Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD
|
|
|
- Hilary Nelson
- 5 years ago
- Views:
Transcription
1 Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those who are in a position to affect content of this CME activity are required to disclose financial relationships with any commercial interest(s) related to the subject matter of this activity. The speaker, activity Director, and planning committee have no relevant financial relationships or conflicts of interest to disclose. 2 1

2 Objectives 1. Determine best methods to accurately triage acute pancreatitis patients and most important treatments in early acute severe pancreatitis. 2. Updates on use of antibiotics, IV fluids, nutrition, and imaging in acute pancreatitis. 3. How to deal with delayed complications of severe acute pancreatitis (pancreatic fluid collections, compartment syndrome, splenic vein thrombosis. 3 Don t mess with the pancreas 2

3 Pancreatic anatomy Background History of acute pancreatitis Causes of acute pancreatitis Endoscopic ultrasound Anatomy 3

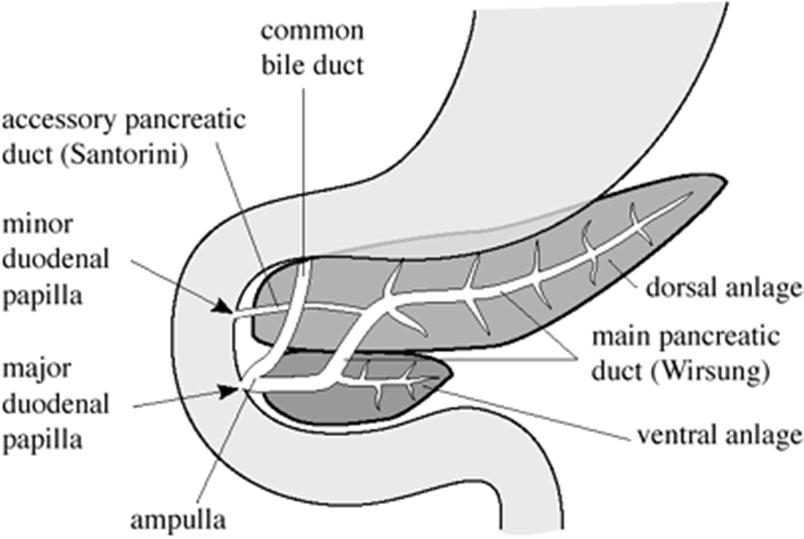
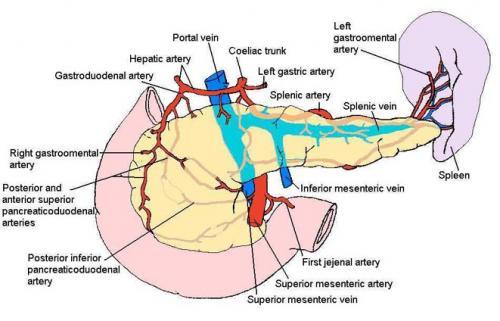
4 Anatomy Anatomy 4
5 History of AP Many deaths, some as early as 320 BC, have been attributed to AP (Alexander the Great). First systematic analysis 1880s, by Dr. Fitz (pathologist at Mass General) Acute Pancreatitis is the most terrible of all the calamities that occur in connection with the abdominal viscera. The suddenness of its onset, the illimitable agony which accompanies it, and the mortality attendant upon it, all render it the most formidable of catastrophies Lord Moynihan (1925) Oreilly. J R Soc Med History of AP Most common GI discharge diagnosis $2.6 billion in 2009 Increase in annual incidence Decreased case fatality rate but overall population mortality has remained unchanged Tenner et al. Am J Gastro


6 Causes of AP Gallstones and ETOH (90%) Drugs aza, PIs, estrogen, tetracyclines, thiazides, loop diuretics, ACEi, etc, etc, etc. Hypertriglyceridemia Hypercalcemia Post ERCP Trauma Infection Genetic Pancreas cancer/cysts Pancreas divisum Autoimmune Types of Echo Endoscopes Radial 6


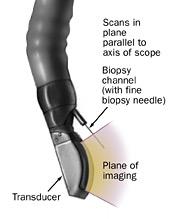
7 Radial Imaging Types of Echo Endoscopes Curvilinear Array 7

