The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess
|
|
|
- Constance Bailey
- 5 years ago
- Views:
Transcription
1 The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program Director University of Michigan
2 Disclosures Contracted Research Millendo Therapeutics Novartis Pharmaceuticals Strongbridge Biopharma Consultant Laboratory Corporation of America Corcept Therapeutics Janssen Pharmaceuticals Novartis Pharmaceuticals Innocrin Pharmaceuticals Diurnal, LTD Alder BioPharmaceuticals Spruce Biosciences
3 Magnitude of the Problem Adrenal Nodules Found in 1-7% of CT Scans Performed for Unrelated Reasons Prevalence Increases with Age, H/O CA US Population >300,000,000 ~3-21 Million Adrenal Nodules ~4,000 Endocrinologists in USA If All Endocrinologists Saw 8/Week, It Could Take Up To 15 Yr To See All(!!)

4 Adrenal CT: Normal Glands

5 CT: Typical Adrenal Nodule
6 Incidental Adrenal Nodules Differential Diagnosis Nonfunctioning Cortical Adenoma Cortisol-Producing Adenoma/Nodular Disorders Aldosterone- or DOC-Producing Adenoma Adrenocortical Carcinoma Pheochromocytoma Myelolipoma Cyst Metastatic Carcinoma Lymphoma Infection/Granuloma Hemorrhage Congenital Adrenal Hyperplasia
7 Incidental Adrenal Nodules Non-Adrenal Tumors Renal Cysts and Masses Accessory Spleen Gastric Duplication Ganglioneuromas Retroperitoneal Tumors
8 Three Parts Of The Evaluation Look at the Scan Size, Imaging Characteristics The OTHER Adrenal Interview & Examine the Patient History, Physical Exam, Recent Changes Laboratory Evaluation Routine & Directed Testing
9 Part 1: Imaging Data Size: <2, 2-4, >4 cm Useful Gauge Noncontrasted CT Density <10 HU = Lipid-Rich Adrenocortical Tumor Might Cause Hormone Excess Homogeneity or Lack Thereof Contrast Enhancement Amount, Pattern, Washout Other Suspicious Features Lymph Nodes, Invasion, IVC Thrombus

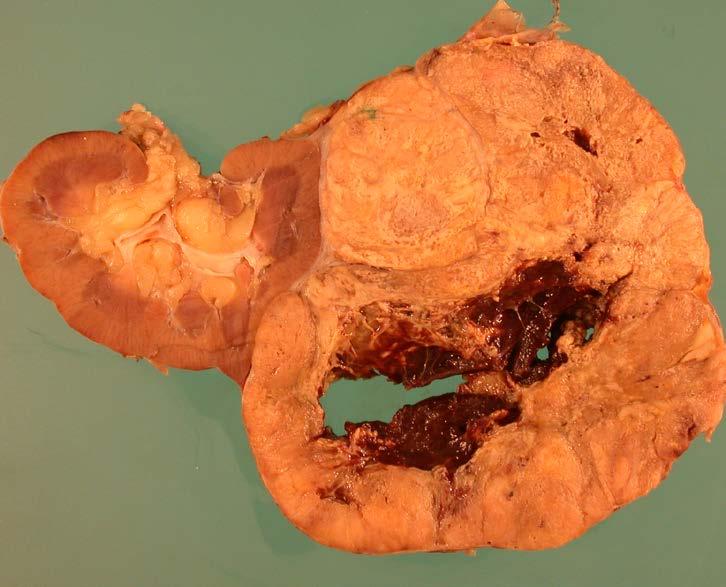
10 Large is Bad Adrenocortical Cancer

11 CT: Pheochromocytoma Large, Heterogeneous
12 Part 1: Ancillary Imaging Data MRI: Signal Loss on Out-of-Phase Images = High Lipid Content Not Routinely Necessary High Signal on T2-Wtd = Pheo, Other 123 I-MIBG, 111 In-Pentotreotide SPECT/CT Should Follow Biochemical Testing 18 F-FDG, 68 Ga-DOTATATE PET/CT Question of CA, Metastasis Preferable to Biopsy Most Cases 10% of Benign Tumors PET-Avid (Pheo)

13 Pheo: Hyperintense On T2-MRI

14 Pheo: Hyperintense On T2-MRI
15 Incidental Adrenal Nodules Part 2: History & Physical Known Malignancy? Weight Change? HTN? Paroxysms? Myopathy? DM? Bruising? Cushing s Stigmata: SC/DC Fat Pads, Thin Skin & Bruising, Muscle Weakness, Plethora Androgen Excess (Women)?
