Dr Amanda Oakley. Dermatologist Dept of Dermatology, Health Waikato Adjunct Associate Professor, Waikato Clinical Campus
|
|
|
- Charlene Ford
- 5 years ago
- Views:
Transcription
1 Dr Amanda Oakley Dermatologist Dept of Dermatology, Health Waikato Adjunct Associate Professor, Waikato Clinical Campus 14:00-16:00 WS #14: Dermoscopy Part 1

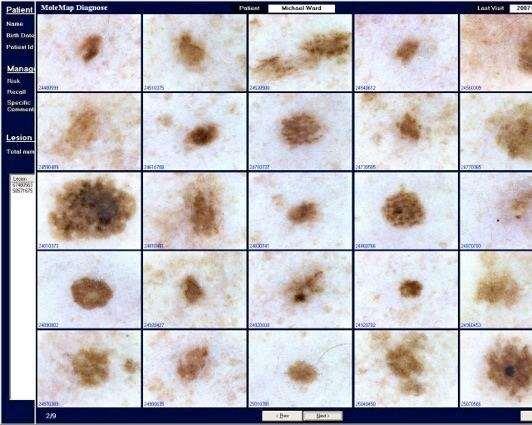
2 Skin Lesions and Dermatoscopy 16 August 2018 Christchurch GPCME Amanda Oakley Dermatologist, Dept of Dermatology, Health Waikato Adjunct Associate Professor, Waikato Clinical Campus Website Manager, DermNet New Zealand Specialist Dermatologist, Tristram Clinic Diagnosing Dermatologist, MoleMap NZ Director, New Zealand Teledermatology Tristram Clinic
3 Declaration of conflict of interest I diagnose for MoleMap NZ Thanks for many images I am Founder and Chief Editor of DermNet NZ Sponsored by PHARMA I have been on various advisory boards over the years but not relevant to this talk

4 This workshop Is not intended to make you an expert Expects you to take a history and to undertake total body skin examination 4
5 Content of workshop Course context Pre-test Introduction to dermatoscopy Clinical features of pigmented skin lesions Dermatoscopy of pigmented skin lesions Interactive exercises 5
6 6
7 Melanoma Standards Standard 1.1 Patients are offered evidence-based information on risk factors, prevention and detection of melanoma early Avoid sunburn and adopt UV protection (physical methods complemented by sunscreen) Strongly discourage use of sunbeds Advise all adults, particularly those aged 50 and over to: Regularly examine their skin Get someone else to check areas difficult to see Seek advice from a doctor about suspicious lesions. Total lack of sun exposure not advisable without vitamin D supplementation
8 Risk factors are age, prior melanoma / skin cancer / sun damage, many/large moles But two-thirds melanoma in average-risk subjects Nearly all skin cancer relates to UVR exposure Protect skin from UVR (sun, indoor tanning beds) Behaviour, clothing, SPF 50+ sunscreen Teach self skin-examination If risk factors, annual full skin check If many moles, digital dermatoscopic surveillance 8
9 Strongest predictors of invasive melanoma in > 65 yr: 2.3 x risk than < 45 Men: 2.1 x risk than women Queenslanders Skin doesn't tan: 4.8 x risk than if tan deeply At age 21 with many moles: 4.4 x those with 0 If >21 lesions treated, 2.5 x higher risk than those who had none treated 9
10 Primary prevention Target: All ages Fair skinned people People who work outdoors People with existing sun damage 10


11 Vitamin D and sun exposure 11
12 Estimate patient s risk of melanoma / NMSC Risk factor widget on BPAC Stay alert to incidental skin lesions Melanoma + NMSC Carry out full skin check Determine what s normal for the patient (moles, freckles, seborrhoeic keratoses, angiomas) 12
13 Take a history Skin cancer, immune suppression (drugs, disease), strong family history of melanoma (2+ < 40 yrs) Examine face and hands for actinic keratoses, solar lentigines Examine all skin for mole number (> 100), pattern Large moles, small dark moles, odd-looking moles Large congenital melanocytic naevi If > 20 cm, send to specialist for assessment 13
14 Melanoma Standards Standard 4.1 Investigation, Diagnosis and Staging Patients have access to a clinician trained in: Early detection and diagnosis of melanoma, including the use of dermatoscopy Surgical skills to undertake excision and direct closure of in-situ or thin melanoma The triage and referral of patients with lesions of uncertain diagnosis, thicker melanoma and lesions on sites where surgery is difficult.

15 Today s workshop is an introduction to dermatoscopy; it takes practice to be good at it Digital dermatoscopy (images) enhances skill Aids referral + clinicopathological correlation Automated devices should not be relied upon Surgical skills also take training + practice If you are not doing lots of surgery, refer to someone who is 15


16 Other resources Please join MelNet DermNet NZ Dermatoscopy Teledermatology for suspected skin cancers 16

17 Not always easy 17
18 Pre-test 10 images of pigmented skin lesions Decide if benign or malignant Select a diagnosis 10 seconds for each case 18
 Melanoma? c) Seborrhoeic keratosis?")
19 Lesion 1 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 19
 Melanoma? c) Seborrhoeic keratosis?")
20 Lesion 2 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 20
 Melanoma? c) Seborrhoeic keratosis?")
21 Lesion 3 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 21
 Melanoma? c) Seborrhoeic keratosis?")
22 Lesion 4 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 22
 Melanoma? c) Seborrhoeic keratosis?")
23 Lesion 5 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 23
 Melanoma? c) Seborrhoeic keratosis?")
24 Lesion 6 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 24
 Melanoma? c) Seborrhoeic keratosis?")
25 Lesion 7 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 25
 Melanoma? c) Seborrhoeic keratosis?")
26 Lesion 8 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 26
 Melanoma? c) Seborrhoeic keratosis?")
27 Lesion 9 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 27
 Melanoma? c) Seborrhoeic keratosis?")
28 Lesion 10 Benign or Malignant? a) Melanocytic naevus? b) Melanoma? c) Seborrhoeic keratosis? d) Basal cell carcinoma? 28
29 Introduction to dermatoscopy 29
30 This workshop is interactive Option A Option B 30
31 Who has their own dermatoscope? I have my own I don t have my own 31
32 What is dermatoscopy? = Dermatoscopy, epiluminescent microscopy Skin examination using: Magnification Good light Means to reduce surface reflection Contact fluid film Polarising filter Improves diagnostic accuracy in expert hands Confirmed by numerous clinical trials 32

