Faculty. Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty: Community Endocrine Group Albany, NY
|
|
|
- Hilda Dalton
- 5 years ago
- Views:
Transcription
1 Faculty Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty: Community Endocrine Group Albany, NY 2
2 Disclosures Robert S. Busch, MD, FACE serves as a speaker for Astra Zeneca, Eli Lilly, Boehringer Ingelheim and Novo Nordisk. 3
3 Learning Objectives 1. Recognize the importance of C-V risk management in the patient with Type 2 DM 2. Describe the mechanism of action and capabilities of PCSK-9 therapies 4
4 PATIENTS WITH DIABETES REMAIN AT INCREASED RISK FOR ASCVD EVENTS Events Per 10,000 Among Adults S (1994) HOPE (2000) Diabetes/Acute MI No Diabetes/Acute MI Diabetes/Stroke No Diabetes/Stroke Gregg EW, Li Y, Wang J, et al. Changes in Diabetes-Related Complications in the United States, N Engl J Med. 2014;370(16): Epub 2014/04/18. doi: /NEJMoa PubMed PMID: Risk 50 80% 5
5 Type 2 DM is a Progressive Disease CLINICAL DIAGNOSIS Glucose (mg/dl) Post-prandial Glucose Fasting Glucose Compensated β-cell Function Obesity Insulin Level Decreasing β-cell Function IGT Diabetes Insulin Resistance Uncontrolled hyperglycemia Relative Insulin Resistance Clinical Features Macrovascular changes Microvascular changes Years Adapted from Type 2 Diabetes BASICS: International Diabetes Center;
6 The Ticking Clock Hypothesis Type 2 DM is associated with microvascular and macrovascular complications. Duration of DM and severity of glycemia are primarily associated with microvascular disease. Metabolic disturbances during the prediabetic period may contribute to macrovascular disease. Macrovascular complications: the clock starts ticking years before the onset of clinical diabetes. Haffner SM et al. JAMA. 1990;263:
7 The ABC s of Diabetes A1C (and ASA) < 7.0% (ACE < 6.5%) Blood Pressure* < 140/90 mmhg (125/75 mmhg) Cholesterol** LDL-C < 100 mg/dl (<70 mg/dl?) Non-HDL-C < 130 mg/dl (<100 mg/dl?) HDL-C > 40 mg/dl (> 50 mg/dl in women) TG s < 150 mg/dl Smoking Cessation ADA. Standards of Medical Care in Diabetes Diabetes Care 2016;39:S1-S106. * JNC 8: < 140/90 mmhg AACE: <130/80 ** NCEP 4: high-dose statin therapy recommended; >50% LDL-C reduction 12
8 Steno Study Design 160 type 2 diabetics with microalbuminuria Randomized treatment assignments Conventional : Treatment for multiple risk factors from general practitioner, in accordance with 1988 Danish Medical Association guidelines Intensive : Treatment for multiple risk factors by a project team (physician, nurse, dietician) at Steno Diabetes Center, involving strict treatment goals Endpoints Primary: CV death, MI, CVA, revascularization, amputation Secondary: nephropathy, retinopathy, neuropathy Eight-year follow-up Gaede et al. N Engl J Med 2003;348:
9 Steno-2: Macrovascular Endpoints* 60 Percent with Event Conventional (n = 80) Intensive (n = 80) 53% RRR P = Years of Follow-Up *CV death, MI, CVA, revascularization, amputation Gaede et al. N Engl J Med 2003;348:
10 18
11 22% RRR The Heart Outcomes Prevention Evaluation Study Investigators. NEJM. 2000;342:
12 20
13 SIMVASTATIN: MAJOR VASCULAR EVENT by YEAR People suffering events (%) PLACEBO SIMVASTATIN Years of follow-up Benefit/1000 (SE): 5(3) 20(4) 35(5) 46(5) 54(7) 60(18) 21
14 SIMVASTATIN: CAUSE-SPECIFIC MORTALITY Cause of death SIMVASTATIN PLACEBO (10269) (10267) Rate ratio & 95% CI STATIN better PLACEBO better Vascular Coronary Other vascular ANY VASCULAR Non-vascular Neoplastic Respiratory Other medical Non-medical NON-VASCULAR ALL CAUSES (7.6%) (9.1%) (5.3%) (5.6%) (12.9%) (14.7%) 17% SE 4 reduction (2P<0.0001) 5% SE 6 reduction (NS) 13% SE 4 reduction (2P<0.001)
15 SIMVASTATIN: MAJOR VASCULAR EVENTS Vascular event SIMVASTATIN PLACEBO (10269) (10267) Rate ratio & 95% CI STATIN better PLACEBO better Major coronary Any stroke Revascularisation ANY OF ABOVE (19.8%) (25.2%) 24% SE 3 reduction (2P< )
16 CARDS 26

