Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต
|
|
|
- Morgan Bradford
- 6 years ago
- Views:
Transcription


1 Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต

2 Content : Electrolyte Emergency!!
3 Serum sodium Normal serum sodium: meq/l Normal serum osmolality: mosm/l Normal urine sodium: meq/kg Normal urine osmolality: mosm/kg
4

5 Body Fluid Compartments: 2/3 ICF: 55%~75% X 50~70% lean body weight TBW Male (60%) > female (50%) Most concentrated in skeletal muscle TBW=0.6xBW ICF=0.4xBW ECF=0.2xBW 1/3 ECF 3/4 1/4 Extravascular Interstitial fluid Intravascular plasma
6 Hyponatremia Posm Nae + Ke TBW PNa < 135 mmol/l Posm Nae Translocational Hyponatremia PseudoHyponatremia True hyponatremia

7 Symptoms Serum Na + (meq/l) < 120 Symptoms Decreased taste Thirst Anorexia, N + V Muscle cramps Weakness Lethargy Restlessness Confusion Delirium Coma Seizures
8 Workup for Hyponatremia 3 mandatory lab tests Serum Osmolality Urine Osmolality Urine Sodium Concentration Additional labs depending on clinical suspicion TSH, cortisol (Hypothryoidism or Adrenal insufficiency) Albumin, BM, triglycerides and SPEP (psuedohyponatremia, cirrhosis, MM)
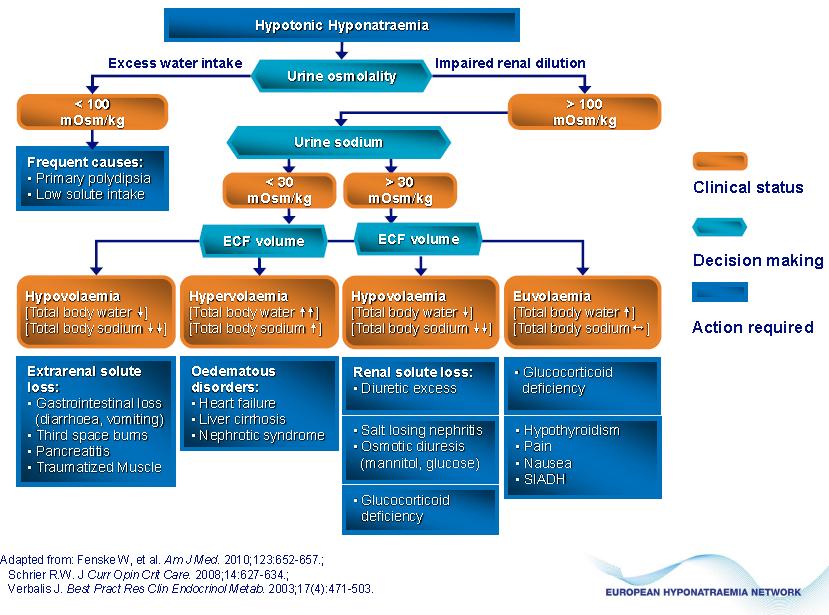
9 Approach Hyponatremia : P Na<135 High Posm (>295) P osm เพ อย นย นภาวะ true hyponatremia Normal Posm ( ) Translocation hypo-natremia glucose or manitol Hyponatremia + Hypo-osmolality Low(<285) True-hypoNatremia Uosm Pseudo-hypo-Natremia yes Inappropriate ADH Work >100 ADH Work Lipid or Protein เพ อย นย นว าม การหล งของ ADH (เม อ U osm.>100) Hypothyroidism Hypoadrenalism SIADH no primary polydipsia Appropriate ADH Work Volume depletion
10
11 Management Depend on: Acute or chronic Asymptomatic or symtomatic Rate of decrease in serum sodium Volume status
12
13 Severe hyponatremia (<125 mmol/l) Acute Acute Duration<48hr. symptomatic Chronic Chronic Duration>48hr. Asymptomatic Chronic rarely<48hr. Emegency correction Needed Emegency hypertonic correction saline Needed hypertonic 1-2 Saline ml/kg/h, 1-2 ml/kg/h, coadministration coadministration of of furosemide furosemide Some immediate Correction needed Hypertonic saline1-2 ml/kg/h Furosemide Water restriction F/U serum, urine electrolyte Not exceed 1.5 mmol/l/h or 20 mmol/d No No immediate correction needed Long term management
14 Severe hyponatremia (<125 mmol/l) symptomatic Asymptomatic Acute Acute Duration<48hr. Chronic Chronic Duration>48hr. Some Some immediate Correction needed Chronic Chronic rarely<48hr. No No immediate correction needed Emegency correction Long term management Treatment irreversible causes Water restriction Democloclocycline mg bid Urea 15-60g/d VV2 2 receptor antagonists
 NaCl Restric")

15 Treatment 1.Corrected P Na level 2.Corrected Etiology(underlying) NaCl Restric water Volume depletion Diuretic Adrenal insufficiency Hypothyroid SIADH Edema Renal failure Primary polydipsia
16 Case consult A 75 year-old woman Watery diarrhea 10/day for 2 days orthostatic presyncope for 1 days drinking 1 litres of water/day Underlying HT on HCTZ (50 mg) 1X1 lab Na 125 meq/l K 3.3 meq/l Cl 110 meq/l HCO 3 18 meq/l # Hyponatremia