33 Why magnify? 34


34 Why reduce surface reflection? No polarisation Polarisation 36












35 Dermatoscopes 37
36 This workshop is interactive Option 1 Option 2 Option 3??? 38


37 Option 4 None of the options are true: I don t know Not applicable 39
38 My dermatoscope is: Polarised Unpolarised A? B? Both? 40


39 My dermatoscope is: Contact Non-contact A? B? Both? 41


40 I have photodermatoscopy: Yes No A? B? Both? 42
41 Which dermatoscope? Depends on budget, interest, digital imaging Choices: Polarised, unpolarised or both Contact or non-contact Ability to attach to a camera Lens size and quality Portability Charger: AC, USB, dock 43

42 Non-contact devices Speedy review of entire skin surface Polarised view

43 Contact devices Add fluid Better quality Best for imaging Polarised and non-polarised options 46



44 Polarised vs unpolarised Both have liquid interface and lens in contact with the skin

45 How to use non-contact dermatoscope Takes practice to focus on skin lesions Allows a quick review of many lesions 50

46 How to use contact dermatoscope Tedious but higher quality Apply fluid to lesion Clean lens between lesions Clean lens between cases 51

47 Photography = digital dermatoscopy Camera Adapter(s) Suitable dermatoscope Archiving system Software suitable for sharing images 53
48 Why take photos? Clinical purposes The record Referral: required for HSCan melanoma referrals Clinicopathological correlation Education Yours Someone else s Research, publication 54







49 Smartphone + device Handyscope, Veos HD1, HD2 For iphone 4, 5, 6 Dermlite DL1, DL2, DL3 For iphone 4, 5, 6, 6+, 6s; ipod Touch; ipad 3, 4, air, mini; Galaxy S3, S4, S5 S6 Heine ic1 For iphone 5, 6 DermLite Hüd For smartphones 55

50 56
51 DermEngine software 57
52 Dermatoscopy training requires: Experience in skin history / examination Elementary course e.g., today s Reference books, articles, online resources A dermatoscope immediately to hand A camera to record lesions of interest Continued practice 58


53 Training in dermatoscopy Online modules: Apps Textbooks International Diploma of Dermatoscopy MMed (Skin Cancer) Program, U of Queensland Healthcert Skin Cancer Certificate Courses Skin Cancer College Australasia Certificatehttp:// 59

54 itunes App Store 60


55 Virtual Dermatoscope 61
56 When to use dermatoscopy All the time! Pigmented and non-pigmented lesions Benign, malignant and of uncertain significance Inflammatory dermatoses Psoriasis, eczema, lichen planus, lupus Infestations Head lice, scabies 62


57 Which of these has scabies? A? B? Both?


58 Which of these has scabies? A? B? Both?

59 Dermatoscopy of burrow
60 Skin examination 66
61 I d like a skin check Take a history Assess risk factors for skin cancer Identify lesion(s) of concern To patient, significant other, health professional Onset, duration, behaviour Effect of previous treatment 67
62 Risk factors for melanoma/nmsc Age, esp. >50 years Previous melanoma Previous keratinocytic skin cancer (BCC, SCC) Many moles Large moles Familial melanoma (2+ young, close relatives) Sunburns (melanoma, BCC) Chronic exposure to UV (AKs, SCCs) 68

63 Skin examination Good light & magnification Whole body Lesion location, distribution, morphology Size Shape Surface Structure Colour Ugly duckling? Dermlite Lumio & Lumio S 69


64 Photograph the lesion Anatomic Close-up 70





65 Take dermatoscopy images Clean lenses, dry carefully Apply fluid to lesion surface Spacer plate out, in contact with lesion, focus & capture 71

66 Dermatoscopy images Polarised Unpolarised 72

67 Dermatoscopy images Polarised Unpolarised 73


68 Still not sure? Excise with 2-mm margin 74 Histopathology: seborrhoeic keratosis
69 Pigmented skin lesions Melanocytic Naevus + melanomas Epithelial Seborrhoeic keratosis + BCC / SCC Vascular Angioma + haemorrhage Other Dermatofibroma 75
70 Benign lesions Rarely need excision. Exceptions: If malignancy cannot be excluded Significant symptoms Cosmetic reasons Benign lesions show symmetry: Single or multiple patterns Assess structure, colour and border (not shape) 76
71 So, which benign lesions: Should be referred? Excised as a precaution? Followed up? Ignored? It isn t always easy! 77

72 High Suspicion of Cancer HSCan (melanoma) Ministry of Health idea Initially for triage Later will be for referral 78


73 Which has red flag A? A? B? Both? 79


74 Red flag A : asymmetry Speckled lentiginous naevus Melanoma in situ 80

75 Which has red flag B? A? B? Both? 81


76 Red flag B : border Melanoma in situ Benign melanocytic naevus 82


77 Which has red flag C? A? B? Both? 83


78 Red flag C : colour Nodular melanoma 2.5 mm Melanoma in situ 84


79 Which has red flag D A? B? Both? 85
80 Red flag D : different SS melanoma 2.5 mm Seborrhoeic keratosis 86

81 Red flag D : different SS melanoma 3 mm Seborrhoeic keatosis 87
82 Which has red flag E? A? B? Both? 88



83 Which has red flag E A? B? Both? 89


84 Evolving: lesion A Seborrhoeic keratosis 2014 Seborrhoeic keratosis

85 Evolving: lesion B Benign naevus 2012 Benign naevus

86 Evolving: lesion B Benign naevus 2012 Benign naevus

87 Evolving lesion : melanoma in situ 93


88 Evolving lesion 2010: monitored 2011: melanoma in situ 94
89 Dermatoscopy of benign lesions No Chaos Symmetry of structure Symmetry of colour Symmetry of border One pattern, 2 concentric/regular patterns or 3 concentric patterns 95
90 Dermatoscopy of malignant lesions Chaos Asymmetry of structure Asymmetry of colour Asymmetry of border abruptness More than one pattern + One of the following clues: 1. Eccentric structureless zones, any colour 2. Gray circles, lines, dots, clods 3. Black dots or clods at periphery 4. Focal pseudopods or radial lines at periphery 5. White lines 6. Thick reticular lines 7. Polymorphous vessels 8. Parallel lines on the ridges (acral lesions only) 9. Large polygons 96

