An Organized Approach to the Patient with Papilledema and IIH
|
|
|
- Susanna Benson
- 5 years ago
- Views:
Transcription
1 An Organized Approach to the Patient with Papilledema and IIH Leonard V. Messner, OD, FAAO James L. Fanelli, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is prohibited. 1
2 Disclosures There are no disclosures to be made that affect the content of this presentation 2
3 Please remember to complete your session evaluations online. 3
4 Papilledema - Key Points Papilledema vs Pseudopapilledema Pathogenesis of papilledema Staging of papilledema Causes of papilledema 4
5 Papilledema Definition: Optic disc edema and elevation owing to elevated intracranial pressure Differentiated from Disc Edema Swelling of the optic disc of unknown etiology 5
6 SAS, ICP, and CSF CSF flows in SAS ON sheath houses ON and SAS Extends to the Lamina Increased ICP Orbital portion ON compressed Compression transmitted forward to the lamina Tourniquet like compression Axonal transport blocked at lamina 6

7 SAS, ICP and CSF 7

8 SAS, ICP and CSF 8
9 Pathogenesis - Neurogenic Elevated ICP Axoplasmic stasis & arrest (lamina cribrosa) Intra axonal edema/cytotoxic edema Leakage of axoplasmic fluid (extracellular edema) Increased extra-axonal osmolarity (extracellular edema) 9


10 Disc and Edema Intra and extracellular swelling Microtubule distortion 10
11 Pathogenesis Tumors/space occupying lesions IIH Increased CSF production Decreased CSF resorption DVST, inflammation, meningitis, SAH Dural venous sinus obstruction Cerebral edema Medications 11
12 Pathogenesis - Vasogenic Obstructed venous outflow Capillary dilation & leakage Capillary nonperfusion / ischemia 12

13 13

14 Histologic Edema: 2 Sources Cytotoxic edema Intracellular edema secondary to Direct cellular injury Vasogenic edema Extracellular edema secondary to Vessel leakage 14

 TVO")
15 Clinical Features - Ocular Bilateral Symmetric Transient diplopia (CN VI) TVO s (+/-) 15
16 Clinical Features - Ocular Vision preservation early in disease process (As opposed to other causes of optic nerve edema) Develops over hours to weeks Progressive deterioration of visual fields Visual recovery is related to management of underlying causes 16
17 Visual Loss VF VA Early Developed Chronic Atrophic 17
18 Clinical Features - Non-ocular Headaches (upon awakening & head movement, cough, Valsalva) Pulsatile intracranial noises Seizure Emesis (+/- nausea) Neurologic dysfunction 18

19 Ocular Signs Blurring of disc margins Elevation of disc Obscuration of the cup Edema of the peripapillary RNFL Retinal and choroidal folds Hyperemic discs Vascular congestion Hemorrhages, exudates and infarcts 19
20 Differentiating Papilledema Optic disc edema secondary to increased intracranial pressure PseudoPapilledema Optic disc edema not related to increased ICP 20
21 Disc Edema NOT ICP Related Ischemic Optic Neuropathies AION NAION Disc Drusen Optic Neuritis Vascular Etiologies Diabetic disc edema C/BRVO Hypertensive disc edema Unilateral disc edema 21
22 Pseudopapilledema- Ophthalmoscopy Venous pulsations + Absence of physiological cupping Vascular anomalies No NFL exudates No NFL infarcts 22



23 Disc Edema-NO ICP elevation VOs Tilted disc ION PPCNVM Drusen 23

24 78 Y/O White Male AMD yearly visit No complaints 20/30 OD, OS, OU 24

25 78 Y/O White Male 25



26 Disc Drusen May be seen on fundoscopy Buried drusen not visible 26


27 52 Y/O Caucasian Pediatrician No complaints 20/20 OD, OS, OU 27
28 Pseudopapilledema-OCT Findings Elevation of the optic nerve head with.. Minimal increase in RNFL thickness Minimal central cup Increased reflectance of hyaline Shadowing near hyaline Separation of deeper retina from RPE Neutral/Negative RPE and BM deflection 28


29 Disc Drusen-OCT findings Elevation Normal RNFL No/minimal cup Increased reflectance Shadowing Separation of outer retina 29


30 Disc Drusen- Shadowing & Separation of Outer Retinal Layers 30


31 Pseudopapilledema-OCT Findings Neutral/Negative RPE and BM deflection 31

32 OCT Findings- Papilledema 32

33 Forward Bowing of RPE/BM 33

34 14 Y/O New Patient Headaches worsening 20/20 20/


35 14 Y/O NP 35
36 36

37 37

38 38

39 39
40 Stages of Papilledema Jackson Hoyt & Beeston Frisen
41 Early (Grade 1-2) Mild disc elevation Halo of edema - early temporal sparing Circumpapillary retino-choroidal folds (Paton s lines) Loss of SVP 41

42 C-Shaped Edema 42

43 C-Shaped Edema 43
44 42 y/o woman c/o headaches VA = 20/20 OD, 20/20 OS 62 inches tall 260 pounds 44

45 45

46 46


47 Developed (Grade 3-4) Marked disc elevation & hyperemic edema Obscuration of major vessels - halo expansion- around to on disc Microvascular disruption capillary telangiectasis collaterals infarcts hemorrhage Grade 3 Grade 4 47

48 48
49 49

50 Chronic (Grade 5) Marked dome-shaped disc elevation ( champagne cork ) Resolution of hemorrhage & infarcts Less hyperemia, more pallor Obscuration of vessels Obliteration of optic cup Refractile bodies 50

51 51

52 52
53 Refractile Bodies Seen fundoscopically Represent lipid exudates from chronic microvascular leakage 53

54 54

55 Frisen Staging Summary 55
56 Atrophic (Post-Papilledema Optic Atrophy) Flattening of disc Resolution of edema Residual collaterals Generalized disc pallor 56

57 Sometimes Bad Outcome 57
58 Other Times Good Outcome Longterm 58
59 Causes of Papilledema Intracranial mass Structural abnormality / Hydrocephalus Vascular (e.g. CVT, AVM) Iatrogenic Idiopathic intracranial hypertension Corbett JJ
60 15 Y/O Female Headaches Recent increase HA x 2 months Blurred vision, difficulty focusing Waxing and waning? Tinnitus 20/25 20/25- ERRLA APD Neuroimaging and biopsy: Astrocytoma 60

