Narelle Hadlow, Peter Ward, Ken Sikaris
|
|
|
- Janis Mitchell
- 5 years ago
- Views:
Transcription

1 Narelle Hadlow, Peter Ward, Ken Sikaris
2 Analytes for consideration Vascular, renal and Na and water changes Consider physiology and review data Na, K, Cl, Urea, Cr, Osm Acid base status Consider physiology and review data Anion gap, bicarbonate
3 Data sources Published ranges Klajnbard, 2010 Clin Chem Lab Med, Danish, 801-subset, 6x in Preg, 391 no Cx,(Plasma, Vitros 950, Cobas Integra 400) Larsson, 2008, BJOG, Swedish, 52 normals, 9x in Preg, (Plasma, Abbott Archi) Lockitch 41 normal + Lit review, (Serum Ektachem 700) Gronowski various publications Abbassi-Ghanavati, 2009, ObsGyn, Database review-above and others Up to Date- various publications (Larsson, Lockitch, Bacq (LFT s), Ardawi, Davison (Osm) PathWest RI KEMH Vitros, Tertiary, Plasma Sonic data RI Serum. SEALS data RI



4 Important Information Sources 1. Normal pregnancies. 801 to 391 Normals, 6 samplings, Plasma, 2.5 and 97.5 percentiles and 90% CI 52 Normal, 9 samplings each Plasma Calc. Lower 2.5 percentile and Upper 97.5 percentile and 90% CI Nordic Ref Int Proj comparisons


5 Important Information Sources 2. Published Texts. Pregnancy RI Textbooks 41 normals studied, plus Literature review Data presented as follows with % of nonpregnant also given
6 Important Information Sources 3. Data Mining -SONIC Tests Thousands S Sodium: S Potassium: S Chloride: S Bicarbonate: S Urea: S Creatinine: S egfr: S Anion Gap: Haemolysis S Bilirubin: S C Bilirubin: S U Bilirubin: S ALP: S GGT: S ALT: S AST: S Total Protein: S Albumin: S Calcium: S Corr Calcium: S Phosphate: S Uric Acid: S LDH: P Glu Fast P Glu AM P Glu PM S Glu Fast S Glu AM S Glu PM

7 Na -Sonic
8 Vascular, renal and Na and water Physiology changes Data Proposed ranges Na, K, Cl, Bicarb, Urea, Cr

9 Vascular, renal and Na and water changes GFR % to 170 ml/min/1.73 m2 from cardiac output & renal Blood flow Creatinine Clearance 50% Creatinine and Urea 30% Eg Creatinine umol/l Sodium 3-5 mmol/l Osmolality up to 10 mmol/kg (nadir 10/40) Eg falls to ~ 270 mmol/kg median
10 Changes driven by Relaxin (Deng et al, Danielson et al, Conrad et al, Davison et al) Osmolality threshold Vasopressin secreted at lower Osm Thirst at lower Osmolality + Nitric Oxide + Endothelial Rec-NO pathway RELAXIN ILGF-from ovary corpus luteum Vasc. Resistance Renal Vasodilation (? Other effects on relaxin on afferent arteriole JGA myoendocrine cells- reduced stretch) RAS activation Systemic vasodilation Sympathetic activity water & Na ~-900 mmol plasma volume (1.5 L) Renal Blood Flow ~60% hcg GFR ~ 50% Creatinine HypoNa, Osmolality
11 Data summary Sodium SODIUM Bias assessment outcome No sign. method bias Summary Data: AACB mmol/l PREGNANT Non Pregnant Weeks Klanjbard mmol/l Larsson mmol/l Up to date mmol/l Lockitch mmol/l Gronowski N/P PathWest mmol/L Sonic Serum mmol/l SEALS mmol/l NOTE:Not Provided = N/P Note different starting points of Klanjbard and Larsson - higher Sonic ** T1: 0 97 days T2: days T3: days
12 Summary - SODIUM ( mmol/L AACB) Agreement Slightly lower, not much change (98% of Non Preg) ~ 2 mmol/l drop average- at upper and lower RI ( or last meeting suggested ) T1-T3 much the same Although minimal might be clinically significant ie provide reassurance
13 Data summary Potassium POTASSIUM Bias assessment outcome No sign. method bias Summary Data: AACB mmol/l Non Pregnant PREGNANT Weeks Klanjbard mmol/l Larsson mmol/l Up to date mmol/l Lockitch mmol/l Gronowski N/P PathWest mmol/l N/P Sonic Serum mmol/l SEALS mmol/l NOTE: Not Provided = N/P Klajnbard, Plasma Sep d < 4 hrs Larsson Plasma Lockitch Serum PathWest Plasma Sonic Serum

14 Summary -POTASSIUM ( mmol/l) P or S Slight drop ( ) begins early pregnancy 95% of NP with slight recovery later. T1-T3 much the same 0.2 would give Previously Proposed at AACB Harmonisation : mmol/l in serum Notes from last AACB Only 5% of 40,000 pregnant women had potassium about 4.5. Only 5% of 40,000 pregnant women had potassium below 3.6 URL of 4.8 includes the rise of potassium in 3 rd trimester (unknown mechanism).
15 Other analytes for Break Out discussion
16 Chloride CHLORIDE Bias assessment outcome No sign. method bias Summary Data: AACB mmol/l PREGNANT Non Pregnant Weeks Klanjbard N/P N/P Larsson mmol/l Up to date mmol/l Lockitch mmol/l Gronowski N/P PathWest mmol/l N/P Sonic Serum mmol/l SEALS mmol/l NOTE: Not Provided = N/P Slight Drop in Chloride

17 Summary CHLORIDE ( mmol/l S/P) Possible v small drop early, Slight rise later-? Clinically significant or not T1 T3 same Proposed last AACB meeting: mmol/l Serum Notes from last meeting Slightly lower for consistency - if everything else drops due to a dilutional effect, why doesn t chloride? RI based on acknowledging this trend and being pragmatic Drop in chloride is commensurate with bicarbonate decreasing.