 One of : Hypertension defined as receiving antihypertensive treatment or")
17 Type 2 diabetes Males or females years of age CARDS Eligibility Criteria No clinical history of coronary, cerebrovascular or severe peripheral vascular disease LDL-C 4.14 mmol/l ( 160 mg/dl) TG 6.78 mmol/l ( 600 mg/dl) One of : Hypertension defined as receiving antihypertensive treatment or SBP 140 mm Hg or DBP 90 mm Hg Retinopathy Microalbuminuria or macroalbuminuria Current smoking 27
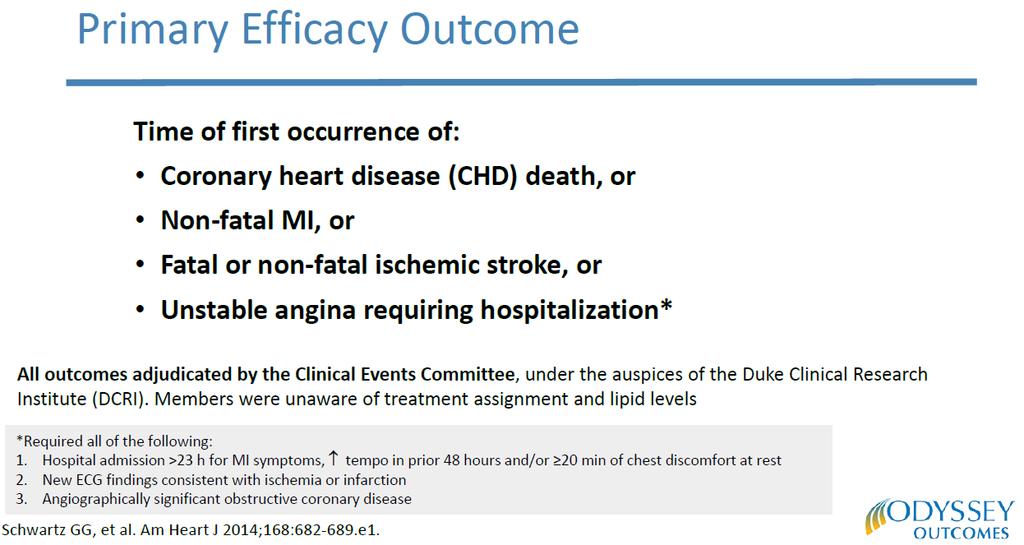
18 Primary Efficacy Parameters CARDS Endpoints Acute CHD death Non-fatal MI including silent MI Hospitalised unstable angina Resuscitated cardiac arrest Coronary revascularisation Stroke Major coronary events Secondary Efficacy Parameters Total mortality Any cardiovascular endpoint Lipid and lipoproteins
19 CARDS Patient Baseline Lipids* Total cholesterol (mmol/l) (mg/dl) Placebo Median (IQR) 5.4 ( ) 207 ( ) Atorvastatin Median (IQR) 5.4 ( ) 207 ( ) LDL-cholesterol (mmol/l) (mg/dl) 3.1 ( ) 118 ( ) 3.1 ( ) 119 ( ) HDL-cholesterol (mmol/l) (mg/dl) 1.4 ( ) 53 (46-61) 1.3 ( ) 52 (45-60) * Subject to final verification
20 Lipid Levels by Treatment 6 Total cholesterol (mmol/l) Average difference 26% 1.4 mmol/l (54mg/dL) p< LDL cholesterol (mmol/l) Average difference 40% 1.2 mmol/l (46mg/dL) p< Years of Study Years of Study Placebo Atorvastatin
21 Cumulative Hazard for Primary Endpoint Relative Risk Reduction 37% (95% CI: 17-52) Cumulative Hazard (%) P=0.001 Placebo 127 events Atorvastatin 83 events Placebo Atorva Years
22 Cumulative Hazard for All Cause Mortality Cumulative Hazard (%) Relative Risk Reduction 27% (95%CI: -1-48) p=0.059 Placebo 82 deaths Atorvastatin 61 deaths Years Placebo Atorva
23 June 3,
24 37