16 Cushing Syndrome Common Features Central Obesity Metabolic: Glucose, TG; K; HTN Women: Amenorrhea, Hirsutism Depression, Psychosis Dorsocervical Fat Pad Supraclavicular More Specific Children: Growth Impairment
17 Cushing Syndrome Discriminatory Features Proximal Muscle Weakness/Myopathy Osteoporosis Wide, Purple Striae Easy Bruising Supraclavicular Fat Pads Disproportionate Head & Neck Fat Facial & Upper Chest Plethora


18
19 Incidental Adrenal Nodules Part 3: Basic Laboratory Evaluation Screen For Cushing s 1 mg ONDST, <1.8 μg/dl = 50 nmol/l 24 h UFC Poor Sensitivity For Early Cushing s Additional Testing if Suspicious Screen For Pheochromocytoma 24 h Urine or Plasma Metanephrines Plasma More Sensitive But Less Specific Avoid Caffeine, Acetaminophen, TCA, SSRIs, Phenoxybenzamine, Levodopa >2x ULN Urine, >1 nmol/l Plasma = Positive ****Most Slightly Elevated NorMN = False Positive Screen For Primary Aldo if HTN &/or Low K
20 Catecholamine Catabolism OH OH HO NH 2 HO NHCH 3 HO Norepinephrine OH COMT HO Epinephrine OH HO NH 2 HO NHCH 3 CH 3 O Normetanephrine MAO CH 3 O Metanephrine OH HO CH 3 O CO 2 H Vanillylmandelic Acid (VMA)
21 Case 1 58 YO WM, Single Episode Hematuria No Paroxysms, Nl BP US: R Adrenal Mass 24 h Urine MN 233 mcg, NMN 2504 mcg MRI: 3.4 cm R adrenal mass High, Heterogeneous Signal T2-weighted No Signal Drop-out Out-of-phase T1 Plasma MN, NMN 0.45 & 7.65 nmol/l

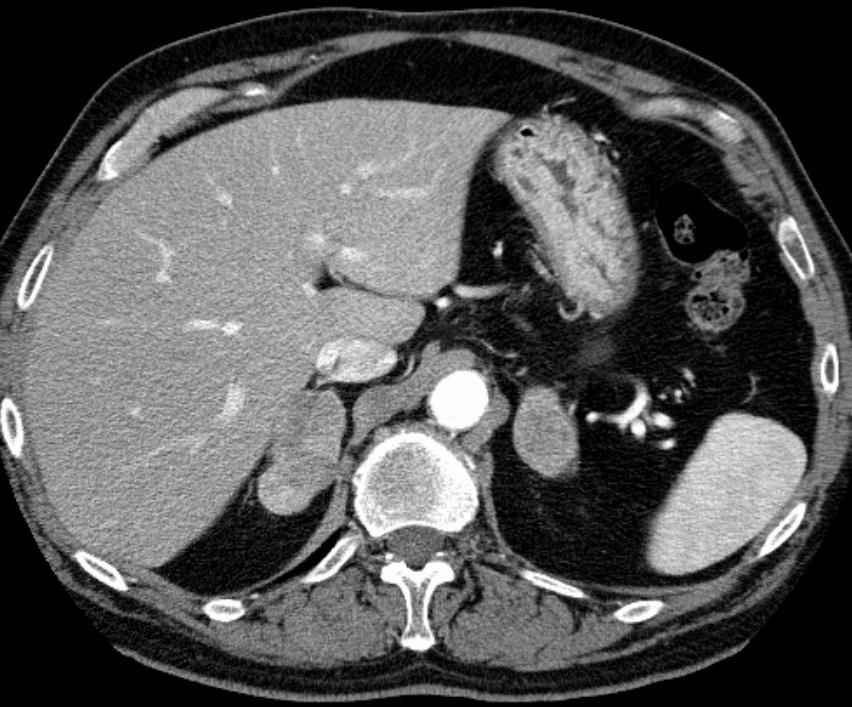
22 Case 1: CT Scan
23 Cushing Syndrome Principles of Testing Cortisol Production is Elevated Urinary Free Cortisol The Diurnal Rhythm is Blunted Serum/Saliva Cortisols at Night Cortisol Production Not Suppressible Dexamethasone Suppression Tests Distinguish From Pseudocushing State ACTH-Dependent or Independent