17 Hypo-osmolar hyponatremia Hypovolemic Non-hypovolemic GI Losses Renal Losses Skin Losses Vommitting diarrhea bleeding obstruction Diuretics hypoaldo saltwasting neph Burns GPP/eryth roderma SIADH Edematous States CNS Disease Pulmonary Drugs CHF NS Cirrhosis Slide courtesy of Adam Oster
18 Hypovolemic Hyponatremia Loss Na > Loss H 2 O Low ECF ---- ADH released increases tubular reabsorption of H 2 O low urine volume Renin released (low renal perfusion) kidneys retain sodium urine sodium low (<20 mmol/l)
19 What caused our patient s hyponatremia? GI losses HCTZ (impairs excretion of free water) as ECF decreases kidney exchanges K for Na to maintain volume - thus low K (Aldosterone)
20 How will you treat our patient off HCTZ Treat diarrhea oral rehydration salts IV NSS + KCl until no further postural drop oral potasium supplement Follow up electrolytes
21 SIADH Euvolemic Hyponatremia DDx hypothyroidism adrenal insufficiency psychogenic polydipsia
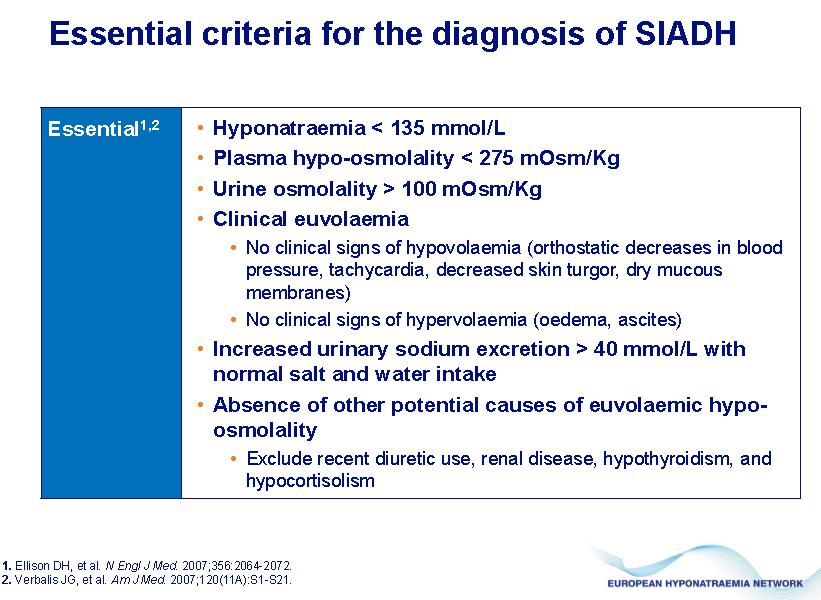
22 SIADH Diagnosis clinically euvolemic normal renal function normal thyroid (TSH) normal adrenal (cortisol stim test) no medications known to cause SIADH-like syndrome


23 SIADH causes Source: Yeates K, et al. CMAJ 2004;170(3):365-9
24
25 SIADH - Treatment acute hypertonic saline goal to increase Na by ~5 over 12 hours or until asymptomatic fluid restriction ml/d goal to increase Na by ~5 over 12 hours chronic fluid restriction Li (inhibits renal effects of ADH) demeclocycline 600 mg po od
26 Management Symptomatic hyponatremia Cause: SIADH W/U: serum osm, urine osm, Na deficit: calculate Form IV: 3%NaCl Rate: 1 meq/l
27 Calculation [Na] deficit = 10x0.6X50 = 300 meq/l Form IV: 3%NaCl (513 mosm/l) Volume: (300X1000)/513 = ml(600 ml) Rate: 1 meq/l/hr(60ml/hr)x 5hr then 0.5 meq/l/hr(30 ml/hr) correct Na not excess 12 meq/l/day
28 Case consult A 58 year-old man BW 50 kg. Underlying: Non small cell lung cancer confusion & lethargy for 2 days P/E Euvolemia Nausea/vomiting no ascites / no edema no sign of hypothyroidism or hypoadrenalism Lab: Na 108 meq/l, K 3.9 meq/l,cl 88 meq/l,co 3 88 meq/l Cr 1.4 mg/dl, serum osm 220 mosm/l urine Na 44 meq/kg, urine osm 660 mosm/kg
29 Consult # Euvolemic hyponatremia----- SIADH
30
31 Hypervolemic hyponatremia Increased ECF CHF cirrhosis / ascites nephrotic syndrome low effective circulating volume body retains Na and H 2 0 low urine Na (<20) Treatment Na and free water restriction
32 Pathophysiology CPM central pontine myelinolysis Acute non-inflammatory demyelination in basis pontis and other CNS sites (in ~10%) Mechanism unknown; felt to occur due to rapid changes in cell volume Actual incidence is unknown Risk factors Na + <120 meq/l for > 48 hrs Aggressive IV resuscitation w/ hypertonic saline Most cases occurred with rates of correction > 12 mmol/l /24 hrs Hypernatremia during treatment