91 Chaos & Clues poster See Melnet website Provided by A/Prof Cliff Rosendahl 97
92 Modified pattern analysis Descriptive dermatoscopy 98
93 Dermoscopic pattern analysis Skin lesions are made up of structures: lines, dots/clods & structureless zones of varying colours... Structures forming neat patterns = naevi Structures disordered / chaotic = cancer 99


94 Patterns of lines 100


95 Clods Cobblestone pattern Globular or brown clod pattern 102


96 Patterns of dots Grey Red 103


97 Structureless patterns Brown (1 component) Skin coloured (2 components) 104


98 Complex patterns in naevi Structureless in structureless Structureless in dot/clods 105


99 Complex patterns in naevi Concentric patterns Repeating pattern 106

100 Disordered pattern in melanoma 107
101 Melanocytic lesions Naevi Melanoma 108
102 Melanocytic naevi Benign proliferation of melanocytes Naevocellular naevus Forming nests, chords, strands Congenital, tardive or acquired Histological classification (Ackerman) Congenital (superficial, superficial and deep), blue, combined, dermal / Unna / Miescher, halo / Sutton, recurrent, Clark, Spitz, Reed Junctional, compound, dermal 109

103 Junctional naevus: histology 110

104 Junctional naevus: dermatoscopy Sometimes a central area of dermal naevus is seen 111

105 Compound naevus: histology 112

106 Compound naevus: dermatoscopy 113

107 Dermal naevus: histology 114


108 Dermal naevus: dermatoscopy 115
109 Melanocytic naevi Congenital naevus Giant >40cm, large >20cm, medium >1.5cm, small Various clinical types Tardive naevus Appears in childhood/adolescence and evolves Similar pathological features to congenital naevus Acquired naevus Later onset, more superficial Follow immunosuppression or sun exposure 116


110 Which lesion is congenital? A? B? Both? 117


111 Both are true congenital naevi Large, distinctive lesions Present at birth A medium-sized >1.5 cm & <20 cm B giant-sized >40 cm
112 Which lesion is congenital? A? B? Both? 119
")
113 A is congenital True congenital naevus Childhood-onset tardive naevus Terminal hair indicates lesion was present at birth or during childhood (developmental) 120


114 Childhood-onset or tardive naevi Onset prior to puberty Sun has minor role A is common mole B is annular or eclipse naevus often found in scalp


115 Blue naevus Often deep blue May be grey, skin-coloured, brown Dermal spindle-shaped dendritic melanocytes 122

116 Blue naevus: histology 123

117 Blue naevus: dermatoscopy 124

118 Which is blue naevus? A? B? Both? 125


119 Dermatoscopy Angioma Blue naevus Clods pattern (lacunar) Structureless pattern (homogeneous) 126

120 Papillomatous dermal naevus (Unna) Often on trunk Soft, protruding mole Skin-coloured, brown, black Develops from flat naevus 127

121 Non-papillomatous dermal naevus: (Miescher) Dome-shaped nodule on face Skin coloured to dark brown May have terminal hair Histology: dermal melanocytes 128

122 Which is dermal naevus? A? B? Both? 129

")
123 Dermatoscopy of dermal naevi Unna naevus Miescher naevus Cobblestone pattern (clods) Structureless pattern (+ vv) 130
 Round or oval Histology of larger lesions")
124 Acquired naevus = Clark naevus Trunk, prox. limbs Any colour (pink, brown, black) Round or oval Histology of larger lesions dysplastic Superficial, flatt(ish) 131


125 Naevus on face Look for holes Hair follicles Sweat ducts No pigment Pseudonetwork 132

126 Acral naevus (palm/sole) Ridges and furrows Pigment in furrows 133
127 Which is facial naevus? A? B? Both? 134


128 Dermatoscopy of special sites Facial naevus Acral naevus (plantar) Pseudoreticular: skin coloured clods Parallel lines (+ lattice-like) 135

129 Eccrine ducts 136
130 Signature naevi* People often have several of similar type More obvious in fair skinned people with many moles Typical for the individual Solid pink Solid brown Lentiginous Perifollicular hypopigmentation Eclipse Cockade *Bolognia 137


131 Patient with many naevi 138

132 Solid brown naevus Structureless, 1-2 colours 139

133 Solid pink naevus Regular vascular pattern 140
134 Lentiginous signature naevus Reticular, structureless centre 141


135 Perifollicular hypopigmentation Reticular, hypopigmented clods 142
")
136 Eclipse naevus 2 patterns (reticular + structureless) 143

137 Cockade naevus 3 patterns (reticular + structureless + clods) 144
138 Cockade means? A knot of ribbons worn on a hat A targetoid naevus A? B? Both? 146






139 Cockade Hungary Brazil Argentina France 147
140 Funny-looking naevi Atypical naevus Benign or melanoma! Atypical Spitz naevus Benign or melanoma! Dysplastic naevus Benign or melanoma! MELTUMP (Melanocytic tumour with uncertain malignant potential) Benign or melanoma! STUMP (Spitzoid tumour with uncertain malignant potential) Benign or melanoma! SAMPUS (superficial atypical melanocytic proliferation) Benign or melanoma! 148




141 Atypical naevus = uncertain biology 149



142 Atypical naevi: dermatoscopy 150

143 Which is benign? A? B? Both? 151


144 Dermatoscopy helps if uncertain Benign compound naevus Melanoma in situ B has greater asymmetry of structure or Chaos 153
145 Melanoma Malignant neoplasia arising from melanocytes In situ or invasive Sometimes, very difficult to diagnose Clinically, dermatoscopically, histologically Most important prognostic factor Breslow thickness 154
146 Melanoma Most lesions (?70%) de novo A few arise within naevi Congenital, tardive, acquired Diagnosed by appearance or behaviour Observed change In flat lesions, dermatoscopic change seen long before clinical change In nodular lesions, change often observed by patient 155