25 Ominous Octet DeFronzo RA. Diabetes. 2009;58:

26 Pro-Active Lancet 2005;366:
27 40
28 41
29 42

30 24% RRR 43 NEJM Feb 17, 2016 DOI: /NEJMoa
31 44
32 45
33 SAVOR-TIMI-53 EXAMINE Patients with endpoint (%) T2D; HbA 1c %; 40 years + CVD; 55 (men) or 60 (women) years + CV risk factors (n=16,492) Saxagliptin (2.5 or 5 mg/day**) + standard of care Placebo + standard of care Patients with endpoint (%) T2D; HbA 1c %; ACS within days (n=5380) Alogliptin (6.25, 12.5 or 25 mg/day*) + standard of care Placebo + standard of care Time (days) Time (months) TECOS ELIXA Patients with endpoint (%) T2D; HbA 1c %; 50 years; CVD history (n=14,671) Sitagliptin (100 or 50 mg/day***) + standard of care Placebo + standard of care T2D; HbA 1c %; ACS within 180 days (n=6068) Lixisenatide (10 or 20 µg/day ) + standard of care Placebo + standard of care ACS, acute coronary syndrome; CI, confidence interval; CV, cardiovascular; EXAMINE, Examination of Cardiovascular Outcomes: Alogliptin vs. Standard of Care in Patients with Type 2 Diabetes Mellitus and Acute Coronary Syndrome; HR, hazard ratio; MI, myocardial infarction; SAVOR TIMI-53, Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Time Diabetes in the Mellitus Thrombolysis trial (months) in Myocardial Infarction 53; T2D, type 2 diabetes; TECOS, Trial Evaluating Cardiovascular Outcomes with Sitagliptin; UA, unstable angina White et al. N Engl J Med 2013;369: ; Sciria et al. N Engl J Med 2013;369: ; Green et al. N Engl J Med 2015;16;373:232 42; Time (months) Pfeffer et al. N Engl J Med 2015;373: Patients with endpoint (%)
34 Selected CVOTs: Assessing CV benefit with antiglycemic agents EMPA-REG 1 LEADER 4 SUSTAIN-6 5 Population T2D + high CV risk T2D + high CV risk T2D Drug (Class) Empagliflozin (SGLT-2i) Liraglutide (GLP-1RA) Semaglutide (GLP-1RA) Objective Non-inferiority Non-inferiority Non-inferiority Endpoint 3-point MACE 3-point MACE 3-point MACE Results HR 0.86 HR 0.87 HR point MACE: first occurrence of CV death, nonfatal MI or nonfatal stroke; MACE+: CV death, nonfatal MI, nonfatal stroke and hospitalisation for UA procedure ACS, acute coronary syndrome; CV, cardiovascular; CVOT, cardiovascular outcomes trial; GLP-1RA, glucagon-like peptide-1 receptor agonist; HR, hazard ratio; LEADER, Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results; MACE, major adverse cardiovascular event; MI, myocardial infarction; SGLT-2i, sodium-glucose cotransporter-2 inhibitor; T2D, type 2 diabetes; UA, unstable angina 1. Zinman et al. N Engl J Med 2015;373: ; 2. Green et al. N Engl J Med 2015;373:232 42; 3. Pfeffer et al. N Engl J Med 2015;373: ; 4. Marso et al. N Engl J Med 2016;375:311 22; 5. Marso et al. N Engl J Med 2016;375:

35 CARDIOVASCULAR OUTCOME DATA FOR SGLT2 INHIBITORS Image: 48

")




36 SGLT-2 Inhibitors: Mechanism of Action (cont) Free Filtration of Solute Active Reabsorption Glucose SGLT-2 SGLT-1 Glucose Juxtoglomerular Complex Proximal Convoluted Tubules Type 2 Diabetes Loop of Henle
37 SGLT2 Inhibition Lowers T max, Allowing Elimination of Excess Glucose Overexpression of SGLT2 shifts T max to the right, allowing excess glucose to be reabsorbed SGLT2 inhibition shifts T max to the left, eliminating excess glucose Urinary Glucose Excretion (g/day) Blockade of SGLT2 Normal T2DM SGLT2 inhibition T2DM 240 mg/dl T max Plasma Glucose (mg/dl) Chao E, et al. Nature Rev Drug Discov. 2010;9: ; Bays H. Curr Med Res Opin. 2009;25: ; DeFronzo RA, et al. Diabetes Obes Metab. 2012;14:5-14; Gerich JE. Diabet Med. 2010;27: ; Kim Y, et al. Diabetes Metab Syndr Obes. 2012;5:
38 EMPA-REG 14% reduction of primary composite outcome: death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke 38% relative risk reduction of death from cardiovascular causes 32% relative risk reduction of death from any cause 35% relative risk reduction of hospitalization for heart failure NEJM, Nov ;373:
39 Primary Outcome Results EMPA-REG OUTCOME (EMPAGLIFLOZIN) 8 1.6% ARR 14% RRR 52
40 Primary Outcome Results EMPA-REG OUTCOME (EMPAGLIFLOZIN) 8 Outcome Pooled Empagliflozin (n = 4687) Placebo (n = 2333) Hazard Ratio (95% CI) Primary Composite Outcome, n (%) Death from Cardiovascular Causes, n (%) 490 (10.5) 282 (12.1) Assessment of Individual Primary Outcome Events 172 (3.7) 137 (5.9) 0.86 (0.74 to 0.99) 0.62 (0.49 to 0.77) Nonfatal Myocardial Infarction, n (%) 213 (4.5) 121 (5.2) 0.87 (0.70 to 1.09) Nonfatal Stroke, n (%) 150 (3.2) 60 (2.6) 1.24 (0.92 to 1.67) Abbreviation: CI confidence interval 53

