PATHOLOGY OF THE SKIN 2. Tumours of the skin
|
|
|
- Dale Leonard
- 5 years ago
- Views:
Transcription
1 PATHOLOGY OF THE SKIN 2. Tumours of the skin Máirín E. McMenamin MB MRCPI FRCPath Dip (Dermatopathol) RCPath St. James s Hospital and University of Dublin, Trinity College
2 Tumour (Neoplasia) Benign or malignant Malignant tumour Primary cutaneous tumour Metastatic tumour
3 Melanocytic (melanoma) Lymphoid (lymphoma) Mycosis fungoides (T cell lymphoma, long term course, clinically can mimic eczema or psoriasis) Subcutaneous panniculitis-like T cell lymphoma Mesenchymal (sarcoma) Dermatofibrosarcoma protuberans Angiosarcoma (aetiologies: chronic sun-exposure and radiation) [Kaposi sarcoma (associated with HHV8)] Primary Cutaneous Malignant Skin Tumours Epithelial (carcinomas) [Non melanoma skin cancer (NMSC): most common human cancer] basal cell carcinoma squamous cell carcinoma skin adnexal carcinomas (e.g. sebaceous carcinoma, Merkel cell carcinoma, microcystic adnexal carcinoma, adenoid cystic carcinoma, apocrine carcinoma) [Some adnexal tumours (benign and malignant) can be associated with visceral malignancy (e.g. sebaceous tumours Muir Torre syndrome)]
 Chronic inflammation Chronic sinus tracts Chronic ulcers (Marjolin ulcer) Immunosupression (some tumours are HPV related)")
4 SKIN CARCINOMA AETIOLOGIC FACTORS Ultraviolet (UV) light (sun / sunbeds) Results in DNA damage: formation of pyrimidine dimers (UV signature mutations) Polycyclic hydrocarbons Ionizing radiation (also implicated in angiosarcoma) Chronic inflammation Chronic sinus tracts Chronic ulcers (Marjolin ulcer) Immunosupression (some tumours are HPV related) Arsenicals
5 Epithelial tumours Bowen s disease Squamous cell carcinoma Basal cell carcinoma Sebaceous naevus (benign) Muir Torre syndrome tumours Merkel cell carcinoma (neuroendocrine tumour of skin)
6 Bowen s disease (squamous cell carcinoma in situ) common on lower limbs in elderly females

7 Keratin horn This can overly actinic keratosis, SCC in situ or invasive SCC
8 Squamous cell carcinoma Most common on sun-exposed skin, especially head and neck Elderly patients M > F May arise at sites of chronic inflammation osteomyelitic sinuses varicose ulcers Frequent and multiple in following cohorts: Immunosuppressed patients (renal transplantation) HPV-related Xeroderma pigmentosum Epidermolysis bullosa (dystrophic variant)


9 Invasive squamous cell carcinoma of pinna of ear with overlying cutaneous horn


10 Arsenical keratoses and squamous cell carcinoma (contamination of irrigation water from ground table water as a result of forced irrigation due to green revolution GM products)
 Gorlin syndrome (naevoid basal cell carcinoma syndrome)")
11 Basal cell carcinoma Most common skin cancer (70%) Most common on sun-exposed skin Increased incidence with age In younger patients arises more commonly on trunk Frequently ulcerates centrally but invades very slowly Local recurrence risk if incompletely excised Rarely metastasizes < 1% UV- induced mutations in patched gene (PTCH) Gorlin syndrome (naevoid basal cell carcinoma syndrome) multiple BCCs, keratocysts of jaw Germline mutations in patched gene (PTCH) on chromosome 9q (component of the Sonic hedgehog signaling pathway)


12 Basal cell carcinoma most commonly presents as small pearly papule or eroded plaque

13 BCC can be extensive and can be problematic when encroaches on eye (following topical treatment with imiquimod)

14 Basal cell carcinoma: basaloid islands invade into dermis with connection to overlying epidermis
15 Basal cell carcinoma Molecular events Primary tumour Activation of the Sonic hedgehog signaling pathway - loss of patched gene (PTCH) - activation of smoothened gene (SMO) Metastases are very rare Accumulation of other genetic events e.g. trisomy 6
")