24 SCS & Adrenal Nodules Who To Screen More Carefully >2 cm Adrenal Mass Clinical Findings: Bruising, SC Fat Pads Recent Changes: DM, HTN, Fat Redistribution How To Test Early AM ACTH, Random DHEAS, ON-DST 24h UFC, Nocturnal Saliva Cortisol Insensitive Repeat, REPEAT, REPEAT Surgery Improves Morbidities in SCS Primarily HTN, Glucose Tolerance IF PRESENT
25 CRH CRH ACTH ACTH Cortisol DHEA-S Cortisol DHEA-S Cortisol DHEA-S Cortisol DHEA-S
26 Discordance In Commercial ACTH Assays Pecori Giraldi F et al. Eur J Endocrinol 2011;164:
27 Case 2 37-yo WF, New Onset HTN, IFG CT: 2.3 cm Left Adrenal Mass Mild Weight Gain, Regular Menses PE: Mild Facial Plethora, Moon Facies, Dermal Atrophy, SC Fat Pads, Central Obesity 10/2013 5/ /2014 ACTH DHEAS ONDST

28 CT Scan 11/ cm
29 Macronodular Hyperplasia
30 Case 3: History 50 y/o WF G5P3, Worsening Hirsutism Mostly Upper Arms Menses Age 16 & Regular, Now Scant Hirsutism Age 16, Rx Electrolysis Cleared chin/moustache/sideburns/nipples By 30s Needed Electrolysis on Abdomen Testosterone = 179 ng/dl (nl <50) CT: No Adrenal Tumor -- BUT

31
32 Case 3: Lab Data Repeat Testosterone 121 ng/dl SHBG 52 nmol/l DHEA-S 427 mcg/dl Basal 17OHP 1,144 ng/dl After Cosyntropin >17,000 ng/dl Diagnosis: Nonclassic 21OHD
33 Incidental Adrenal Nodules Follow-Up Recommendations Directed Annual History And Physical Repeat Screening: Index Of Suspicion Repeat Imaging As Indicated Probably Everyone In 1 Year, Stop If Stable Larger Nodules Sooner/More Frequently Indications For Surgery Hyperfunction Or Mass Effect Size >6 cm (?3 cm) Or Worrisome Features >3 cm Often Subtle Cortisol Excess
34 Subclinical Cushing Syndrome Mild ACTH-Independent Hypercortisolism ~25% Subtle Cortisol Excess (SCS) Evident On Careful Testing 90% Have Hypertension 50% Have DM, Dyslipidemia, Obesity 10% Progress to Overt Cushing Syndrome Prevalence Higher if >2.5 cm
