MedKorat Endocrine Day 2018 Approach to common adrenal disorder
|
|
|
- Cora Waters
- 5 years ago
- Views:
Transcription



1 MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018
2 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma CAH


3 A 61-year-old man, Pulmonary TB, fatigue Pulse 90/min, regular Thyroid not enlarged Hyperpigmented skin Other : normal
4 Adrenal insufficiency The symptoms and signs of adrenal insufficiency depend upon the rate and extent of loss of adrenal function, whether mineralocorticoid production is preserved, and the degree of stress. The onset of adrenal insufficiency is often very gradual, and it may go undetected until an illness or other stress precipitates adrenal crisis.
5 Causes of adrenal insufficiency Primary adrenal insufficiency Secondary adrenal insufficiency Exogenous steroid prolong used Pituitary disease CIRCI (Critical illness related adrenal insufficiency)

6 Chronic primary adrenal insufficiency

7 Chronic primary adrenal insufficiency
8 Laboratory tests Morning serum cortisol 1 mcg ACTH stimulation test 0 (before bolus), 20, 40 minutes for serum cortisol Insulin-induced hypoglycemia test *Step 1 : Test for diagnosis (screening test then confirmation test) *Step 2 : localization (hormonal test) *Step 3 : Imaging Most rational test of hypothalamic-pituitary-adrenal response to stress Test is safe, if a clinician is present, in patients with no history of seizures or cardiovascular or cerebrovascular disease Insulin (usually at a dose of 0.15 units/kg; in patients with low basal cortisol levels, the dose should be reduced to 0.1 units/kg) is given with the aim to achieve hypoglycemia < 35 mg/dl Cortisol concentrations are measured at 0, 30, and 45 minutes, even if glucose has been given to reduce symptoms of hypoglycemia.
9 Serum morning cortisol < 3 mcg/dl 3-18 mcg/dl > 18 mcg/dl Dynamic test - 1 mcg ACTH stimulation test - Insulin induced hypoglycemia test Exclude adrenal insufficiency Adrenal insufficiency < 18 mcg/dl > 18 mcg/dl Morning serum ACTH level High Low or within normal limit CT adrenal gland MRI pituitary gland


10 Causes of primary adrenal insufficiency

11 Treatment of chronic primary adrenal insufficiency

12 Treatment of chronic primary adrenal insufficiency
13 A 61-year-old woman, no underlying disease, UTI sepsis BP 80/40 mmhg, pulse 120/min Dry lips, dry tongue Adequate hydration, empiric ATB, moderate dose of vasopressure >>> cannot maintain BP Cortisol at severe sepsis : 9 mcg/dl
14 Glucocorticoid therapy in septic shock Laboratory assays of plasma cortisol concentration and response to adrenocorticotropic hormone (ACTH) stimulation are likely unreliable in critically ill patients. Guidelines support use of a change in baseline cortisol at 60 min of <9 mcg/dl after cosyntropin (250 mcg) administration a random plasma cortisol of <10 mcg/dl Severe septic shock : SBP <90 mmhg for > 1 hour despite adequate fluid resuscitation and moderate to high dose of vasopressor administration UptoDate2018 Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017
15 Glucocorticoid therapy in septic shock Most patients with septic shock, suggest not routinely using intravenous glucocorticoid therapy as initial treatment When the decision is made to use glucocorticoid therapy, we suggest hydrocortisone alone (<400 mg per day in divided doses) Adverse effects : hypernatremia, hyperglycemia, and neuromuscular weakness. The risk of superinfection does not appear to be consistently elevated among studies. Typically administer hydrocortisone for at least 3 days (typically for 5-7 days) and taper the dose as guided by the clinical response. UptoDate2018 Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017
16 A 61-year-old woman, no underlying disease, UTI sepsis BP 80/40 mmhg, pulse 120/min Dry lips, dry tongue Adequate hydration, empiric ATB, moderate dose of vasopressure >>> cannot maintain BP Cortisol at severe sepsis : 9 mcg/dl Hydrocortisone 100 mg IV q 8 hours