16 Paget s disease of the breast Mammary carcinoma in situ (DCIS) grows in epidermis of nipple May be associated with underlying invasive mammary carcinoma Also Paget s disease can occur in the genital area Cytokeratin



17 Sebaceous naevus Common on scalp and head and neck Congenital lesions Composed of a proliferation of sebaceous glands, apocrine glands Tumours can arise within them (both benign and malignant) (Benign) trichoblastoma Most common benign tumour to arise in sebaceous naevus
18 Muir Torre syndrome Autosomal dominant condition Associated with visceral malignancy especially hereditary non polyposis colorectal carcinoma DNA missmatch repair gene mutations Sebaceomas, cystic sebaceous neoplasms

")

19 Muir Torre syndrome Most classic sebaceous neoplasm in this syndrome is the sebaceoma (majority of these are benign) Sebaceoma Basaloid solid variant with sebaceous differentiation Cystic variant of sebaceoma
20 Sebaceous carcinomas Most common around the eye Can be aggressive
21 Merkel cell carcinoma (Primary cutaneous neuroendocrine cell carcinoma) Elderly patient Sun exposed areas Rapidly growing purplish nodules Aggressive behaviour Cytokeratin positive (dot-like) Neuroendocrine markers positive (chromogranin)
22 Melanocytic naevi and melanoma
23 Melanocytic naevus Benign melanocytic lesion Many variants Most common variants Junctional Compound Dermal Congenital or acquired Giant congenital naevus Less common variants that can clinically mimic melanoma Regressing / halo naevus Spindle cell naevus of Reed Spitz Dysplastic



24 Melanocytic naevi Junctional naevus Melanocytes along dermoepidermal junction Compound naevus Melanocytes along junction and in dermis

25 Giant congenital naevus (Garment naevus) 1/20,000 infants Risk of development of melanoma 6% (2 peaks: <10 y and adult life)
 with background naevus cells (below) Melanoma")
26 Melanoma arising in a congenital naevus: large melanoma cells (above) with background naevus cells (below) Melanoma Naevus



27 Inflamed/halo naevi Benign lymphocytic autoimmune response to naevus Naevus can regress entirely
 nodules of compound naevus")
 Most commonly occurs")

28 Melanoma mimics Naevus spilus (speckled naevus) nodules of compound naevus within a junctional naevus Spindle cell naevus (of Reed) Most commonly occurs on thigh of young women Recurrent naevus (after incomplete excision some naevi recur)




29 Spitz naevus Most commonly occurs in children but can occur in adults Usually amelanotic Composed of large plump cells or spindle cells Can mimic melanoma Epithelioid cell variant Spindle cell variant



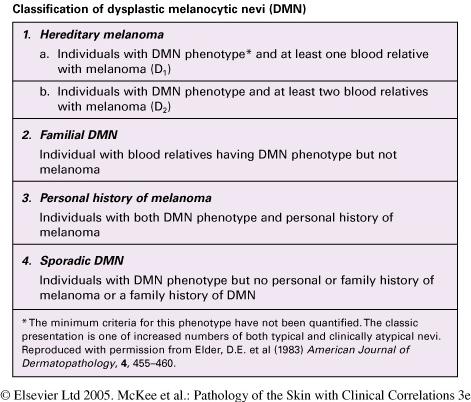
30 Dysplastic naevus syndrome Clinically atypical large naevi Histologically naevi show cytological and architectural atypia of melanocytes with dermal fibrosis and lymphocytic inflammation Dysplastic naevi can mimic melanoma Risk of melanoma
31