41 June 14, % reduction of incident or worsening nephropathy 44% relative risk reduction of doubling of serum creatinine 55% relative risk reduction of renal-replacement therapy 54
 Placebo Empagliflozin 0 0 6 12 18 24 30 36 42 48 9 6 3 Cumulative Incidence of Death From CV Causes P<0.001 Hazard ratio, 0.")
42 EMPA-REG Trial-Demonstrates Rapid Improvement in 3-Point MACE Empa 10, 25 mg or standard of care Patients With Event, % Patients With Event, % Cumulative Incidence of the Primary Outcome a P=0.04 for superiority Hazard ratio, 0.86 (95.02% CI, ) Placebo Empagliflozin Cumulative Incidence of Death From CV Causes P<0.001 Hazard ratio, 0.62 (95% CI, ) Death from a CV event, non-fatal MI, or stroke 14% risk reduction 38% risk reduction Placebo Empagliflozin Patients With Event, % P=0.002 Hazard ratio, 0.65 (95% CI, ) Hospitalization for Heart Failure 35% risk reduction Placebo a Cumulative incidence of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke. N=7020 patients with T2DM at high risk of cardiovascular events. Empagliflozin Month 55
43 Empa-Reg Renal Data Incidence of nephropathy by 39 % Warner C, et al. NEJM. DOI: /NEJMoa