17 Virilization Ambiguous genitalia
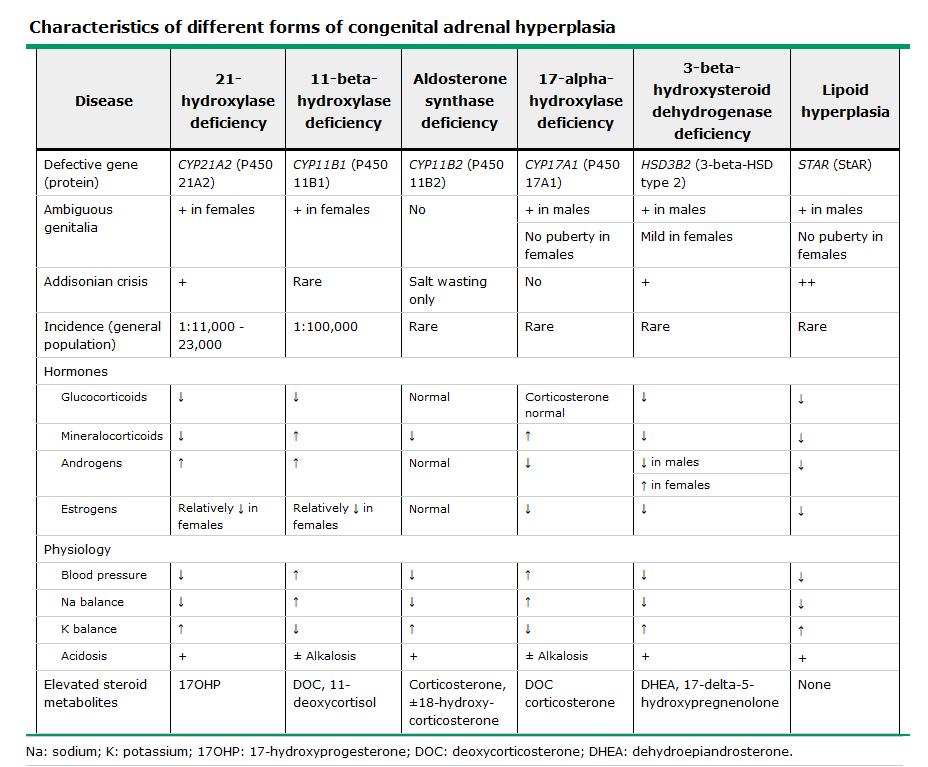
18 Congenital adrenal hyperplasia Inherited defects in the enzymatic steps of cortisol biosynthesis Primary adrenal insufficiency, as they impair cortisol synthesis Clinical manifestations are related to 1 processes: Impaired synthesis of cortisol Impaired synthesis of aldosterone Excessive synthesis of precursor steroids because of the increase in ACTH secretion, which leads to oversecretion of steroids whose production does not require the deficient enzyme. Excessive androgenic hormones, which cause virilization Excessive synthesis of mineralocorticoids such as deoxycorticosterone, which can cause hypertension.
19 Cortisol biosynthesis (steroidogenesis)
20 Copyrights apply
21 21-hydroxylase deficiency