147 Observed change
148 Clinical subtypes of melanoma Lentigo maligna melanoma Lentiginous melanoma Superficial spreading melanoma Nodular melanoma Acral lentiginous melanoma Desmoplastic melanoma Mucosal melanoma Naevoid melanoma Animal melanoma Non-cutaneous melanoma 157
149 Clinical ABCD rule for melanoma Asymmetry of shape Border irregularity Colour variability Diameter >6 mm Evolving For lay people to detect melanoma Features may not apply to early melanoma or nodular melanoma 158

 Colour")
150 Clinical A(B)CD rule for melanoma Asymmetry of structure (Border irregularity) Colour variability Different 159


151 Ugly duckling sign 160


152 ABCD+. Which is melanoma? A? B? Both? 161


153 Dermatoscopy Congenital naevus Melanoma in situ Less disordered More disordered 162
154 Which is melanoma? A? B? Both? 163
155 Both reported as melanoma in situ 164


156 Blue colour suggests invasion 165
157 Clinicopathological correlation Check lab report against clinical images Is the pathology diagnosis consistent with your clinical diagnosis? If not, contact the pathologist This needs to be done promptly 166


158 Histology melanoma in situ Revised report: Invasive melanoma, 1.8 mm thickness 167
159 Pigmented non-melanocytic lesions Solar lentigo Seborrhoeic keratosis Keratinocytic cancer BCC, SCC 168
160 Solar lentigo Circumscribed light brown macule May develop into seborrhoeic keratoses In sun-damaged skin Melanin in basal keratinocytes Melanocytes normal or increased number Elongated rete ridges 169




161 Solar lentigo 170

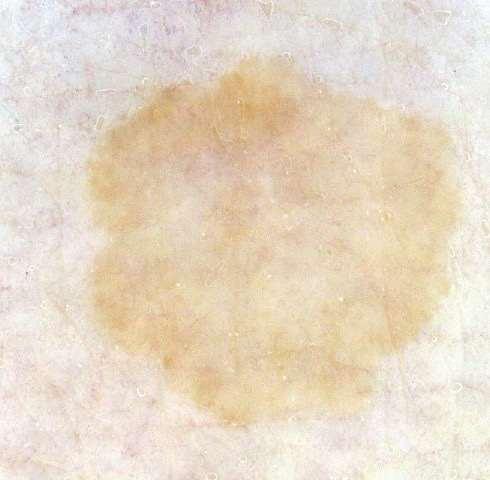
162 Solar lentigo Sharp edge Structureless, yellowish 171


163 Solar lentigo Moth-eaten edge Subtle structures 172
164 Seborrhoeic keratoses Skin coloured, yellow, brown, black Smooth to verrucous Irregular structure Flat or thickened Very variable in appearance Stuck-on 173




165 Seborrhoeic keratoses 174


166 Seborrhoeic keratosis Stuck on, warty Orange clods, curved thick lines 175


167 Seborrhoeic keratosis Yellowish, greasy White clods 176
 clods")
168 Seborrhoeic keratosis Yellowish, greasy White (& orange) clods 177


169 Seborrhoeic keratosis Thick curved lines 178

170 Which is solar lentigo? A? B? Both? 179

171 Pseudoreticular pattern in both Solar lentigo Melanocytic naevus Moth-eaten Roundish 180
172 Which is seborrhoeic keratosis? A? B? Both? 181
173 A is seborrhoeic keratosis Seborrhoeic keratosis Melanoma Easy! The seborrhoeic keratosis is scaly / warty 182
174 Which is seborrhoeic keratosis? A? B? Both? 183
175 B is seborrhoeic keratosis Dermal papillomatous naevus Seborrhoeic keratosis Discontinuous clods Interlinked clods + thick lines 184

176 Is precise diagnosis important? No if both are benign! Dermal papillomatous naevus Seborrhoeic keratosis 185
177 Does it wobble? Yes: melanocytic naevus No: seborrhoeic keratosis


178 Not always easy Seborrhoeic keratosis Melanoma Both can have have irregular and complex structures 187
179 Keratinocytic cancers Basal cell carcinoma Locally destructive On hair-bearing skin only Various types: Nodular Superficial Morphoeiform Fibroepithelial Infundibulocystic May be pigmented Actinic keratoses Rough white lesions on erythematous base May be pigmented SCC in situ Red scaly plaque May be pigmented Invasive SCC 188
180 Basal cell carcinoma Slow growing tumours on any site Locally destructive Early ulceration & bleeding May be pigmented Various subtypes: Nodulocystic Micronodular Morphoeic / sclerosing Ulcerative Superficial Basisquamous 189



181 Basal cell carcinoma 190

182 Dermatoscopy of basal cell carcinoma Irregular, bleeding, growing Irregular, bleeding, branched red lines 191


183 Dermatoscopy of Pink, shiny, enlarging basal cell carcinoma Peripheral dirty pigment, red branched lines 192
184 Actinic / solar keratosis Fluctuating small scaly plaques on areas chronically exposed to sunlight (face, hands) Tender, red or brown superficial lesions Variable adherent scale or horn Only on other sites when face and hands are badly affected Uncommon in darker skin types Uncommon in indoor workers 193




185 Actinic keratoses 194


186 Pigmented actinic keratosis Scaly irregular tender patch Strawberry + superficial network of broken-up lines 195


187 Strawberry Yellow dot within white circle with curved red lines 196
188 SCC in situ / intraepidermal ca One or more slowly-enlarging, red to brown, irregular plaques On any site May ulcerate or bleed Scale is prominent Bowen disease Often confused with eczema or psoriasis 197




189 SCC in situ All 4 of these were all found on the same patient s trunk and limbs 198

190 SCC is / IEC Irregular red scaly plaque Dotted blood vessels 199


191 SCC is / IEC Irregular red/brown scaly plaque Dotted blood vessels, may b in rows like the pigment 200
192 Invasive SCC Usually arise from actinic keratosis or IEC Fast-growing indurated, tender plaques or nodules Variable scale, horn and ulceration Variable differentiation: Keratoacanthoma Microinvasive disease Well differentiated Moderately well Undifferentiated Anaplastic 201




193 Invasive SCC 202

194 Squamous cell carcinoma Tender scaly growing nodule Central scale, white periphery 203


195 Squamous cell carcinoma Ulcerated tender growing nodule Central ulcer, white circles, white periphery 204


196 Which is BCC? A? B? Both? 205


197 Dermatoscopy Pigmented BCC 0.4 mm amelanotic melanoma Irregular peripheral pigment Small focus of pigment network 206