 2 Chiodini I, et al. Clin Endocrinol (Oxf).")
35 Association between osteoporosis/vcf and Subclinical Hypercortisolism (SH) Chiodini (2009) 2 Chiodini I, et al. Clin Endocrinol (Oxf). 2009;70(2):

36 Effect of Mild Cushing syndrome (CS) on Mortality Di Dalmazi (2014): retrospective, single-center study of 198 consecutive patients with adrenal incidentaloma Mean f/u 7.2 years 34% baseline and 43% at study end had dysregulated cortisol Mean follow-up period 7.5 years; mean age range years Subclinical CS, n=10 Stable subclinical CS, n=10 Worsened, n=23 (moved up at least 1 category) Intermediate phenotype, n=59 Stable intermediate phenotype, n=51 Non-secreting, n=129 Stable non-secreting, n=114 Baseline Post-DST cortisol (ng/dl) >5.0 = Subclinical CS = Intermediate phenotype (IP) <1.8 = Non-secreting Study end Di Dalmazi G, et al. Lancet Diabetes Endocrinol. 2014;2(5):
37 Di Dalmazi: Higher mortality in patients with subclinical CS Kaplan-Meier analysis: mortality by status at follow-up Worsened Stable intermediate phenotype/subclinical Cushing s syndrome (Stable IP/subclinical CS) Stable non-secreting 100 All-cause mortality 100 Cardiovascular-specific mortality Proportion surviving (%) Number at risk Stable non-secreting Stable IP/subclinical CS Worsened Follow-up (years) Follow-up (years) Di Dalmazi G, et al. Lancet Diabetes Endocrinol. 2014;2(5):
38 Association of SH with CV Events Morelli (2014): retrospective multicenter study of 206 patients with adrenal incidentaloma and no overt signs of hypercortisolism Minimum follow-up period 5 years (median 72.3 months) Positive SH diagnosis if: 1-mg DST cortisol >5 μg/dl -OR- At least 2 of the following: ACTH <10 pg/ml and/or UFC >ULN and/or 1-mg DST cortisol >3 μg/dl SH patients were older and had larger adenomas Without SH Baseline SH Developed SH during follow-up n (%) 167 (81.1%) 24 (11.6%) 15 (7.3%) Mean age, y Adenoma diameter, cm 2.2 ± ± ±0.7 Morelli V, et al. J Clin Endocrinol Metab. 2014;99(3):
39 Increased Cardiovascular Event (CVE) in SH Outcome Odds ratio (OR) P value Prevalent CVE 3.1 <0.05 Incident CVE Worsening metabolic profile* *Increase in at least 2 parameters: body weight, blood pressure, glycemia, and/or LDL cholesterol Risk of incident CVE: Adenoma diameter >2.4 cm and DST cortisol >1.8 μg/ml confers elevated risk, even in the absence of SH Sensitivity 1.5 μg/dl (41.4 nmol/l) 2.0 μg/dl (55.2 nmol/l) 1-mg DST cortisol levels with the best sensitivity and specificity for predicting incident CVE Morelli V, et al. J Clin Endocrinol Metab. 2014;99(3): Specificity
 >1.")
40 Cortisol as a Marker for Increased Mortality in Patients with Incidental Adrenocortical Adenomas 206 patients consecutive patients with incidental adrenal nodule (benign) with mean f/u 4.2 yrs Overnight 1 mg DST: <1.8 µg/dl (n=95) >1.8 µg/dl (n=111) Kaplan-Meier survival curve according to post-dex cortisol excluding extraadrenal malignancy Debono M, et al JCEM 2014;99:
41 Postoperative Changes Characteristic Improvement Easy Bruising 100% (9/9) Facial Plethora 100% (3/3) Weight Gain 89% (8/9) Hypertension 75% (6/8) Diabetes 67% (2/3) Significant Fatigue 80% (4/5) Proximal Weakness 75% (6/8) Abnormal Fat Pads 63%(5/8) Mitchell et al 2007 Surgery 142:900

42 Mild Adrenal Cushing Syndrome Surgical Outcomes Chiodini et al 2010 JCEM 95:2736
43 Primary Aldosteronism Key Points Most Common Cause of Secondary HTN High End-Organ Damage Curable or Targeted Therapy Low Rates of Screening & Diagnosis Fear of Embarking On Workup Confusion About Approach <1% Ever Screened Syndrome With Many Etiologies
44 Funder et al 2016 JCEM 101:1889
45 Primary Aldosteronism Whom To Screen? HTN + Hypokalemia Patients With Resistant HTN Or Controlled With 4 Drugs Patients With HTN At Age < 40 Or FH HTN or CVA Age <40 Considering Secondary Causes Sustained BP >150/100 HTN + Known Adrenal Mass or OSA HTN + First-Degree Relative With PA
46 Primary Aldosteronism Screening Procedure: Stop Drugs? Most Drugs OK for Screening Most Drugs PRA & Aldo (β-blockers PRA) If PRA is Suppressed, Screen is Valid Up to 4 Wk: Spironolactone, Eplerenone BUT STILL OK if PRA Suppressed Best: α 1 -Blocker + Verapamil Can Always Rescreen After Off Drugs
47 ARR Sensitivity & Specificity Nishizaka 2005 Am J Hypertens 18:805
48 Who Has Primary Aldo? ARR Interpretation Aldo PRA ARR K <0.6 >
49 Primary Aldosteronism Where Progress is Needed Getting Patients Screened Simplify Confirmatory Testing Secondary Criteria for AVS Other Ways to Identify Who Has Bilateral Disease & Does NOT Need CT & AVS Titrating Medical Therapy Dealing With The Heterogeneity of PA