")
32 Blue naevus Scalp, face, neck and chest are common sites Melanotic dendritic spindled melanocytes Epithelioid variant is associated with Carney complex (associated with cardiac myxomas and lentigines) Epithelioid blue naevus
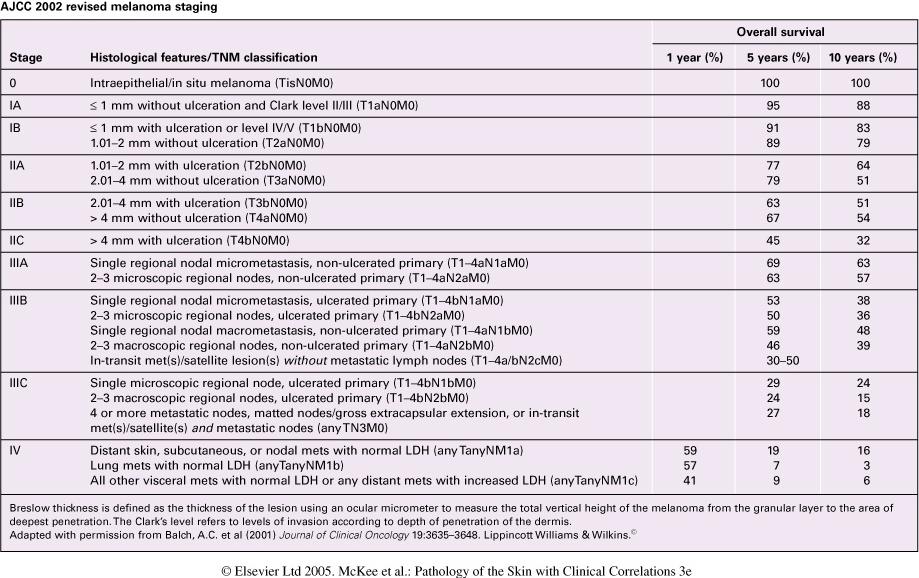
33 Malignant melanoma Incidence is increasing, especially in Australia changes in ozone layer diagnostic criteria have changed and increased screening Incidence increases with age Prognosis related to stage at presentation, depth of invasion, level of invasion (Clark) and ulceration Most important prognostic indicators in localized melanoma 1. Tumour thickness (Breslow depth) 2. Ulceration Most common on sun-exposed skin (intermittent exposure worse) Acral lentiginous melanoma relatively more common in dark skinned races Metastasis by both lymphatic route (lymph nodes) and haematogenous route (liver, lungs) Sentinel node mapping for melanomas >1<4 mm Breslow depth 5 year survival 56% when + and 90% when negative Some variants (naevoid melanoma) are very difficult to diagnosis Primary lesion can regress completely - can present with metastases
34 Melanoma is increasing in incidence, especially in higher socioeconomic groups

35 Clinical diagnosis of melanoma ABCD rule (not specific for melanoma as atypical naevi can share these features)
36 Malignant melanoma Histologic types Superficial spreading melanoma Nodular melanoma Lentigo maligna melanoma Acral lentiginous melanoma Naevoid melanoma Small cell melanoma Desmoplastic Mucosal sites lentiginous melanoma Copyright M. McMenamin




37 Superficial spreading malignant melanoma Nodular melanoma (amelanotic case) Lentigo maligna melanoma Acral lentiginous melanoma



38 HISTOLOGY OF MALIGNANT MELANOMA Malignant epithelioid cells invade the epidermis and dermis


39 HMB-45 can be positive in melanoma Other helpful immunostains are S100 protein and melan A



40 Lentigo maligna A form of melanoma in situ that occurs on chronically sun damaged skin Generally grows in situ for years before invading dermis when it is termed lentigo maligna melanoma Melan A immunostain can highlight the lentigo maligna cells




41 Desmoplastic melanoma Can arise in setting of lentigo maligna Lesions usually clinically benign can mimic scar Can mimic a scar Perineural invasion is common; therefore high rate of local recurrence Melanoma cells stained with S100 protein




42 Acral lentiginous melanoma Subungual melanoma Hutchinson s sign can be seen in advanced cases pigmentation extends onto nail fold Extension down eccrine ducts typical of acral lentiginous melanoma Heterologous osseous and cartiginous metaplasia can be seen Melanoma involves eccrine ducts Heterologous osseous and cartiginous metaplasia in acral lentiginous melanoma
43 Malignant melanoma Poor prognostic indicators Primary tumour Depth (Breslow) measured in mm 0-1 mm 1-2 mm 2-4 mm > 4 mm Ulceration Site Male sex Vascular invasion Perineural invasion : increased local recurrence Lymph node metastases Site of involvement Number of involved lymph nodes Distant Metastases Site Visceral mets:worst Lung mets: intermediate Skin mets: better Elevated blood LDH (lactate dehydrogenase)
44


45 Adverse prognostic indicators in melanoma Lymphovascular invasion Confers increased risk of metastasis Peri / intraneural invasion Confers increased risk of local recurrence