198 Which is BCC? A B A? B? Both? 207

199 Dermatoscopy Dermal naevus Nonpigmented basal cell carcinoma Structureless + terminal hairs Branched red lines + scale + ulcer 208


200 Which is BCC? A? B? Both? 209


201 Dermatoscopy Angioma Pigmented basal cell carcinoma Purple clods Irregular clods + dirty dishwater 210

202 Dirty dishwater 211


203 Dirty dishwater Irregular leaf-like clods and dots, grey-brown colour 212
It can be helpful in some cases of actinic keratosis, Bowen s disease and squamous cell carcinoma
 Dermoscopy Introduction, Terminology and Structures (to be read in conjunction with the Diagnostic Dermoscopic Algorithm) Copyright to Cunliffe TP (Jan. 2017) All rights reserved Introduction Dermoscopy
Dermoscopy Introduction, Terminology and Structures (to be read in conjunction with the Diagnostic Dermoscopic Algorithm) Copyright to Cunliffe TP (Jan. 2017) All rights reserved Introduction Dermoscopy
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
INTRODUCTION HOUSEKEEPING June 11 th Dr John Adams Dermatologist/Dermoscopist MOLEMAP NZ/Australia MOLESAFE USA
 INTRODUCTION HOUSEKEEPING June 11 th 2015 Dr John Adams Dermatologist/Dermoscopist MOLEMAP NZ/Australia MOLESAFE USA Program Skin cancer statistics. Dermoscopy description and usefulness. Patient /lesion
INTRODUCTION HOUSEKEEPING June 11 th 2015 Dr John Adams Dermatologist/Dermoscopist MOLEMAP NZ/Australia MOLESAFE USA Program Skin cancer statistics. Dermoscopy description and usefulness. Patient /lesion
Skin lesions The Good and the Bad. Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry
 Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
22/04/2015. Dermoscopy of Melanoma. Ilsphi Browne. Overview
 Dermoscopy of Melanoma Ilsphi Browne Overview The device Dermoscopic criteria (terminology) Colour Patterns Global features Local features Approach to diagnosing pigmented lesions Other uses in general
Dermoscopy of Melanoma Ilsphi Browne Overview The device Dermoscopic criteria (terminology) Colour Patterns Global features Local features Approach to diagnosing pigmented lesions Other uses in general
Fundamentals of dermoscopy
 Fundamentals of dermoscopy Learning objectives Upon completion of this session, participants should be able to: describe the basic principles of dermoscopy identify features associated with pigmented and
Fundamentals of dermoscopy Learning objectives Upon completion of this session, participants should be able to: describe the basic principles of dermoscopy identify features associated with pigmented and
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Mole mapping and monitoring. Dr Stephen Hayes. Associate Specialist in Dermatology, University Hospital Southampton
 Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Dermoscopy in everyday practice. What and Why? When in doubt cut it out? Trilokraj Tejasvi MD
 Dermoscopy in everyday practice Trilokraj Tejasvi MD Assistant Professor, Department of Dermatology, Director Teledermatology services, University of Michigan, Faculty Associate, GLOBAL REACH, Michigan
Dermoscopy in everyday practice Trilokraj Tejasvi MD Assistant Professor, Department of Dermatology, Director Teledermatology services, University of Michigan, Faculty Associate, GLOBAL REACH, Michigan
Appendix : Dermoscopy
 Go Back to the Top To Order, Visit the Purchasing Page for Details APP Appendix : Dermoscopy Dermoscopy, also known as dermatoscopy, epiluminoscopy and epiluminescent microscopy, is an effective non-invasive
Go Back to the Top To Order, Visit the Purchasing Page for Details APP Appendix : Dermoscopy Dermoscopy, also known as dermatoscopy, epiluminoscopy and epiluminescent microscopy, is an effective non-invasive
VACAVILLE DERMATOLOGY
 Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Disclosure. Objectives. PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016
 PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016 1 Disclosure The speaker has no conflict of interest, financial agreement, or working affiliation with any group or organization.
PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016 1 Disclosure The speaker has no conflict of interest, financial agreement, or working affiliation with any group or organization.
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
50 interactive dermoscopic case discussions Dr Stephen Hayes
 50 interactive dermoscopic case discussions Dr Stephen Hayes Annotations will be found on your memory drive, as will 100 case discussions and other learning material Melanoma 2mm thick Ugly duckling-one
50 interactive dermoscopic case discussions Dr Stephen Hayes Annotations will be found on your memory drive, as will 100 case discussions and other learning material Melanoma 2mm thick Ugly duckling-one
Revised Pattern Analysis: a method for the accurate diagnosis of pigmented skin lesions
 Dermatoscopy for Students A concise outline of: Revised Pattern Analysis: a method for the accurate diagnosis of pigmented skin lesions And Chaos and Clues: a decision algorithm for routine practice to
Dermatoscopy for Students A concise outline of: Revised Pattern Analysis: a method for the accurate diagnosis of pigmented skin lesions And Chaos and Clues: a decision algorithm for routine practice to
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
6/17/2018. Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things. Bad?
 Dermoscopy of Brown(ish) Things. Bad?") Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things Jennie T. Clarke, MD ssociate Professor of Dermatology University of Utah School of Medicine Bad? 1 Brown(ish) Things Bad Melanoma Pigmented basal
Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things Jennie T. Clarke, MD ssociate Professor of Dermatology University of Utah School of Medicine Bad? 1 Brown(ish) Things Bad Melanoma Pigmented basal
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
The impact of GP sub-specialisation and dermatoscopy use on diagnostic accuracy for melanomas in Australia
 The impact of GP sub-specialisation and dermatoscopy use on diagnostic accuracy for melanomas in Australia Cliff Rosendahl, Gail Williams, Diann Eley, Tobias Wilson, Greg Canning, Jeffrey Keir, Ian McColl,
The impact of GP sub-specialisation and dermatoscopy use on diagnostic accuracy for melanomas in Australia Cliff Rosendahl, Gail Williams, Diann Eley, Tobias Wilson, Greg Canning, Jeffrey Keir, Ian McColl,
Dermoscopy-a BRIEF introduction
 Dermoscopy-a BRIEF introduction Aim of presentation -to tell you what dermoscopy is -to show some of what it can do -point the interested learner to further resources Overview of dermoscopy Dermoscopy