50 Adrenals Are Life; The Rest is Just Details
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Primary Aldosteronism & Implications for Primary Hypertension
 & Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
& Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens
 Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Adrenal Incidentalomas. Dr A Tabarin University Hospital of Bordeaux (France)
") Adrenal Incidentalomas Dr A Tabarin University Hospital of Bordeaux (France) Adrenal Incidentalomas - Basics Definition : Incidental Discovery Rate of discovery # 4 % over 50 yo Bilateral AI : 10-15 %
Adrenal Incidentalomas Dr A Tabarin University Hospital of Bordeaux (France) Adrenal Incidentalomas - Basics Definition : Incidental Discovery Rate of discovery # 4 % over 50 yo Bilateral AI : 10-15 %
Differential Diagnosis of Cushing s Syndrome
 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Inquadramento Clinico dell IncIdentaloma SurrenalIco
 Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
Cushing s Syndrome. Diagnosis. GuidelineCentral.com. Key Points. Diagnosis
 Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
ADRENAL LESIONS 10/09/2012. Adrenal + lesion. Introduction. Common causes. Anatomy. Financial disclosure. Dr. Boraiah Sreeharsha. Nothing to declare
 ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Nephtali R. Gomez, M.D. To The Incidental Adrenal Mass
 Nephtali R. Gomez, M.D. To The Incidental Adrenal Mass The Complete Idiot s Guide to The Incidental Adrenal Mass Defini:on Any adrenal mass 1cm or more in diameter discovered on a radiologic exam performed
Nephtali R. Gomez, M.D. To The Incidental Adrenal Mass The Complete Idiot s Guide to The Incidental Adrenal Mass Defini:on Any adrenal mass 1cm or more in diameter discovered on a radiologic exam performed
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Clinical Cases of Endocrine Hypertension
 Clinical Cases of Endocrine Hypertension Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan Disclosures
Clinical Cases of Endocrine Hypertension Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan Disclosures
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
ADRENAL DISORDERS Anand Vaidya, MD MMSc
 ADRENAL DISORDERS Anand Vaidya, MD MMSc Director, Center for Adrenal Disorders Division of Endocrinology, Diabetes, & Hypertension Brigham and Women s Hospital Assistant Professor of Medicine, Harvard
ADRENAL DISORDERS Anand Vaidya, MD MMSc Director, Center for Adrenal Disorders Division of Endocrinology, Diabetes, & Hypertension Brigham and Women s Hospital Assistant Professor of Medicine, Harvard
Adrenal Incidentalomas. G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine
 Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas. Dilemmas in Management of Pheochromocytoma and Paraganglioma
 Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas Dilemmas in Management of Pheochromocytoma and Paraganglioma William F. Young, Jr., MD, MSc Mayo Clinic Rochester, MN, USA
Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas Dilemmas in Management of Pheochromocytoma and Paraganglioma William F. Young, Jr., MD, MSc Mayo Clinic Rochester, MN, USA
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
RECURRENT ADRENAL DISEASE. Megan Applewhite Endorama 2/19/2015 SR , SC
 RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules. Celeste Thomas November 1, 2012
 57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
THE WORK-UP OF ADRENAL INCIDENTALOMA
 THE WORK-UP OF ADRENAL INCIDENTALOMA Maria Cristina De Martino Dipartimento di Medicina Clinica e Chirurgia, Sezione di Endocrinologia Università Federico II di Napoli Definition and epidemiology Most
THE WORK-UP OF ADRENAL INCIDENTALOMA Maria Cristina De Martino Dipartimento di Medicina Clinica e Chirurgia, Sezione di Endocrinologia Università Federico II di Napoli Definition and epidemiology Most
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Odise Cenaj, Harvard Medical School Year III. Gillian Lieberman, MD
 February 2012 Radiologic evaluation of adrenal masses and an atypical radiologic presentation of adrenocortical carcinoma in a patient with primary aldosteronism Odise Cenaj, Harvard Medical School Year
February 2012 Radiologic evaluation of adrenal masses and an atypical radiologic presentation of adrenocortical carcinoma in a patient with primary aldosteronism Odise Cenaj, Harvard Medical School Year
Current Management of Adrenal Cortical Carcinoma
