Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC.
|
|
|
- Gary Allison
- 6 years ago
- Views:
Transcription
1 Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC.
2 Objectives 1. Review approach to hyponatremia Physiology & pathophysiology review Case-based common clinical questions Three-step process to working up hyponatremia SIADH review 2. Review approach to hypo/hyperkalemia Physiology & pathophysiology review Clinical manifestations & mechanisms Principles of treatment


3 Hyponatremia
4 Clinical Case An 84 year-old female from a nursing home is noted to have increasing confusion. She has had a poor appetite over the past year with significant weight loss. Over the past few days, the nurses have also noted some nausea, vomiting with no diarrhea, fever or other complaints. Med review notable for HCTZ and amitryptiline On exam, she has some dry oral mucosa but she is not orthostatic. There is no evidence of CHF, ascites or edema. She is awake, but disoriented. Neuro exam is nonfocal. Labs: Na 121 (130 2 months ago), normal renal/liver function. Serum osm 250, urine osm 280, urine Na 30
5 Questions we will answer 1. What are the potential causes of hyponatremia in this patient? 2. What other laboratory data is needed? 3. How might her diet be contributing to her hyponatremia? 4. How is the urine Na helpful? What in this case would limit its usefulness? 5. Does her urine osm of under 300 rule out SIADH? 6. How does water intake or inadequately hypertonic fluid intake worsen hyponatremia with SIADH?
6 Hyponatremia Defined Definition: serum Na+ <135 meq/l Generally associated with decreased osmolality <275 Most common electrolyte abnormality in North America A disorder of water retention Most forms of hyponatremia are associated with elevated ADH (whether appropriate or inappropriate), which concentrates urine and lowers free water excretion

7 Sodium Physiology Serum Sodium Regulation Stimulation of thirst Secretion of ADH Feedback mechanisms of the renin-angiotensinaldosterone system Renal handling of filtered sodium
8 Sodium Physiology Thirst Stimulation Osmolality Main driving force Only requires an increase of 2% - 3% Blood volume or pressure is reduced Requires a decrease of 10% - 15% Thirst center is located in the anterolateral center of the hypothalamus Respond to NaCL and angiotensin II
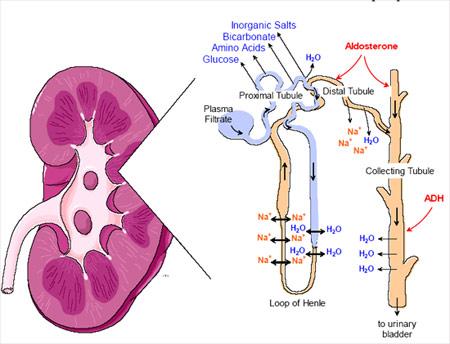
9 Renal Phsyiology
10 Hyponatremica: Clinical Manifestations Generally asymptomatic if Na+ level >125 Symptoms often non-specific: Headache, nausea, vomiting, muscle cramps Disorientation, depressed reflexes, lethargy, restlessness Delerium Seizure, coma, brainstem herniation & death More profound when change is large or rapid (hours) Serious complications more commonly seen in young women, pregnancy, after surgery and primary polydipsia
11 Approach to Hyponatremia Volume overloaded, dry or euvolemic? Osmolality (hyper, iso, or hypo) Is blood concentrated? For hypotonic hyponatremia, continue to 3 rd step: Urinary sodium excretion and FeNa % Is the urine concentrated?