Dermoscopy-a BRIEF introduction Aim of presentation -to tell you what dermoscopy is -to show some of what it can do -point the interested learner to further resources Overview of dermoscopy Dermoscopy
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Malignant non-melanocytic lesions
 Malignant non-melanocytic lesions Course C023: Fundamentals of Dermoscopy March 4, 2019, 11:20 AM - 11:50 PM Room: 146B Jason B. Lee, MD Professor & Vice Chair Director of Dermatopathology & Pigmented
Malignant non-melanocytic lesions Course C023: Fundamentals of Dermoscopy March 4, 2019, 11:20 AM - 11:50 PM Room: 146B Jason B. Lee, MD Professor & Vice Chair Director of Dermatopathology & Pigmented
Finding Melanoma. Is not easy!
 Finding Melanoma Is not easy! Finding Melanoma Victoria mean depth at diagnosis is 1.5 mm. Melanoma 1.5mm Has Stage 1B Mortality 10% Melanoma Spotting a killer! Spotting a killer Visual Clues What are
Finding Melanoma Is not easy! Finding Melanoma Victoria mean depth at diagnosis is 1.5 mm. Melanoma 1.5mm Has Stage 1B Mortality 10% Melanoma Spotting a killer! Spotting a killer Visual Clues What are
Histopathological and SIAscopic Correlation of Pigmented Skin Lesions
 Histopathological and SIAscopic Correlation of Pigmented Skin Lesions Professor Sujatha Fernando MBBS(Hon), MSc(London, Distinction), FRSTM&H, FRCPA, FIAC, FACTM Senior Consultant in Anatomical Pathology,
Histopathological and SIAscopic Correlation of Pigmented Skin Lesions Professor Sujatha Fernando MBBS(Hon), MSc(London, Distinction), FRSTM&H, FRCPA, FIAC, FACTM Senior Consultant in Anatomical Pathology,
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Regression 2/3/18. Histologically regression is characterized: melanosis fibrosis combination of both. Distribution: partial or focal!
 Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Dermatoscopic features of cutaneous non-facial non-acral lentiginous growth pattern melanomas
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Dermatoscopic features of cutaneous non-facial non-acral lentiginous growth pattern melanomas Jeff Keir 1 1 Department of Dermatology, School of Medicine,
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Dermatoscopic features of cutaneous non-facial non-acral lentiginous growth pattern melanomas Jeff Keir 1 1 Department of Dermatology, School of Medicine,
comedo-like openings (clods, brown or orange & circles) milia-like cysts (dots or clods, white) 1/29/18 Dotted vessels are also commonly seen in SCC
 milia-like cysts (dots or clods, white) 1/29/18 Dotted vessels are also commonly seen in SCC") Brown circles Dotted vessels are also commonly seen in SCC Step1 1. Nevus (unequivocal) 2. DF/IDN 3. BCC 4. SCC Network Patchy network Peripheral network & central hypopigmentation DF: network with central
Brown circles Dotted vessels are also commonly seen in SCC Step1 1. Nevus (unequivocal) 2. DF/IDN 3. BCC 4. SCC Network Patchy network Peripheral network & central hypopigmentation DF: network with central
Skin Cancer. Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts Dr Elizabeth Ogden
 Skin Cancer Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts 13.10.16 Skin Cancer Melanoma mole cancer - is a true cancer which can metastasize and kill Non Melanoma skin cancer
Skin Cancer Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts 13.10.16 Skin Cancer Melanoma mole cancer - is a true cancer which can metastasize and kill Non Melanoma skin cancer
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper:
 This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/127789/ Version: Accepted Version Article: Muinonen-Martin,
This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/127789/ Version: Accepted Version Article: Muinonen-Martin,
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Skin Cancer A Personal Approach. Dr Matthew Strack Dunedin New Zealand
 Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Oral and Maxillofacial Surgery Department
 Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Prediction without Pigment: a decision algorithm for non-pigmented skin malignancy
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Prediction without Pigment: a decision algorithm for non-pigmented skin malignancy Cliff Rosendahl 1, Alan Cameron 1, Philipp Tschandl 2, Agata Bulinska
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Prediction without Pigment: a decision algorithm for non-pigmented skin malignancy Cliff Rosendahl 1, Alan Cameron 1, Philipp Tschandl 2, Agata Bulinska
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Key factors in successfully integrating dermoscopy into your clinical practice
 Key factors in successfully integrating dermoscopy into your clinical practice S051 Dilemmas and challenges in skin cancer therapies and management Monday, March 4 th 2019 (9AM-12PM) Room 209A 10:56-11:09AM
Key factors in successfully integrating dermoscopy into your clinical practice S051 Dilemmas and challenges in skin cancer therapies and management Monday, March 4 th 2019 (9AM-12PM) Room 209A 10:56-11:09AM
Talking to Your Clients About Skin Cancer. Objectives 9/9/2017. Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017
 Talking to Your Clients About Skin Cancer Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017 Objectives Provide general information about skin cancer and how skin cancers commonly
Talking to Your Clients About Skin Cancer Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017 Objectives Provide general information about skin cancer and how skin cancers commonly
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Dermoscopy. Enhanced Diagnostic Ability: Pigmented Lesions. Ted Rosen, MD Baylor College of Medicine Houston, Texas
 Dermoscopy Enhanced Diagnostic Ability: Pigmented Lesions Ted Rosen, MD Baylor College of Medicine Houston, Texas Faculty Disclosure Statement No conflicts relevant to this workshop! Sir William Osler
Dermoscopy Enhanced Diagnostic Ability: Pigmented Lesions Ted Rosen, MD Baylor College of Medicine Houston, Texas Faculty Disclosure Statement No conflicts relevant to this workshop! Sir William Osler
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report
 Case Reports in Oncological Medicine, Article ID 206260, 4 pages http://dx.doi.org/10.1155/2014/206260 Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report Sharad P. Paul 1,2,3 1 Skin
Case Reports in Oncological Medicine, Article ID 206260, 4 pages http://dx.doi.org/10.1155/2014/206260 Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report Sharad P. Paul 1,2,3 1 Skin