18 Urea UREA Bias assessment outcome Summary Data: AACB No agreed range PREGNANT Non Pregnant Weeks Klanjbard mmol/l Larsson mmol/l Up to date 7-20 mg/dl Lockitch mmol/l Gronowski N/P PathWest 3-8 mmol/l Sonic Serum mmol/l SEALS mmol/l NOTE: Not Provided = N/P Significant decrease to 65-75% of normal
19 Summary UREA mmol/l Significant decrease to 63-75% of normal? Clinical significance Persistent over T1-T3 Proposed Last AACB meeting: mmol/l Tolerant interval Confirm with reanalysis of data plus contributed data for other platforms
20 Creatinine CREATININE Bias assessment outcome No sign. method bias Summary Data: AACB umol/l PREGNANT Non Pregnant Weeks Klanjbard umol/l Larsson umol/l Up to date mg/dl Lockitch umol/l Gronowski N/P PathWest umol/l <80 <75 <90 Sonic Serum umol/l SEALS umol/l NOTE: Not Provided = N/P Significant decrease to 70% of normal
21 Summary -CREATININE (45-90 umol/l S/P) Significant decrease over pregnancy -~70% of usual, Consistent T1-T3 Previous Discussion at AACB Lower creatinine in 2 nd trimester of pregnancy is less concerning than the similar trend for urea? Proposed: µmol/l Confirm with reanalysis of data plus contributed data for other platforms
 ph slightly alkalotic 7.4 7.")
22 Physiology of Acid Base changes Progesterone sensitivity to pco2 in medulla - respiration and ventilation Later gravid uterus, lung capacity mild hyperventilation Chronic mild respiratory alkalosis with metabolic compensation pco2 from 40 mm Hg to mm Hg Compensatory renal excretion of bicarbonate HCO 3 from 25 to 22 mmol/l ( 2-4 mmol/l) ph slightly alkalotic Pa O 2 maintained normal to sl.
23 Anion Gap ANION GAP Bias assessment outcome Summary Data: AACB - No agreed range PREGNANT Non Pregnant Weeks Klanjbard N/P N/P Larsson N/P N/P Up to date 7-16 mmol/l Lockitch mmol/l Gronowski N/P PathWest mmol/l S N/P Sonic Serum mmol/l(+k) SEALS NOT REPORTED NOT REPORTED NOTE: Not Provided = N/P Limited Data Steady or some report increase
24 Bicarbonate BICARBONATE Bias assessment outcome Summary Data: AACB mmol/l PREGNANT Non Pregnant Weeks Klanjbard N/P N/P Larsson N/P N/P Up to date mmol/l Lockitch mmol/l Gronowski N/P PathWest mmol/l Sonic Serum mmol/l SEALS mmol/l NOTE:Not Provided = N/P Decrease to 85 % of normal

25
26 Summary - ANION GAP and BICARBONATE (Bicarbonate mmol/l, P/S) Bicarbonate drops significantly 85% of non pregnant Over all T1-T3 Anion Gap Median is relatively steady (Lockitch suggests slight rise) Past discussion at AACB Proposed: Anion Gap Confirm with reanalysis of data plus contributed data for other platforms Proposed: Bicarb mmol/l Effect of hyperventilation in pregnancy Appears constant over pregnancy We need more data
27 Suggested Reference Intervals last AACB meeting Non Pregnant 1st / 2 nd / 3rd Trimester Little evidence of major trimester specific changes Sodium Potassium Chloride Bicarbonate Anion Gap Urea Creatinine
28 Thank you!

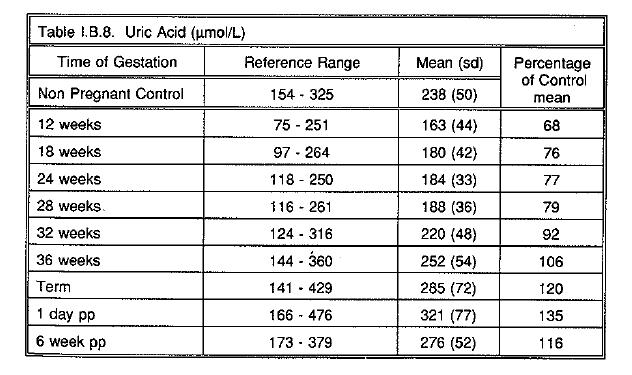
29 Uric Acid Normal handling complex free filtered, reasb pct, resecretion and re-absorption. Only 10% of filtered is excreted 8-16/40 UA clearance (? 2 nd to GFR) so levels ~ 25% After 20 weeks - Uric acid levels due to tubular reabsorption
30 Uric Acid URIC ACID Bias assessment outcome Summary Data: AACB Nil agreed PREGNANT Non Pregnant Weeks Klanjbard umol/l Larsson umol/l Up to date mg/dl Lockitch umol/l Gronowski umol/l PathWest mmol/l Specifically designed to accommodate 3rd trimester but no Pregnancy RI Sonic Serum mmol/l <0.31 <0.32 <0.33 <0.34 <0.35 <0.36 SEALS mmol/l NOTE: Not Provided = N/P

31 Klajnbard
32 Sonic Urate Sonic Urate T1 (0-97 days): mmol/l T2 ( days): mmol/l T3 ( days): mmol/l T3 ( days): mmol/l T3 ( days): mmol/l T3 ( days): mmol/l T3 ( days): mmol/l T3 ( days): mmol/l T3 ( days): mmol/l T3 ( days): mmol/l
33 Summary URIC ACID Significant change in UA Fall in UA early on -68% to later rise -106% T1 and T3 Different!! Rule of thumb 30/40 UA < /40 < 0.31 etc After 30 weeks, data agrees with clinician opinion Bhattacharaya analysis supports a rise of 0.01 mmol/l per week up to 38 weeks Proposed decision points: Up to 30 weeks <0.30 mmol/l weeks <0.36 mmol/l Urate in 1 st and 2 nd trimesters is predictive of where it will end up in 3 rd trimester Confirm with reanalysis of data plus contributed data for other platforms.