33 CPM central pontine myelinolysis Clinical Features Usually neurologic deterioration hrs after rapid Na + correction Confusion, horizontal gaze paralysis, spastic quadriplegia, pseudobulbar palsy, encephalopathy coma, locked-in syndrome Dx MRI Tx supportive
34 Treatment summary Hypovolemic hyponatremia Correct with NS (0.9%) which is mildly hypertonic compared to pts serum Euvolemic hyponatremia: Restrict free water intake Identify underlying cause SIADH: Giving normal saline will worsen condition due to free water retention Can Tx with lithium and demeclocycline inhibit action of ADH Hypervolemic hyponatremia: Restrict free water intake +/- diuretics may worsen due to further Na+ loss dialysis if large amount of fluid needs to be taken off Slide courtesy of M Haager
35 Dry Source of Sodium loss? Hyponatremia Normovolemic (excess total body water but no edema) Fluid overloaded (excess water > excess Na + ) Renal: -Diuretics -Adrenal insufficiency -Salt-wasting nephritis -Bicarbonate loss -RTA -metabolic alkalosis -ketonuria -Osmotic diuresis -glucose -mannitol Extra-renal losses -GI losses -Third spacing Urine Na + <10 mmol/l SIADH Drugs Glucocorticoid deficiency Hypothyroidism Pain / emotion Urine Na + >20 mmol/l Nephrotic Syndrome Cirrhosis CHF Urine Na + <10 mmol/l Acute / Chronic Renal Failure Urine Na + >20 mmol/l Urine Na + >20 mmol/l Normal Saline Water restriction
36 Hypernatremia Symptoms anorexia N/V fatigue irritable Signs lethargy stupor coma muscle twitching hyperreflexia spasticity tremor ataxia focal neurological signs
37 Causes of Hypernatremia Reduced H 2 O intake disorders of thirst can t get H20 Increased H 2 O loss GI V&D NG 3rd spacing renal DI osmotic diuresis post-obstructive diuresis dermal burns perspiration Gain in Na exogenous Na intake NaCl NaHCO 3 hypertonic NS salt water drowning increased Na reabsorption hyperaldosteronism cushing s disease exogenous corticosteroids congenital adrenal hyperplasia
38 Management of hypernatremia Hypovolemic goal: restore volume deficits 0.9% NS Euvolemic DI oral fluids hypotonic saline (0.45%) vasopressin Hypervolemic increase renal sodium excretion > H20 diuretics +/- hypotonic saline may need dialysis
39 Case 93 year old man from nursing home, BW 40 kg Dementia, bed ridden not eating well Drowsiness P/E JVP flat, dry mouth Na = 160 meq/l BUN 40 mg/dl, Cr 0.8 mg/dl Urine sp.gr
40 # Hypernatremia Dehydration Water deficit: TBWX(Na-normal Na)/normal Na 0.6X40X( )/140 = 3.4 L Rate increase Na not excess 12 meq/l Duration: 48 hr
41 Potassium a precisely controlled cation Mostly intracellular Precise transcellular gradients required for neuronal transmission and cardiac conduction Also important in acid-base balance and buffering. K+/H+ pump Extracellular K controlled by serum ph change in ph of mEq change in K+ aldosterone insulin catecholamines
42 Hyperkalemia - etiology pseudohyperkalemia hemolysis increased intake impaired renal excretion renal failure hypoaldosteronism K-sparing diuretics Transcellular shifts acidosis insulin deficient drugs B-Blockers sux digitalis cellular injury rhabdomyolysis tumour lysis syndrome crush/burn