61
62 62
63 1 month post surgery 63
64 64

65 August
66 66
67 67
68 68
69 Causes of Papilledema Intracranial mass Structural abnormality / Hydrocephalus Vascular (e.g. CVT, AVM) Iatrogenic Idiopathic intracranial hypertension Corbett JJ
70 17 y/o AA Male Six week hx of vision loss, OS > OD Worse at near than distance Previous spectacle Rx (not sure of last exam) Occasional stress headaches Increasing problems with dizziness passed out one year earlier while getting off bus 70
71 Neuro-ophthalmic Examination BCVA: 20/200 OD 20/400 OS Sluggish pupils OU (? LAPD) Downbeat nystagmus (greater down left & down right) Visual fields: Bitemporal hemianopia denser below than above 71


72 72
73 73

74 74

75 75

76 76
77 Hydrocephalus and kids shunts Shunt failure 77

78 Sometime, big things come in small packages 78
79 35 y/o Woman c/o headaches VA = 20/20, OU 79


80 80

81 81

82 Sagital Sinus Obstruction 82


83 CSF Production and Drainage CSF produced from arterial blood in the choroidal plexus in lateral and 4 th ventricles Exits 4 th ventricles Into SAS 83

84 84


85 T1 Weighted T2 Weighted 85



86 CSF Production and Drainage CSF is absorbed into the dural venous sinuses by the arachnoid villi 86
87 CSF Production and Drainage About 650 cc of CSF is produced per day Normal CSF pressure mm H2O (8-15 mmhg) Normal CSF pressure is LOW Normal Dural Venous sinus pressure is LOWER! Therefore, anything that impedes dural venous sinus drainage will result in impaired CSF drainage 87

 88")
88 Dural Venous Sinus Thrombosis Imaging: MRV/CTV International Study of Cerebral Venous and Dural Venous Sinus Thrombosis (ISCVT) 88
89 Papilledema - Key Points Neuroimaging studies for neuro-ophthalmic disorders Pathogenesis of papilledema Papilledema vs Pseudopapilledema Staging of papilledema Causes of papilledema 89
90 Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) 90
91 IIH - Key Points Defining pseudotumor cerebri & IIH Pathogenesis of IIH Clinical features and neuroradiology Prognostic factors and management OCT analysis of papilledema Visual fields! 91
92 34 y/o Woman VA = 20/20, OU + HA x 2 yrs. Normal neuro exam BMI: 39 92
93 93
94 Pseudotumor Cerebri & Idiopathic Intracranial Hypertension 94
95 Pseudotumor Cerebri elevated ICP no mass No known cause Identifiable cause Idiopathic Intracranial Hypertension Iatrogenic Hypervitaminotosis Inflammatory Venous sinus thrombosis 95

96 Dandy WE Ann Surg

97 Smith JL J Clin Neuro-ophthalmol
98 Dandy Criteria for IIH (Modified) Signs & symptoms of elevated ICP (e.g. papilledema, headaches) No localizing neurologic signs (except CN VI paresis) ICP >250 mm H2O (normal CSF) No evidence of mass/structural lesion on MRI Empty sella No ventriculomegaly No secondary cause of elevated ICP Smith JL. J Clin Neuro-ophthalmol

99 Revised Diagnostic Criteria for the Pseudotumor Cerebri Syndrome in Adults and Children Wall M, et al. Neurology
100 Neuroradiology Findings with IIH Empty sella Posterior scleral flattening Optic nerve distension Ectopic displacement of cerebellar tonsils Dural venous sinus stenosis 100
101 Neuroradiology Findings with IIH Empty sella Posterior scleral flattening Optic nerve distension Ectopic displacement of cerebellar tonsils Dural venous sinus stenosis 101
102 102
103 Neuroradiology Findings with IIH Empty sella Posterior scleral flattening Optic nerve distension Ectopic displacement of cerebellar tonsils Dural venous sinus stenosis 103
104 104
105 Neuroradiology Findings with IIH Empty sella Posterior scleral flattening Optic nerve distension Ectopic displacement of cerebellar tonsils Dural venous sinus stenosis Aiken AH, et al. Am J Neuroradiol
106 106
107 Neuroradiology Findings with IIH Empty sella Posterior scleral flattening Optic nerve distension Ectopic displacement of cerebellar tonsils Dural venous sinus stenosis Farb RI, et al. Neurology
108 28 y/o AA Woman c/o moderate, progressive headaches x 1 month Normal neurologic exam BVA: 20/20 OD 20/20 OS BMI:

109 109

110 110

111 111
112 112
113 113
114 114
115 115
116 27 y/o AA Woman c/o moderate, progressive headaches x 1-2 month Normal neurologic exam BVA: 20/20 OD 20/20 OS BMI:

117 117
118 118

119 119

120 120
121 Epidemiology of IIH % female 15 to 44 years Obesity MAI = /100, /100,000 if obese female yrs. Giuseffi V, et al. Neurology 1991 Ireland B, et al. Arch Neurol 1990 Radhakrishnan K. et al. Arch Neurol
122 Pathogenesis of IIH (???) Increased cerebral blood volume - Raichle 1978 Increased arachnoid resistance to CSF drainage - Aisenberg 1980 Increased intra-abdominal pressure with cerebral venous hypertension - Sugerman 2001 Reduced CSF absorption by extracranial lymphatics Johnston
123 Baseline Clinical Profile (IIHTT) Headache (84%) Back pain (53%) Tinnitus (52%) Vision loss Transient vision loss (68%) Symptomatic vision loss (32%) Visual fields (86% {5% > 15db}) Enlarged blind spot Inferior arcuate defects Wall M JAMA Neurol


124 The rest of the story 20/20 20/20 124

125 -2.54 db db 125

126 12 mos later db db 126


127 19 mos later 20/20 20/30 127
128 19 mos later HVF db db 128
129 Risk Factors for Poor Visual Prognosis Male gender African American Morbid obesity Marked weight gain Obstructive sleep apnea Concomitant medications Acute onset of signs and symptoms of elevated ICP (fulminant IIH) High-grade papilledema Lack of headaches Lack of ophthalmic oversight Biousse V. NANOS
130 Gender Men represent approx 10% of all IIH Less likely to have headache ( estrogen factor ) Less likely to seek care Digre & Corbett Arch Neurol 1989 Bruce BB, et al. Neurology
131 Race No strong influence on development of IIH African Americans = more aggressive disease: 3X more likely to have severe vision loss 5X more likely to develop blindness Bruce BB, et al. Neurology
132 Obesity NORDIC ave. BMI = 39 Increased severity of papilledema and visual loss if BMI 40 Recent weight gain (5-15%) even in non-obese patients Szewka AJ, et al. J Neuroophthalmol 2013 Wall & George. Brain
133 Medications Many meds proposed to induce IIH, few testretest data Tetracycline derivatives (minocycline) cyclosporine, lithium, nalidixic acid, nitrofurantoin, oral contraceptives, levonorgestrel, danaxol, and tamoxifen Friedman DI. Am J Clin Dermatol 2005 Fraser CL, et al. Arch Neurol
134 14 y/o Girl HAs x 2-3 weeks Rx minocycline x 1 month for acne VA: 20/20 OU BMI:

135 135

136 136

137 137
138 138
139 MRI / MRV normal D/C minocycline Follow-up x 3 weeks 139

140 Reduction in RNFL: 32 microns OD 142 microns OS 140

141 By 4 mos: Reduction in RNFL: 109 microns OD 196 microns OS 141
142 Co-Morbidities Anemia Hypertension Obstructive sleep apnea Biousse V, et al. Am J Ophthalmol 2003 Wall M. Neurol Clin
143 Pregnancy Independent of weight gain, not a risk factor for IIH Beware of cerebral venous sinus thrombosis (end of pregnancy & post partum period) Biousse V, et al. Neurology
144 35 y/o woman c/o progressive & severe HA s, emesis & nausea 2 weeks post partum VA = 20/20, OD & OS 144


145 145

146 146
147 Clinical Findings Predictive of Poor Outcomes Absence of headaches Severity of papilledema (+/-) Marked visual field defects at presentation Fulminant course (malignant IIH) Biousse V. NANOS
148 Management of IIH Observation CAI s / diuretics? value Surgery VP shunt ONSF Weight loss 5-10% BMI Visual Fields 148

149 149
 (The IIH Pilot Trial) UK prospective study 50 IIH patients: ½ Rx acetazolamide ½ observation All patients")
150 Acetazolamide for IIH (?) (The IIH Pilot Trial) UK prospective study 50 IIH patients: ½ Rx acetazolamide ½ observation All patients advised to lose weight No benefit to acetazolamide (12 mos.) Matthews T, et al. NANOS
 To identify proteomic and genetic risk factors for IIH by screening a large cohort of IIH patients and controls.")
151 NORDIC IIH Treatment Trial Specific Aim 1: The trial is focused on determining the efficacy of low sodium diet with or without acetazolamide to reduce or reverse visual loss. Specific Aim 2: (a) To identify proteomic and genetic risk factors for IIH by screening a large cohort of IIH patients and controls. 151
152 Mild IIH 152
153 IIHTT 6-Month Results Acetazolamide better than diet alone for visual field improvement (PMD reduction of 1.43 vs db) Acetazolamide arm showed better weight reduction than diet alone Acetazolamide arm showed better resolution of papilledema & improvement of QOL scores vs. diet alone Wall M, et al. JAMA Neurol
154 25 y/o AA Woman c/o progressive vision loss OU h/o recurrent headaches (am > pm) BVA: 20/30 OD 20/40 OS 154

155 155
156 156

157 157

158 158

159 159

160 160
161 38 y/o AA Woman Medical history = SLE Tx with po prednisone Approx. 200 lb weight gain (>400 lbs.) BVA: 20/20 OD 20/20 OS 161

162 162

163 163

164 164

165 OD 165

166 OS 166
167 Cont. MRI / MRV normal Coordinated care through HMO PCP Nothing done IEI 5 mos. later complaining of progressive severe HA (10/10) BVA: 20/20 OD 20/20 OS 167

168 168

169 169

170 OD 170

171 OS 171
172 32 y/o Hispanic Woman c/o progressive, debilitating headaches x 2 mos. Normal neurologic exam BVA: 20/20 OD 20/20 OS BMI:

173 173

174 174

175 175

176 176

177 177

178 178

179 179

180 180
181 F/U x 6 mos Rx Diamox (500 mg BID) Weight loss (approx. 25 lbs.) Improvement in headaches 181

182 182

183 183

184 184

185 185


186 186
187 F/U x 14 mos D/C Diamox x 3 months Weight loss (BMI reduction from 38 to 30) Headache free 187