8 Curvilinear Imaging: Pancreatitis Diagnosis of acute pancreatitis Triaging acute pancreatitis Management of acute pancreatitis Management of specific complications from severe acute pancreatitis 8
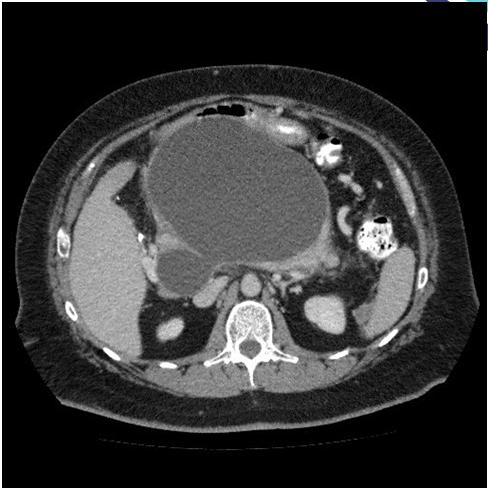
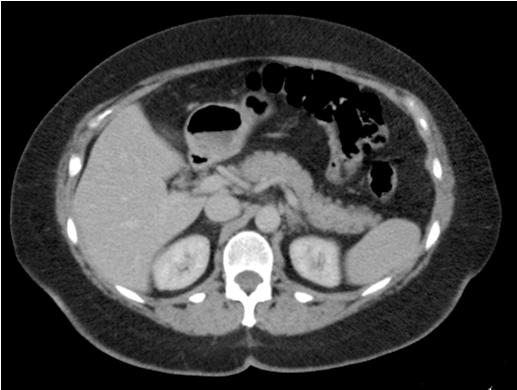
 vs Necrotizing Severity: Mild no end organ failure or local/systemic complications Moderate no organ failure or transient organ failure")
9 Acute Pancreatitis Diagnosis: Atlanta Criteria (Must have 2 of 3) Characteristic abdominal pain Lipase/amylase elevation Imaging showing pancreas inflammation Banks et al. Gut Acute Pancreatitis Classification: Interstitial (80 90%) vs Necrotizing Severity: Mild no end organ failure or local/systemic complications Moderate no organ failure or transient organ failure (<48 hrs) and/or local complications. Severe persistent end organ damage (>48 hours) 9
10 What defines organ failure Shock (SBP <90) Respiratory failure (PaO2 <60) Renal failure (Creat >2 AFTER rehydration) GI bleeding (>500mL/24 hours) Acute Pancreatitis Assessing disease severity: Ranson Criteria needs 48 hours APACHE hard to calculate BISAP BUN >25, impaired MS, SIRS, Age>60, Pleural effusion CT severity index necrosis or not (needs contrast and does not help in the first 72 hours) CRP (takes 72 hours to be accurate) ****Lipase does not predict severity and does not need to be followed after initial diagnosis 10

11 Triaging: Don t worry about any scoring system Determine severity based on presence of organ failure and patient comorbidities Reassess often!!! Management of AP: Fluids How much? How long? Does type matter? 11

12 Fluids How much: Aggressive vs Controlled fluid resuscitation 15ml/kg/hr vs 5 10ml/kg/hr Two retrospective trials from Mayo Clinic showed increased SIRS and increased mortality in the Non aggressive groups A prospective study of 247 pts by de Madaria in 2011 showed that resuscitation with more than 4 L in the first 24 hours lead to persistent organ failure and increased risk of fluid collections Gardner et al. Pacreatology Warndord et al. Clin Gastro Hepatol AGA guidelines: Aggressive hydration ( ml/hr) should be provided to all pts unless CV or renal comorbidities exist. This is most beneficial in the first hours and may have little benefit beyond. Tenner et al. Am J Gastro




13 My recommendations: Give 1 liter bolus up front and then give ml per hour for 6 8 hours and then reassess! urine output, BUN, hct, and blood pressure. BUN at hospitalization and change in BUN at 24 hours predict mortality. What type of fluid? 13
14 Crystalloid vs Colloid Colloids: better with optimizing hemodynamic response and also reduce intraabdominal HTN. Crystalloids: cheaper and more unlimited resource, less risk of intravascular overload. AGA recommends crystalloids unless the hct < 25 or albumin is <2.0 What Crystalloid? Fluids: Wu et al. Clinical Gastro and Hep,
15 Fluids Wu et al. Clinical Gastro and Hep, Summary: Crystalloid > Colloid Fluids Lactated ringers > normal saline Early aggressive hydration.but not too aggressive (3 4 liters in first day is a good goal but use clinical signs) 15