43 Hyperkalemia Mechanisms INCREASED INTAKE IMPAIRED EXCRETION TRANSCELLULAR SHIFT CELLULAR INJURY RENAL FAILURE NON RENAL FAILURE Slide courtesy of A. Oster
44 Hyperkalemia - etiology pseudohyperkalemia hemolysis increased intake impaired renal excretion renal failure hypoaldosteronism K-sparing diuretics Transcellular shifts acidosis insulin deficient drugs B-Blockers digitalis cellular injury rhabdomyolysis tumour lysis syndrome crush/burn
45 Hyperkalemia Clinical Features Cardiac 2/3 degree heart block wide complex tachycardias VF asystole ECG progression peaked T waves loss of P waves prolonged PR interval widening of QRS sine wave pattern ventricular fibrillation asystole
46 Non-specific muscle cramps weakness paralysis paresthesias tetany Hyperkalemia Neurological SSx focal neurological deficits
47 Management Principles Cardiac monitoring stabilize myocardium shift K into cells decrease GI absorption treat underlying cause
48 Immediate Management Calcium mechanism antagonises K and stabilizes myocardium indications dysrhythmia hypotension ECG changes onset 0-5 minutes duration minutes dose 5-30ml 10% calcium gluconate IV
49 Immediate Management Ventolin Mechanism shifts K into cells onset 15 minutes duration 2-4 hours dose 5-10mg neb repeat prn
50 Immediate Management Glucose and Insulin mechanism shifts K into cells onset 15 minutes duration 4-6 hours dose units of R 1 amp D50W (no D50W if hyperglycemic)
51 Immediate Management bicarbonate mechanism shifts K into cells only works if acidotic dose 1 amp (44 meq) IV push over 5 minutes onset 15 minutes duration 2 hours beware if hypertonic hypernatremic alkalotic
52 Delayed Therapy Exchange Resins kayelalate (polystyrene sulfonate) mechanism ion exchange resin removes K from body onset 1 hour duration dose 1-3 hours 1g binds 1mEq of K oral or rectal 20g in 70% sorbitol po (Rosen) 30g pr retained for 30 minutes
53 Mechanism removes K from blood Delayed Therapy hemodialysis can remove meq Indications renal failure unstable patient unresponsive to other treatment
54 Hypokalemia Spectrum of Symptoms Asymptomatic K Neuromuscular K usually < 2.5 lethargy confusion fasciculations weakness decreased DTRs paralysis (K<2) Cardiovascular usually no symptoms in patients without heart disease palpitations ectopy dysrhythmias 1-2 degree HB atrial fibrillation ventricular fibrillation
55 GI Hypokalemia Spectrum of Symptoms impairs intestinal smooth muscle N/V paralytic ileus Renal polyuria polydipsia
56 Hypokalemia Decreased Intake decreased dietary intake decreased absorption Transcellular Shifts alkalosis insulin B2 agonists eg: ventolin - lowers K ~ 0.4 mmol/l x 4 hours coffee Increased Loss renal hyperaldosteronism renal tubular defects mineralocorticoids glucocorticoids (alter GFR) +++diuretics drugs GI N/V/D Skin burns perspiration
57 Hypokalemia ECG findings small or absent T waves prominent U waves ST segment depression Slide courtesy A. Oster