188 188
189 189

190 Total RNFL Reduction OD: 386 to 97 OS: 442 to

191 191


192 192
193 193
194 IIH - Key Points Defining pseudotumor cerebri & IIH Pathogenesis of IIH Clinical features and neuroradiology Prognostic factors and management OCT analysis of papilledema Visual fields! 194
195 Thank you! 195
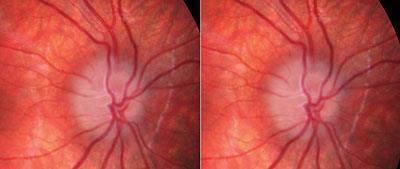
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings. Jonathan A. Micieli, MD Valérie Biousse, MD
 Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
Papilledema. Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D.
 Papilledema Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D. Papilledema specifically refers to optic nerve head swelling secondary to increased intracranial pressure (IICP). Optic nerve swelling from
Papilledema Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D. Papilledema specifically refers to optic nerve head swelling secondary to increased intracranial pressure (IICP). Optic nerve swelling from
Pearls, Pitfalls and Advances in Neuro-Ophthalmology
 Pearls, Pitfalls and Advances in Neuro-Ophthalmology Nancy J. Newman, MD Emory University Atlanta, GA Consultant for Gensight Biologics, Santhera Data Safety Monitoring Board for Quark AION Study Medical-legal
Pearls, Pitfalls and Advances in Neuro-Ophthalmology Nancy J. Newman, MD Emory University Atlanta, GA Consultant for Gensight Biologics, Santhera Data Safety Monitoring Board for Quark AION Study Medical-legal
12/2/16. Ways to differentiate:
 Nate Lighthizer, O.D., F.A.A.O. Assistant Dean for Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic Oklahoma College of Optometry lighthiz@nsuok.edu
Nate Lighthizer, O.D., F.A.A.O. Assistant Dean for Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic Oklahoma College of Optometry lighthiz@nsuok.edu
THE SWOLLEN DISC. Valerie Biousse, MD Emory University School of Medicine Atlanta, GA
 THE SWOLLEN DISC Valerie Biousse, MD Emory University School of Medicine Atlanta, GA Updated from: Neuro-Ophthalmology Illustrated. Biousse V, Newman NJ. Thieme, New-York,NY. 2 nd Ed, 2016. Edema of the
THE SWOLLEN DISC Valerie Biousse, MD Emory University School of Medicine Atlanta, GA Updated from: Neuro-Ophthalmology Illustrated. Biousse V, Newman NJ. Thieme, New-York,NY. 2 nd Ed, 2016. Edema of the
Neuro-Ocular Grand Rounds
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology
 David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology") Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology 26 year old 5 3, 300 pound female with papilledema,
Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology 26 year old 5 3, 300 pound female with papilledema,
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
OPTIC NERVE SWELLING IN CHILDHOOD
 OPTIC NERVE SWELLING IN CHILDHOOD Melissa W. Ko, MD, FAAN One of the main findings on a pediatric neurologic examination that can instill fear and lead to an urgent referral to neuro-ophthalmology is the
OPTIC NERVE SWELLING IN CHILDHOOD Melissa W. Ko, MD, FAAN One of the main findings on a pediatric neurologic examination that can instill fear and lead to an urgent referral to neuro-ophthalmology is the
Khalil Zahra, M.D Neuro-interventional radiology
 Khalil Zahra, M.D Neuro-interventional radiology 1 Disclosure None 2 Outline Etiology and pathogensis Imaging techniques and Features Literature review Treatment modalities Endovascular techniques Long
Khalil Zahra, M.D Neuro-interventional radiology 1 Disclosure None 2 Outline Etiology and pathogensis Imaging techniques and Features Literature review Treatment modalities Endovascular techniques Long
11/10/2017. Headache and Increased Pressure: A tale of 2 cases. Kathleen Digre MD University of Utah TWO CASES. 23 yo medical practice manager
 Headache and Increased Pressure: A tale of 2 cases Kathleen Digre MD University of Utah TWO CASES 23 yo medical practice manager September 2016 began developing intense frontal headaches first intermittent
Headache and Increased Pressure: A tale of 2 cases Kathleen Digre MD University of Utah TWO CASES 23 yo medical practice manager September 2016 began developing intense frontal headaches first intermittent
Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD
 Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD 58 YOWM! C/O I think there is something wrong with my vision, but I m not sure what it is.! +PMH for HTN, atrial fibrillation,
Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD 58 YOWM! C/O I think there is something wrong with my vision, but I m not sure what it is.! +PMH for HTN, atrial fibrillation,
Differential Diagnosis of ONH Edema Beth A. Steele, OD, FAAO
 Differential Diagnosis of ONH Edema Beth A. Steele, OD, FAAO bsteele@uab.edu Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is
Differential Diagnosis of ONH Edema Beth A. Steele, OD, FAAO bsteele@uab.edu Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is
Intracranial hypertension and headache. Daniel Tibussek, MD
 Intracranial hypertension and headache. Daniel Tibussek, MD none Disclosures Overview Case Clinical presentation of pediatric PTC Nomenclature, Definition What is intracranial hypertension? Diagnostic
Intracranial hypertension and headache. Daniel Tibussek, MD none Disclosures Overview Case Clinical presentation of pediatric PTC Nomenclature, Definition What is intracranial hypertension? Diagnostic
Dr/ Marwa Abdellah EOS /16/2018. Dr/ Marwa Abdellah EOS When do you ask Fluorescein angiography for optic disc diseases???
 When do you ask Fluorescein angiography for optic disc diseases??? 1 NORMAL OPTIC DISC The normal optic disc on fluorescein angiography is fluorescent due to filling of vessels arising from the posterior
When do you ask Fluorescein angiography for optic disc diseases??? 1 NORMAL OPTIC DISC The normal optic disc on fluorescein angiography is fluorescent due to filling of vessels arising from the posterior
Alan G. Kabat, OD, FAAO (901)
") THE SWOLLEN OPTIC DISC: EMERGENCY OR ANOMALY? Alan G. Kabat, OD, FAAO (901) 252-3691 Memphis, Tennessee alan.kabat@alankabat.com Course description: The swollen disc presents a diagnostic dilemma. While
THE SWOLLEN OPTIC DISC: EMERGENCY OR ANOMALY? Alan G. Kabat, OD, FAAO (901) 252-3691 Memphis, Tennessee alan.kabat@alankabat.com Course description: The swollen disc presents a diagnostic dilemma. While
Optic Nerve Anomalies