12 Volume Status Volume status Hypotonic hyponatremia has 3 main groups: Hypovolemic both H2O and Na decreased (ΔH20 < ΔNa) Losses from diarrhea, vomiting, dehydration, malnutrition Euvolemic H20 increased and Na stable SIADH, thyroid disease, primary polydipsia Hypervolemic H20 increased and Na increased (Δ H2O > Δ Na) CHF, cirrhosis, renal failure
13 Osmolality Serum Osmolality =(2 Na + )+(glucose)+(urea) in mosm/kg Hypertonic - >295 Hyperglycemia, mannitol, glycerol Isotonic Historically pseudo-hyponatremia from elevated lipids or protein. Less common in contemporary laboratory equipment Hypotonic - <280 Xxcess fluid intake, low solute intake, renal disease, SIADH, hypothyroidism, adrenal insufficiency, CHF, cirrhosis, etc. Hypotonic hyponatremia warrants further workup
14 Urine Studies Urine Studies For euvolemic hyponatremia, check urine osmolality Urine osmolality <100 usually excess water intake Primary polydipsia, tap water enemas, post-turp Urine osmolality >100 - impaired renal concentration SIADH (often >300), hypothyroidism, cortisol deficiency Check urine sodium & calculate FeNa % (Una/Pna)/(Ucr/Pcr) A low urine sodium (<10) and low FeNa (<1%) implies the kidneys are appropriately reabsorbing sodium A high urine sodium (>20) and high FeNa (>1%) implies the kidneys are not reabsorbing sodium
15 Hyponatermia Isotonic ( ) mosm/kg of water Hypotonic (<280) mosm/kg of water Hypertonic (>295) mosm/kg of water Plasma Osmolality 2 [Na] + [glucose]/18 +[BUN]/2.8 + [Ethanol]/4.6

16 Hyponatermia Isotonic ( ) Lab artifact Absorption of Glycine or Sorbitol in bladder irrigation Hyperlipidemia Hyperproteinemia

17 Hyponatermia Hypertonic (>295) Excess of another Effective unmeasured Osmoles Radiographic contrast Hyperglycemia 100mg /dl gluà decrease Na Mannitol
18 Hyponatermia Hypotonic (<280) Hypervolemic Euvolemic Hypovolemic Volume Status orthostatics, JVP, Skin turgor, Mucous membrane, Peripheral edema
19 Hyponatermia Hypotonic (<280) Hypervolemic Urine Na <10 FENa<1% Urine Na >20 FENa>1% CHF Cirrhosis Nephrotic syndrome Renal Failure
20 Hyponatermia Hypotonic (<280) Hypovolemic Urine Na>20 FENa >1% Urine Na<10 FENa<1% (Renal loss) Diuretics Adrenal Insufficiency CSW (Extra-renal loss) GI loss Insensible loss Third spacing
21 Hyponatermia Hypotonic (<280) The most common Euvolemic Urine osm <100 Urine osm >100 Primary polydipsia Low Solute (beer potomania, very low protein + sodium diet) SIADH Adrenal insufficiency Hypothyroidism
22 Some special attention to the etiologies of the most common cause of hyponatremia which is?

23 Ellison et al, New Engl J Med 356: , 2007 SIADH
24 SIADH Diagnosis Essential Features Decreased effective osmolality ( <275 mosm/kg of water) Urinary Osmolality > 100 mosm/kg of water Clinical Euvolemia No sign of volume depletion of ECF No orthostasis, tachycardia, decreased skin turgor or dry mucous membrane No sign of excessive volume of ECF No edema or ascites Urinary Na > 40 mmol/l Normal thyroid and adrenal function No recent use of diuretic agents Ellison DH, Berl T, N Engl J Med.356(20): ,2007

25 Etiologies of SIADH Mitchell H. Rosner. Hyponatremia: An Update on the Management of SIADH. Renal CME.
26 SIADH Tips for primary care A careful review of medication record can often identify one or more potential contributors to SIADH Judicious changes to medications can correct underlying problem and/or provide very useful information prior to referral Consider imaging studies to rule out malignancy
27 Hyponatremia: Treatment Approach to treatment Outpatient Treating the underlying cause Fluid +/- sodium restriction Solute intake and urea administration Inpatient Isotonic fluid administration Hypertonic fluid administration Vasopressin receptor antagonist (V 2 R-A)
28 Clinical Case An 84 year-old female from a nursing home is noted to have increasing confusion. She has had a poor appetite over the past year with significant weight loss. Two weeks ago HCTZ was added. Over the past few days, the nurses have also noted some nausea, vomiting with no diarrhea, fever or other complaints. On exam, she has some dry oral mucosa but she is not orthostatic. There is no evidence of CHF, ascites or edema. She is awake, but lethargic. Neuro exam is nonfocal. Labs: Na 121 (130 2 months ago), normal renal/liver function. Serum osm 250, urine osm 280, urine Na 30. Volume: Euvolemic Osmolality: Serum is hypo-osmotic (250) Urine studies: Urine is inappropriately dilute (280), Urine sodium not low.