16 Nutrition/Refeeding Management of AP: Nutrition How to refeed in mild AP: RCT with 101 pts Sathiaraj et al. APT

17 Severe Pancreatitis Enteral vs parenteral Nutrition Yi et al. Intern Med 2012 Mortality Nutrition: Yi et al. Intern Med
18 Nutrition Infectious complications Yi et al. Intern Med 2012 Organ failure Nutrition Yi et al. Intern Med

19 Nutrition NJ vs NG Nutrition Metaanalysis of 157 pts Chang et al. Critical Care
20 Nutrition Summary In mild AP: start early, low fat diet In severe AP: Enteral feedings via NG/NJ Management of AP Antibiotics: Treat extra pancreatic infections (20% of AP) NOT recommended for prophylaxis of infected necrosis Used if suspected or proven infected necrosis Consider CT guided aspiration to guide therapy Suspect if known necrosis and clinical deterioration (usually after 10 days) Which abx? Carbapenums, fluoroquinolones + metronidazole Tenner et al. Am J Gastro


21 Management of early complications Splanchnic vein thrombosis Abdominal compartment syndrome Venous anatomy of the abd Nadkarni et al. Pancreas

22 Jiang. WJG Splanchnic vein thrombosis Should we anticoagulate? Only if extension to SMV or portal vein with ischemia to the bowel or liver Risk of variceal bleeding? Only 4% in severe AP with thrombosis Splenectomy? Only for chronic pancreatitis with SVT 22

23 Abdominal compartment syndrome Intraabdominal hypertension = sustained pressure over 15mmHg ACS: abdominal pressure >20mmhg + new organ dysfunction Abdominal Compartment Syndrome Why do patients with pancreatitis get this? Third spacing/ascites Aggressive fluid resuscitation Ileus One study showed that 60% of patients in the ICU with severe AP had IAH and these pts had higher organ dysfunction, longer hospital stays, and higher mortality. Al Bahrani et al. Pancreas


24 Abdominal compartment syndrome How should we monitor this? 24

25 Late Complications Management of Complications Local Complications: Timing and indication for CT scan? 72 hours if severe pancreatitis or clinical deterioration Acute peripancreatic fluid collections 4 wks Pseudocysts Acute necrotic collection 4 wks Walled off necrosis 25
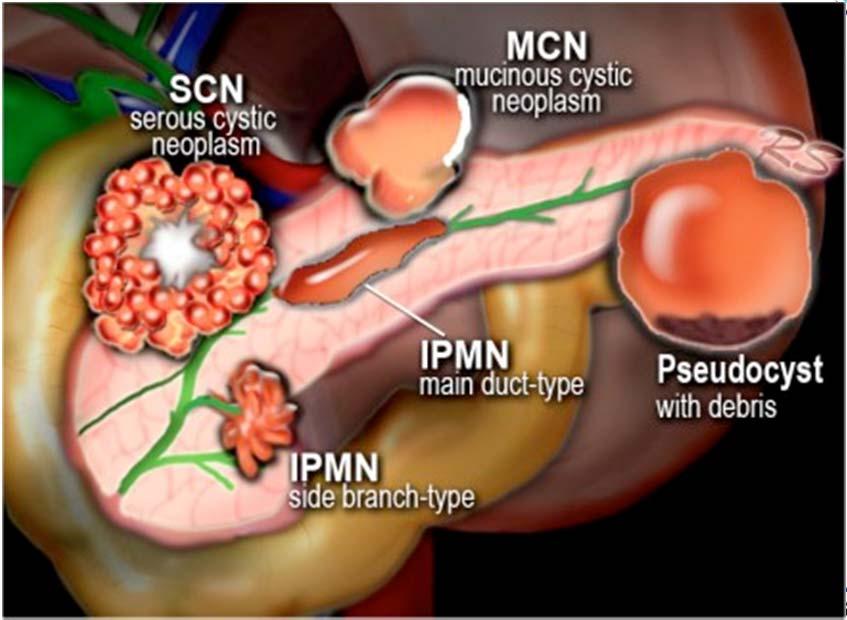
26 Pancreatic Cysts Walled Off Fluid Collections 26
27 Walled off Fluid Collections Expectant management: If asymptomatic (~ 40 60% in some studies) Symptoms: Pain, N/V, early satiety, jaundice, unexplained fever Often takes 6 12 months to resolve, sometimes longer Vitas et al. Surgery Walled off Fluid Collections Drainage options: Surgical drainage Percutaneous drainage Endoscopic drainage Combination of 2 or more of the above 27
28 Surgical Drainage Most invasive and most morbid Laparascopic cystgastrostomy Open necroscetomy NEJM study 2010 Van Santvoort et al. NEJM