 Optic Nerve Anomalies Raman Bhakhri, OD, FAAO Southern California College of Optometry Marshall B. Ketchum University Goals for today Review some of the optic nerve anomalies that can be seen in practice
Optic Nerve Anomalies Raman Bhakhri, OD, FAAO Southern California College of Optometry Marshall B. Ketchum University Goals for today Review some of the optic nerve anomalies that can be seen in practice
Is it Papilloedema? John Ross Ainsworth Orthoptic staff Birmingham Children s Hospital Birmingham and Midland Eye Centre University of Birmingham
 Is it Papilloedema? John Ross Ainsworth Orthoptic staff Birmingham Children s Hospital Birmingham and Midland Eye Centre University of Birmingham Aims Children/young people A bit about hypoplasia / NFL
Is it Papilloedema? John Ross Ainsworth Orthoptic staff Birmingham Children s Hospital Birmingham and Midland Eye Centre University of Birmingham Aims Children/young people A bit about hypoplasia / NFL
NANOS Patient Brochure
 NANOS Patient Brochure Pseudotumor Cerebri Copyright 2016. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for
NANOS Patient Brochure Pseudotumor Cerebri Copyright 2016. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for
Idiopathic Intracranial Hypertension
 Idiopathic Intracranial Hypertension Dr. Mar'n Su+onBrown MD. FRCPC Neuro-Ophthalmology, Neurology Div of Neurology, Island Health Clinical Assistant Professor, Div of Neurology, UBC Stroke Rapid Assessment
Idiopathic Intracranial Hypertension Dr. Mar'n Su+onBrown MD. FRCPC Neuro-Ophthalmology, Neurology Div of Neurology, Island Health Clinical Assistant Professor, Div of Neurology, UBC Stroke Rapid Assessment
Optic Disc: Anatomy, Variants, Unusual discs. Kathleen B. Digre, MD Professor Neurology, Ophthalmology
 Optic Disc: Anatomy, Variants, Unusual discs Kathleen B. Digre, MD Professor Neurology, Ophthalmology THE OPHTHALMOSCOPE DIRECT OPHTHALMOSCOPY Jan Purkinje 1823 Hermann von Helmholtz 1851 Hand held ophthalmoscope
Optic Disc: Anatomy, Variants, Unusual discs Kathleen B. Digre, MD Professor Neurology, Ophthalmology THE OPHTHALMOSCOPE DIRECT OPHTHALMOSCOPY Jan Purkinje 1823 Hermann von Helmholtz 1851 Hand held ophthalmoscope
BMB Disclosures. Papilledema can be a. Neurological Emergency, Causing Preventable Blindness
 Reasonable Doubt: Can High Intracranial Pressure Occur Without Papilledema? 15 February 2013 Jonathan C. Horton hortonj@vision.ucsf.edu http://www.ucsf.edu/hortonlab BMB Disclosures Financial Disclosures
Reasonable Doubt: Can High Intracranial Pressure Occur Without Papilledema? 15 February 2013 Jonathan C. Horton hortonj@vision.ucsf.edu http://www.ucsf.edu/hortonlab BMB Disclosures Financial Disclosures
Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt
 The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (5), Page 4556-4560 Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt Ali K. Ali, Maamoun M. Abo Shousha, Mohammed
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (5), Page 4556-4560 Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt Ali K. Ali, Maamoun M. Abo Shousha, Mohammed
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Optic Nerve Disorders: Structure and Function and Causes
 Optic Nerve Disorders: Structure and Function and Causes Using Visual Fields, OCT and B-scan Ultrasound to Diagnose and Follow Optic Nerve Visual Losses Ohio Ophthalmological Society and Ophthalmic Tech
Optic Nerve Disorders: Structure and Function and Causes Using Visual Fields, OCT and B-scan Ultrasound to Diagnose and Follow Optic Nerve Visual Losses Ohio Ophthalmological Society and Ophthalmic Tech
PITFALLS IN PAPILLOEDEMA
 PITFALLS IN PAPILLOEDEMA SRC 2013 Why care about papilloedema? Dr Neil Shuey FRACP MBBS(Hons) MScOptom St Vincent s Hospital, Melbourne Royal Victorian Eye & Ear Hospital Disclosures: Travel grants Biogen
PITFALLS IN PAPILLOEDEMA SRC 2013 Why care about papilloedema? Dr Neil Shuey FRACP MBBS(Hons) MScOptom St Vincent s Hospital, Melbourne Royal Victorian Eye & Ear Hospital Disclosures: Travel grants Biogen
Sequential non-arteritic anterior ischemic optic neuropathy (NAION) Jonathan A. Micieli, MD Valérie Biousse, MD
 Jonathan A. Micieli, MD Valérie Biousse, MD") Sequential non-arteritic anterior ischemic optic neuropathy (NAION) Jonathan A. Micieli, MD Valérie Biousse, MD A 68 year old white woman had a new onset of floaters in her right eye and was found to have
Sequential non-arteritic anterior ischemic optic neuropathy (NAION) Jonathan A. Micieli, MD Valérie Biousse, MD A 68 year old white woman had a new onset of floaters in her right eye and was found to have
Prevalence of venous sinus stenosis in Pseudotumor cerebri(ptc) using digital subtraction angiography (DSA)
 using digital subtraction angiography (DSA)") Prevalence of venous sinus stenosis in Pseudotumor cerebri(ptc) using digital subtraction angiography (DSA) Dr.Mohamed hamdy ibrahim MBBC,MSc,MD, PhD Neurology Degree Kings lake university (USA). Fellow
Prevalence of venous sinus stenosis in Pseudotumor cerebri(ptc) using digital subtraction angiography (DSA) Dr.Mohamed hamdy ibrahim MBBC,MSc,MD, PhD Neurology Degree Kings lake university (USA). Fellow
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetazolamide, in idiopathic intracranial hypertension, 49 52, 60 Angiography, computed tomography, in cranial nerve palsy, 103 107 digital
Index Note: Page numbers of article titles are in boldface type. A Acetazolamide, in idiopathic intracranial hypertension, 49 52, 60 Angiography, computed tomography, in cranial nerve palsy, 103 107 digital
Learn Connect Succeed. JCAHPO Regional Meetings 2015
 Learn Connect Succeed JCAHPO Regional Meetings 2015 OPTIC NEUROPATHY AS EASY AS 1,2,3,4 OPTIC NERVE ANATOMY M. Tariq Bhatti, MD Departments of Ophthalmology and Neurology Duke Eye Center and Duke University
Learn Connect Succeed JCAHPO Regional Meetings 2015 OPTIC NEUROPATHY AS EASY AS 1,2,3,4 OPTIC NERVE ANATOMY M. Tariq Bhatti, MD Departments of Ophthalmology and Neurology Duke Eye Center and Duke University
Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health
 Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health History 15 year old African female with CC of Headache. Onset: 2 weeks ago Location: Frontal Character: Sharp & Throbbing Radiation: None
Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health History 15 year old African female with CC of Headache. Onset: 2 weeks ago Location: Frontal Character: Sharp & Throbbing Radiation: None
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Neuro-Ophthalmic Masqueraders
 Neuro-Ophthalmic Masqueraders Leonid Skorin, Jr., OD, DO, MS, FAAO, FAOCO Mayo Clinic Health System in Albert Lea Denise Goodwin, OD, FAAO Pacific University College of Optometry Please silence all mobile
Neuro-Ophthalmic Masqueraders Leonid Skorin, Jr., OD, DO, MS, FAAO, FAOCO Mayo Clinic Health System in Albert Lea Denise Goodwin, OD, FAAO Pacific University College of Optometry Please silence all mobile
The Optic Nerve Head In Glaucoma. Clinical Pearl #1. Characteristics of Normal Disk 9/26/2017. Initial detectable damage Structure vs function
 The Optic Nerve Head In Glaucoma Clinical Pearl #1 Eric E. Schmidt, O.D., F.A.A.O. Omni Eye Specialists Wilmington,NC schmidtyvision@msn.com Glaucoma is an optic neuropathy Initial detectable damage Structure
The Optic Nerve Head In Glaucoma Clinical Pearl #1 Eric E. Schmidt, O.D., F.A.A.O. Omni Eye Specialists Wilmington,NC schmidtyvision@msn.com Glaucoma is an optic neuropathy Initial detectable damage Structure
Learn Connect Succeed. JCAHPO Regional Meetings 2017
 Learn Connect Succeed JCAHPO Regional Meetings 2017 NO FINANCIAL DISCLOSURES Technician s Role in Neuro-Ophthalmology Workup Beth Koch COT, ROUB Cleveland 9/16/2017 What Tests Are You Expected To Perform?
Learn Connect Succeed JCAHPO Regional Meetings 2017 NO FINANCIAL DISCLOSURES Technician s Role in Neuro-Ophthalmology Workup Beth Koch COT, ROUB Cleveland 9/16/2017 What Tests Are You Expected To Perform?
CONFESSIONS OF A PSEUDOTUMOR CEREBRIST
 CONFESSIONS OF A PSEUDOTUMOR CEREBRIST Jean B Kassem, M.D. Neuro-Ophthalmology, Orbital Surgery, Oculoplastics Bellingham Eye Physicians Bellingham, WA Goals Understand Intracranial Hypertension and its
CONFESSIONS OF A PSEUDOTUMOR CEREBRIST Jean B Kassem, M.D. Neuro-Ophthalmology, Orbital Surgery, Oculoplastics Bellingham Eye Physicians Bellingham, WA Goals Understand Intracranial Hypertension and its
The headache profile of idiopathic intracranial hypertension
 The headache profile of idiopathic intracranial hypertension Michael Wall CEPHALALGIA Wall M. The headache profile of idiopathic intracranial hypertension. Cephalalgia 1990;10:331-5. Oslo. ISSN 0333-1024
The headache profile of idiopathic intracranial hypertension Michael Wall CEPHALALGIA Wall M. The headache profile of idiopathic intracranial hypertension. Cephalalgia 1990;10:331-5. Oslo. ISSN 0333-1024
Rebound Intracranial Hypertension Following Treatment of Spinal CSF Leaks
 Rebound Intracranial Hypertension Following Treatment of Spinal CSF Leaks Deborah I. Friedman, MD, MPH University of Texas Southwestern Medical Center Dallas, Texas Disclosures (past 2 years): Role Advisory
Rebound Intracranial Hypertension Following Treatment of Spinal CSF Leaks Deborah I. Friedman, MD, MPH University of Texas Southwestern Medical Center Dallas, Texas Disclosures (past 2 years): Role Advisory
Picture of patient with apparent lid retraction and poor elevation. Shows you Orbital CT-Scan with muscle involvement including IR and asks is this
 NEUROLOGY Q: MENINGIOMAS AND SKULL (*2) Real skull is given, and you are asked to point to tuberculum sella What kind of meningioma occurs at this location? Where is the anterior clinoid process? Where
NEUROLOGY Q: MENINGIOMAS AND SKULL (*2) Real skull is given, and you are asked to point to tuberculum sella What kind of meningioma occurs at this location? Where is the anterior clinoid process? Where
IDIOPATHIC INTRACRANIAL HYPERTENSION
 IDIOPATHIC INTRACRANIAL HYPERTENSION ASSESSMENT OF VISUAL FUNCTION AND PROGNOSIS FOR VISUAL OUTCOME Doctor of Philosophy thesis Anglia Ruskin University, Cambridge Fiona J. Rowe Department of Orthoptics,
IDIOPATHIC INTRACRANIAL HYPERTENSION ASSESSMENT OF VISUAL FUNCTION AND PROGNOSIS FOR VISUAL OUTCOME Doctor of Philosophy thesis Anglia Ruskin University, Cambridge Fiona J. Rowe Department of Orthoptics,
Chapter 2 Long Duration Flight Data
 Chapter 2 Long Duration Flight Data Astronaut s bodies suffer in microgravity. Without effective countermeasures, muscles atrophy, bones shed calcium, and eyesight deteriorates. We ve known about this
Chapter 2 Long Duration Flight Data Astronaut s bodies suffer in microgravity. Without effective countermeasures, muscles atrophy, bones shed calcium, and eyesight deteriorates. We ve known about this
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA
 OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
Neuropathy (NAION) and Avastin. Clinical Assembly of the AOCOO-HNS Foundation May 9, 2013
 and Avastin. Clinical Assembly of the AOCOO-HNS Foundation May 9, 2013") Non Arteritic Ischemic Optic Neuropathy (NAION) and Avastin Shalom Kelman, MD Clinical Assembly of the AOCOO-HNS Foundation May 9, 2013 Anterior Ischemic Optic Neuropathy Acute, painless, visual loss,
Non Arteritic Ischemic Optic Neuropathy (NAION) and Avastin Shalom Kelman, MD Clinical Assembly of the AOCOO-HNS Foundation May 9, 2013 Anterior Ischemic Optic Neuropathy Acute, painless, visual loss,
Evaluation of ONH Pallor in Glaucoma Patients and Suspects. Leticia Rousso, O.D. Joseph Sowka, O.D
 Evaluation of ONH Pallor in Glaucoma Patients and Suspects Leticia Rousso, O.D Joseph Sowka, O.D I. Abstract This case report will evaluate a young glaucoma suspect with unilateral sectoral optic nerve
Evaluation of ONH Pallor in Glaucoma Patients and Suspects Leticia Rousso, O.D Joseph Sowka, O.D I. Abstract This case report will evaluate a young glaucoma suspect with unilateral sectoral optic nerve
CHAPTER 13 CLINICAL CASES INTRODUCTION
 2 CHAPTER 3 CLINICAL CASES INTRODUCTION The previous chapters of this book have systematically presented various aspects of visual field testing and is now put into a clinical context. In this chapter,
2 CHAPTER 3 CLINICAL CASES INTRODUCTION The previous chapters of this book have systematically presented various aspects of visual field testing and is now put into a clinical context. In this chapter,
My Doc told me I needed an eye exam because.. Bruce Onofrey, OD, RPh, FAAO Professor, U. Houston UEI
 My Doc told me I needed an eye exam because.. Bruce Onofrey, OD, RPh, FAAO eyedoc3@aol.com Professor, U. Houston UEI Drugs can blind you (the patient) Cataract Glaucoma Uveitis Dry eye Macular disease