46 Adverse prognostic factor Microsatellite deposits

47 Metastatic melanoma


48 Regression Melanoma undergoes apoptosis and scarring, melanophages, lymphocytic inflammation and a proliferation of blood vessels is seen in its place Melanoma can disappear entirely

49 Sentinel lymph node examination Performed in cases of melanomas of Breslow depth 1-4mm Lymph node draining the area of melanoma is detected using radioactive tracer and blue dye Lymph node is excised and examined thoroughly by pathologist If metastasis present completion lymphadenectomy is performed Sentinel lymph node examination adds prognostic information but the technique has not reliably been shown to improve survival and there are some controversies regarding this procedure
50 Malignant melanoma Molecular events Primary tumour Genes implicated p16 (CDKN2A) CDK 4 MC1R (melanocortin 1 receptor) B-RAF N-RAS p53 cyclin D1 ckit Nodal metastases Accumulation of other genetic events including frequent chromosomal aberrations Melanoma families: Mutations in p16 (CNKN2A) CDK4
51 FUTURE FOR MELANOMA DIAGNOSIS Cytogenetics/genetics in ambiguous melanocytic lesions /prognosis? FISH probes are in development distinguish between melanoma and Spitz naevi melanoma: multiple chromosomal aberrations -9, -10, -6q, 8p +7, +8q, +6p, +1q, +17, +20 naevi: none / rare aberrations Spitz naevi 50% normal, 50% +11p Currently no effective therapy for locally advanced melanoma: need to identify targets for molecular targeted therapy?
52 Selected mesenchymal tumours Dermatofibrosarcoma protuberans Kaposi sarcoma Cutaneous angiosarcoma Atypical fibroxanthoma


53 Dermatofibrosarcoma protuberans Spindle cell sarcoma Initially grows in dermis as a plaque, then invades subcutis and becomes a tumour High local recurrence Potential for metastasis when dedifferentiates into higher grade sarcoma (fibrosarcomatous change)


54 Kaposi sarcoma Vascular tumour (v reactive vascular proliferation?) HHV8 (Kaposi sarcoma virus) Different subtypes: endemic, HIV, renal transplant associated


55 Kaposi sarcoma: spindle cell vascular proliferation HHV8 immunostain is positive



56 Cutaneous angiosarcoma Arises on sun damaged skin of head and neck Location at other sites (e.g. breast) can be associated with prior radiotherapy or lymphoedema Can present as subtle bruise in early stage Poor prognosis, no effective therapy high recurrence rate following excision
57 Atypical fibroxanthoma Rapidly growing fleshy or ulcerated nodules on sun exposed skin, generally on bald scalps Sun induced malignant mesenchymal proliferations but they have a good prognosis and essentially do not metastasize Bizarre pleomorphic tumour cells with giant cells and spindle cells Have to exclude diagnosis of carcinoma by cytokeratin immunostain and melanoma by S100 protein and other melanocytic markers (HMB-45 and melan A)


58 Atypical fibroxanthoma
")


59 Atypical fibroxanthoma (AFX) Polyoid tumour composed of bizarre pleomorphic cells with tumour giant cells and many mitoses
60 Lymphoma Many different types of cutaneous lymphoma, both T and B cell lymphomas Mycosis fungoides (T cell lymphoma with epidermotropism) that has a chronic course CD30 positive cutaneous lymphoproliferative disorders Lymphomatoid papulosis Anaplastic large cell lymphoma Subcutaneous panniculitis-like T cell lymphoma CD8 positive and can mimic panniculitis of lupus erythematosus



61 Mycosis fungoides Commonest cutaneous lymphoma, chronic course, clinically can mimic eczema T cell lymphoma with epidermotropism and late dissemination to lymph nodes Malignant T lymphocytes present in epidermis