29 NEJM 2010 Van Santvoort et al. NEJM 2010 Percutaneous drainage Advantages: Least invasive Successful for most locations Drain can be placed before maturity Disadvantages: Fistula formation External drain Takes a long time Risk of infection 29



")
30 Endoscopic Cystgastrostomy --Can only be done after the cyst is mature (4-6 weeks from initial pancreatitis) Necrosectomy 30
31 Endoscopic Necrosectomy Advantages: 80 85% successful alone (455 pt systematic review) Typically well tolerated Allows for debridement Disadvantages: Location limited by GI lumen Tedious Risk of bleeding, air embolism 6% mortality (during same systematic review) Brunschot et al. Surg Endosc Miscellaneous management of AP When to do ERCP in gallstone pancreatitis? When should GB come out after pancreatitis? How high are triglycerides that cause AP? Acute on chronic pancreatitis 31

32 Questions? 32
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Acute Pancreatitis. Encourage You to Read!
 Acute Pancreatitis Laith H. Jamil, MD, FACG Associate Director of Interventional Endoscopy Cedars Sinai Medical Center Los Angeles, CA Encourage You to Read! Copyright 2015 American College of Gastroenterology
Acute Pancreatitis Laith H. Jamil, MD, FACG Associate Director of Interventional Endoscopy Cedars Sinai Medical Center Los Angeles, CA Encourage You to Read! Copyright 2015 American College of Gastroenterology
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Acute Pancreatitis:
 American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good. Karen Lo R 3 University of Colorado Oct 11, 2010
 Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good Karen Lo R 3 University of Colorado Oct 11, 2010 Overview Pancreas: The History Pancreas: The Organ The Disease Pathogenesis
Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good Karen Lo R 3 University of Colorado Oct 11, 2010 Overview Pancreas: The History Pancreas: The Organ The Disease Pathogenesis
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Acute Pancreatitis. Falk Symposium 161 Dresden
 Acute Pancreatitis Falk Symposium 161 Dresden 12.10.2007 Incidence of Acute Pancreatitis (Malmö) Lindkvist B, et al Clin Gastroenterol Hepatol 2004;2:831-837 Gallstones Alcohol AGA Medical Position Statement
Acute Pancreatitis Falk Symposium 161 Dresden 12.10.2007 Incidence of Acute Pancreatitis (Malmö) Lindkvist B, et al Clin Gastroenterol Hepatol 2004;2:831-837 Gallstones Alcohol AGA Medical Position Statement
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Pancreatitis: Critical care and Nutritional Considerations. Vance L. Smith, MD Montefiore Medical Center Acute Care Surgery
 Pancreatitis: Critical care and Nutritional Considerations Vance L. Smith, MD Montefiore Medical Center Acute Care Surgery No disclosures Pathophysiology Mr. H. 42 yo male found to have gallstone pancreatitis
Pancreatitis: Critical care and Nutritional Considerations Vance L. Smith, MD Montefiore Medical Center Acute Care Surgery No disclosures Pathophysiology Mr. H. 42 yo male found to have gallstone pancreatitis
A Comparative Study of Different Predictive Severity Scoring Systems for Acute Pancreatitis in Relation To Outcome A Prospective Study
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 12 Ver. 2 (December. 2018), PP 01-09 www.iosrjournals.org A Comparative Study of Different
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 12 Ver. 2 (December. 2018), PP 01-09 www.iosrjournals.org A Comparative Study of Different
Endoscopic Management of Acute Pancreatitis. Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018
 Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Nothing to declare. Probable causes for the change
 acute pancreatitis March 25, 2017 C. S PITCHUMONI. MD,MACP,MACG,MPH.FRCP (c) Adjunct Professor of Medicine New York Medical College Professor of Medicine Rutgers university Nothing to declare Lesser sac?
acute pancreatitis March 25, 2017 C. S PITCHUMONI. MD,MACP,MACG,MPH.FRCP (c) Adjunct Professor of Medicine New York Medical College Professor of Medicine Rutgers university Nothing to declare Lesser sac?
Exocrine functions: secretion of digestive enzymes (eg. lipase, amylase,
 Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Joint Trust Management of Acute Severe Pancreatitis in Adults
 A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Emergency Surgery Course Graz, March ACUTE PANCREATITIS. Carlos Mesquita Coimbra
 ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
Correspondence should be addressed to Supot Pongprasobchai;
 Hindawi Gastroenterology Research and Practice Volume 2017, Article ID 3525349, 7 pages https://doi.org/10.1155/2017/3525349 Research Article Severity, Treatment, and Outcome of Acute Pancreatitis in Thailand:
Hindawi Gastroenterology Research and Practice Volume 2017, Article ID 3525349, 7 pages https://doi.org/10.1155/2017/3525349 Research Article Severity, Treatment, and Outcome of Acute Pancreatitis in Thailand:
University of Colorado
 University of Colorado Dept. of Surgery Grand Rounds Prophylactic Antibiotics in Severe Acute Pancreatitis Eduardo Gonzalez, PGY2 Mortality from Acute Pancreatitis SAP 1 - >30% necrosis - SBP2.0,
University of Colorado Dept. of Surgery Grand Rounds Prophylactic Antibiotics in Severe Acute Pancreatitis Eduardo Gonzalez, PGY2 Mortality from Acute Pancreatitis SAP 1 - >30% necrosis - SBP2.0,
American College of Gastroenterology Guideline: Management of Acute Pancreatitis
 PRACTICE GUIDELINES nature publishing group 1 American College of Gastroenterology Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG1, John Baillie, MB, ChB, FRCP, FACG 2, Joh n D
PRACTICE GUIDELINES nature publishing group 1 American College of Gastroenterology Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG1, John Baillie, MB, ChB, FRCP, FACG 2, Joh n D
Randomized Controlled Trials in Pancreatic Diseases. James Buxbaum MD University of Southern California Los Angeles County Hospital
 Randomized Controlled Trials in Pancreatic Diseases James Buxbaum MD University of Southern California Los Angeles County Hospital Randomized Trials in Pancreatic Diseases Focus acute pancreatitis Challenges
Randomized Controlled Trials in Pancreatic Diseases James Buxbaum MD University of Southern California Los Angeles County Hospital Randomized Trials in Pancreatic Diseases Focus acute pancreatitis Challenges
Sepsis in Acute Pancreatitis. MD Smith Department of Surgery University of the Witwatersrand, Johannesburg Chris Hani Baragwanath Academic Hospital
 Sepsis in Acute Pancreatitis MD Smith Department of Surgery University of the Witwatersrand, Johannesburg Chris Hani Baragwanath Academic Hospital Introduction Self limiting disease in 85% Minority develop
Sepsis in Acute Pancreatitis MD Smith Department of Surgery University of the Witwatersrand, Johannesburg Chris Hani Baragwanath Academic Hospital Introduction Self limiting disease in 85% Minority develop
Acute Pancreatitis: New Developments and Strategies for the Hospitalist
 REVIEWS Acute Pancreatitis: New Developments and Strategies for the Hospitalist John F. Dick, III, MD 1 *, Timothy B. Gardner, MD, MS 2, Edward J. Merrens, MD, MS 1 1 Geisel School of Medicine, Section
REVIEWS Acute Pancreatitis: New Developments and Strategies for the Hospitalist John F. Dick, III, MD 1 *, Timothy B. Gardner, MD, MS 2, Edward J. Merrens, MD, MS 1 1 Geisel School of Medicine, Section
Management of Acute Pancreatitis
 Management of Acute Pancreatitis A Clinical Practice Guideline developed by the University of Toronto s Best Practice in Surgery JA Greenberg, M Bawazeer, J Hsu, J Marshall, JO Friedrich, A Nathens, N
Management of Acute Pancreatitis A Clinical Practice Guideline developed by the University of Toronto s Best Practice in Surgery JA Greenberg, M Bawazeer, J Hsu, J Marshall, JO Friedrich, A Nathens, N
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Acute pancreatitis Case reports. Clinical problems. Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4)
 Surgical treatment of AP? (P 3 & 4)") Case reports Clinical problems Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4) Case reports Case 1 Case 1 Patient KD History M, 63 y Obesity BMI 30.3 kg/m 2 Gallbladder stones No concomitant
Case reports Clinical problems Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4) Case reports Case 1 Case 1 Patient KD History M, 63 y Obesity BMI 30.3 kg/m 2 Gallbladder stones No concomitant