44 CANVAS and CANVAS-R Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes Image: 57
45 Study Design CANVAS AND CANVAS-R (CANAGLIFLOZIN) 9 MULTICENTER, INTERNATIONAL, DOUBLE-BLIND, NON-INFERIORITY TO SUPERIORITY, PLACEBO-CONTROLLED, RANDOMIZED TRIAL Key Inclusion Criteria T2DM 7% HbA 1c 10.5% Antidiabetic medication naïve OR treated with 1 approved agent 30-years-old with symptomatic ASCVD OR 50-years-old with 2 CV risk factors egfr 30 ml/min/1.73 m 2 80% adherence during the 2-week placebo run-in period Key Exclusion Criteria T1DM Antidiabetic regimen not stable for at least 8 weeks 1 severe hypoglycemic episode 6 months prior to screening Acute ASCVD event occurring 3 months before screening egfr < 30 ml/min/1.73 m 2 58
46 Baseline Characteristics CANVAS AND CANVAS-R (CANAGLIFLOZIN) 9 Baseline Characteristics Canagliflozin (n = 5795) Placebo (n = 4347) Male, n (%) 3759 (64.9) 2750 (63.3) Age, years 63.2 ± ± 8.2 Diabetes Duration, years 13.5 ± ± 7.8 HbA 1c (%) 8.2 ± ± 0.9 Body Mass Index (kg/m 2 ) 31.9 ± ± 6.0 Established Cardiovascular Disease, n (%) 3756 (64.8) 2900 (66.7) egfr, MDRD (ml/min/1.73 m 2 ) 76.7 ± ± 20.8 Median Urine Albumin-to-Creatinine Ratio (mg/g), [interquartile range] 12.4 [6.71 to 40.9] 12.1 [6.57 to 43.9] Neuropathy, n (%) 1787 (30.8) 1323 (30.4) Current Smoker, n (%) 1020 (17.6) 786 (18.1) Low-Density Lipoprotein Cholesterol (mg/dl) 88.9 ± ± 34.8 Abbreviations: ± standard deviation; egfr estimated glomerular filtration rate; MDRD Modification of Diet in Renal Disease 59
47 Baseline Medications CANVAS AND CANVAS-R (CANAGLIFLOZIN) 9 Baseline Class/Medication Use Canagliflozin (n = 5795) Placebo (n = 4347) Antihypertensives, n (%) Not Available Not Available Renin-Angiotensin-Aldosterone System Inhibitors, n (%) 4645 (80.2) 3471 (79.8) Beta Blockers, n (%) 3039 (52.4) 2382 (54.8) Diuretics, n (%) 2536 (43.8) 1954 (45.0) Antilipemics, n (%) Not Available Not Available Statins, n (%) 4329 (74.7) 3270 (75.2) Ezetimibe, n (%) Not Available Not Available Antithrombotics, n (%) 4233 (73.0) 3233 (74.4) Aspirin, n (%) Not Available Not Available Antihyperglycemics, n (%) Not Available Not Available Insulin, n (%) 2890 (49.9) 2205 (50.7) Metformin, n (%) 4447 (76.7) 3378 (77.7) Sulfonylureas, n (%) 2528 (43.6) 1833 (42.2) 60
 9 4.")
48 Primary Outcome Results CANVAS AND CANVAS-R (CANAGLIFLOZIN) 9 4.6* ARR 14% RRR *Events per 1000 patient years 61
49 Primary Outcome Results CANVAS AND CANVAS-R (CANAGLIFLOZIN) 9 Outcome Canagliflozin (n = 5795) Placebo (n = 4347) Hazard Ratio Number of Participants with an (95% CI) Event per 1000 Patient Years Primary Composite Outcome Death from Cardiovascular Causes Assessment of Individual Primary Outcome Events Nonfatal Myocardial Infarction Nonfatal Stroke Abbreviation: CI confidence interval 0.86 (0.75 to 0.97) 0.87 (0.72 to 1.06) 0.85 (0.69 to 1.05) 0.90 (0.71 to 1.15) 62
50 Safety Data CANVAS AND CANVAS-R (CANAGLIFLOZIN) 9 Outcome Canagliflozin* Placebo* EFFECTS HIGHEST OF CANAGLIFLOZIN LEVEL ON ATRAUMATIC LOWER Number ATRAUMATIC of Participants with an LOWER-LIMB Event per 1000 Patient Years AMPUTATIONS LIMB AMPUTATION IN THE INCANVAS KEY SUBGROUPS PROGRAM P Value Any Serious Adverse Event Adverse Events Leading to Canagliflozin Placebo Outcome Hazard Ratio 0.07 Discontinuation (Per 1000 Patient Years) (Per 1000 Patient Years) (95% CI) Adverse Events History of Interest of Amputation from the CANVAS Program Amputation < Yes Diabetic Ketoacidosis (1.11 to ) Fracture, 1.88 No All (1.27 to 2.78) Fracture, Low-Trauma Genital Infections, Male History of Peripheral Vascular Disease < Yes Adverse Events of Interest from CANVAS (0.80 to 2.40) Hypoglycemia Mycotic No Genital Infections, Female (1.53 to < 3.58) Volume Abbreviation: Depletion CI confidence interval n* population size varies depending on the data set being analyzed 63
51 Cardiovascular Outcomes Data for Sodium-Glucose Cotransporter-2 Inhibitors Agent Empagliflozin (Jardiance) Canagliflozin (Invokana) Clinical Trial EMPA-REG 8 CANVAS/CANVAS-R 9 Study Design Intervention Patient Population Primary Composite Endpoint Primary Composite Endpoint Outcome, P vs. I DB, INT, MC, NI S, PC, R trial Empagliflozin 10 or 25 mg PO once daily 18-years-old; acute coronary event > 2 months before informed consent; T2DM (57% > 10 years duration); baseline HbA 1c : 8.1%; 99% with CV disease Death from CV causes, nonfatal MI (excluding silent MI), nonfatal stroke 12.1% vs. 10.5% [HR 0.86; 95% CI: ; p < for NI; p = 0.04 for S] DB, INT, MC, NI S, PC, R trial Canagliflozin 100 mg to 300 mg PO once daily 30-years-old with a coexisting CV condition or 50-years-old with 2 CV risk factors; T2DM (mean: 14 years); baseline HbA 1c : 8.2%; 65% with CV disease Death from CV causes, nonfatal MI (excluding silent MI), nonfatal stroke 31.5 vs. 26.9* [HR 0.86; 95% CI: ; p < for NI; p = 0.02 for S] ARR / RRR 1.6% / 13.2% 4.6* / 14.6% Number Needed to Treat 63 patients over 3.1 years * Number of participants with an event per 1000 patient years Abbreviations: ARR absolute risk reduction; CI confidence interval; CV cardiovascular; DB double-blind; HR hazard ratio; I intervention; INT international; MC multi-center; MI myocardial infarction; NI noninferiority; P placebo; PC placebo-controlled; PO by mouth; R randomized; RRR relative risk reduction; S superiority; T2DM type 2 diabetes mellitus 64