58 Management Oral KCl elixir(20meq/15ml) K-Phos(4.4mEq/ml) useful if hypophosphatemic K-Citrate (0.9mEq/ml) useful in RTA IV KCl (10/20/40mEq/100cc) 10-20mEq/h >20mEq/h requires central line and cardiac monitor S/E s transient hyperkalemia burning at IV site
59 End
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
K+ Ann Crawford, RN, PhD, CNS, CEN
 Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Objectives. Objectives
 Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Hyponatraemia- Principles, Investigation and Management. Sirazum Choudhury Biochemistry
 Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
VanderbiltEM.com. ACEP 2013 Electrolyte Emergencies. Mastering Emergency Medicine. Electrolyte Emergency Questions. Electrolyte Emergency Questions
 ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09. Terminal Learning Objective. References. Hours: 2.0 Last updated: November 2015
 SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital
 Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Chapter 2. Fluid, Electrolyte, and Acid-Base Imbalances
 Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Electrolyte abnormalities are commonly associated with
 Electrolyte abnormalities are commonly associated with cardiovascular emergencies. These abnormalities may cause or contribute to cardiac arrest and may hinder resuscitative efforts. In some cases therapy
Electrolyte abnormalities are commonly associated with cardiovascular emergencies. These abnormalities may cause or contribute to cardiac arrest and may hinder resuscitative efforts. In some cases therapy
Nephrology / Urology. Hyperkalemia Causes and Definition Lecturio Online Medical Library. Definition. Epidemiology of Hyperkalemia.
 Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Normal serum osmolarity 275 to 295 mosm/l. Osmolarity: conc. of solution expressed as total # of solute particles per liter
 Fluid Homeostasis IV Crystalloid Solutions Normal serum osmolarity 275 to 295 mosm/l 2000-3000 ml H2O/day maintain fluid balance Insensible loses (850-1150mL) -Respiratory tract 500-700mL -Skin 250-350mL
Fluid Homeostasis IV Crystalloid Solutions Normal serum osmolarity 275 to 295 mosm/l 2000-3000 ml H2O/day maintain fluid balance Insensible loses (850-1150mL) -Respiratory tract 500-700mL -Skin 250-350mL
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Lethal Electrolyte Disorders. Yrd.Doç.Dr.Süha Türkmen Karadeniz Technical University Department of Emergency Medicine
 Lethal Electrolyte Disorders Yrd.Doç.Dr.Süha Türkmen Karadeniz Technical University Department of Emergency Medicine Compartments Değişken Total body fluid Total Body weight Total Body weight ECF
Lethal Electrolyte Disorders Yrd.Doç.Dr.Süha Türkmen Karadeniz Technical University Department of Emergency Medicine Compartments Değişken Total body fluid Total Body weight Total Body weight ECF
A Mnemonic for the Treatment of Hyperkalemia. Nick Wolters, PGY1 Resident Grandview Medical Center
 A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hypoglycemia, Electrolyte disturbances and acid-base imbalances
 Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC.
 Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC. Objectives 1. Review approach to hyponatremia Physiology & pathophysiology review Case-based common clinical questions Three-step process to
Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC. Objectives 1. Review approach to hyponatremia Physiology & pathophysiology review Case-based common clinical questions Three-step process to
Overview. Fluid & Electrolyte Disorders. Water distribution. Introduction 5/10/2014
 Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Hyponatremia and Hypomagnesemia
 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Critical issues in electrolyte and acid-base disturbance. Atiporn Ingsathit MD. PhD.
 Critical issues in electrolyte and acid-base disturbance Atiporn Ingsathit MD. PhD. Topics Hyponatremia Hypernatemia Hypokalemia Hyperkalemia Metabolic acidosis Hyponatremic patient Find truly hypo-osmotic
Critical issues in electrolyte and acid-base disturbance Atiporn Ingsathit MD. PhD. Topics Hyponatremia Hypernatemia Hypokalemia Hyperkalemia Metabolic acidosis Hyponatremic patient Find truly hypo-osmotic
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
A case of DYSELECTROLYTEMIA. Dr. Prathyusha Dr. Lalitha janakiraman s unit
 A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Electrolyte Abnormalities in the Transplant Recipient
 Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Hyperkalemia Protect, Shift, and Eliminate
 Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Metabolic Abnormalities in Critically Ill Patients
 CHAPTER 66 Metabolic Abnormalities in Critically Ill Patients A. M. Bhagwati Introduction Critically ill patients have a unique set of problems, ranging from metabolic, endocrine, nutritional, respiratory
CHAPTER 66 Metabolic Abnormalities in Critically Ill Patients A. M. Bhagwati Introduction Critically ill patients have a unique set of problems, ranging from metabolic, endocrine, nutritional, respiratory
Workshop on Hyponatremia
 Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Dr. Carlos Fernando Estrada Garzona. Departamento de Farmacología Universidad de Costa Rica
 Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
BIOL 221 Chapter 26 Fluids & Electrolytes. 35 slides
 BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender
 BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA
 Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA Why Electrolytes are Important? IMMEDIATE LIFE THREAT. You can Save or KILL the patient fixing it. USEFUL CLUE to the UNDERLYING
Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA Why Electrolytes are Important? IMMEDIATE LIFE THREAT. You can Save or KILL the patient fixing it. USEFUL CLUE to the UNDERLYING
Hyponatraemia. Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals
 Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Fluids, Electrolytes, and Nutrition
 Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
BIOL 2402 Fluid/Electrolyte Regulation
 Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital
 JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
hyponatremia/hypo-osmolality/hypotonic dehydration
 E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
Fluid, Electrolyte, and Acid Base Balance
 25 Fluid, Electrolyte, and Acid Base Balance Lecture Presentation by Lori Garrett Note to the Instructor: For the third edition of Visual Anatomy & Physiology, we have updated our PowerPoints to fully
25 Fluid, Electrolyte, and Acid Base Balance Lecture Presentation by Lori Garrett Note to the Instructor: For the third edition of Visual Anatomy & Physiology, we have updated our PowerPoints to fully
Fluids, Electrolytes, Management. Introduction 10/29/2012
 Fluids, Electrolytes, Management Franchot van Slot MD/PhD Hospitalist, Multicare Health Systems Adjunct Professor, Pacific University Introduction Multiple physical principles Non-intuitive concepts Clear
Fluids, Electrolytes, Management Franchot van Slot MD/PhD Hospitalist, Multicare Health Systems Adjunct Professor, Pacific University Introduction Multiple physical principles Non-intuitive concepts Clear
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