Surgical Management of Acute Pancreatitis
 Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
A Prospective Study of Bedside Index for Severity in Acute Pancreatitis Score in Acute Pancreatitis
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/210 A Prospective Study of Bedside Index for Severity in Acute Pancreatitis Score in Acute Pancreatitis S Kasturi Bai
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/210 A Prospective Study of Bedside Index for Severity in Acute Pancreatitis Score in Acute Pancreatitis S Kasturi Bai
U Nordic Forum - Trauma & Emergency Radiology. Lecture Objectives. MDCT in Acute Pancreatitis. Acute Pancreatitis: Etiologies
 Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Original Article. Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome
 Tropical Gastroenterology 2015;36(1):31 35 Original Article Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome Surinder S Rana 1, Vishal Sharma 1, Deepak
Tropical Gastroenterology 2015;36(1):31 35 Original Article Gastrointestinal bleeding in acute pancreatitis: etiology, clinical features, risk factors and outcome Surinder S Rana 1, Vishal Sharma 1, Deepak
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance of Gillian Lieberman, MD
 Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Morning Report. Allison Haden, MD October 1, 2002
 Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Anubhav Harshit Kumar* and Mahavir Singh Griwan ORIGINAL ARTICLE. Abstract. Department of Surgery, Pt. B. D. Sharma PGIMS, Rohtak, India
 Gastroenterology Report, 2017, 1 5 doi: 10.1093/gastro/gox029 Original article ORIGINAL ARTICLE A comparison of APACHE II, BISAP, Ranson s score and modified CTSI in predicting the severity of acute pancreatitis
Gastroenterology Report, 2017, 1 5 doi: 10.1093/gastro/gox029 Original article ORIGINAL ARTICLE A comparison of APACHE II, BISAP, Ranson s score and modified CTSI in predicting the severity of acute pancreatitis
Endoscopic pancreatic necrosectomy in 2017
 Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
Does it matter what we drain?
 Endoscopic Management of Pancreatic Fluid Collections Shyam Varadarajulu, MD Medical Director Center for Interventional Endoscopy Florida Hospital, Orlando Does it matter what we drain? Makes all the difference!
Endoscopic Management of Pancreatic Fluid Collections Shyam Varadarajulu, MD Medical Director Center for Interventional Endoscopy Florida Hospital, Orlando Does it matter what we drain? Makes all the difference!
Harsukh Educational Charitable Society International Journal of Community Health and Medical Research
 Harsukh Educational Charitable Society International Journal of Community Health and Medical Research Journal home page: www.ijchmr.com doi: 10.21276/ijchmr Official Publication of Harsukh Educational
Harsukh Educational Charitable Society International Journal of Community Health and Medical Research Journal home page: www.ijchmr.com doi: 10.21276/ijchmr Official Publication of Harsukh Educational
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Purpose of review To review the changing insights in the pathophysiology and management of acute pancreatitis.
 REVIEW C URRENT OPINION Acute pancreatitis Jan J. De Waele Purpose of review To review the changing insights in the pathophysiology and management of acute pancreatitis. Recent findings The outdated 1992
REVIEW C URRENT OPINION Acute pancreatitis Jan J. De Waele Purpose of review To review the changing insights in the pathophysiology and management of acute pancreatitis. Recent findings The outdated 1992
Overview. The Pancreas Pancreatitis Signs + Symptoms Investigations Grading Systems Role of Surgery Management of Chronic Pancreatitis Summary
 James Bain May 2014 1. What are the grading systems for Pancreatitis? 2. What is the role of surgery in acute pancreatitis? 3. What the principles of managing chronic pancreatitis? Overview The Pancreas
James Bain May 2014 1. What are the grading systems for Pancreatitis? 2. What is the role of surgery in acute pancreatitis? 3. What the principles of managing chronic pancreatitis? Overview The Pancreas
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