62 Hypopigmented variant of mycosis fungoides Can mimic fungal infection More common in black patients

63 Late tumour stage mycosis fungoides


64 Tumour stage mycosis fungoides Dermal proliferation of malignant T lymphocytes (CD4 positive)
")

65 Metastases to skin (secondary cancer) Predilection for location of metastases on scalp and head and neck

66 Sister Mary Joseph nodule Umbilical deposit of metastatic colon carcinoma


67 Metastatic breast adenocarcinoma Metastatic renal cell carcinoma
68
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Update on Cutaneous Mesenchymal Tumors. Thomas Brenn
 Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Cutaneous Adnexal Tumors
 Cutaneous Adnexal Tumors Lesions with Predominant Follicular Differentiation Special Emphasis on Basal Cell Carcinoma 2014-04-01 Prof. Dr. med. Katharina Glatz Pathologie Cutaneous Adnexal Tumors Hair
Cutaneous Adnexal Tumors Lesions with Predominant Follicular Differentiation Special Emphasis on Basal Cell Carcinoma 2014-04-01 Prof. Dr. med. Katharina Glatz Pathologie Cutaneous Adnexal Tumors Hair
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 2. Variations on the acquired nevus 3. Dermal melanocytosis
 Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis
 - Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
Pathology. Skin Tumor. Bayan N. Mohammad 15/10/2015. Mohammad al-orjani. Page 0 of 23
 #7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
#7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Subject Index. Dry desquamation, see Skin reactions, radiotherapy
 Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
SEBACEOUS NEOPLASMS. Dr. Prachi Saraogi Clinical Fellow in Dermatology
 SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Cancer Reporting for Dermatologists. Florida Department of Health Florida Cancer Data System. March 9, Agenda
 Cancer Reporting for Dermatologists Florida Department of Health Florida Cancer Data System March 9, 2011 Agenda Welcome Introductions Cancer Reporting in Florida BETA Participation Expectations Review
Cancer Reporting for Dermatologists Florida Department of Health Florida Cancer Data System March 9, 2011 Agenda Welcome Introductions Cancer Reporting in Florida BETA Participation Expectations Review
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Bone, soft tissue and skin tumors. By: Shefaa qa qa
 Bone, soft tissue and skin tumors By: Shefaa qa qa Bone tumors Most bone neoplasms develop during the first several decades of life and have a propensity for the long bones of the extremities. The occurrence
Bone, soft tissue and skin tumors By: Shefaa qa qa Bone tumors Most bone neoplasms develop during the first several decades of life and have a propensity for the long bones of the extremities. The occurrence
NEOPLASIA. 3. Which of the following tumour is benign a. Chondrosarcoma b. Osteochondroma c. Chondroblastoma d. Ewing s tumour e.
 NEOPLASIA 1. malignant neoplasms a. are independent of hormonal influence b. are always composed of homogenous cell lines c. arise from differentiated cells by a process of anaplasia d. display abnormal
NEOPLASIA 1. malignant neoplasms a. are independent of hormonal influence b. are always composed of homogenous cell lines c. arise from differentiated cells by a process of anaplasia d. display abnormal
Diploma Examination. Dermatopathology: First paper. Tuesday 20 March Candidates must answer FOUR questions. Time allowed: 3 hours
 Dermatopathology: First paper Tuesday 20 March 2018 Candidates must answer FOUR questions Time allowed: 3 hours 1. Give an account of the genetic aberrations encountered in Spitzoid neoplasms and how these
Dermatopathology: First paper Tuesday 20 March 2018 Candidates must answer FOUR questions Time allowed: 3 hours 1. Give an account of the genetic aberrations encountered in Spitzoid neoplasms and how these
Atypical Nevi When to Re-excise. Catherine Barry, DO Dermatopathologist
 Atypical Nevi When to Re-excise Catherine Barry, DO Dermatopathologist Why talk about skin cancer? Because it s the most common type of cancer! Non-melanoma Skin Cancers Basal Cell Carcinoma Squamous Cell
Atypical Nevi When to Re-excise Catherine Barry, DO Dermatopathologist Why talk about skin cancer? Because it s the most common type of cancer! Non-melanoma Skin Cancers Basal Cell Carcinoma Squamous Cell
Diploma examination. Dermatopathology: First paper. Tuesday 21 March Candidates must answer FOUR questions ONLY. Time allowed: Three hours