29 Case Questions 1. What are the potential causes of hyponatremia in this patient? Thiazide diuretic Recent n/v and volume loss (although not orthostatic) Poor solute intake/ tea and toast diet (may be why urine osm not as high as expected with classic SIADH) Possible CNS event (stroke, subdural) Underlying SIADH (suggested by inappropriately high urine osm, amitriptyline)
30 Case Questions 2. What other laboratory data would be needed? TSH AM cortisol level (although not orthostatic) Could consider neuroimaging given underlying dementia and risk for CVA, subdural, etc

31 Case Questions 3. How might her diet contribute? Each liter of urine requires 50 mosm of solute intake For the `tea and toaster` inadequate solute intake therefore impairs free water clearance Thomas Berl. Impact of Solute Intake on Urine Flow and Water Excretion. JASN (6):
32 Case Questions 4. How is the urine Na helpful in differentiating SIADH from hypovolemia? What in this case would limit its usefulness? Urine Na should be normal/elevated with SIADH and should be low with hypovolemia Thiazide diuretic use may elevate urine Na
33 Case Questions 5. Does her urine osm of under 300 rule out SIADH? No; classically urine osmolality is 300 or greater, but the urine osm of 220 in the setting of a serum na of 121 is inappropriately elevated Should be producing maximally dilute urine so anything over 100 is often inappropriate
34 Case Questions 6. How does water intake or hypotonic fluid intake worsen the hyponatremia with SIADH? Example: patient with SIADH with urine osm of liter of NS has 308 mosmol of NaCl, 1000 ml free water Isotonic Saline NaCl H2O In ml Out ml Net ml retained Due to renal handling, the saline bolus actually only provides MORE net free water
35 Case Questions 7. How would you manage this patient? Discontinue thiazide, amitriptyline Consider water restriction. Need to address both the amount of intake of both free water and solutes in setting of recent vomiting Avoid rapid correction Recheck lytes in in 5-7 days No immediate indication for intravenous resuscitation. If vomitting persisted, consider small amount of normal saline (would be relatively hypertonic to urine osm of 220)
 Assess serum osmolality 3) Check urine sodium,")
36 Take Home Points Work-up in 3 important steps 1) Assess volume status 2) Assess serum osmolality 3) Check urine sodium, osmolality
37 Take Home Points When to Refer Urine Na < that is persistent or a recent change Often there is the opportunity to try conservative measures before referral: Medication changes, volume correction or restriction What to include in Referral Include medication history and recent changes Labs: Historical sodium values, present serum osm, urine osm, urine Na, lytes, urea creatinine, TSH, random cortisol
38 References 1. Ellison DH, Berl T. The syndrome of inappropriate antidiuresis. N Engl J Med May 17;356(20): Decaux G. Is Asymptomatic Hyponatremia Really Asymptomatic? The American Journal of Medicine. 2006;119:S79-S Fenske W, Maier SK, Blechschmidt A, Allolio B, Störk S. Utility and limitations of the traditional diagnostic approach to hyponatremia: a diagnostic study. Am J Med. 2010;123: Gross P. Treatment of Hyponatremia. Inter Med.2008, 47: Ozturk S, Ozsenel E, Kazancioglu R, Turkmen A. A case of fluoxetine-induced syndrome of inappropriate antidiuretic hormone secretion. Nat Clin Pract Nephrol. 2008;4: Sica DA. Hyponatremia and heart failure--pathophysiology and implications. Congest Heart Fail. 2005;11: Sterns RH, Hix JK, Silver S. Treating profound hyponatremia: a strategy for controlled correction. Am J Kidney Dis. 2010;56: Updhyay A, Jaber BL, Madias NE. Incidence and prevalence of hyponatremia, Am J Med Jul;119(7 Suppl 1):S Verbalis JG, Goldsmith SR, Greenberg A, Schrier RW, Sterns RH. Hyponatremia treatment guidelines 2007: expert panel recommendations,am J Med Nov;120(11 Suppl 1):S1-21
")
39 Disorders of Potassium Homeostasis (optional)
40 Potassium Homeostasis Gastrointestinal absorption of potassium is complete resulting in daily excess intake of about 1 mmol/kg/d Excess potassium is excreted through the kidneys (90%) and through the gut (10%) The most important site of regulation is the distal nephron, under the influence of the renalangiotensin-aldosterone system
41 Potassium Homeostasis Maintain the osmotic integrity of cells Osmotic pressure in ICF Maintain acid-base balance Potassium-hydrogen exchange Contribute to the reactions that take place in cells Carbohydrate and amino-acid metabolism Involved in excitability of muscle cells