34 Osmolarity (mosm/kg H 2 O) OSMOLARITY Bias assessment outcome Summary Data: PREGNANT Non Pregnant Weeks Klanjbard N/P N/P Larsson N/P N/P Up to date mosmol/kg Lockitch N/P (+/- 4) Gronowski N/P PathWest NIL available Sonic Serum mosmol/kg (from Chart Data) SEALS mmol/kg NOTE: Not Provided = N/P PathWest Measured Sonic calculated (1.85(Na+K)+Urea+Gluc)
Reference Intervals. Graham Jones / Gus Koerbin
 Reference Intervals Graham Jones / Gus Koerbin Adult CRI - Harmonisation Harmonisation 1 2012: (13 tests + 1 calculation) Harmonisation 2 2013: Confirm 2012 recommendations. Discussed: albumin, globulin,
Reference Intervals Graham Jones / Gus Koerbin Adult CRI - Harmonisation Harmonisation 1 2012: (13 tests + 1 calculation) Harmonisation 2 2013: Confirm 2012 recommendations. Discussed: albumin, globulin,
Impact of Proposed HRI s on Laboratory Report Flagging Rates
 Impact of Proposed HRI s on Laboratory Report Flagging Rates A/Prof. Ken Sikaris Melbourne Pathology BSc(Hons), MBBS, FRCPA, FAACB, FFSc CBN 2011 WORKSHOP 2012 WORKSHOP 2013 WORKSHOP 2014 GENERAL CONCEPTS
Impact of Proposed HRI s on Laboratory Report Flagging Rates A/Prof. Ken Sikaris Melbourne Pathology BSc(Hons), MBBS, FRCPA, FAACB, FFSc CBN 2011 WORKSHOP 2012 WORKSHOP 2013 WORKSHOP 2014 GENERAL CONCEPTS
The Whats and Hows of Reference Intervals. Graham Jones Department of Chemical Pathology St Vincent s Hospital, Sydney
 The Whats and Hows of Reference Intervals Graham Jones Department of Chemical Pathology St Vincent s Hospital, Sydney Surabaya Indonesia 2016 Acknowledgements Reference Intervals - Summary What are they
The Whats and Hows of Reference Intervals Graham Jones Department of Chemical Pathology St Vincent s Hospital, Sydney Surabaya Indonesia 2016 Acknowledgements Reference Intervals - Summary What are they
Evidence Based Commutability: Bias 2 Study. Janice Gill Manager RCPAQAP Chemical Pathology Adelaide SA
 Evidence Based Commutability: Bias 2 Study Janice Gill Manager RCPAQAP Chemical Pathology Adelaide SA Australian Bias Studies conducted by Gus Koerbin, ACT Pathology on behalf of AACB Harmonisation Committee
Evidence Based Commutability: Bias 2 Study Janice Gill Manager RCPAQAP Chemical Pathology Adelaide SA Australian Bias Studies conducted by Gus Koerbin, ACT Pathology on behalf of AACB Harmonisation Committee
KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin
![KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin](/thumbs/87/96174332.jpg "KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin") Renal Physiology MCQ KD01 [Mar96] [Apr01] Renal blood flow is dependent on: A. Juxtaglomerular apparatus B. [Na+] at macula densa C. Afferent vasodilatation D. Arterial pressure (poorly worded/recalled
Renal Physiology MCQ KD01 [Mar96] [Apr01] Renal blood flow is dependent on: A. Juxtaglomerular apparatus B. [Na+] at macula densa C. Afferent vasodilatation D. Arterial pressure (poorly worded/recalled
The kidney. (Pseudo) Practical questions. The kidneys are all about keeping the body s homeostasis. for questions Ella
 Practical questions. The kidneys are all about keeping the body s homeostasis. for questions Ella") The kidney (Pseudo) Practical questions for questions Ella (striemit@gmail.com) The kidneys are all about keeping the body s homeostasis Ingestion Product of metabolism H 2 O Ca ++ Cl - K + Na + H 2 O
The kidney (Pseudo) Practical questions for questions Ella (striemit@gmail.com) The kidneys are all about keeping the body s homeostasis Ingestion Product of metabolism H 2 O Ca ++ Cl - K + Na + H 2 O
Quality Initiative In Pathology. Harmonisation of Laboratory Testing
 Quality Initiative In Pathology Harmonisation of Laboratory Testing Harmonisation: what do we mean? Agreement of test results irrespective of the method used or the testing laboratory Requires: Common
Quality Initiative In Pathology Harmonisation of Laboratory Testing Harmonisation: what do we mean? Agreement of test results irrespective of the method used or the testing laboratory Requires: Common
Breakout Session C: Harmonisation of the Alert Table.
 Breakout Session C: Harmonisation of the Alert Table. RCPA-AACB High Risk Results Working Party Andrew Georgiou Craig Campbell Grahame Caldwell Hans Schneider Penelope Coates Que Lam Rita Horvath Robert
Breakout Session C: Harmonisation of the Alert Table. RCPA-AACB High Risk Results Working Party Andrew Georgiou Craig Campbell Grahame Caldwell Hans Schneider Penelope Coates Que Lam Rita Horvath Robert
mid ihsan (Physiology ) GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B **
 GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B **") (Physiology ) mid ihsan GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B ** Colloid pressure in the efferent arteriole is: A- More than that leaving
(Physiology ) mid ihsan GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B ** Colloid pressure in the efferent arteriole is: A- More than that leaving
ROTUNDA HOSPITAL DEPARTMENT OF LABORATORY MEDICINE
 This active test table informs the user of Biochemistry tests available in house. s referred to other sites are recorded in the Referred Table. Issue date: 4 TH April 2016 Contact Phone Number ext.1345/2522
This active test table informs the user of Biochemistry tests available in house. s referred to other sites are recorded in the Referred Table. Issue date: 4 TH April 2016 Contact Phone Number ext.1345/2522
Provided by MedicalStudentExams.com NORMAL LABORATORY VALUES
 NORMAL LABORATORY VALUES 1. BLOOD, PLASMA, SERUM 2. CEREBROSPINAL FLUID 3. HEMATOLOGIC 4. SWEAT 5. URINE 6. SYNOVIAL FLUID 7. TOXIC LEVELS 8. Tumour Markers 9. Differential of Cerebral Spinal Fluid 10.
NORMAL LABORATORY VALUES 1. BLOOD, PLASMA, SERUM 2. CEREBROSPINAL FLUID 3. HEMATOLOGIC 4. SWEAT 5. URINE 6. SYNOVIAL FLUID 7. TOXIC LEVELS 8. Tumour Markers 9. Differential of Cerebral Spinal Fluid 10.