 Dermatopathology: First paper Tuesday 21 March 2017 1. Discuss the role of fluorescent in-situ hybridization (FISH) and emerging molecular techniques in the diagnosis of cutaneous melanocytic lesions,
Dermatopathology: First paper Tuesday 21 March 2017 1. Discuss the role of fluorescent in-situ hybridization (FISH) and emerging molecular techniques in the diagnosis of cutaneous melanocytic lesions,
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
BAP-oma & BEYOND MICHAEL A NOWAK, MD
 BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
Myxo-inflammatory Fibroblastic sarcoma
 AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Appendageal skin tumors
 Appendageal skin tumors Ibrahim Khalifeh, M.D. Associate Professor Department of Pathology American University of Beirut Medical Center Beirut, Lebanon Appendageal tumors Neoplasms whose differentiation
Appendageal skin tumors Ibrahim Khalifeh, M.D. Associate Professor Department of Pathology American University of Beirut Medical Center Beirut, Lebanon Appendageal tumors Neoplasms whose differentiation
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Case 18. M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is:
 Case 18 M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is: A. Pilomatrical carcinoma B. Adnexal carcinoma NOS C. Metastatic squamous cell carcinoma D.Primary squamous cell carcinoma
Case 18 M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is: A. Pilomatrical carcinoma B. Adnexal carcinoma NOS C. Metastatic squamous cell carcinoma D.Primary squamous cell carcinoma
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
MALIGNANT MELANOMA. Dr D. Tenea Department of Dermatology University of Pretoria
 MALIGNANT MELANOMA Dr D. Tenea Department of Dermatology University of Pretoria BACKGROUND History MM. of the skin is a malignant neoplasm of the epidermal melanocytes The incidence rates show considerable
MALIGNANT MELANOMA Dr D. Tenea Department of Dermatology University of Pretoria BACKGROUND History MM. of the skin is a malignant neoplasm of the epidermal melanocytes The incidence rates show considerable
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Chapter 6 Squamous Cell Carcinoma: Variants and Challenges
 Chapter 6 Squamous Cell Carcinoma: Variants and Challenges Michael B. Morgan EPIDEMIOLOGY: Second most common skin cancer, rare in the dark-skinned races. ETIOLOGY: Ultraviolet light, HPV infection. PATHOGENESIS:
Chapter 6 Squamous Cell Carcinoma: Variants and Challenges Michael B. Morgan EPIDEMIOLOGY: Second most common skin cancer, rare in the dark-skinned races. ETIOLOGY: Ultraviolet light, HPV infection. PATHOGENESIS:
Skin SSG (Anglia East & Anglia West)
") Skin SSG (Anglia East & Anglia West) Author: Dr Jennifer Garioch, Consultant Dermatologist Dr Pamela Todd, Consultant Dermatologist Approved by: Anglia Cancer Network Skin NSSG Approved on: Reviewed and
Skin SSG (Anglia East & Anglia West) Author: Dr Jennifer Garioch, Consultant Dermatologist Dr Pamela Todd, Consultant Dermatologist Approved by: Anglia Cancer Network Skin NSSG Approved on: Reviewed and
 Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Gross Appearance & Histology of Skin Cancer. Kyle Mannion M.D. January 21, 2005
 Gross Appearance & Histology of Skin Cancer Kyle Mannion M.D. January 21, 2005 Actinic Keratosis 5-20% will develop squamous/basal cell ca Almost solely from solar damage Usually develop during 4 th decade
Gross Appearance & Histology of Skin Cancer Kyle Mannion M.D. January 21, 2005 Actinic Keratosis 5-20% will develop squamous/basal cell ca Almost solely from solar damage Usually develop during 4 th decade
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Journal of International Academy of Forensic Science & Pathology (JIAFP)
") Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Journal of International Academy of Forensic Science & Pathology (JIAFP) ISSN 2395-0722 MICROCYSTIC ADNEXAL CARCINOMA-A CASE REPORT WITH REVIEW OF LITERATURE Case Report Sulakshana M S 1,Natarajan M 2
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Oliver J. Wisco, DO, FAAD Melanoma Specialist & Mohs Surgeon Bend Memorial Clinic
 A Primary Care Approach to Skin Cancer Oliver J. Wisco, DO, FAAD Melanoma Specialist & Mohs Surgeon Bend Memorial Clinic 1 Disclosures Speaker for MiMedx Consultant for MiMedx NO PERTINENT CONFLICTS OF
A Primary Care Approach to Skin Cancer Oliver J. Wisco, DO, FAAD Melanoma Specialist & Mohs Surgeon Bend Memorial Clinic 1 Disclosures Speaker for MiMedx Consultant for MiMedx NO PERTINENT CONFLICTS OF