42 Potassium Homeostasis 98% of potassium is intracellular The remaining 2% is extracellular and tightly regulated between meq/l Hyperkalemia Hypokalemia Mild-to-Moderate meq/l meq/l Severe >6.5 meq/l and/or symptomatic < meq/l and/or symptomatic
43 Hypokalemia: Clinical Manifestations Neuromuscular impairment Muscle weakness, fatigue, cramps, paralysis Gastrointestinal motility Anorexia, nausea, vomitting, paralytic ileus Cardiovascular manifestations Arrhythmias, increased sensitivity to digitalis toxicity Impaired renal transportation function polyuria, impaired bicarb reabsorption, nephropathy Metabolic alkalosis
44 Hypokalemia: Clinical Manifestations ECG Changes ST segment depression T wave flattening Prominent U wave Prolongation of PR interval
45 Hypokalemia: Mechanisms 1. Decreased intake Anorexia 2. Excessive loss of K + GI: V/D/laxative Renal 3. K + shift into cells Alkalosis Insulin Catecholamines Hypothermia Hyperthyroid 4. Blood dilution
46 Hypokalemia: Renal Mechanisms Hyperaldosteronism Primary Secondary Polyuria Diuretics Loop, thiazide, acetozolamide Renal tubular acidosis type I & II Hypomagnesemia Salt-wasting nephropathies Barrter,Gitelman and Liddle s Syndrome Other Black licorice, CAH, Cushing s
47 Trans-tubular K gradient (TTKG) (Upot/Ppot)/(Uosm/Posm) Appropriate renal response Hyperkalemia TTKG >10 Hypokalemia TTKG < 2 Caveat for interpretation: Una must NOT be <10
48 Hypokalemia: Principles of Treatment 1. Etiological treatment to correct the underlying disorder including hypomagnesemia 2. Replacement of potassium Oral potassium chloride is preferred to intravenous With hypokalemia and oliguria, extracellular potassium may be driven by shift related to volume depletion and acidosis Generally only replace once confirmed patient is urinating 3. Potassium-sparing diuetics Reasonable to refer if considering these agents
49 Hyperkalemia: Clinical Manifestations Neuromuscular impairment Muscle weakness and paralysis Cardiovascular manifestations Conduction abnormalities: bundle branch & AV blocks Arrhythmias: bradycardia, asystole, vtach, vfib Impaired renal transportation function Impaired ammonium excretion Metabolic acidosis
 Widening QRS -> sine wave pattern and")
50 Hyperkalemia: Clinical Manifestations ECG Changes Peaked T wave Prolongation of the PR interval ST elevation (which may mimic myocardial infarction) Widening QRS -> sine wave pattern and asystole
51 Hyperkalemia: Mechanisms 1. Pseudohyperkalemia 2. Release from cells Crush injuries/rhabdo Tumor-lysis syndrome 3. K + shift out of cells Acidosis Insulin deficiency Beta-blockade Exercise Hyperthyroid 4. Reduced renal excretion
52 Hyperkalemia: Renal Mechanisms Acute and chronic renal disease Impaired sodium and water delivery Hypoaldosteronism Low renin: Diabetes, NSAIDs, drugs Angiotensin inhibitors: ACEi & ARBs Impaired aldosterone secretion: primary hypoaldosteronism, heparin Reduced response to aldosterone Potassium-sparing diuretics Certain antibiotics: trimethoprim, pentamidine
53 Hyperkalemia: Principles of Treatment Rapid-acting therapies (K>6.5 or with ECG changes): Calcium Calcium gluconate 1000mg over 2-3minutes Insulin with glucose 10 units regular insulin with 1 amp D50 Beta-2 adrenergic agonist Salbutamol 4 puffs q5min x3 or alburerol nebulized Sodium bicarbonate 150mEq in 1L D5W over 4-6 hours
54 Hyperkalemia: Principles of Treatment 1. Correct the underlying disorder 2. Potassium removal Loop or thiazide diuretics Cation-exchange resins (Kayexelate 30 grams) Dialysis 3. Prevention of future episodes Generally avoid co-administration of ACE-I with ARBs or direct-renin inhibitors (Aliskiren) with ACE-I/ARB Dietary restriction in CKD
55 References Evans KJ, Greenberg A. Hyperkalemia: a review. J Intensive Care Med Sep-Oct;20(5): Harel Z et al. The effect of combination treatment with aliskiren and blockers of the renin-angiotensin system on hyperkalaemia and acute kidney injury: Systematic review and meta-analysis. BMJ 2012 Jan 9; 344:e42. - Hollander JC, Calvert CJ. Hyperkalemia. Am Fam Physician 2006; 73: Kamel KS, Wei C. Controversial issues in the treatment of hyperkalaemia. Nephrol Dial Transplant. 2003;18: Sood MM, Sood AR, Richardson R. Emergency management and commonly encountered outpatient scenarios in patients with hyperkalemia. Mayo Clin Proc Dec; 82(12): The ONTARGET Investigators. Telmisartan, Ramipril, or Both in Patients at High Risk for Vascular Events. N Engl J Med 2008; 358:
56 Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC.