GENERAL. Compulsory module GEN II Example questions (Acute and Routine Clinical Chemistry)
") GENERAL Compulsory module GEN II Example questions (Acute and Routine Clinical Chemistry) ESSAY ANSWER QUESTIONS 2 Questions - each question is worth 35 marks.all questions should be attempted Question
GENERAL Compulsory module GEN II Example questions (Acute and Routine Clinical Chemistry) ESSAY ANSWER QUESTIONS 2 Questions - each question is worth 35 marks.all questions should be attempted Question
Physiology questions review
 Physiology questions review 1- The consumption of O2 by the kidney: a- decrease as blood flow increases b- regulated by erythropoiten c- remains constant as blood flow increase d- direct reflects the level
Physiology questions review 1- The consumption of O2 by the kidney: a- decrease as blood flow increases b- regulated by erythropoiten c- remains constant as blood flow increase d- direct reflects the level
Water, Electrolytes, and Acid-Base Balance
 Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Authorised: JSWoodford, Lead of Speciality. Biochemistry Reference Intervals, October Page 1 of 5
 AFP All All < 15 ug/l Albumin All 0-3M 25-40 g/l Albumin All 3-12M 32-45 g/l Albumin All 1-70Y 34-48 g/l Albumin All >70Y 32-46 g/l Alk Phos All 0-10Y 80-350 U/L Alk Phos M 10-14Y 45-400 U/L Alk Phos F
AFP All All < 15 ug/l Albumin All 0-3M 25-40 g/l Albumin All 3-12M 32-45 g/l Albumin All 1-70Y 34-48 g/l Albumin All >70Y 32-46 g/l Alk Phos All 0-10Y 80-350 U/L Alk Phos M 10-14Y 45-400 U/L Alk Phos F
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
General Chemistry Scheme Guide
 General Chemistry Scheme Guide Copyright WEQAS. All rights reserved. No part of this document may be reproduced or utilised in any form without permission from WEQAS Contents. Scheme details and repertoire.....
General Chemistry Scheme Guide Copyright WEQAS. All rights reserved. No part of this document may be reproduced or utilised in any form without permission from WEQAS Contents. Scheme details and repertoire.....
What tests should be on the Alert List?
 What tests should be on the Alert List? Dr Que Lam On behalf RCPA-AACB High Risk Results Working Party: Alan McNeil, Grahame Caldwell, Craig Campbell, Penelope Coates, Robert Flatman, Andrew Georgiou,
What tests should be on the Alert List? Dr Que Lam On behalf RCPA-AACB High Risk Results Working Party: Alan McNeil, Grahame Caldwell, Craig Campbell, Penelope Coates, Robert Flatman, Andrew Georgiou,
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Questions? Homework due in lab 6. PreLab #6 HW 15 & 16 (follow directions, 6 points!)
") Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Chemistry Reference Ranges and Critical Values
 Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-25 U/L 10-35 U/L 10-30 U/L 10-25 U/L 10-30 U/L 10-35 U/L 10-25 U/L 10-35 U/L 10-25 U/L 10-20 U/L 10-35 U/L Albumin 0-6
Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-25 U/L 10-35 U/L 10-30 U/L 10-25 U/L 10-30 U/L 10-35 U/L 10-25 U/L 10-35 U/L 10-25 U/L 10-20 U/L 10-35 U/L Albumin 0-6
Chemistry Reference Ranges and Critical Values
 Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-30 U/L 10-30 U/L 10-20 U/L Albumin 0-6 days 6 days - 37 months 37 months - 7 years 7-20 years 2.6-3.6 g/dl 3.4-4.2 g/dl
Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-30 U/L 10-30 U/L 10-20 U/L Albumin 0-6 days 6 days - 37 months 37 months - 7 years 7-20 years 2.6-3.6 g/dl 3.4-4.2 g/dl
Renal physiology D.HAMMOUDI.MD
 Renal physiology D.HAMMOUDI.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood glucose
Renal physiology D.HAMMOUDI.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood glucose
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Chapter 23. Composition and Properties of Urine
 Chapter 23 Composition and Properties of Urine Composition and Properties of Urine (1 of 2) urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless
Chapter 23 Composition and Properties of Urine Composition and Properties of Urine (1 of 2) urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless
Acid and Base Balance
 Acid and Base Balance 1 2 The Body and ph Homeostasis of ph is tightly controlled Extracellular fluid = 7.4 Blood = 7.35 7.45 < 7.35: Acidosis (acidemia) > 7.45: Alkalosis (alkalemia) < 6.8 or > 8.0: death
Acid and Base Balance 1 2 The Body and ph Homeostasis of ph is tightly controlled Extracellular fluid = 7.4 Blood = 7.35 7.45 < 7.35: Acidosis (acidemia) > 7.45: Alkalosis (alkalemia) < 6.8 or > 8.0: death
Acid Base Balance. Professor Dr. Raid M. H. Al-Salih. Clinical Chemistry Professor Dr. Raid M. H. Al-Salih
 Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Tables of Normal Values (As of February 2005)
") Tables of Normal Values (As of February 2005) Note: Values and units of measurement listed in these Tables are derived from several resources. Substantial variation exists in the ranges quoted as normal
Tables of Normal Values (As of February 2005) Note: Values and units of measurement listed in these Tables are derived from several resources. Substantial variation exists in the ranges quoted as normal
Setting of quality standards
 Setting of quality standards Graham Jones Department of Chemical Pathology St Vincent s Hospital, Sydney AACB ASM Adelaide October 2014 Setting of Quality Standards - 2013 The 2013 QC workshop revealed
Setting of quality standards Graham Jones Department of Chemical Pathology St Vincent s Hospital, Sydney AACB ASM Adelaide October 2014 Setting of Quality Standards - 2013 The 2013 QC workshop revealed
RENAL PHYSIOLOGY. Physiology Unit 4
 RENAL PHYSIOLOGY Physiology Unit 4 Renal Functions Primary Function is to regulate the chemistry of plasma through urine formation Additional Functions Regulate concentration of waste products Regulate
RENAL PHYSIOLOGY Physiology Unit 4 Renal Functions Primary Function is to regulate the chemistry of plasma through urine formation Additional Functions Regulate concentration of waste products Regulate
Acid-Base Balance Workshop. Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli
 Acid-Base Balance Workshop Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli Objectives Normal Acid-Base Physiology Simple Acid-Base Disorders Compensations and Disorders The Anion Gap Mixed
Acid-Base Balance Workshop Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli Objectives Normal Acid-Base Physiology Simple Acid-Base Disorders Compensations and Disorders The Anion Gap Mixed
Acids and Bases their definitions and meanings
 Acids and Bases their definitions and meanings Molecules containing hydrogen atoms that can release hydrogen ions in solutions are referred to as acids. (HCl H + Cl ) (H 2 CO 3 H + HCO 3 ) A base is an
Acids and Bases their definitions and meanings Molecules containing hydrogen atoms that can release hydrogen ions in solutions are referred to as acids. (HCl H + Cl ) (H 2 CO 3 H + HCO 3 ) A base is an
Guidelines for approach to a child with
 Guidelines for approach to a child with Metabolic acidosis (including RTA) Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith
Guidelines for approach to a child with Metabolic acidosis (including RTA) Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith
Stability of VACUETTE Lithium Heparin Separator tubes with modified centrifugation conditions
 Stability of VACUETTE Lithium Heparin Separator tubes with modified centrifugation conditions Background: Greiner-Bio-One, Austria has been selling plastic evacuated tubes (VACUETTE ) for venous blood
Stability of VACUETTE Lithium Heparin Separator tubes with modified centrifugation conditions Background: Greiner-Bio-One, Austria has been selling plastic evacuated tubes (VACUETTE ) for venous blood
Date... Name... Group... Urine sample (Tube No 2)
") Date... Name... Group... Instructions for the practical lesson on biochemistry Topic: Non-protein nitrogen compounds Task 1: Estimation of creatinine in serum and urine 1. Trichloroacetic acid 1.22 mol/l
Date... Name... Group... Instructions for the practical lesson on biochemistry Topic: Non-protein nitrogen compounds Task 1: Estimation of creatinine in serum and urine 1. Trichloroacetic acid 1.22 mol/l
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
1. remove: waste products: urea, creatinine, and uric acid foreign chemicals: drugs, water soluble vitamins, and food additives, etc.