My Doc told me I needed an eye exam because.. Bruce Onofrey, OD, RPh, FAAO eyedoc3@aol.com Professor, U. Houston UEI Drugs can blind you (the patient) Cataract Glaucoma Uveitis Dry eye Macular disease
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Greater than expected prevalence of pseudotumor cerebri: a prospective study
 Surgery for Obesity and Related Diseases 9 (2013) 77 82 Original article Greater than expected prevalence of pseudotumor cerebri: a prospective study Isam N. Hamdallah, M.D., Hazem N. Shamseddeen, M.D.,
Surgery for Obesity and Related Diseases 9 (2013) 77 82 Original article Greater than expected prevalence of pseudotumor cerebri: a prospective study Isam N. Hamdallah, M.D., Hazem N. Shamseddeen, M.D.,
Unexplained visual loss in seven easy steps
 Unexplained visual loss in seven easy steps Andrew G. Lee, MD Chair Ophthalmology, Houston Methodist Hospital, Professor, Weill Cornell MC; Adjunct Professor, Baylor COM, U Iowa, UTMB Galveston, UT MD
Unexplained visual loss in seven easy steps Andrew G. Lee, MD Chair Ophthalmology, Houston Methodist Hospital, Professor, Weill Cornell MC; Adjunct Professor, Baylor COM, U Iowa, UTMB Galveston, UT MD
OCT Angiography The Next Frontier
 Choroid Retina avascular 5/13/2017 OCT Angiography The Next Frontier Pierce Kenworthy OD, FAAO June 9, 2017 OCT Angiography (OCTA) 2016 Non-invasive, motion contrast imaging Represents erythrocyte movement
Choroid Retina avascular 5/13/2017 OCT Angiography The Next Frontier Pierce Kenworthy OD, FAAO June 9, 2017 OCT Angiography (OCTA) 2016 Non-invasive, motion contrast imaging Represents erythrocyte movement
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Question 1: Comment on the optic nerve appearance of each eye.
 Case 2 - Right Optic Nerve Head Drusen (ONHD) A 41 year old female was referred by her optometrist for a workup for unilateral optic disc drusen, OCT, and visual field changes. The patient was otherwise
Case 2 - Right Optic Nerve Head Drusen (ONHD) A 41 year old female was referred by her optometrist for a workup for unilateral optic disc drusen, OCT, and visual field changes. The patient was otherwise
Spaceflight Associated Neuro-ocular Syndrome (SANS): Current Clinical Insight & Questions of Interest
: Current Clinical Insight & Questions of Interest") Spaceflight Associated Neuro-ocular Syndrome (SANS): Current Clinical Insight & Questions of Interest Tyson Brunstetter, OD, PhD, MBA, FAAO, FAsMA Captain, Medical Service Corps, U.S. Navy Deputy SANS
Spaceflight Associated Neuro-ocular Syndrome (SANS): Current Clinical Insight & Questions of Interest Tyson Brunstetter, OD, PhD, MBA, FAAO, FAsMA Captain, Medical Service Corps, U.S. Navy Deputy SANS
The Glaucoma Suspect. Evaluating the Suspect Disk. Dr Michael Forrest. ! the usual suspects: ! is it glaucoma? ! is it swollen?
 Evaluating the Suspect Disk Dr Michael Forrest Senior Lecturer, The University of Queensland Northside Eye Specialists, Nundah Visiting Ophthalmologist, Mater Hospital, Brisbane Australian Vision Convention
Evaluating the Suspect Disk Dr Michael Forrest Senior Lecturer, The University of Queensland Northside Eye Specialists, Nundah Visiting Ophthalmologist, Mater Hospital, Brisbane Australian Vision Convention
The Diagnostic Dilemma of Pseudopapilledema. Tiffenie Harris, OD, FAAO Associate Professor Western University College of Optometry
 The Diagnostic Dilemma of Pseudopapilledema Tiffenie Harris, OD, FAAO Associate Professor Western University College of Optometry Author s Bio Dr. Harris is a graduate of Indiana University School of Optometry.
The Diagnostic Dilemma of Pseudopapilledema Tiffenie Harris, OD, FAAO Associate Professor Western University College of Optometry Author s Bio Dr. Harris is a graduate of Indiana University School of Optometry.
Non-arteritic anterior ischemic optic neuropathy (NAION) with segmental optic disc edema. Jonathan A. Micieli, MD Valérie Biousse, MD
 with segmental optic disc edema. Jonathan A. Micieli, MD Valérie Biousse, MD") Non-arteritic anterior ischemic optic neuropathy (NAION) with segmental optic disc edema Jonathan A. Micieli, MD Valérie Biousse, MD A 75 year old white woman lost vision in the inferior part of her visual
Non-arteritic anterior ischemic optic neuropathy (NAION) with segmental optic disc edema Jonathan A. Micieli, MD Valérie Biousse, MD A 75 year old white woman lost vision in the inferior part of her visual
Pseudotumor Cerebri Secondary to Minocycline Intake
 Pseudotumor Cerebri Secondary to Minocycline Intake Earl Robert G. Ang, MD, J. C. Chava Zimmerman, MD, and Elissa Malkin, DO, MPH Background: Pseudotumor cerebri, or idiopathic intracranial hypertension,
Pseudotumor Cerebri Secondary to Minocycline Intake Earl Robert G. Ang, MD, J. C. Chava Zimmerman, MD, and Elissa Malkin, DO, MPH Background: Pseudotumor cerebri, or idiopathic intracranial hypertension,
No Financial Interest
 Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
3/16/2018. Optic nerve axons of retinal ganglion cells. 1.2 million nerve fibers. ON sheath: continuous with the meninges dura arachnoid and pia mater
 Optic nerve axons of retinal ganglion cells 1.2 million nerve fibers. ON sheath: continuous with the meninges dura arachnoid and pia mater 1 1.Visual Acuity 2.Color Vision 3.Pupil 4.Contrast sensitivity
Optic nerve axons of retinal ganglion cells 1.2 million nerve fibers. ON sheath: continuous with the meninges dura arachnoid and pia mater 1 1.Visual Acuity 2.Color Vision 3.Pupil 4.Contrast sensitivity
CSF. Cerebrospinal Fluid(CSF) System
 System") Cerebrospinal Fluid(CSF) System By the end of the lecture, students must be able to describe Physiological Anatomy of CSF Compartments Composition Formation Circulation Reabsorption CSF Pressure Functions
Cerebrospinal Fluid(CSF) System By the end of the lecture, students must be able to describe Physiological Anatomy of CSF Compartments Composition Formation Circulation Reabsorption CSF Pressure Functions
Objectives. Unexplained Vision Loss: Where Do I Go From Here. History. History. Drug Induced Vision Loss
 Objectives Unexplained Vision Loss: Where Do I Go From Here Denise Goodwin, OD, FAAO Coordinator, Neuro-ophthalmic Disease Clinic Pacific University College of Optometry goodwin@pacificu.edu Know the importance