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
K+ Ann Crawford, RN, PhD, CNS, CEN
 Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Overview. Fluid & Electrolyte Disorders. Water distribution. Introduction 5/10/2014
 Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Cerebral Salt Wasting
 Cerebral Salt Wasting Heather A Martin MSN, RN, CNRN, SCRN Swedish Medical Center 1 Disclosures none 2 2 The problem Hyponatremia is the most common disorder of electrolytes encountered in medical practice
Cerebral Salt Wasting Heather A Martin MSN, RN, CNRN, SCRN Swedish Medical Center 1 Disclosures none 2 2 The problem Hyponatremia is the most common disorder of electrolytes encountered in medical practice
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Hyponatremia and Hypomagnesemia
 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Body water content. Fluid compartments. Regulation of water output. Water balance and ECF osmolallty. Regulation of water intake
 Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
Nephrology / Urology. Hyperkalemia Causes and Definition Lecturio Online Medical Library. Definition. Epidemiology of Hyperkalemia.
 Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต
 Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต Content : Electrolyte Emergency!! Serum sodium Normal serum sodium: 135-145 meq/l Normal serum osmolality: 285-295 mosm/l Normal urine sodium: 10-20
Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต Content : Electrolyte Emergency!! Serum sodium Normal serum sodium: 135-145 meq/l Normal serum osmolality: 285-295 mosm/l Normal urine sodium: 10-20
Hyponatraemia- Principles, Investigation and Management. Sirazum Choudhury Biochemistry
 Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
A case of DYSELECTROLYTEMIA. Dr. Prathyusha Dr. Lalitha janakiraman s unit
 A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
K+ Na+ Na+ Na+ 4/28/2018. What does Potassium do for you? Regulation of Muscle and Nerve Function. Regulation of Muscle and Nerve Function
 What does Potassium do for you? Aids in the conversion of glucose into glycogen Assists in carbohydrate and protein metabolism 2018 Spring Fling EMS Conference Maintains balance between cells and body
What does Potassium do for you? Aids in the conversion of glucose into glycogen Assists in carbohydrate and protein metabolism 2018 Spring Fling EMS Conference Maintains balance between cells and body
Objectives. Objectives
 Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Hyponatremia FOSPED 2018
 Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
BIOL 2402 Fluid/Electrolyte Regulation
 Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Hyponatraemia. Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals
 Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital
 JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
Extracellular fluid (ECF) compartment volume control
 compartment volume control") Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Hyperkalemia Protect, Shift, and Eliminate
 Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
BIOL 221 Chapter 26 Fluids & Electrolytes. 35 slides
 BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender
 BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are
 Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Faculty version with model answers
 Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Workshop on Hyponatremia
 Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline
 BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline Fluid divisions 1. Extracellular fluid (ECF) 2. Intracellular fluid (ICF) Stabilization 1. Fluid balance 2. Electrolyte balance
BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline Fluid divisions 1. Extracellular fluid (ECF) 2. Intracellular fluid (ICF) Stabilization 1. Fluid balance 2. Electrolyte balance
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Metabolic Abnormalities in Critically Ill Patients
 CHAPTER 66 Metabolic Abnormalities in Critically Ill Patients A. M. Bhagwati Introduction Critically ill patients have a unique set of problems, ranging from metabolic, endocrine, nutritional, respiratory
CHAPTER 66 Metabolic Abnormalities in Critically Ill Patients A. M. Bhagwati Introduction Critically ill patients have a unique set of problems, ranging from metabolic, endocrine, nutritional, respiratory
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
SAMSCA (tolvaptan) oral tablet
 oral tablet") SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Total Body Potassium
 Potassium Kate Driver BMLSc MAACB Immunochemistry Product Manager ANZ PI Diasorin Australia kate.driver@diasorin.com.au AACB QLD Branch Education Representative Australasian Association of Clinical Biochemists
Potassium Kate Driver BMLSc MAACB Immunochemistry Product Manager ANZ PI Diasorin Australia kate.driver@diasorin.com.au AACB QLD Branch Education Representative Australasian Association of Clinical Biochemists
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 2. Fluid, Electrolyte, and Acid-Base Imbalances
 Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Hyperkalemia. Katarzyna Bigaj PGY -1
 Hyperkalemia Katarzyna Bigaj PGY -1 Definition Hyperkalaemia is defined as a potassium level > 5.5 meq/l Moderate hyperkalaemia is a serum potassium > 6.0 meq/l Severe hyperkalaemia is a serum potassium
Hyperkalemia Katarzyna Bigaj PGY -1 Definition Hyperkalaemia is defined as a potassium level > 5.5 meq/l Moderate hyperkalaemia is a serum potassium > 6.0 meq/l Severe hyperkalaemia is a serum potassium
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital
 Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
NORMAL POTASSIUM DISTRIBUTION AND BALANCE
 NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
Diuretics having the quality of exciting excessive excretion of urine. OED. Inhibitors of Sodium Reabsorption Saluretics not Aquaretics
 Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
hyponatremia/hypo-osmolality/hypotonic dehydration
 E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
Assessment of the Patient with Endocrine Dysfunction. Objective. Endocrine. Endocrine Facts. Physical Assessment 10/3/2013
 Objective Endocrine Jennifer MacDermott, MS, RN, ACNS BC, NP C, CCRN Clinical Nurse Specialist Surgical Intensive Care Unit Identify abnormal assessment finding sin a patient with endocrine dysfunction.