 Making Water! OR is it really Just Water Just Ask the Nephron!! Author: Patricia L. Ostlund ostlundp@faytechcc.edu (910) 678-9892 Fayetteville Technical Community College Fayetteville, NC 28303 Its just
Making Water! OR is it really Just Water Just Ask the Nephron!! Author: Patricia L. Ostlund ostlundp@faytechcc.edu (910) 678-9892 Fayetteville Technical Community College Fayetteville, NC 28303 Its just
Acid-Base Tutorial 2/10/2014. Overview. Physiology (2) Physiology (1)
 Physiology (1)") Overview Acid-Base Tutorial Nicola Barlow Physiology Buffering systems Control mechanisms Laboratory assessment of acid-base Disorders of H + ion homeostasis Respiratory acidosis Metabolic acidosis Respiratory
Overview Acid-Base Tutorial Nicola Barlow Physiology Buffering systems Control mechanisms Laboratory assessment of acid-base Disorders of H + ion homeostasis Respiratory acidosis Metabolic acidosis Respiratory
Filtration and Reabsorption Amount Filter/d
 Renal Physiology 2011 Lisa M. Harrison-Bernard, PhD Contact me at lharris@lsuhsc.edu Renal Physiology Lecture 3 Renal Clearance and Glomerular Filtration Filtration and Reabsorption Amount Filter/d Amount
Renal Physiology 2011 Lisa M. Harrison-Bernard, PhD Contact me at lharris@lsuhsc.edu Renal Physiology Lecture 3 Renal Clearance and Glomerular Filtration Filtration and Reabsorption Amount Filter/d Amount
Confirmation - A Practical Approach
 Data Mining i for Reference Interval Confirmation - A Practical Approach Graham Jones Chemical Pathologist St Vincent s Hospital, Sydney AACB Webinar 5 th June 2013 Summary A little (more) background Current
Data Mining i for Reference Interval Confirmation - A Practical Approach Graham Jones Chemical Pathologist St Vincent s Hospital, Sydney AACB Webinar 5 th June 2013 Summary A little (more) background Current
1. What is the acid-base disturbance in this patient?
 /ABG QUIZ QUIZ 1. What is the acid-base disturbance in this patient? Presenting complaint: pneumonia 1 point Uncompensated metabolic alkalosis Partially compensated respiratory alkalosis Mixed alkalosis
/ABG QUIZ QUIZ 1. What is the acid-base disturbance in this patient? Presenting complaint: pneumonia 1 point Uncompensated metabolic alkalosis Partially compensated respiratory alkalosis Mixed alkalosis
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Functions of Proximal Convoluted Tubules
 1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
Ren e a n l a l f un u c n t c io i n o s n Biochemistry II Lecture (J.S.) 1
 1") Renal functions Biochemistry II Lecture 10 2008 (J.S.) 1 The main functions of the kidneys Maintaining of the composition, osmolality, and volume of ECF Excretion of nitrogenous catabolites (urea, uric
Renal functions Biochemistry II Lecture 10 2008 (J.S.) 1 The main functions of the kidneys Maintaining of the composition, osmolality, and volume of ECF Excretion of nitrogenous catabolites (urea, uric
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Urine Formation. Urinary Physiology Urinary Section pages Urine Formation. Glomerular Filtration 4/24/2016
 Urine Formation Urinary Physiology Urinary Section pages 9-17 Filtrate Blood plasma minus most proteins Urine
Urine Formation Urinary Physiology Urinary Section pages 9-17 Filtrate Blood plasma minus most proteins Urine
Ch 17 Physiology of the Kidneys
 Ch 17 Physiology of the Kidneys Review Anatomy on your own SLOs List and describe the 4 major functions of the kidneys. List and explain the 4 processes of the urinary system. Diagram the filtration barriers
Ch 17 Physiology of the Kidneys Review Anatomy on your own SLOs List and describe the 4 major functions of the kidneys. List and explain the 4 processes of the urinary system. Diagram the filtration barriers
Terminology. Terminology. Terminology. Molarity number of moles of solute / Liter of solution. a) Terminology b) Body Fluid Compartments
 Terminology b) Body Fluid Compartments") Integrative Sciences: Biological Systems A Fall 2011 Body Fluids Compartments, Renal Clearance and Renal Excretion of Drugs Monday, November 21, 2011 Lisa M. Harrison-Bernard, Ph.D. Department of Physiology;
Integrative Sciences: Biological Systems A Fall 2011 Body Fluids Compartments, Renal Clearance and Renal Excretion of Drugs Monday, November 21, 2011 Lisa M. Harrison-Bernard, Ph.D. Department of Physiology;
Harmonisation of Reference Ranges
 Harmonisation of Reference Ranges Ken Sikaris BSc(Hons), MBBS, FRCPA, FAACB, FFSc Vice President, AACB (Education) Chemical Pathologist, Melbourne Pathology Director of Clinical Support Systems, Sonic
Harmonisation of Reference Ranges Ken Sikaris BSc(Hons), MBBS, FRCPA, FAACB, FFSc Vice President, AACB (Education) Chemical Pathologist, Melbourne Pathology Director of Clinical Support Systems, Sonic
Introduction to the kidney: regulation of sodium & glucose. Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health
 Introduction to the kidney: regulation of sodium & glucose Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health Objectives Overview of kidney structure & function Glomerular
Introduction to the kidney: regulation of sodium & glucose Dr Nick Ashton Senior Lecturer in Renal Physiology Faculty of Biology, Medicine & Health Objectives Overview of kidney structure & function Glomerular
Dr Bill Bartlett Blood Sciences, Ninewells Hospital & Medical School, NHS Tayside, Scotland, UK.
