaffin carcinoid pattern majority G1 (G3 neuro-endocrine carcinoma does not occur at this site) mutation and/or LOH of MEN1 gene (11q13) multiple in ~25% (worse outcome) multiple tumours are usually spread from a single tumour (X-chromosome inactivation analysis) sometimes EC-cell hyperplasia but not familial Guo et al, 2000
67
68

69
70 Ileal neuro-endocrine tumours incidental finding obstruction/intussusception haemorrhage carcinoid syndrome when liver metastases or very bulky intraperitoneal disease intestinal ischaemia related to mesenteric sclerosis
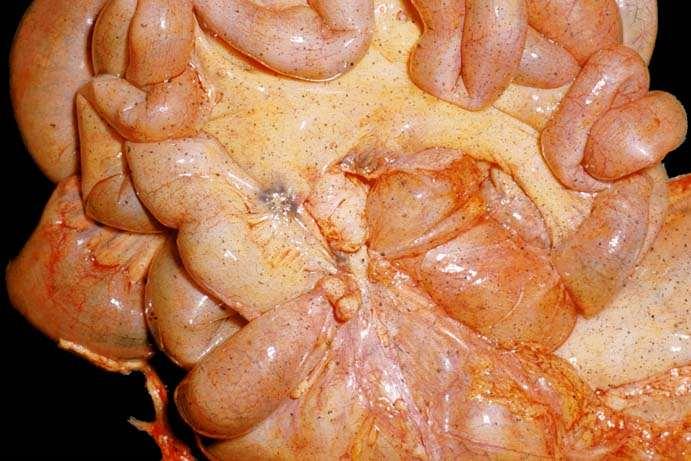
71
72
73 Behaviour of ileal NETs progression slow 5 year survival ~50% related to: metastases (liver, lymph node) size (>2 cm) angioinvasion G2 (Ki67 > 2%) unrelated to: depth of invasion multiplicity post-operative therapy partly governed by grade Dhall G et al. Hum Pathol 2012; 43:
74 Appendiceal neuro-endocrine tumours EC-cell tumours L-cell tumours goblet cell carcinoids and/or MANECs
75 Appendiceal neuro-endocrine tumours EC-cell tumours: 90% acinar, clear-cell, balloon-cell patterns grade 1 argentaffin, chromogranin A +ve contain serotonin and substance P may contain S-100-positive Schwann-like cells

76



77 acinar balloon cell EC-cell tumours clear cell
78 Appendiceal neuro-endocrine tumours L-cell tumours: 5-10% trabecular or tubular grade 1 non-argentaffin but argyrophil often chromogranin A-negative contain enteroglucagons, PP or PYY may be misdiagnosed as goblet cell carcinoid or metastatic carcinoma (esp breast)
79 no intracytoplasmic mucin L-cell tumours
80 G1 appendiceal neuro-endocrine tumours metastasis uncommon but related to tumours >2 cm or with deep mesoappendiceal invasion BUT virtually all metastatic tumours present at original surgery right hemicolectomy is recommended when involvement of the resection margin deep (>3mm) mesoappendiceal invasion tumour size >2cm Plockinger U et al. Neuroendocrinology 2008; 87:
81 Goblet cell carcinoid females > males incidental or appendicitis often diffuse growth pattern may coexist with adenomas or conventional neuro-endocrine tumours propensity for transcoelomic spread, especially to ovary lymph node and liver metastases relatively unusual 11% have distant metastases at presentation 75% overall 5 year survival
82 Goblet cell carcinoid mixed tumour composed of: - mucous cells - enterocytes/colonocytes - endocrine cells (EC-cells or L-cells) - Paneth cells now regarded as MANEC by WHO and considered under adenocarcinoma of the appendix
83
84 synaptophysin
85 Clinical history 60M. Previous appendicitis and mass. Conservative treatment & subsequent appendicectomy.

86
87

88
89 Ki67/MIB1
90 Adenocarcinoma ex-goblet cell carcinoid
91 Tang classification for the natural history and prognosis of goblet cell carcinoids of the appendix
92 Goblet cell carcinoid / MANEC 20-30% have aggressive features nuclear pleomorphism >2/10 hpf mitoses solid sheets fused cribriform glands single file structures diffusely infiltrating signet ring cells conversely those on the benign end of the spectrum have a good prognosis, especially if small and confined to the appendix Tang LH et al. Am J Surg Pathol 2008; 32:

93
94 Management of goblet cell carcinoid/manec Right hemicolectomy with bilateral salpingo-oophorectomy except when, after extensive histological evaluation, tumour is < 10mm low grade (<2 mitoses/10 HPF) localised to appendiceal wall with no caecal, mesoappendiceal or serosal invasion Plockinger U et al. Neuroendocrinology 2008; 87:
95 Colorectal neuro-endocrine tumours grade 1-2 EC-cell tumours: usually in caecum and ascending colon argentaffin, contain serotonin and substance P grade 1-2 L-cell tumours: usually in rectum trabecular and argyrophil often chromogranin A negative but synaptophysin and SV2 positive contain enteroglucagons, glicentin, PP or PYY minor components of other peptides prostatic acid phosphatase (but not PSA) positive
96 Colorectal neuro-endocrine tumours proximal tumours larger than rectal tumours may arise in long-standing ulcerative colitis virtually never functioning apart from very rare carcinoid syndrome with EC cell tumours
97 synaptophysin
98
99 Colorectal neuro-endocrine tumours behaviour related to: size stage grade 78% metastatic tumours >2 cm 8% tumours <2 cm metastasised <3% tumours <1 cm metastasised 46% tumours invading muscularis propria metastasised
100 Management of colorectal neuro-endocrine tumours endoscopic resection for G1, T1a lesions small (<10mm) confined to mucosa/submucosa no lymphovascular invasion completely excised relatively common in the rectum remainder treated as for colorectal cancer
101 G3 colorectal neuro-endocrine carcinomas and MANECs bulky, rapidly growing masses large cell mostly in proximal colon and may be admixed with conventional adenocarcinoma small cell mostly in distal rectum/anal canal, sometimes admixed with squamous cell carcinoma virtually never functional usually positive for synaptophysin may arise in adenomas or in chronic UC median survival 5 months Gaffey MJ et al. Am J Surg Pathol 1990; 14:

102
103 The pathology of neuroendocrine tumours of the gut: take home messages site in the GI tract has a profound influence on the morphology, natural history, hormone elaboration, management & prognosis of NETs grade is an important factor in treatment and prognosis and is an important assessment. This is largely determined by proliferative activity and the Ki67/MIB1 score hyperplasia from chronic hyperstimulation and/or inherited abnormalities of neuro-endocrine cell growth are sometimes important in their pathogenesis important pathological determinants are site, cell type, degree of differentiation, stage and grade clinicopathological correlation is essential in determining management and discussion in an MDTM is beneficial a dataset for pathology reporting, developed through clinical and pathological consensus, is advised
104 Thank you for listening!
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Polypoid lesions of the gastrointestinal tract
 Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
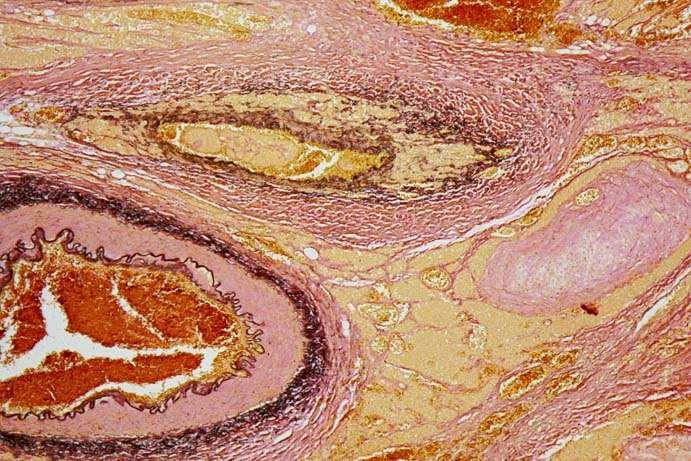
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis.
 Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
12/7/2011. Pathological mimics of malignancy in the GI tract. Professor Neil A Shepherd President, British Division of the IAP
 Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Unexpected Findings at Endoscopy
 The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract
 Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Original Report. Carcinoid Tumors of the Stomach: A Clinical and Radiographic Study
 Aaron J. Binstock 1 C. Daniel Johnson 1 David H. Stephens 1 Ricardo V. Lloyd 2 Joel G. Fletcher 1 Received July 25, 2000; accepted after revision September 29, 2000. 1 Department of Radiology, Mayo Clinic,
Aaron J. Binstock 1 C. Daniel Johnson 1 David H. Stephens 1 Ricardo V. Lloyd 2 Joel G. Fletcher 1 Received July 25, 2000; accepted after revision September 29, 2000. 1 Department of Radiology, Mayo Clinic,
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Appendiceal Pathology. Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016
 Appendiceal Pathology Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016 Appendicitis Appendicitis Appendicitis Scattered groups of neutrophils
Appendiceal Pathology Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016 Appendicitis Appendicitis Appendicitis Scattered groups of neutrophils
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Rare GI Malignancies
 Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs
 APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs Specimen handling and gross examination should be performed according to the Royal College of Pathologists
APPENDIX 5 PATHOLOGY 1. Handling and gross examination of gastrointestinal and pancreatic NETs Specimen handling and gross examination should be performed according to the Royal College of Pathologists
Serotonin- and Somatostatin-Positive Goblet Cell Carcinoid of the Duodenum
 2012 66 4 351 356 Serotonin- and Somatostatin-Positive Goblet Cell Carcinoid of the Duodenum a b* c c c a a b d a c b d 352 Ohara et al. received remedies at another hospital. Hematemesis then recurred
2012 66 4 351 356 Serotonin- and Somatostatin-Positive Goblet Cell Carcinoid of the Duodenum a b* c c c a a b d a c b d 352 Ohara et al. received remedies at another hospital. Hematemesis then recurred
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Commonly Encountered Neuro-Endocrine Tumors of the Gut
 Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
3/22/2017. Disclosure of Relevant Financial Relationships. Disclosure of Relevant Financial Relationships. Grading G1. Grading. Ki67 index V.
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
CASE REPORT. Introduction. Case Report. Kimitoshi Kubo 1, Noriko Kimura 2, Katsuhiro Mabe 1, Yusuke Nishimura 1 and Mototsugu Kato 1
 doi: 10.2169/internalmedicine.0842-18 Intern Med 57: 2951-2955, 2018 http://internmed.jp CASE REPORT Synchronous Triple Gastric Cancer Incorporating Mixed Adenocarcinoma and Neuroendocrine Tumor Completely
doi: 10.2169/internalmedicine.0842-18 Intern Med 57: 2951-2955, 2018 http://internmed.jp CASE REPORT Synchronous Triple Gastric Cancer Incorporating Mixed Adenocarcinoma and Neuroendocrine Tumor Completely
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Stage 4 gastric adenocarcinoma icd 10
 > Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
> Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
Proceedings of the 36th World Small Animal Veterinary Congress WSAVA
 www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
A218 : Esophagus cancer tissues. (formalin fixed)
") (formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
(formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
Type 2 gastric neuroendocrine tumor: report of one case
 Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
BC CRC Update Unusual Colorectal Tumors
 BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ.
 Professor of Surgery, Taibah Univ.") By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Pancreatic Cancer: The ABCs of the AJCC and WHO
 Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Syllabus. Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix. Appendiceal tumors. Summary provided Complete presentation
 2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a
 G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a Conventional adrenocortical neoplasm. Each of the below parameters is scored 0 when absent and 1 when present. 3 or more of these
G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a Conventional adrenocortical neoplasm. Each of the below parameters is scored 0 when absent and 1 when present. 3 or more of these
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Goblet Cell Carcinoids of the Appendix
 40 Ulster Med J 2006; 75 (1) 40-45 The Ulster Medical Journal Review Goblet Cell Carcinoids of the Appendix R Arnold, K McCallion, C McGailie Accepted 14 October 2005 INTRODUCTION Carcinoid tumours are
40 Ulster Med J 2006; 75 (1) 40-45 The Ulster Medical Journal Review Goblet Cell Carcinoids of the Appendix R Arnold, K McCallion, C McGailie Accepted 14 October 2005 INTRODUCTION Carcinoid tumours are
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
NEOPLASIA. 3. Which of the following tumour is benign a. Chondrosarcoma b. Osteochondroma c. Chondroblastoma d. Ewing s tumour e.
 NEOPLASIA 1. malignant neoplasms a. are independent of hormonal influence b. are always composed of homogenous cell lines c. arise from differentiated cells by a process of anaplasia d. display abnormal
NEOPLASIA 1. malignant neoplasms a. are independent of hormonal influence b. are always composed of homogenous cell lines c. arise from differentiated cells by a process of anaplasia d. display abnormal
Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis
 Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis ALAN P. LYSS, MD,* JOHN J. THOMPSON, MD,t AND JOHN H. GLICK, MD* F Patients with ulcerative colitis are at increased risk of
Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis ALAN P. LYSS, MD,* JOHN J. THOMPSON, MD,t AND JOHN H. GLICK, MD* F Patients with ulcerative colitis are at increased risk of
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Gastrointestinal Malignancies. Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline
 Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Tumors of the Intestines. Malignant Lesion. Adenocarcinoma. sessile Serrated Adenomas
 Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Collecting Cancer Data: GIST/NET 1/9/14
 Collecting Cancer Data: Gastrointestinal Stromal Tumor (GIST) Gastrointestinal Neuroendocrine Tumors (NET) 2013 2014 NAACCR Webinar Series January 9, 2014 Q&A Please submit all questions concerning webinar
Collecting Cancer Data: Gastrointestinal Stromal Tumor (GIST) Gastrointestinal Neuroendocrine Tumors (NET) 2013 2014 NAACCR Webinar Series January 9, 2014 Q&A Please submit all questions concerning webinar
Neoplasms of the Canine, Feline and Lemur Liver:
 Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given