CLINICAL CASE OF THE MONTH. A 35 Year Old Woman with Abdominal Pain
 CASE REPORT JOURNAL OF THE LOUISIANA STATE MEDICAL SOCIETY CLINICAL CASE OF THE MONTH A 35 Year Old Woman with Abdominal Pain Melissa Spera, MD, Camille Thelin, MD, Abby Gandolfi, MD, Nicholas Clayton,
CASE REPORT JOURNAL OF THE LOUISIANA STATE MEDICAL SOCIETY CLINICAL CASE OF THE MONTH A 35 Year Old Woman with Abdominal Pain Melissa Spera, MD, Camille Thelin, MD, Abby Gandolfi, MD, Nicholas Clayton,
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Mild. Moderate. Severe
 2012 Revised Atlanta Classification Acute pancreatitis Classified based on absence or presence of local and/or systemic complications Mild Acute Pancreatits Moderate Severe P. A. Banks, T. L. Bollen, C.
2012 Revised Atlanta Classification Acute pancreatitis Classified based on absence or presence of local and/or systemic complications Mild Acute Pancreatits Moderate Severe P. A. Banks, T. L. Bollen, C.
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Patients With Severe Acute Pancreatitis Should Be More Often Treated In An Intensive Care Department
 ISPUB.COM The Internet Journal of Emergency and Intensive Care Medicine Volume 6 Number 2 Patients With Severe Acute Pancreatitis Should Be More Often Treated In An Intensive Care Department M Dinis-Ribeiro,
ISPUB.COM The Internet Journal of Emergency and Intensive Care Medicine Volume 6 Number 2 Patients With Severe Acute Pancreatitis Should Be More Often Treated In An Intensive Care Department M Dinis-Ribeiro,
Early Fluid Resuscitation Reduces Morbidity Among Patients With Acute Pancreatitis
 CLINICAL GASTROENTEROLOGY AND HEATOLOGY 2011;9:705 709 Fluid Resuscitation Reduces Morbidity Among atients With Acute ancreatitis MATTHEW G. WARNDORF, JANE T. KURTZMAN, MICHAEL J. BARTEL, MOUGNYAN COX,
CLINICAL GASTROENTEROLOGY AND HEATOLOGY 2011;9:705 709 Fluid Resuscitation Reduces Morbidity Among atients With Acute ancreatitis MATTHEW G. WARNDORF, JANE T. KURTZMAN, MICHAEL J. BARTEL, MOUGNYAN COX,
Severe Dengue Infection in ICU. Shirish Prayag MD, FCCM Pune, India
 Severe Dengue Infection in ICU Shirish Prayag MD, FCCM Pune, India Greetings from India Declaration Honararia from MSD, Astra Zenecea, Fresenius Kabi, Pfizer, Intas, Glenmark for conducting lectures. No
Severe Dengue Infection in ICU Shirish Prayag MD, FCCM Pune, India Greetings from India Declaration Honararia from MSD, Astra Zenecea, Fresenius Kabi, Pfizer, Intas, Glenmark for conducting lectures. No
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Multi modality Imaging in Acute Pancreatitis. Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009
 Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosure 6/13/2015. Acute Pancreatitis - Update. Causes of mortality DEATH
 Disclosure Acute Pancreatitis - Update Jamie S. Barkin, MD, MACP. MACP Professor of Medicine Division of Gastroenterology I do not have any relevant financial relationships with any commercial interests.
Disclosure Acute Pancreatitis - Update Jamie S. Barkin, MD, MACP. MACP Professor of Medicine Division of Gastroenterology I do not have any relevant financial relationships with any commercial interests.
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
THE CLINICAL course of severe
 ORIGINAL ARTICLE Improved Prediction of Outcome in Patients With Severe Acute Pancreatitis by the APACHE II Score at 48 Hours After Hospital Admission Compared With the at Admission Arif A. Khan, MD; Dilip
ORIGINAL ARTICLE Improved Prediction of Outcome in Patients With Severe Acute Pancreatitis by the APACHE II Score at 48 Hours After Hospital Admission Compared With the at Admission Arif A. Khan, MD; Dilip
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
ACG Postgraduate Course. Multidisciplinary Approach to Acute Pancreatitis Medical Management of Acute Pancreatitis
 ACG Postgraduate Course Multidisciplinary Approach to Acute Pancreatitis Medical Management of Acute Pancreatitis Timothy B. Gardner, MD MS FACG Assistant Professor of Medicine Geisel School of Medicine
ACG Postgraduate Course Multidisciplinary Approach to Acute Pancreatitis Medical Management of Acute Pancreatitis Timothy B. Gardner, MD MS FACG Assistant Professor of Medicine Geisel School of Medicine