 Dr Bill Bartlett Blood Sciences, Ninewells Hospital & Medical School, NHS Tayside, Scotland, UK. Bill.Bartlett@nhs.net www.biologicalvariation.com Biological variation affects the clinical utility of reference
Dr Bill Bartlett Blood Sciences, Ninewells Hospital & Medical School, NHS Tayside, Scotland, UK. Bill.Bartlett@nhs.net www.biologicalvariation.com Biological variation affects the clinical utility of reference
RENAL TUBULAR ACIDOSIS An Overview
 RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
Chapter 15 Fluid and Acid-Base Balance
 Chapter 15 Fluid and Acid-Base Balance by Dr. Jay M. Templin Brooks/Cole - Thomson Learning Fluid Balance Water constitutes ~60% of body weight. All cells and tissues are surrounded by an aqueous environment.
Chapter 15 Fluid and Acid-Base Balance by Dr. Jay M. Templin Brooks/Cole - Thomson Learning Fluid Balance Water constitutes ~60% of body weight. All cells and tissues are surrounded by an aqueous environment.
(KFTs) IACLD CME, Monday, February 20, Mohammad Reza Bakhtiari, DCLS, PhD
 IACLD CME, Monday, February 20, Mohammad Reza Bakhtiari, DCLS, PhD") Kidney Function Tests (KFTs) IACLD CME, Monday, February 20, 2012 Mohammad Reza Bakhtiari, DCLS, PhD Iranian Research Organization for Science & Technology (IROST) Tehran, Iran Composition and Properties
Kidney Function Tests (KFTs) IACLD CME, Monday, February 20, 2012 Mohammad Reza Bakhtiari, DCLS, PhD Iranian Research Organization for Science & Technology (IROST) Tehran, Iran Composition and Properties
Lecture 16: The Nephron
 Lecture 16: The Nephron Reading: OpenStax A&P Text Chapter 25 Primary functions of the kidneys 1. Regulating osmolarity (blood concentration!) A. Regulating blood pressure B. Maintaining ion balance C.
Lecture 16: The Nephron Reading: OpenStax A&P Text Chapter 25 Primary functions of the kidneys 1. Regulating osmolarity (blood concentration!) A. Regulating blood pressure B. Maintaining ion balance C.
H 2 O, Electrolytes and Acid-Base Balance
 H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
Global Report #01 27/11/2013. Patient percentile monitoring compared to internal quality control (IQC) monitoring
 monitoring") Patient Percentile Monitoring Global Report #01 CONTENT Project status Patient percentile monitoring compared to internal quality control (IQC) monitoring Comparison of outpatient/all patient monitoring
Patient Percentile Monitoring Global Report #01 CONTENT Project status Patient percentile monitoring compared to internal quality control (IQC) monitoring Comparison of outpatient/all patient monitoring
Biochemistry of acid-base disorders. Alice Skoumalová
 Biochemistry of acid-base disorders Alice Skoumalová Main topics of the lecture: Measurement of acid-base dysbalance Classification of the acid-base disorders 4 basic acid-base disorders and their compensaiton
Biochemistry of acid-base disorders Alice Skoumalová Main topics of the lecture: Measurement of acid-base dysbalance Classification of the acid-base disorders 4 basic acid-base disorders and their compensaiton
BUFFERING OF HYDROGEN LOAD
 BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
Acid-Base Balance 11/18/2011. Regulation of Potassium Balance. Regulation of Potassium Balance. Regulatory Site: Cortical Collecting Ducts.
 Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
BIOL2030 Human A & P II -- Exam 6
 BIOL2030 Human A & P II -- Exam 6 Name: 1. The kidney functions in A. preventing blood loss. C. synthesis of vitamin E. E. making ADH. B. white blood cell production. D. excretion of metabolic wastes.
BIOL2030 Human A & P II -- Exam 6 Name: 1. The kidney functions in A. preventing blood loss. C. synthesis of vitamin E. E. making ADH. B. white blood cell production. D. excretion of metabolic wastes.
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
RENAL PHYSIOLOGY. Danil Hammoudi.MD
 RENAL PHYSIOLOGY Danil Hammoudi.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood
RENAL PHYSIOLOGY Danil Hammoudi.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood
Coping with Analytical Interferences
 Coping with Analytical Interferences (Handling Icteric, Hemolytic and Lipaemic Samples) Graham Jones Department of Chemical Pathology St Vincent s Hospital, Sydney Surabaya Indonesia 2016 Acknowledgements
Coping with Analytical Interferences (Handling Icteric, Hemolytic and Lipaemic Samples) Graham Jones Department of Chemical Pathology St Vincent s Hospital, Sydney Surabaya Indonesia 2016 Acknowledgements
Physio 12 -Summer 02 - Renal Physiology - Page 1
 Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University
 Metabolic Acidosis Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com
Metabolic Acidosis Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com
Acid-Base Physiology. Dr. Tamás Bense Dr. Alexandra Turi
 Acid-Base Physiology Dr. Tamás Bense Dr. Alexandra Turi What is a blood gas assessment? We get it from an arterial sample (a.radialis, a. brachialis, a. femoralis) Invasive technique If the patient is
Acid-Base Physiology Dr. Tamás Bense Dr. Alexandra Turi What is a blood gas assessment? We get it from an arterial sample (a.radialis, a. brachialis, a. femoralis) Invasive technique If the patient is
SydPath Reference Intervals for Clinical Trials (Contract Pathology Unit) Unauthorised Copy
 Unauthorised Copy") HAEMATOLOGY APTT 1 150 M 25 35 sec APTT 1 150 F 25 35 sec Basophils Cord 2 weeks M 0.0 0.4 10^9/L Basophils Cord 2 weeks F 0.0 0.4 10^9/L Basophils 2 wks 3 mths M 0.0 0.2 10^9/L Basophils 2 wks 3 mths