52 Proposed Cardioprotective Effects with SGLT2i 15 SODIUM-GLUCOSE COTRANSPORTER-2 INHIBITORS PANCREATIC ADIPOSE TISSUE ALPHA CELLS LIVER FFA Ketones Glucagon Aortic Stiffness and Wall Stress Weight loss Preload Afterload Improved glycemic control Extracellular Fluid Volume Uric acid excretion NaCl/H 2 O excretion Angiotensin 1-7 AT 2 Blood pressure Systemic vascular resistance 65
53 Clinical Considerations SODIUM-GLUCOSE COTRANSPORTER-2 INHIBITORS Advantages Disadvantages Appreciable reductions in HbA 1c Decrease in blood pressure and serum uric acid Placebo-like risk for hypoglycemia Positive cardiovascular outcomes data 8,9 Potential renal- 9,12 and heart failureprotective 13,14 effects Weight loss Amputations o Potentially unique to canagliflozin Cost Diabetic ketoacidoisis Genitourinary tract infections Increased LDL-C Polyuria Transient increase in serum creatinine Urinary tract infections leading to pyelonephritis and urosepsis Volume depletion/dizziness/hypotension Abbreviation: LDL-C low-density lipoprotein cholesterol 10. American Diabetes Association. Pharmacologic Approaches to Glycemic Treatment. Sec. 8. In Standards of Medical Care in Diabetes Diabetes Care 2017;40(Suppl. 1):S64 S Garber AJ, Abrahamson MJ, Barzilay JI, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm Executive Summary. Endocr Pract. 2017;23(2): Epub 2017/01/18. doi: /ep cs. PubMed PMID:

54 Clinical Considerations SODIUM-GLUCOSE COTRANSPORTER-2 INHIBITORS Patient education Polyuria Hydration Hygiene Signs and symptoms of DKA When to hold therapy 16 Patients at increased risk for amputations Glycosuria 2+ Image: Handelsman Y, Henry RR, Bloomgarden ZT, et al. American Association of Clinical Endocrinologists and American College Of Endocrinology Position Statement on the Association of SGLT-2 Inhibitors and Diabetic Ketoacidosis. Endocr Pract. 2016;22(6): Epub 2016/04/16. doi: /ep ps. PubMed PMID:

55 NEJM, Dec 3,
56 ELIXA 69
57 NEJM June 13, % reduction of primary composite outcome: death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke 22% relative risk reduction of death from cardiovascular causes 15% relative risk reduction of death from any cause No change in relative risk reduction of hospitalization for heart failure 70

58 Study Design THE LEADER TRIAL (LIRAGLUTIDE) 29 MULTICENTER, INTERNATIONAL, DOUBLE-BLIND, NON-INFERIORITY TO SUPERIORITY, PLACEBO-CONTROLLED, RANDOMIZED TRIAL Key Inclusion Criteria T2DM HbA 1c 7% Antidiabetic medication naïve OR treated with 1 oral antidiabetic medication and/or long-acting, NPH or premixed insulin 50-years-old with established CVD or chronic renal failure OR 60-years-old with 1 CV risk factor Key Exclusion Criteria T1DM Use of a GLP-1 RA, DPP-4 inhibitor, pramlintide or rapid-acting insulin Family or personal history of MEN2 or medullary thyroid cancer Acute coronary or cerebrovascular event occurring 14 days before randomization 72
59 Primary outcomes in LEADER and EMPA-REG Timing of separation of treatment arms suggest different cardioprotective MoAs 3 Point MACE improvement not driven by glycemic efficacy! LEADER 1 EMPA-REG 2 Proportion of individuals with a MACE event (%) HR: 0.87 (95% CI: 0.78;0.97) p=0.01 (superiority) Placebo Liraglutide HR: 0.86 (95% CI: 0.74;0.99) p=0.04 (superiority) Placebo Empaglifozin Time from randomisation (months) 3-point MACE: first occurrence of CV death, nonfatal MI or nonfatal stroke CI, confidence interval; HR, hazard ratio; LEADER, Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results; MACE, major adverse cardiovascular event; MoA, mode of action 1. Marso et al. N Engl J Med 2016;375:311 22; 2. Zinman et al. N Engl J Med 2015;373:
60 Primary Outcome Results THE LEADER TRIAL (LIRAGLUTIDE) Outcome Primary Composite Outcome, n (%) Liraglutide (n = 4668) Placebo (n = 4672) 608 (13.0) 694 (14.9) Hazard Ratio (95% CI) 0.87 (0.78 to 0.97) Assessment of Individual Primary Outcome Events Death from Cardiovascular Causes, n (%) Nonfatal Myocardial Infarction, n (%) 219 (4.7) 278 (6.0) 281 (6.0) 317 (6.8) Nonfatal Stroke, n (%) 159 (3.4) 177 (3.8) 0.78 (0.66 to 0.93) 0.88 (0.75 to 1.03) 0.89 (0.72 to 1.11) Abbreviation: CI confidence interval 29. Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2016;375(4): Epub 2016/06/14. doi: /NEJMoa PubMed PMID: ; PubMed Central PMCID: PMCPMC