 Current Management of Adrenal Cortical Carcinoma American Association of Clinical Endocrinologists Texas Chapter of the AACE Annual Meeting And Texas Endocrine Surgery Symposium August 4, 2017 Jeffrey
Current Management of Adrenal Cortical Carcinoma American Association of Clinical Endocrinologists Texas Chapter of the AACE Annual Meeting And Texas Endocrine Surgery Symposium August 4, 2017 Jeffrey
Transitions For the CAH Patient
 Transitions For the CAH Patient Richard J. Auchus, M.D., Ph.D. Division of Metabolism, Endocrinology & Diabetes Department of Internal Medicine DSD Program University of Michigan Disclosures Contracted
Transitions For the CAH Patient Richard J. Auchus, M.D., Ph.D. Division of Metabolism, Endocrinology & Diabetes Department of Internal Medicine DSD Program University of Michigan Disclosures Contracted
ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain
 ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain OUR APPROACH Incidental adrenal nodule/mass Isaac R Francis, M.B;B.S University of Michigan, Ann Arbor, Michigan Disclosures None (in memory) M Korobkin,
ESUR 2018, Sept. 13 th.-16 th., 2018 Barcelona, Spain OUR APPROACH Incidental adrenal nodule/mass Isaac R Francis, M.B;B.S University of Michigan, Ann Arbor, Michigan Disclosures None (in memory) M Korobkin,
Trust Guideline for the Investigation of Incidental Adrenal Masses in Adults
 A clinical guideline recommended for use For Use in: A&E, Medical Assessment Unit, ITU/HDU Medical and Surgical wards By: Medical, Clinical investigation unit and Surgical staff For: Investigation of incidental
A clinical guideline recommended for use For Use in: A&E, Medical Assessment Unit, ITU/HDU Medical and Surgical wards By: Medical, Clinical investigation unit and Surgical staff For: Investigation of incidental
3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013
 3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013 Presentation Sisters referred by Peds Oncology to Endo clinic for adrenocortical carcinoma screening
3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013 Presentation Sisters referred by Peds Oncology to Endo clinic for adrenocortical carcinoma screening
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Hypertension: Who and How (and Why) to Investigate. Jessica Triay Andy Levy
 to Investigate. Jessica Triay Andy Levy") Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
The Adrenal Glands. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement. II.
 The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
Il Carcinoma Surrenalico
 Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
PHEOCHROMOCYTOMA. Anita Chiu, MD Kings County Hospital Center January 13, 2011
 PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
A short & obese - girl
 A short & obese - girl Presented by :Dr.Amit P Ghawade (DNB Resident-1st Year ) Guide :Dr.S.Ramkumar MD(pediatrics) ICH & HC, Chennai, DM(endocrinology) AIIMS, Delhi Department of Pediatric Endocrinology
A short & obese - girl Presented by :Dr.Amit P Ghawade (DNB Resident-1st Year ) Guide :Dr.S.Ramkumar MD(pediatrics) ICH & HC, Chennai, DM(endocrinology) AIIMS, Delhi Department of Pediatric Endocrinology
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
Physiology. The Hypothalamic Pituitary Adrenal Axis. Elena A Christofides, MD, FACE
 Elena A Christofides, MD, FACE Endocrinology Associates, Inc Endocrinology Research Associates, Inc Physiology 2 The Hypothalamic Adrenal Axis A Complex Set of Feedback Influences* Hypothalamus releases
Elena A Christofides, MD, FACE Endocrinology Associates, Inc Endocrinology Research Associates, Inc Physiology 2 The Hypothalamic Adrenal Axis A Complex Set of Feedback Influences* Hypothalamus releases
14 Girl with Cushing s Disease: An Update. Kristen Dillard, MD Endorama October 17, 2013
 14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School
 Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School May 21st, 2010 56 year old male patient History of hypertension, hyperlipidemia and insulin-resistance 2009:
Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School May 21st, 2010 56 year old male patient History of hypertension, hyperlipidemia and insulin-resistance 2009:
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
ADRENAL INCIDENTALOMAS _ A MANAGEMENT APPROACH Dr Tan Khai Tong
 T H E M E : A S T H M A ARENAL INCIENTALOMAS _ A MANAGEMENT APPROACH r Tan Khai Tong SUMMARY The adrenal incidentaloma is an increasingly common clinical problem. Although most of these masses are innocuous,