22 17-hydroxylase deficiency
23 11-hydroxylase deficiency
24 A 61-year-old woman, Underlying HT, proximal muscle weakness BP 160/100 mmhg, Pulse 80/min, regular Proximal muscle weakness grade 3 Serum K = 2.3 mmol/l
25 Secondary Hypertension Endocrine hypertension Mineralocorticoid hypertension Pheochromocytoma Cushing s syndrome, Acromegaly, Thyroid diseases Renal disease Renovascular hypertension Renal parenchymal disease Other : NSAIDs, oral contraceptive drug, Sleep apnea
26 History suggest Secondary HT Age < 30 years in nonobese, negative family history of hypertension and no other risk factors (eg, obesity) for hypertension. Very strong family hx severe HT, renal disease Abrupt onset of HT Sudden acceleration of previous existing HT Rapid deterioration of renal function or after tx with ACEI Unresponse of standard anti HT Rapid hypo K after tx with standard dose diuretic Hx renal trauma, flank pain, hematuria suggest renal infarct Sudden onset HT with systemic emboli or emboli or infarction Periodic paralysis or muscle weakness Headache, palpitation, sweating Refractory HT = on anti HT moderate dose 3 with diuretic drug
27 Physical examination Malignant HT grade III or IV retinopathy Occlusive vascular disease : pulseless, bruit AAA Radiofemoral pulse disparity Sign of Cushing Interscapular murmur Muscle wasting Postural hypotension with or without reflex tachycardia Wide swing in BP Abdominal or flank mass Polycystic kidney Tremor, wt loss Hyperthyroidism Sign of pheochromocytoma
28 Lab evaluation CBC UA Serum BUN, Cr, uric, Electrolyte FBS Lipid EKG
29 Hypokalemia Pseudohypo K Transcellular K shift -Periodic hypo K paralysis -B12 Rx pernicious anemia K loss ( True K deficiency ) 24 hr urine K Extrarenal loss Urine K < 20 meq/l Renal loss Urine K > 20 meq/l
30 Renal K loss High BP Normal BP High plasma renin Low plasma renin Low HCO 3 - High HCO 3 - Malignant HT Renovascular dz. Renin tumor Aldosterone High -Hyperaldosteronism -Bilateral hyperplasia RTA < 10 meq/l Vomiting Urine Cl Low Mineralocorticoid ingestion CAH Cushing syndrome >10 meq/l Batter syndrome Diuretic Mg def.
31 Primary aldosteronism Patient groups with high prevalence of primary aldosteronism Moderate/ severe HT : SBP > 160, DBP > 100 (JNC7) Resistant HT : SBP >140, DBP > 90 despite treatment with 3 hypertensive medication HT with spontaneous or diuretic induced PA is hypo K HT with adrenal incidentaloma J Clin Endocrinol Metab 93: , 2008
32 Primary aldosteronism Subtype prevalence (%) Aldosterone producing adenoma (APA) 65 Idiopathic hyperaldosteronism (IHA) 34 Aldosterone producing carcinoma < 1 Primary adrenal hyperplasia (PAH) < 1 Glucocorticoid-remediable aldosteronism (GRA) < 1 J Clin Endocrinol Metab 93: , 2008
33 Primary Aldosteronism (PA) Step 1 PRA (Plasma renin activity).. ng/ml/h PAC (Plasma aldosterone conc.) > 15 ng/dl ARR (Aldosterone-renin ratio) > J Clin Endocrinol Metab 93: , 2008
34 Protocol The test is performed by measuring a morning (preferably 8 AM), ambulatory. Random PAC and PRA Correct hypo K Normal sodium intake Withdraw agents that markedly affect the ARR for at least 4 weeks: A. Spironolactone, epherenone, amiloride, and triamterene B. Potassium-washing diuretics C. Products derived from liquorice root J Clin Endocrinol Metab 93: , 2008
35 Protocol If the results of ARR off above the agents are not diagnosis, withdraw other medications that may affect the ARR for at least 2 weeks : A. Beta blocker, clonidine, alpha-methyldopa, NSAIDs B. ACEI, ARB, renin inhibitors, dihydropyridine CCB Medications that have minimal effects on ARR Verapamil SR, Hydralazine, Prazosin, Doxazosin J Clin Endocrinol Metab 93: , 2008
36 HT with HypoK Correct K TTKG Avoid antiht : ACEI, ARB, ß blk, diuretic, CCB Normal Na intake PAC ng/dl PRA ng/ml/hr PAC PRA PAC PRA PAC/PRA & PAC 15 -CAH -11ßHSD def. -Exogenous mineralocorticoid -Cushing s syndrome -Liddle syndrome -Essential HT PAC PRA 2 Hyperaldosteronism
37 Primary Aldosteronism (PA) Step 1 PRA (Plasma renin activity).. ng/ml/h PAC (Plasma aldosterone conc.) > 15 ng/dl ARR (Aldosterone-renin ratio) > Step 2 Confirmation test : Saline infusion of 2 liters over 4 hours Post-infusion Plasma aldosterone level < 5 ng/dl...unlikely PA Plasma aldosterone level > 10 ng/dl...very probably sign of PA Step 3 Adrenal CT J Clin Endocrinol Metab 93: , 2008
38 Adrenal venous sampling (AVS) Lateralization of excessive aldosterone secretion Sensitivity 95% and specificity 100% Infusion cosyntropin (ACTH) 50 µg/hr before 30 min and continuous during AVS Correct blood : aldosterone, cortisol (both adrenal vein, IVC below renal vein)