Derm quiz. Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52. bit.ly/2a8asoy. Scan the QR code with your phone
 Dermatology quiz Derm quiz Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52 OR bit.ly/2a8asoy OR Scan the QR code with your phone Contents Childhood rashes Pigmented lesions Sun damage Pityriasis References
Dermatology quiz Derm quiz Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52 OR bit.ly/2a8asoy OR Scan the QR code with your phone Contents Childhood rashes Pigmented lesions Sun damage Pityriasis References
Dermoscopy. Synonyms. Dermoscopy. Definition. Dermoscopy opens up a world of colour and structure that can t be seen with the naked eye
 Synonyms Dermoscopy Australasian College of Dermatologists G.P Training Module Dermoscopy Dermatoscopy Epiluminescence microscopy Skin surface microscopy Incident light microscopy Oil immersion microscopy
Synonyms Dermoscopy Australasian College of Dermatologists G.P Training Module Dermoscopy Dermatoscopy Epiluminescence microscopy Skin surface microscopy Incident light microscopy Oil immersion microscopy
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Introduction to Dermoscopy. Nicholas Compton, MD June 16, 2010
 Introduction to Dermoscopy Nicholas Compton, MD June 16, 2010 Overview What is dermoscopy Brief history Types of dermoscopy General approach to lesion of interest 2 step algorithm 3-point checklist Practice
Introduction to Dermoscopy Nicholas Compton, MD June 16, 2010 Overview What is dermoscopy Brief history Types of dermoscopy General approach to lesion of interest 2 step algorithm 3-point checklist Practice
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Thursday 21 st August Skin Problems
 Thursday 21 st August 2014 Skin Problems Skin Problems The Sun and the Skin Sun Damage Recognising the early signs of skin cancer The Big 3 inflammatory condi=ons Acne & Rosacea Eczema (Including Seborrhoeic
Thursday 21 st August 2014 Skin Problems Skin Problems The Sun and the Skin Sun Damage Recognising the early signs of skin cancer The Big 3 inflammatory condi=ons Acne & Rosacea Eczema (Including Seborrhoeic
BLINCK A diagnostic algorithm for skin cancer diagnosis combining clinical features with dermatoscopy findings
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com BLINCK A diagnostic algorithm for skin cancer diagnosis combining clinical features with dermatoscopy findings Peter Bourne, MBBS 1, Cliff Rosendahl,
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com BLINCK A diagnostic algorithm for skin cancer diagnosis combining clinical features with dermatoscopy findings Peter Bourne, MBBS 1, Cliff Rosendahl,
MELANOMA. Some people are more likely to get a m Melanoma than others:
 MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MODULE 1. LOCAL AND GENERAL CRITERIA IN PIGMENTED MELANOCYTIC LESIONS.
 DERMOSCOPY TEACHING PROGRAMME Dermoscopy Teaching Programme Module 1 MODULE 1. LOCAL AND GENERAL CRITERIA IN PIGMENTED MELANOCYTIC LESIONS. Dermoscopy is a non-invasive in vivo technique that provides
DERMOSCOPY TEACHING PROGRAMME Dermoscopy Teaching Programme Module 1 MODULE 1. LOCAL AND GENERAL CRITERIA IN PIGMENTED MELANOCYTIC LESIONS. Dermoscopy is a non-invasive in vivo technique that provides
MELANOMA. 4 Fitzroy Square, London W1T 5HQ Tel: Fax: Registered Charity No.
 MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
Periocular skin cancer
 Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Professor Michael Eccles
 Professor Michael Eccles Developmental Genetics & Pathology Laboratory Pathology Department University of Otago Dunedin 15:00-15:15 Melanoma Metastasis and Treatment Resistance Melanoma metastasis and
Professor Michael Eccles Developmental Genetics & Pathology Laboratory Pathology Department University of Otago Dunedin 15:00-15:15 Melanoma Metastasis and Treatment Resistance Melanoma metastasis and
Actinic keratosis (AK): Dr Sarma s simple guide
: Dr Sarma s simple guide") Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Non-melanocytic Patterns
 Non-melanocytic Lesions Non-melanocytic Patterns Michelle Tarbox, MD Assistant Professor of Dermatology and Dermatopathology Texas Tech University Health Sciences Center 2018 Seborrheic keratoses Acanthotic
Non-melanocytic Lesions Non-melanocytic Patterns Michelle Tarbox, MD Assistant Professor of Dermatology and Dermatopathology Texas Tech University Health Sciences Center 2018 Seborrheic keratoses Acanthotic
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Identifying Benign and Malignant Skin Lesions. No Disclosures. Common Benign Lesions. Benign Lesions 2/25/2018. Stucco Keratoses.
 Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Hauora Maori. Map. Non-Melanoma Skin Lesion. Clinically Seborrhoeic Keratosis. Management Options. Punch Biopsy. Refer to Public Skin Lesion Service
 Care map information Information resources for patients and carers Updates to this Care Map Hauora Maori Pacific Skin lesion history Clinical examination and diagnostic test Suspicious of Melanoma Non-Melanoma
Care map information Information resources for patients and carers Updates to this Care Map Hauora Maori Pacific Skin lesion history Clinical examination and diagnostic test Suspicious of Melanoma Non-Melanoma
Associate Professor Amanda Oakley. Professor H. Peter Soyer. Academic Dermatologist The University of Queensland Brisbane. Dermatologist Hamilton
 Associate Professor Amanda Oakley Dermatologist Hamilton Professor H. Peter Soyer Academic Dermatologist The University of Queensland Brisbane 8:30-10:30 WS #3: Dermoscopy Workshop Part 1 11:00-13:00 WS
Associate Professor Amanda Oakley Dermatologist Hamilton Professor H. Peter Soyer Academic Dermatologist The University of Queensland Brisbane 8:30-10:30 WS #3: Dermoscopy Workshop Part 1 11:00-13:00 WS
Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19
 VivaScope 1500 and 3000 imaging systems for detecting skin cancer lesions Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19 NICE 2018. All rights reserved. Subject to Notice of
VivaScope 1500 and 3000 imaging systems for detecting skin cancer lesions Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19 NICE 2018. All rights reserved. Subject to Notice of
Dermoscopy STFM Richard Usatine, MD 5/2/16. Disclosure Statement: Some Dermatoscopes. Dermoscopy Video. Thanks to Dr.
 Disclosure Statement: Dermoscopy STFM 2016 Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, Clinic University of Texas
Disclosure Statement: Dermoscopy STFM 2016 Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, Clinic University of Texas