T H E M E : A S T H M A ARENAL INCIENTALOMAS _ A MANAGEMENT APPROACH r Tan Khai Tong SUMMARY The adrenal incidentaloma is an increasingly common clinical problem. Although most of these masses are innocuous,
Morbidity & Mortality. Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005
 Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
MedKorat Endocrine Day 2018 Approach to common adrenal disorder
 MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Cushing s syndrome and adrenal insufficiency
 Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
CUSHING S SYNDROME. Chapter 8. Case: A 43-year-old man with delusions
 Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018
 Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting Adenomas
 Case Report Endocrinol Metab 2013;28:133-137 http://dx.doi.org/10.3803/enm.2013.28.2.133 pissn 2093-596X eissn 2093-5978 Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting
Case Report Endocrinol Metab 2013;28:133-137 http://dx.doi.org/10.3803/enm.2013.28.2.133 pissn 2093-596X eissn 2093-5978 Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
A 5-Year Prospective Follow-Up Study of Lipid-Rich Adrenal Incidentalomas: No Tumor Growth or Development of Hormonal Hypersecretion
 Original Article Endocrinol Metab 2015;30:481-487 http://dx.doi.org/10.3803/enm.2015.30.4.481 pissn 2093-596X eissn 2093-5978 A 5-Year Prospective Follow-Up Study of Lipid-Rich Adrenal Incidentalomas:
Original Article Endocrinol Metab 2015;30:481-487 http://dx.doi.org/10.3803/enm.2015.30.4.481 pissn 2093-596X eissn 2093-5978 A 5-Year Prospective Follow-Up Study of Lipid-Rich Adrenal Incidentalomas:
Adrenal venous sampling as used in a patient with primary pigmented nodular adrenocortical disease
 Original Article on Translational Imaging in Cancer Patient Care Adrenal venous sampling as used in a patient with primary pigmented nodular adrenocortical disease Xiaoxin Peng 1, Yintao Yu 1, Yi Ding
Original Article on Translational Imaging in Cancer Patient Care Adrenal venous sampling as used in a patient with primary pigmented nodular adrenocortical disease Xiaoxin Peng 1, Yintao Yu 1, Yi Ding
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
Adrenal Disorders. Disclosure: I do not have any conflicts of interest
 Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal disease Real and Unreal. Objectives. Real
 Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management
 Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management Ohk-Hyun Ryu, MD. Associate Professor, Department of Internal Medicine Division of Endocrinology and Metabolism College of Medicine,
Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management Ohk-Hyun Ryu, MD. Associate Professor, Department of Internal Medicine Division of Endocrinology and Metabolism College of Medicine,
ENDOCRINOLOGY 3. R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice
 Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Case Report Adrenal Lymphangioma Masquerading as a Catecholamine Producing Tumor
 Case Reports in Endocrinology Volume 2015, Article ID 380151, 4 pages http://dx.doi.org/10.1155/2015/380151 Case Report Adrenal Lymphangioma Masquerading as a Catecholamine Producing Tumor Israel Hodish,
Case Reports in Endocrinology Volume 2015, Article ID 380151, 4 pages http://dx.doi.org/10.1155/2015/380151 Case Report Adrenal Lymphangioma Masquerading as a Catecholamine Producing Tumor Israel Hodish,
Incidental adrenal masses A primary care approach
 CLINICAL Incidental adrenal masses A primary care approach Rasha Gendy, Prem Rashid Background The common use of cross-sectional imaging for the investigation of abdominal and thoracic illness has resulted
CLINICAL Incidental adrenal masses A primary care approach Rasha Gendy, Prem Rashid Background The common use of cross-sectional imaging for the investigation of abdominal and thoracic illness has resulted
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW
 CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
AME Position Statement on Adrenal Incidentaloma.
 This is an author version of the contribution published on: Questa è la versione dell autore dell opera: AME Position Statement on Adrenal Incidentaloma. Vol. 164 doi: 10.1530/EJE-10-1147 The definitive
This is an author version of the contribution published on: Questa è la versione dell autore dell opera: AME Position Statement on Adrenal Incidentaloma. Vol. 164 doi: 10.1530/EJE-10-1147 The definitive