HAEMATOLOGY APTT 1 150 M 25 35 sec APTT 1 150 F 25 35 sec Basophils Cord 2 weeks M 0.0 0.4 10^9/L Basophils Cord 2 weeks F 0.0 0.4 10^9/L Basophils 2 wks 3 mths M 0.0 0.2 10^9/L Basophils 2 wks 3 mths
Physiology week 16 Renal 2 (volume/buffers)
") Physiology week 16 Renal 2 (volume/buffers) Defense of Tonicity and Volume Defense of tonicity Tonicity = osmolality of a solution relative to plasma Osmolality measures [ ] all particles in solution,
Physiology week 16 Renal 2 (volume/buffers) Defense of Tonicity and Volume Defense of tonicity Tonicity = osmolality of a solution relative to plasma Osmolality measures [ ] all particles in solution,
Renal physiology II. Basic renal processes. Dr Alida Koorts BMS
 Renal physiology II Basic renal processes Dr Alida Koorts BMS 7-12 012 319 2921 akoorts@medic.up.ac.za Basic renal processes 1. filtration 2. reabsorption 3. secretion Glomerular filtration The filtration
Renal physiology II Basic renal processes Dr Alida Koorts BMS 7-12 012 319 2921 akoorts@medic.up.ac.za Basic renal processes 1. filtration 2. reabsorption 3. secretion Glomerular filtration The filtration
REFERENCE INTERVALS. Units Canine Feline Bovine Equine Porcine Ovine
 REFERENCE INTERVALS Biochemistry Units Canine Feline Bovine Equine Porcine Ovine Sodium mmol/l 144-151 149-156 135-151 135-148 140-150 143-151 Potassium mmol/l 3.9-5.3 3.3-5.2 3.9-5.9 3.0-5.0 4.7-7.1 4.6-7.0
REFERENCE INTERVALS Biochemistry Units Canine Feline Bovine Equine Porcine Ovine Sodium mmol/l 144-151 149-156 135-151 135-148 140-150 143-151 Potassium mmol/l 3.9-5.3 3.3-5.2 3.9-5.9 3.0-5.0 4.7-7.1 4.6-7.0
Renal System Physiology
 M58_MARI0000_00_SE_EX09.qxd 7/18/11 2:37 PM Page 399 E X E R C I S E 9 Renal System Physiology Advance Preparation/Comments 1. Prior to the lab, suggest to the students that they become familiar with the
M58_MARI0000_00_SE_EX09.qxd 7/18/11 2:37 PM Page 399 E X E R C I S E 9 Renal System Physiology Advance Preparation/Comments 1. Prior to the lab, suggest to the students that they become familiar with the
Copyright 2009 Pearson Education, Inc. Copyright 2009 Pearson Education, Inc. Figure 19-1c. Efferent arteriole. Juxtaglomerular apparatus
 /6/0 About this Chapter Functions of the Kidneys Anatomy of the urinary system Overview of kidney function Secretion Micturition Regulation of extracellular fluid volume and blood pressure Regulation of
/6/0 About this Chapter Functions of the Kidneys Anatomy of the urinary system Overview of kidney function Secretion Micturition Regulation of extracellular fluid volume and blood pressure Regulation of
Renal-Related Questions
 Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Evaluation of VACUETTE CAT Serum Fast Separator Blood Collection Tube for Routine Chemistry Analytes in Comparison to VACUTAINER RST Tube
 Evaluation of VACUETTE CAT Serum Fast Separator Blood Collection Tube for Routine Chemistry Analytes in Comparison to VACUTAINER RST Tube Background: Greiner-Bio-One, Austria has been selling plastic evacuated
Evaluation of VACUETTE CAT Serum Fast Separator Blood Collection Tube for Routine Chemistry Analytes in Comparison to VACUTAINER RST Tube Background: Greiner-Bio-One, Austria has been selling plastic evacuated
10 Essential Blood Tests PART 1
 Presents 10 Essential Blood Tests PART 1 The Blood Chemistry Webinars With DR. DICKEN WEATHERBY Creator of the Blood Chemistry Software Essential Blood Test #1: Basic Chem Screen and CBC http://bloodchemsoftware.com
Presents 10 Essential Blood Tests PART 1 The Blood Chemistry Webinars With DR. DICKEN WEATHERBY Creator of the Blood Chemistry Software Essential Blood Test #1: Basic Chem Screen and CBC http://bloodchemsoftware.com
Comparison of VACUETTE Heparin Gel Tubes for Common Chemistry Analytes
 Comparison of VACUETTE Heparin Gel Tubes for Common Chemistry Analytes Background: Greiner-Bio-One, Austria has been selling plastic evacuated tubes (VACUETTE ) for venous blood collection since 9. The
Comparison of VACUETTE Heparin Gel Tubes for Common Chemistry Analytes Background: Greiner-Bio-One, Austria has been selling plastic evacuated tubes (VACUETTE ) for venous blood collection since 9. The
Traceability in External Quality Assessment: How Weqas ensures traceability in EQA and stresses its importance to users. David Ducroq.
 Traceability in External Quality Assessment: How Weqas ensures traceability in EQA and stresses its importance to users David Ducroq Weqas Unit 6, Parc Tŷ Glas Llanishen Cardiff UK www.weqas.com Programme
Traceability in External Quality Assessment: How Weqas ensures traceability in EQA and stresses its importance to users David Ducroq Weqas Unit 6, Parc Tŷ Glas Llanishen Cardiff UK www.weqas.com Programme
Schedule of Accreditation issued by United Kingdom Accreditation Service 2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK
 2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK Biochemistry Department University Hospital of North Durham Durham County Durham DH1 5TW Contact: Dr Tim Lang Tel: +44 (0) 191 333 2694 Fax:
2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK Biochemistry Department University Hospital of North Durham Durham County Durham DH1 5TW Contact: Dr Tim Lang Tel: +44 (0) 191 333 2694 Fax:
Non-Anion Gap Metabolic Acidosis. App.GoSoapbox.com then Join Now. Joel M. Topf, M.D.