 Increased insulin secretion, decreased glucagon secretion (pancreas) Fluid reduction Hemodynamic effects Heart metabolism Glomeruli Increased Proximal glucose Established")

61 GLP-1RA and SGLT-2i Proposed cardioprotective MoA Liraglutide Vasodilation Empagliflozin Proposed cardioprotective MoA 1,2 Plaque stability SGLT-2i Proposed cardioprotective MoA 3 Anti-atherosclerotic GLP-1R Reduced GLP-1RA platelet aggregation Anti-inflammatory effects Established effects Hyperglycaemia Weight Inflammation Visceral adiposity BP Endothelial function Blood flow Smooth muscle proliferation Platelet aggregation Increased glucose uptake and glucagon synthesis (adipose, muscle, liver) Decreased appetite and food intake (brain) Increased insulin secretion, decreased glucagon secretion (pancreas) Fluid reduction Hemodynamic effects Heart metabolism Glomeruli Increased Proximal glucose Established tubule effects filtration Hyperglycaemia Weight Visceral adiposity BP Distaltubule Increased urinary glucose excretion BP, blood pressure; GLP-1RA, glucagon-like peptide-1 receptor agonist; MoA, mode of action; SGLT-2i, sodium-glucose cotransporter-2 inhibitor 1. Marso N Engl J Med 2016;375:311 22; 2. Drucker. Cell Metab 2016;24:15 30; 3. Zinman et al. N Engl J Med 2015;373:

62 NEJM, Sep 16,
63 NEJM, Sep 16,
64 Pending Diabetes CV Outcome Studies Schnell et al. Cardiovasc Diabetol. 2016;15:
65 Diabetes CV Outcome Studies 81
66 PCSK9 (Proprotein convertase subtilisin/kexin type 9) A secreted protein which targets the LDL receptor for degradation Gain of function mutations cause high LDL-C Loss of function mutations cause low LDL-C Inhibition lowers LDL-C levels Up-regulated by statin therapy 82
67 How is cholesterol removed from blood? LIVER Circulating LDL particles (which contain a large ApoB protein) are grabbed by an LDL receptor 83
68 How is cholesterol removed from blood? LIVER The entire complex is then internalized into the hepatocyte for LDL destruction 84
69 How is cholesterol removed from blood? Then the LDL particle is destroyed LIVER Before the LDL particle is destroyed, the LDL receptor migrates back to the hepatocyte cell surface so that it can grab more LDL molecules 85
70 How is cholesterol removed from blood? When PCSK9 is present, however, the LDL-C receptor gets stuck and cannot migrate back to the surface LIVER It therefore gets destroyed along with the LDL And the number of LDL-C receptors on the cell surface is depleted 86