SKIN. 3. How is the skin structured around the finger joints to allow for flexible movement of the fingers?
 SKIN Objectives for Exam #1: 1. List various skin structures and describe their functions. 2. Describe skin responses to increases and decreases in body temperature. 3. Provide examples of various skin
SKIN Objectives for Exam #1: 1. List various skin structures and describe their functions. 2. Describe skin responses to increases and decreases in body temperature. 3. Provide examples of various skin
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee
 I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
Be SunSmart Everywhere!
 Be SunSmart Everywhere! DID YOU KNOW? Sun exposure adds up day after day, and it happens every time you re in the sun. Damage is permanent and irreversible. MYTH Sunburn happens only when we go to the
Be SunSmart Everywhere! DID YOU KNOW? Sun exposure adds up day after day, and it happens every time you re in the sun. Damage is permanent and irreversible. MYTH Sunburn happens only when we go to the
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
Non-Melanocytic Pattern Dermoscopy
 Non-Melanocytic Pattern Dermoscopy I have no conflicts of interest to disclose Except that I LOVE dermoscopy Michelle Tarbox, MD Assistant Professor of Dermatology and Dermatopathology Texas Tech University
Non-Melanocytic Pattern Dermoscopy I have no conflicts of interest to disclose Except that I LOVE dermoscopy Michelle Tarbox, MD Assistant Professor of Dermatology and Dermatopathology Texas Tech University
10/3/2018. Dermoscopy: Looking beneath the surface of the skin. Dermoscopy for Family Medicine 10/11/2018
 Dermoscopy for Family Medicine 10/11/2018 Jane M. Grant-Kels, MD, FAAD Founding Chair Emeritus, Dept of Dermatology Professor of Dermatology, Pathology & Pediatrics Director of the Cut Oncology Ctr & Melanoma
Dermoscopy for Family Medicine 10/11/2018 Jane M. Grant-Kels, MD, FAAD Founding Chair Emeritus, Dept of Dermatology Professor of Dermatology, Pathology & Pediatrics Director of the Cut Oncology Ctr & Melanoma
The GP s approach to the patient who is worried about sun, skin and moles. Dr Stephen Hayes
 The GP s approach to the patient who is worried about sun, skin and moles Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Dr Stephen Hayes DECLARATION OF INTERESTS
The GP s approach to the patient who is worried about sun, skin and moles Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Dr Stephen Hayes DECLARATION OF INTERESTS
Rosettes in actinic keratosis and squamous cell carcinoma: distribution, association to other dermoscopic signs and description of the rosette pattern
 DOI: 10.1111/jdv.14474 JEADV ORIGINAL ARTICLE Rosettes in actinic keratosis and squamous cell carcinoma: distribution, association to other dermoscopic signs and description of the rosette pattern B. Lozano-Masdemont,
DOI: 10.1111/jdv.14474 JEADV ORIGINAL ARTICLE Rosettes in actinic keratosis and squamous cell carcinoma: distribution, association to other dermoscopic signs and description of the rosette pattern B. Lozano-Masdemont,
Gross Appearance & Histology of Skin Cancer. Kyle Mannion M.D. January 21, 2005
 Gross Appearance & Histology of Skin Cancer Kyle Mannion M.D. January 21, 2005 Actinic Keratosis 5-20% will develop squamous/basal cell ca Almost solely from solar damage Usually develop during 4 th decade
Gross Appearance & Histology of Skin Cancer Kyle Mannion M.D. January 21, 2005 Actinic Keratosis 5-20% will develop squamous/basal cell ca Almost solely from solar damage Usually develop during 4 th decade
MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2
 MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2 In the second part of our feature on pigmented skin lesions, dermatology specialist Dr Sweta Rai describes the steps to rational decision-making
MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2 In the second part of our feature on pigmented skin lesions, dermatology specialist Dr Sweta Rai describes the steps to rational decision-making
Actinic Keratoses and Bowen s disease
 Actinic Keratoses and Bowen s disease Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Actinic Keratoses and Bowen s disease Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest risk.
 Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
They can develop anywhere on the skin and also inside the mouth. They can develop in normal skin or where there is an existing skin mole.
 What are malignant melanomas? Malignant melanomas are one type of skin cancer. They can develop anywhere on the skin and also inside the mouth. They can develop in normal skin or where there is an existing
What are malignant melanomas? Malignant melanomas are one type of skin cancer. They can develop anywhere on the skin and also inside the mouth. They can develop in normal skin or where there is an existing
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Dermoscopy. Sir William Osler. Dermoscopy. Dermoscopy. Melanoma USA Primary Care Update Faculty Disclosure Statement
 Diagnostic Ability: Pigmented Lesions Ted Rosen, MD Baylor College of Medicine Houston, Texas Enhanced 2010 Primary Care Update Faculty Disclosure Statement Ted Rosen, MD Speakers Bureau: Abbott, Amgen,
Diagnostic Ability: Pigmented Lesions Ted Rosen, MD Baylor College of Medicine Houston, Texas Enhanced 2010 Primary Care Update Faculty Disclosure Statement Ted Rosen, MD Speakers Bureau: Abbott, Amgen,
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Diagnosis of Lentigo Maligna Melanoma. Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ
 Diagnosis of Lentigo Maligna Melanoma Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ Conflict of Interest: None Topics Epidemiology and Natural History Clinical and Histologic
Diagnosis of Lentigo Maligna Melanoma Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ Conflict of Interest: None Topics Epidemiology and Natural History Clinical and Histologic
LENTIGO SIMPLEX. Epidemiology
 LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
Abrupt Intralesional Color Change on Dermoscopy as a New Indicator of Early Superficial Spreading Melanoma in a Japanese Woman
 Published online: June 24, 2015 1662 6567/15/0072 0123$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: June 24, 2015 1662 6567/15/0072 0123$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Melanoma. Consultation on draft guideline - stakeholder comments. Comments to be submitted before 5pm on Friday 13 March 2015
 Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)