 Higher side : Lower side ratio >")
39 Cortisol gradient (Adrenal vein : IVC) > 5:1 No Not cannulate to adrenal vein Yes Cortisol-corrected aldosterone = PAC (ng/dl)/ cortisol (mcg/dl) Higher side : Lower side ratio > 4 APA 3-4 Overlap < 3 IHA
40 Medical treatment Spironolactone : IHA Start: mg/d max 400 mg/d serum K response promptly but HT response ~ 4-8 weeks Side effect : painful gynecomastia, erectile dysfunction, decrease libido, menstrual irregularity
41 Surgical treatment APA, PAH Laparoscopic adrenalectomy F/U : PAC postop day 1-2 F/U : K q 1 week x 4 BP normalized in 1-3 month after Surgery
42 Cushing s syndrome (CS) ACTH dependent Pituitary adenoma >> Cushing s disease Ectopic ACTH ACTH independent Adrenal tumor Ectopic ACTH รถ = Carcinoid tumor Pan = Pancreatic tumor ค นเล ก = Small cell lung CA หมอเมด = Medullary CA thyroid ให ฟร = Pheochromocytoma

43 Who should be tested? Suggest testing for hypercortisolism in patients in whom a diagnosis is most likely, including the following : Osteoporosis or HT in young adults Multiple progressive features of Cushing's syndrome (CS), particularly those that are predictive of CS such as facial plethora, proximal myopathy, striae (>1 cm wide and red/purple), and easy bruising Unexplained severe features (resistant HT, osteoporosis) at any age Adrenal incidentalomas Exclude exogenous glucocorticoids Before evaluation for possible CS, it has excluded exogenous glucocorticoid intake

44 Signs and symptoms of Cushing's syndrome More common Less common
45 Examples of conditions associated with physiologic hypercortisolism that may have some clinical features of CS : Pregnancy Patients with severe obesity, especially those with visceral obesity or PCOS Patients with psychological stress, especially patients with a severe major depressive disorder and melancholic symptoms Poorly controlled diabetes mellitus Rarely, chronic alcoholism Examples of conditions associated with physiologic hypercortisolism that are unlikely to have clinical features of CS : Physical stress (illness, hospitalization/surgery, pain) Malnutrition, anorexia nervosa Intense chronic exercise Hypothalamic amenorrhea High corticosteroid-binding globulin (CBG) (increased serum cortisol but not UFC) Glucocorticoid resistance Pseudo Cushing s
46
47 Initial testing Any one of Urine free cortisol x 2d Subsequence testing Any other one or two of the rest Urine free cortisol x 2d Late night salivary cortisol x 2d Late night salivary cortisol x 2d 1 mg overnight DST 1 mg overnight DST Standard low dose DST Standard low dose DST LDDST CRH test Midnight serum cortisol
48 DDx of Cushing s syndrome ACTH < 5 pg/ml ACTH > 20 pg/ml ACTH independent CS ACTH dependent CS CT adrenal gland -equivocal or negative MRI -clinical suspicious of ectopic ACTH Plasma ACTH 5-20 pg/ml : less definitive!! -But usually indicate that cortisol secretion is ACTH-dependent. -For these patients, a CRH stimulation test may be helpful BIPSS Ectopic ACTH syndrome Chest & Abdominal imaging Pituitary Adenoma
49 Pheochromocytoma Catecholamine-producing neuroendocrine tumours from chromaffin cells of adrenal medulla or extraadrenal paraganglia. Paraganglioma : extra-adrenal pheochromocytomas and tumors from parasympathetic tissue Lancet 2005; 366:
50 Pheochromocytoma 80-85% of pheochromocytomas arise from adrenal medulla 15-20% are from extra-adrenal chromaffin Catecholamine-producing extra-adrenal paragangliomas usually found in abdomen Tumors from parasympathetic tissue in H&N, most not produce catecholamines Lancet 2005; 366:
51 Hereditary Pheochromocytoma Multiple endocrine neoplasia type 2 Von Hippel-Lindau syndrome Neurofibromatosis type 1 Familial paragangliomas Hereditary forms most often before age 40 years Lancet 2005; 366:


52

53 Lancet 2005; 366:
54 Biochemistry testing Urinary and plasma catecholamines, Urinary metanephrines (normetanephrine and metanephrine) Urinary vanillylmandelic acid (VMA) Plasma-free metanephrines (normetanephrine and metanephrine)

55 Lancet 2005; 366:

56 Interference with measurements of cathecholamine Lancet 2005; 366:
57
58 Imaging procedures CT ± contrast or MRI abdomen include pelvis 123 I-metaiodobenzylguanidine (MIBG) PET Lancet 2005; 366:
59 Preoperative management α-adrenoceptors with phenoxybenzamine, prazosin, doxazosin, or urapidil eg. Doxazosin is given in increasing doses from 1 to 16 mg once a day ß-adrenoceptor blocker **after α-blocker eg. propranolol 40 mg three times daily or atenolol mg once daily Calcium-channel blockers Treatment usually lasts for days Lancet 2005; 366:
60 Adequate preoperative preparation Several criteria have been proposed BP below 160/90 mmhg for at least 24 h Orthostatic hypotension should be present, but BP in the upright position should not fall below 80/45 mmhg Lancet 2005; 366:
61 Postoperative hypotension Treatment consists of fluid replacement and occasionally intravenous ephedrine. If ephedrine infusion is ineffective, vasopressin might be used. Risk of hypoglycaemia is related to rebound hyperinsulinaemia due to recovery of insulin release after tumour removal Lancet 2005; 366:
62 Surgical treatment Laparoscopic removal of intra-adrenal and extra-adrenal phaeochromocytomas is now the preferred surgery Lancet 2005; 366:
63 Adrenal incidentaloma Prevalence is higher in older, obese, DM, and hypertensive patients Functional? Malignancy? Bilateral masses : -Metastatic disease -Congenital adrenal hyperplasia -Lymphoma -ACTH-dependent Cushing s -Primary aldosteronism -Infiltrative disease of adrenal glands -Infection (eg, tuberculosis, fungal) -Cortical adenomas -Hemorrhage -Pheochromocytoma -Amyloidosis -Bilateral macronodular adrenal hyperplasia (BMAH)