71 The theory behind PCSK9 inhibitors LIVER X If PCSK9 is inhibited, the LDL-C receptor can migrate back to the cell surface And surface LDL receptors will be restored which will reduce the serum LDL-C level 87
72 90
73 DOI: /NEJMoa
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus
 Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
The Role Of SGLT-2 Inhibitors In Clinical Practice. Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs
 The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?!
 2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Dapagliflozin and cardiovascular outcomes in type 2
 EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
Terapia con agonisti GLP1 e outcome cardiovascolare. Edoardo Mannucci
 Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Effect of SGLT-2 Inhibitors on the Heart. Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic
 Effect of SGLT-2 Inhibitors on the Heart Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic Disclosures Speaker - Johnson and Johnson - Merck Research - Merck - Novo
Effect of SGLT-2 Inhibitors on the Heart Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic Disclosures Speaker - Johnson and Johnson - Merck Research - Merck - Novo
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Invokana (canagliflozin) NEW INDICATION REVIEW
 NEW INDICATION REVIEW") Invokana (canagliflozin) NEW INDICATION REVIEW Introduction Brand name: Invokana Generic name: Canagliflozin Pharmacological class: Sodium-glucose cotransporter 2 (SGLT2) inhibitor Strength and Formulation:
Invokana (canagliflozin) NEW INDICATION REVIEW Introduction Brand name: Invokana Generic name: Canagliflozin Pharmacological class: Sodium-glucose cotransporter 2 (SGLT2) inhibitor Strength and Formulation:
Endocrinologist Sweetgrass Endocrinology
 Endocrinologist Sweetgrass Endocrinology Sanders, Cummings Ask Justice Department to Investigate Insulin Prices The Department of Justice and the FTC are asked to investigate whether Lilly, Novo Nordisk,
Endocrinologist Sweetgrass Endocrinology Sanders, Cummings Ask Justice Department to Investigate Insulin Prices The Department of Justice and the FTC are asked to investigate whether Lilly, Novo Nordisk,
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE
 CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Cardiovascular Consequences of Diabetes Mellitus
 Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI. Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona
 PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona Disclosure Dr Massimo Boemi has been granted as speaker
PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona Disclosure Dr Massimo Boemi has been granted as speaker
Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician
 Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
CV outcomes Studies and Implications for diabetes management. Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
 CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
SESSION 4 12:30pm 1:45pm
 SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
CV Risk Management in Diabetes Mellitus
 CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
Disclosures. Objectives. Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials 8/28/2017
 Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications
 American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Class Update: Sodium-glucose Cotransporter 2 (SGLT2) Inhibitors
 Inhibitors") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Class Update: Sodium glucose Cotransporter 2 (SGLT2) Inhibitors
 Inhibitors") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
La lezione dei trials di safety cardiovascolare. Edoardo Mannucci
 La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
New Strategies for Cardiovascular Risk reduction in Diabetes
 New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Integrating Data on Macrovascular and Microvascular Outcomes into Diabetes Management: Evolving Treatment Strategies
 Emerging Challenges in Primary Care Integrating Data on Macrovascular and Microvascular Outcomes into Diabetes Management: Evolving Treatment Strategies 1 Faculty Richard S. Beaser, MD Senior Staff Physician,
Emerging Challenges in Primary Care Integrating Data on Macrovascular and Microvascular Outcomes into Diabetes Management: Evolving Treatment Strategies 1 Faculty Richard S. Beaser, MD Senior Staff Physician,
1/11/18. Emerging Challenges in Primary Care
 1/11/18 Emerging Challenges in Primary Care Integrating Data on Macrovascular and Microvascular Outcomes into Diabetes Management: Evolving Treatment Strategies 1 Faculty Richard S. Beaser, MD Senior Staff
1/11/18 Emerging Challenges in Primary Care Integrating Data on Macrovascular and Microvascular Outcomes into Diabetes Management: Evolving Treatment Strategies 1 Faculty Richard S. Beaser, MD Senior Staff
Current Updates & Challenges In Managing Diabetes in CVD
 Current Updates & Challenges In Managing Diabetes in CVD Preventive Cardiovascular Conference 2016 Instituit Jantung Negara 12 th November 2016 Nor Azmi Kamaruddin Diabetes Clinic Department of Medicine
Current Updates & Challenges In Managing Diabetes in CVD Preventive Cardiovascular Conference 2016 Instituit Jantung Negara 12 th November 2016 Nor Azmi Kamaruddin Diabetes Clinic Department of Medicine
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Diabetes Update: Diabetes Management In Primary Care. Jonathon M. Firnhaber, MD, FAAFP
 Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare
 Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
HEART FAILURE AND DIABETES MELLITUS: DANGEROUS LIASONS MICHEL KOMAJDA, MD
 HEART FAILURE AND DIABETES MELLITUS: DANGEROUS LIASONS MICHEL KOMAJDA, MD Author affiliations: Department of Cardiology, Hôpital Saint Joseph, Paris, France Address for correspondence: Michel Komajda,
HEART FAILURE AND DIABETES MELLITUS: DANGEROUS LIASONS MICHEL KOMAJDA, MD Author affiliations: Department of Cardiology, Hôpital Saint Joseph, Paris, France Address for correspondence: Michel Komajda,
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Review of FDA Guidance on Cardiovascular Outcomes for Diabetes Medication Trials and Application to Clinical Management
 Katherine S. O Neal Pharm.D., MBA, BCACP, CDE, BC-ADM, AE-C Associate Professor The University of Oklahoma Health Sciences Center College of Pharmacy Department of Internal Medicine Oklahoma City, OK Member,
Katherine S. O Neal Pharm.D., MBA, BCACP, CDE, BC-ADM, AE-C Associate Professor The University of Oklahoma Health Sciences Center College of Pharmacy Department of Internal Medicine Oklahoma City, OK Member,
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center