 Non-Anion Gap Metabolic Acidosis App.GoSoapbox.com 665-971-584 then Join Now Joel M. Topf, M.D. http://pbfluids.com @kidney_boy App.GoSoapbox.com 665-971-584 32 y.o. female with fatigue, weakness and muscle
Non-Anion Gap Metabolic Acidosis App.GoSoapbox.com 665-971-584 then Join Now Joel M. Topf, M.D. http://pbfluids.com @kidney_boy App.GoSoapbox.com 665-971-584 32 y.o. female with fatigue, weakness and muscle
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
** Accordingly GFR can be estimated by using one urine sample and do creatinine testing.
 This sheet includes the lecture and last year s exam. When a patient goes to a clinic, we order 2 tests: 1) kidney function test: in which we measure UREA and CREATININE levels, and electrolytes (Na+,
This sheet includes the lecture and last year s exam. When a patient goes to a clinic, we order 2 tests: 1) kidney function test: in which we measure UREA and CREATININE levels, and electrolytes (Na+,
Biochemistry case studies. Dr Narelle Hadlow Clinical Associate Professor School of Medicine, UWA
 Biochemistry case studies Dr Narelle Hadlow Clinical Associate Professor School of Medicine, UWA 72 y.o. woman History of HT, diuretics History of hypertension, complains thirsty, feels under the weather
Biochemistry case studies Dr Narelle Hadlow Clinical Associate Professor School of Medicine, UWA 72 y.o. woman History of HT, diuretics History of hypertension, complains thirsty, feels under the weather
RENAL FUNCTION An Overview
 RENAL FUNCTION An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ. Temple 1 Kidneys
RENAL FUNCTION An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ. Temple 1 Kidneys
BIOCHEMICAL REPORT. Parameters Unit Finding Normal Value. Lipase U/L Amylase U/L
 Lipase U/L 88.9 10-195 Amylase U/L 1181.1 371.3-1192.6 West Delhi :- 7/148, Opp. MCD Office, Major Pankaj Batra Marg, Near Ramesh Nagar, New Delhi-15, Ph. : 011-47562566,9999830187 Liver Function Test
Lipase U/L 88.9 10-195 Amylase U/L 1181.1 371.3-1192.6 West Delhi :- 7/148, Opp. MCD Office, Major Pankaj Batra Marg, Near Ramesh Nagar, New Delhi-15, Ph. : 011-47562566,9999830187 Liver Function Test
MODULE 8: URINALYSIS AND ACID BASE BALANCE
 MODULE 8: URINALYSIS AND ACID BASE BALANCE This lab involves a tutorial that teaches you how to analyze a urine reagent strip. If you are taking the lab on campus, you will be given the opportunity to
MODULE 8: URINALYSIS AND ACID BASE BALANCE This lab involves a tutorial that teaches you how to analyze a urine reagent strip. If you are taking the lab on campus, you will be given the opportunity to
ACID/BASE. A. What is her acid-base disorder, what is her anion gap, and what is the likely cause?
 These fluid and electrolyte problems are modified from those in a previous textbook for this sequence, Renal Pathophysiology edited by James A. Shayman M.D., Professor of Internal Medicine, University
These fluid and electrolyte problems are modified from those in a previous textbook for this sequence, Renal Pathophysiology edited by James A. Shayman M.D., Professor of Internal Medicine, University
Evaluation Report of the Pneumatic Tube Transport System (PEVCO) connecting Dialysis Hospital to. Mubarak Hospital. Dr.
 connecting Dialysis Hospital to. Mubarak Hospital. Dr.") 5 Evaluation Report of the Transport System (PEVCO) connecting Dialysis Hospital to Mubarak Hospital Dr. Anwar AlAnjeri Senior Registrar Clinical Biochemistry Laboratory Mubarak Hospital Introduction:
5 Evaluation Report of the Transport System (PEVCO) connecting Dialysis Hospital to Mubarak Hospital Dr. Anwar AlAnjeri Senior Registrar Clinical Biochemistry Laboratory Mubarak Hospital Introduction:
Collin County Community College RENAL PHYSIOLOGY
 Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 12 Urinary System 1 RENAL PHYSIOLOGY Glomerular Filtration Filtration process that occurs in Bowman s Capsule Blood is filtered and
Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 12 Urinary System 1 RENAL PHYSIOLOGY Glomerular Filtration Filtration process that occurs in Bowman s Capsule Blood is filtered and
11/05/1431. Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate
 Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate Chapter 27 pages 327 347 1 OBJECTIVES At the end of this lecture you should be able to describe: Absorptive Characteristics
Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate Chapter 27 pages 327 347 1 OBJECTIVES At the end of this lecture you should be able to describe: Absorptive Characteristics
Renal Reabsorption & Secretion
 Renal Reabsorption & Secretion Topics for today: Nephron processing of filtrate Control of glomerular filtration Reabsorption and secretion Examples of solute clearance rates Hormones affecting kidney
Renal Reabsorption & Secretion Topics for today: Nephron processing of filtrate Control of glomerular filtration Reabsorption and secretion Examples of solute clearance rates Hormones affecting kidney
Acid-Base Imbalance-2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD
 Yanal A. Shafagoj MD. PhD") AcidBase Imbalance2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD Introduction Disturbance in acidbase balance are common clinical problem that range in severity from mild to life threatening, the acute
AcidBase Imbalance2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD Introduction Disturbance in acidbase balance are common clinical problem that range in severity from mild to life threatening, the acute
3/17/2017. Acid-Base Disturbances. Goal. Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine
 Acid-Base Disturbances Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders Discuss the approach
Acid-Base Disturbances Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders Discuss the approach
Renal Physiology Part II. Bio 219 Napa Valley College Dr. Adam Ross
 Renal Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Fluid and Electrolyte balance As we know from our previous studies: Water and ions need to be balanced in order to maintain proper homeostatic
Renal Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Fluid and Electrolyte balance As we know from our previous studies: Water and ions need to be balanced in order to maintain proper homeostatic
014 Chapter 14 Created: 9:25:14 PM CST
 014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
9/14/2017. Acid-Base Disturbances. Goal. Provide an approach to determine complex acid-base disorders
 Acid-Base Disturbances NCNP October 10, 2017 Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders
Acid-Base Disturbances NCNP October 10, 2017 Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders
Renal Physiology II Tubular functions
 Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
B. PANITUMUMAB DOSE LEVEL 0 No dose reduction 1 Level -1 2 Level Other, specify in comments for this cycle
 Radiation Therapy Oncology Group Phase II Study Pre-operative Chemo- Radiation + Panitumumab for Potentially Operable Lung Cancer Concurrent Summary Form AMENDED DATA YES INSTRUCTIONS: Submit all pages
Radiation Therapy Oncology Group Phase II Study Pre-operative Chemo- Radiation + Panitumumab for Potentially Operable Lung Cancer Concurrent Summary Form AMENDED DATA YES INSTRUCTIONS: Submit all pages