Objective Endocrine Jennifer MacDermott, MS, RN, ACNS BC, NP C, CCRN Clinical Nurse Specialist Surgical Intensive Care Unit Identify abnormal assessment finding sin a patient with endocrine dysfunction.
RENAL TUBULAR ACIDOSIS An Overview
 RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
Utility and Limitations of the Traditional Diagnostic Approach to Hyponatremia: A Diagnostic Study
 CLINICAL RESEARCH STUDY Utility and Limitations of the Traditional Diagnostic Approach to Hyponatremia: A Diagnostic Study Wiebke Fenske, a Sebastian K. G. Maier, b Anne Blechschmidt, a Bruno Allolio,
CLINICAL RESEARCH STUDY Utility and Limitations of the Traditional Diagnostic Approach to Hyponatremia: A Diagnostic Study Wiebke Fenske, a Sebastian K. G. Maier, b Anne Blechschmidt, a Bruno Allolio,
Electrolyte Abnormalities in the Transplant Recipient
 Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4:
 Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
HYPONATRAEMIA GUIDELINES
 HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Disclaimer. Chapter 3 Disorder of Water, Electrolyte and Acid-base Professor A. S. Alhomida. Disorder of Water and Electrolyte
 Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09. Terminal Learning Objective. References. Hours: 2.0 Last updated: November 2015
 SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
** TMP mean page 340 in 12 th edition. Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2:
 QUESTION Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2: Urine flow rate = 1 ml/min Urine inulin concentration = 100 mg/ml Plasma inulin concentration = 2 mg/ml
QUESTION Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2: Urine flow rate = 1 ml/min Urine inulin concentration = 100 mg/ml Plasma inulin concentration = 2 mg/ml
Saint-Antoine Hospital, Paris. Medical Intensive Unit Care. Hafid Ait-Oufella, MD.PhD. Dyscalcemia. Dyskalemia
 Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris Potassium K + Molecular weight: 39 1gr K + =2.5mmol Potassium disorders in ICU : Our experience
Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris Potassium K + Molecular weight: 39 1gr K + =2.5mmol Potassium disorders in ICU : Our experience
Iposodiemia: diagnosi e trattamento
 Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
 Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
Questions? Homework due in lab 6. PreLab #6 HW 15 & 16 (follow directions, 6 points!)
") Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
Fluid and electrolyte balance, imbalance
 Fluid and electrolyte balance, imbalance Body fluid The fluids are distributed throughout the body in various compartments. Body fluid is composed primarily of water Water is the solvent in which all solutes
Fluid and electrolyte balance, imbalance Body fluid The fluids are distributed throughout the body in various compartments. Body fluid is composed primarily of water Water is the solvent in which all solutes
About Salt, Sodium and Natremic Disorders
 BASICS KERALA MEDICAL JOURNAL About Salt, Sodium and Natremic Disorders R Kasi Viswesaran Ananthapuri Hospital and Research Institute, Trivandrum - 695024* ABSTRACT Published on 26 th March 2009 The factors
BASICS KERALA MEDICAL JOURNAL About Salt, Sodium and Natremic Disorders R Kasi Viswesaran Ananthapuri Hospital and Research Institute, Trivandrum - 695024* ABSTRACT Published on 26 th March 2009 The factors