RENAL TUBULAR ACIDOSIS An Overview
 RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
3.Which is not a cause of hypokalemia? a) insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD
 insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD") Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Sym pt om s of "hyponat rem ia" Serum [Na + ] m Eq/ L: - Asymptomatic
![Sym pt om s of hyponat rem ia Serum [Na + ] m Eq/ L: - Asymptomatic](/thumbs/94/122329913.jpg "Sym pt om s of hyponat rem ia Serum [Na + ] m Eq/ L: - Asymptomatic") Sym pt om s of "" Serum [Na + ] >130 m Eq/ L: - Asymptomatic Serum [Na + ] 120-130 m Eq/ L: - Nausea, vomiting - Fatigue, muscle cramps - Abdominal symptoms - Mild cognitive - Gait disturbances Serum [Na
Sym pt om s of "" Serum [Na + ] >130 m Eq/ L: - Asymptomatic Serum [Na + ] 120-130 m Eq/ L: - Nausea, vomiting - Fatigue, muscle cramps - Abdominal symptoms - Mild cognitive - Gait disturbances Serum [Na
BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline
 BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline Fluid divisions 1. Extracellular fluid (ECF) 2. Intracellular fluid (ICF) Stabilization 1. Fluid balance 2. Electrolyte balance
BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline Fluid divisions 1. Extracellular fluid (ECF) 2. Intracellular fluid (ICF) Stabilization 1. Fluid balance 2. Electrolyte balance
Fluid & Electrolyte Therapy. Prof. Soliman Ali Hassan Prof. of Surgery Taibah university
 Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Volume and Electrolytes. Fluid and Electrolyte Management. Why 125ml? Question. Normal fluid requirement. Normal losses
 Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Hyponatremia: A Review
 Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Case Studies of Electrolyte Disorders ACOI Board Review Mark D. Baldwin D.O. FACOI
 Case Studies of Electrolyte Disorders ACOI Board Review 2018 Mark D. Baldwin D.O. FACOI Disclosures None, just working for The Man Question 1 The first thing in evaluating a patient who has a disorder
Case Studies of Electrolyte Disorders ACOI Board Review 2018 Mark D. Baldwin D.O. FACOI Disclosures None, just working for The Man Question 1 The first thing in evaluating a patient who has a disorder
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Assessment of the Patient with Endocrine Dysfunction. Objective. Endocrine. Endocrine Facts. Physical Assessment 10/3/2013
 Objective Endocrine Jennifer MacDermott, MS, RN, ACNS BC, NP C, CCRN Clinical Nurse Specialist Surgical Intensive Care Unit Identify abnormal assessment finding sin a patient with endocrine dysfunction.
Objective Endocrine Jennifer MacDermott, MS, RN, ACNS BC, NP C, CCRN Clinical Nurse Specialist Surgical Intensive Care Unit Identify abnormal assessment finding sin a patient with endocrine dysfunction.
NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
Hyponatremia FOSPED 2018
 Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013 Cells form 4 basic tissue groups: 1. Epithelial 2. Connective
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013 Cells form 4 basic tissue groups: 1. Epithelial 2. Connective
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
FLUIDS AND ELECTROLYTES
 FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
Metabolism of water and electrolytes. 2. Special pathophysiology disturbances of intravascular volume and
 Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University
 RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
Extracellular fluid (ECF) compartment volume control
 compartment volume control") Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Hyperglycaemic Emergencies GRI EDUCATION
 Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Symptoms of Tissue Disease
 Pathophysiology JP Advis DVM, Ph.D. Bartlett Hall, Animal Sciences, Cook, 932-9240, advis@aesop.rutgers.edu 02 Course website: rci.rutgers.edu/~advis Lectures, tests, grades, office hours, textbook, Material
Pathophysiology JP Advis DVM, Ph.D. Bartlett Hall, Animal Sciences, Cook, 932-9240, advis@aesop.rutgers.edu 02 Course website: rci.rutgers.edu/~advis Lectures, tests, grades, office hours, textbook, Material