Fluorescence spectroscopy and microscopy of cutaneous tumours correlation between micro- and macro- spectral measurements
 Fluorescence spectroscopy and microscopy of cutaneous tumours correlation between micro- and macro- spectral measurements E. Borisova 1, L. Avramov 1, M. Lomova 2, O. Semyachkina-Glushkovskaya 2, D. Gorin
Fluorescence spectroscopy and microscopy of cutaneous tumours correlation between micro- and macro- spectral measurements E. Borisova 1, L. Avramov 1, M. Lomova 2, O. Semyachkina-Glushkovskaya 2, D. Gorin
History A 89 year old gentleman presenting with a scalp/forehead nodule. Patient had squamous cell carcinoma 18 m at same site, excised. Outside diagn
 Case III History A 89 year old gentleman presenting with a scalp/forehead nodule. Patient had squamous cell carcinoma 18 m at same site, excised. Outside diagnoses: Squamous cell carcinoma. R/O: SCC, Melanoma,
Case III History A 89 year old gentleman presenting with a scalp/forehead nodule. Patient had squamous cell carcinoma 18 m at same site, excised. Outside diagnoses: Squamous cell carcinoma. R/O: SCC, Melanoma,
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Skin SSG (Anglia East & Anglia West)
") Guidelines for Referrals between Skin LMDT and SMDT Skin SSG (Anglia East & Anglia West) Author: Dr Jennifer Garioch, Consultant Dermatologist Dr Pamela Todd, Consultant Dermatologist Approved by: Anglia
Guidelines for Referrals between Skin LMDT and SMDT Skin SSG (Anglia East & Anglia West) Author: Dr Jennifer Garioch, Consultant Dermatologist Dr Pamela Todd, Consultant Dermatologist Approved by: Anglia
Skin lesions The Good and the Bad. Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry
 Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Multiple Primary Melanoma in a Thai Male: A Case Report
 Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Racial differences in six major subtypes of melanoma: descriptive epidemiology
 Wang et al. BMC Cancer (2016) 16:691 DOI 10.1186/s12885-016-2747-6 RESEARCH ARTICLE Racial differences in six major subtypes of melanoma: descriptive epidemiology Yu Wang 1, Yinjun Zhao 2 and Shuangge
Wang et al. BMC Cancer (2016) 16:691 DOI 10.1186/s12885-016-2747-6 RESEARCH ARTICLE Racial differences in six major subtypes of melanoma: descriptive epidemiology Yu Wang 1, Yinjun Zhao 2 and Shuangge
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
American College of Mohs Surgery. Diagnostic Quality Control Program (Review of Answers)
") American College of Mohs Surgery Diagnostic Quality Control Program 2010 (Review of Answers) Question 1 A flesh-colored plaque on the right ala of an otherwise healthy 57 year-old male is referred for
American College of Mohs Surgery Diagnostic Quality Control Program 2010 (Review of Answers) Question 1 A flesh-colored plaque on the right ala of an otherwise healthy 57 year-old male is referred for
Table of Contents. Preface xi. Acknowledgments xiii. Part I Overview of the Diagnostic Process 1. 1 Overview of Grading and Staging 3
 Table of Contents Preface xi Acknowledgments xiii Part I Overview of the Diagnostic Process 1 1 Overview of Grading and Staging 3 Identification of the process 3 Identification of tumor types 5 Grading
Table of Contents Preface xi Acknowledgments xiii Part I Overview of the Diagnostic Process 1 1 Overview of Grading and Staging 3 Identification of the process 3 Identification of tumor types 5 Grading
64 y.o. F with CLL and leg tumour
 64 y.o. F with CLL and leg tumour Case History Excision with split-skin grafting Histology moderately differentiated squamous cell carcinoma with large areas of necrosis and brisk mitotic activity.
64 y.o. F with CLL and leg tumour Case History Excision with split-skin grafting Histology moderately differentiated squamous cell carcinoma with large areas of necrosis and brisk mitotic activity.
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee
 I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
Modalities of Radiation
 Modalities of Radiation Superficial radiotherapy Orthovoltage Megavoltage Photons Electrons Brachytherapy Interstitial Moulds When to refer? The vast majority of skin cancers will be managed without any
Modalities of Radiation Superficial radiotherapy Orthovoltage Megavoltage Photons Electrons Brachytherapy Interstitial Moulds When to refer? The vast majority of skin cancers will be managed without any
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Skin Cancers Emerging Trends and Treatment Approaches
 Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None