VIDEO ASSISTED RETROPERITONEAL DEBRIDEMENT IN HUGE INFECTED PANCREATIC PSEUDOCYST
 Trakia Journal of Sciences, Vol. 13, Suppl. 2, pp 102-106, 2015 Copyright 2015 Trakia University Available online at: http://www.uni-sz.bg ISSN 1313-7050 (print) doi:10.15547/tjs.2015.s.02.022 ISSN 1313-3551
Trakia Journal of Sciences, Vol. 13, Suppl. 2, pp 102-106, 2015 Copyright 2015 Trakia University Available online at: http://www.uni-sz.bg ISSN 1313-7050 (print) doi:10.15547/tjs.2015.s.02.022 ISSN 1313-3551
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE. T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar
 ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar LEARNING OBJECTIVES q Through a series of cases illustrate the updated Atlanta symposium
ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar LEARNING OBJECTIVES q Through a series of cases illustrate the updated Atlanta symposium
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC Sept
 Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Chronic Pancreatitis
 Gastro Foundation Fellows Weekend 2017 Chronic Pancreatitis Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Aetiology in SA Alcohol (up to 80%) Idiopathic Tropical Obstruction Autoimmune
Gastro Foundation Fellows Weekend 2017 Chronic Pancreatitis Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Aetiology in SA Alcohol (up to 80%) Idiopathic Tropical Obstruction Autoimmune
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
Slide 1. Slide 2. Slide 3. Acute Pancreatitis: An Evidence-Based Clinical Approach in Case. Important Clinical Questions
 Slide 1 Acute Pancreatitis: An Evidence-Based Clinical Approach in 2014 David G. Forcione, MD Associate Director Interventional Endoscopy Slide 2 Case A 68 yo M p/w acute onset of sharp epigastric pain,
Slide 1 Acute Pancreatitis: An Evidence-Based Clinical Approach in 2014 David G. Forcione, MD Associate Director Interventional Endoscopy Slide 2 Case A 68 yo M p/w acute onset of sharp epigastric pain,
What Is Pancreatitis?
 What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions
 MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
Pancreatic Disease. Chapter. Overview. Diagnosis of the Disease. Francisco Igor B. Macedo and Danny Sleeman. Laboratory Testing
 Chapter 128 Pancreatic Disease Francisco Igor B. Macedo and Danny Sleeman Overview Acute pancreatitis has an annual incidence of 5 to 40 per 100,000 with an overall mortality of 1.5 per 100,000 (1). The
Chapter 128 Pancreatic Disease Francisco Igor B. Macedo and Danny Sleeman Overview Acute pancreatitis has an annual incidence of 5 to 40 per 100,000 with an overall mortality of 1.5 per 100,000 (1). The
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Percutaneous Catheter Drainage in the Management of Severe Acute Pancreatitis
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 8 Ver. II (Aug. 2017), PP 29-37 www.iosrjournals.org Percutaneous Catheter Drainage in the
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 8 Ver. II (Aug. 2017), PP 29-37 www.iosrjournals.org Percutaneous Catheter Drainage in the
JMSCR Vol 04 Issue 08 Page August 2016
 www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i8.08 Acute Pancreatitis with Normal Amylase
www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i8.08 Acute Pancreatitis with Normal Amylase
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
MANAGEMENT OF DENGUE INFECTION IN ADULTS (Revised 2 nd Edition) QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS") 1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Acute and Chronic Pancreatitis
 Acute and Chronic Pancreatitis Diagnosis of Acute Pancreatitis Two of the following three features: Darwin L. Conwell, MD,MS Associate Director BWH Center for Pancreatic Disease Brigham and Women s Hospital
Acute and Chronic Pancreatitis Diagnosis of Acute Pancreatitis Two of the following three features: Darwin L. Conwell, MD,MS Associate Director BWH Center for Pancreatic Disease Brigham and Women s Hospital
MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13
 MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS
MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no