64 Adrenal incidentaloma Functional testing Pheochromocytoma Cushing s syndrome Primary aldosteronism : only in HT
65 EVALUATION FOR MALIGNANCY Size Adrenocortical carcinomas were significantly associated with mass size 90 % being more than 4 cm in diameter when discovered Imaging phenotype : CT, MRI
66 Imaging phenotype (CT, MRI) Benign adenoma Round and homogeneous density, smooth contour and sharp margination Diameter < 4 cm, unilateral Low unenhanced CT attenuation values (<10 HU) Rapid contrast medium washout (10 minutes after contrast, an absolute contrast medium washout of > 50 %) Isointensity with liver on both T1 & T2 weighted MRI sequences Chemical shift evidence of lipid on MRI Pheochromocytomas Increased attenuation on nonenhanced CT (>20 HU) Increased mass vascularity Delay in contrast medium washout (10 minutes after contrast, an absolute contrast medium washout of < 50 %) High signal intensity on T2 weighted MRI Cystic and hemorrhagic changes Variable size and may be bilateral
67 FOLLOW-UP For incidentalomas with a benign appearance on imaging, repeat imaging after 6 to 12 months should be performed to reevaluate for possible malignancy
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Hypertension: Who and How (and Why) to Investigate. Jessica Triay Andy Levy
 to Investigate. Jessica Triay Andy Levy") Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
The Adrenal Glands. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement. II.
 The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
Cushing s Syndrome. Diagnosis. GuidelineCentral.com. Key Points. Diagnosis
 Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
ظظظ/ Omar Sami. Hussam Twaissi. Mousa Abbadi
 ظظظ/ 5 Omar Sami Hussam Twaissi Mousa Abbadi The doctor started this lecture by revising what we have taken in lecture number four, I won t re-write these stuff as it becomes boring so often. This sheet
ظظظ/ 5 Omar Sami Hussam Twaissi Mousa Abbadi The doctor started this lecture by revising what we have taken in lecture number four, I won t re-write these stuff as it becomes boring so often. This sheet
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Endocrine Emergencies: Recognition and Management
 Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Adrenal Disorders. Disclosure: I do not have any conflicts of interest
 Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Gland Disorders
 1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to
 Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
4/23/2015. Objectives DISCLOSURES
 2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
Pathophysiology of Adrenal Disorders
 Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
ADRENAL LESIONS 10/09/2012. Adrenal + lesion. Introduction. Common causes. Anatomy. Financial disclosure. Dr. Boraiah Sreeharsha. Nothing to declare
 ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Adrenal Insufficiency
 Adrenal Insufficiency Normal adrenal physiology Clinical features, Laboratory findings Common causes of primary adrenal insufficiency Evaluation of suspected adrenal insufficiency Acute and chronic management
Adrenal Insufficiency Normal adrenal physiology Clinical features, Laboratory findings Common causes of primary adrenal insufficiency Evaluation of suspected adrenal insufficiency Acute and chronic management
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
Southern Derbyshire Shared Care Pathology Guidelines. Secondary Hypertension
 Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess
 The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
PHEOCHROMOCYTOMA. Anita Chiu, MD Kings County Hospital Center January 13, 2011
 PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
CUSHING S SYNDROME. Chapter 8. Case: A 43-year-old man with delusions
 Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
ENDOCRINOLOGY 3. R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice
 Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
Adrenal disease Real and Unreal. Objectives. Real
 Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School
 Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School May 21st, 2010 56 year old male patient History of hypertension, hyperlipidemia and insulin-resistance 2009:
Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School May 21st, 2010 56 year old male patient History of hypertension, hyperlipidemia and insulin-resistance 2009:
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Karim Said. 41 year old farmer. Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy
 Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
ADRENAL GLANDS. G M Kellerman. Hunter Area Pathology Service
 ADRENAL GLANDS G M Kellerman Hunter Area Pathology Service ADRENAL FUNCTIONS THE ADRENAL GLANDS ACTUALLY HAVE 4 QUITE SEPARATE FUNCTIONS 1. MINERALOCORTICOID SECRETION BY THE ZONA GLOMERULOSA OF THE CORTEX
ADRENAL GLANDS G M Kellerman Hunter Area Pathology Service ADRENAL FUNCTIONS THE ADRENAL GLANDS ACTUALLY HAVE 4 QUITE SEPARATE FUNCTIONS 1. MINERALOCORTICOID SECRETION BY THE ZONA GLOMERULOSA OF THE CORTEX
Read the following article and answer the questions that follow. Refer to the Keys section to check your answers.
 ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
9/11/2012. Chapter 11. Learning Objectives. Learning Objectives. Endocrine Emergencies. Differentiate type 1 and type 2 diabetes
 Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Adrenal and retropetionium
 Adrenal and retropetionium Disorders of the Adrenal Cortex Hyperaldosteronism: Hyperaldosteronism may be secondary to stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow
Adrenal and retropetionium Disorders of the Adrenal Cortex Hyperaldosteronism: Hyperaldosteronism may be secondary to stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Adrenocortical Insufficiency: Addison's Disease
 280 PHYSIOLOGY CASES AND PROBLEMS Case 49 Adrenocortical Insufficiency: Addison's Disease Susan Oglesby is a 41-year-old divorced mother of two teenagers. She has always been in excellent health. She recently
280 PHYSIOLOGY CASES AND PROBLEMS Case 49 Adrenocortical Insufficiency: Addison's Disease Susan Oglesby is a 41-year-old divorced mother of two teenagers. She has always been in excellent health. She recently
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
PROBLEMS WITH REGULATION AND METABOLISM. Objectives A & P 8/11/2011
 PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT?
 ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Secondary hypertension How to approach?
 Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
ENDOCRINE FORMS OF HYPERTENSION. Michael Stowasser
 ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
Inquadramento Clinico dell IncIdentaloma SurrenalIco
 Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
Management of adrenal incidentalomas
 31 Management of adrenal incidentalomas KEVIN MURTAGH, NANA MUHAMMAD AND MAREK MILLER The return of a scan result with reference to an incidental finding of an adrenal mass is a common scenario. 1 The
31 Management of adrenal incidentalomas KEVIN MURTAGH, NANA MUHAMMAD AND MAREK MILLER The return of a scan result with reference to an incidental finding of an adrenal mass is a common scenario. 1 The
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of