Objectives Unexplained Vision Loss: Where Do I Go From Here Denise Goodwin, OD, FAAO Coordinator, Neuro-ophthalmic Disease Clinic Pacific University College of Optometry goodwin@pacificu.edu Know the importance
Use of scanning laser ophthalmoscopy to monitor papilloedema in idiopathic intracranial hypertension
 Br J Ophthalmol 998;8:35 3 Ophthalmology, Royal Victoria Hospital, Belfast D A Mulholland S J A Rankin Neurology, Royal Victoria Hospital, Belfast J J Craig Correspondence to: Mr David A Mulholland, Ophthalmology,
Br J Ophthalmol 998;8:35 3 Ophthalmology, Royal Victoria Hospital, Belfast D A Mulholland S J A Rankin Neurology, Royal Victoria Hospital, Belfast J J Craig Correspondence to: Mr David A Mulholland, Ophthalmology,
NASA s Visual Impairment & Intracranial Pressure Risk: Utilizing the ISS for Risk Reduction
 NASA s Visual Impairment & Intracranial Pressure Risk: Utilizing the ISS for Risk Reduction Christian Otto, M.D. Lead Scientist, NASA VIIP Project Page No. 1 1 St Annual ISS Research & Development Conference
NASA s Visual Impairment & Intracranial Pressure Risk: Utilizing the ISS for Risk Reduction Christian Otto, M.D. Lead Scientist, NASA VIIP Project Page No. 1 1 St Annual ISS Research & Development Conference
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Ocular Manifestations of Systemic Disease: Grand Rounds Kimberly K. Reed, O.D., FAAO
 Ocular Manifestations of Systemic Disease: Grand Rounds Kimberly K. Reed, O.D., FAAO Course description: This course describes several ocular presentations that result from a systemic disease or condition.
Ocular Manifestations of Systemic Disease: Grand Rounds Kimberly K. Reed, O.D., FAAO Course description: This course describes several ocular presentations that result from a systemic disease or condition.
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
What is IIH? Idiopathic Intracranial Hypertension (IIH)
") What is IIH? Idiopathic Intracranial Hypertension (IIH) What is Idiopathic Intracranial Hypertension? Idiopathic intracranial hypertension (IIH), also known as benign intracranial hypertension or pseudotumour
What is IIH? Idiopathic Intracranial Hypertension (IIH) What is Idiopathic Intracranial Hypertension? Idiopathic intracranial hypertension (IIH), also known as benign intracranial hypertension or pseudotumour
Mark Dunbar: Disclosure
 Important Things to Understand About OCT Mark T. Dunbar, O.D., F.A.A.O. Bascom Palmer Eye Institute University of Miami, School of Medicine Mark Dunbar: Disclosure Optometry Advisory Board for: Allergan
Important Things to Understand About OCT Mark T. Dunbar, O.D., F.A.A.O. Bascom Palmer Eye Institute University of Miami, School of Medicine Mark Dunbar: Disclosure Optometry Advisory Board for: Allergan
Learn Connect Succeed. JCAHPO Regional Meetings 2017
 Learn Connect Succeed JCAHPO Regional Meetings 2017 You have some Nerve Asking Me to Work Up that Patient! What I Need to know about the Neuro- Ophthalmology Patient Financial Disclosures No relevant financial
Learn Connect Succeed JCAHPO Regional Meetings 2017 You have some Nerve Asking Me to Work Up that Patient! What I Need to know about the Neuro- Ophthalmology Patient Financial Disclosures No relevant financial
Headache Syndrome. Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL
 Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Blindness In An Elderly Woman
 Blindness In An Elderly Woman A 74 y/o woman with a chief complaint of: a cloud in front of my right eye and I can t t see through it Symptoms began 24 hours prior to examination. Visual loss was painless
Blindness In An Elderly Woman A 74 y/o woman with a chief complaint of: a cloud in front of my right eye and I can t t see through it Symptoms began 24 hours prior to examination. Visual loss was painless
Endoscopic Optic Nerve Sheath Fenestration for Treatment of Papilledema Secondary to Intracranial Venous Hypertension: Report of Two Cases
 Case Report Endoscopic Optic Nerve Sheath Fenestration for Treatment of Papilledema Secondary to Intracranial Venous Hypertension: Report of Two Cases Wuttipong Tirakotai MD, MSc, Dr.med*, Patcharapim
Case Report Endoscopic Optic Nerve Sheath Fenestration for Treatment of Papilledema Secondary to Intracranial Venous Hypertension: Report of Two Cases Wuttipong Tirakotai MD, MSc, Dr.med*, Patcharapim
Professor Helen Danesh-Meyer. Eye Institute Auckland
 Professor Helen Danesh-Meyer Eye Institute Auckland Bitten by Ophthalmology Emergencies Helen Danesh-Meyer, MBChB, MD, FRANZCO Sir William and Lady Stevenson Professor of Ophthalmology Head of Glaucoma
Professor Helen Danesh-Meyer Eye Institute Auckland Bitten by Ophthalmology Emergencies Helen Danesh-Meyer, MBChB, MD, FRANZCO Sir William and Lady Stevenson Professor of Ophthalmology Head of Glaucoma
Sahand Ensafi PA, CCPA, B.H.Sc.,Department of Emergency Medicine, University Health Network
 Sahand Ensafi PA, CCPA, B.H.Sc.,Department of Emergency Medicine, University Health Network No Disclosures Definitions Ophthalmologic Blindness Practical definition? WHO V/A less than 3/60 (snellen)
Sahand Ensafi PA, CCPA, B.H.Sc.,Department of Emergency Medicine, University Health Network No Disclosures Definitions Ophthalmologic Blindness Practical definition? WHO V/A less than 3/60 (snellen)
A Curious Case of Bilateral Optic Disc Edema Brittney Dautremont, DO, MPH
 A Curious Case of Bilateral Optic Disc Edema Brittney Dautremont, DO, MPH PGY2 Ophthalmology Resident Grandview Medical Center Dayton, OH CASE PRESENTATION 51 year old white female presenting with blurred
A Curious Case of Bilateral Optic Disc Edema Brittney Dautremont, DO, MPH PGY2 Ophthalmology Resident Grandview Medical Center Dayton, OH CASE PRESENTATION 51 year old white female presenting with blurred
Cases of visual impairment caused by cerebral venous sinus occlusion-induced intracranial hypertension in the absence of headache
 Zhao et al. BMC Neurology (2018) 18:159 https://doi.org/10.1186/s12883-018-1156-7 CASE REPORT Open Access Cases of visual impairment caused by cerebral venous sinus occlusion-induced intracranial hypertension
Zhao et al. BMC Neurology (2018) 18:159 https://doi.org/10.1186/s12883-018-1156-7 CASE REPORT Open Access Cases of visual impairment caused by cerebral venous sinus occlusion-induced intracranial hypertension
MOHAMED LOTFY, M.D.*; MOATAZ A. EL-AWADY, M.D.**; ASHRAF E. ZAGHLOUL, M.D.** and TAREK NEHAD, M.D.***
 Med. J. Cairo Univ., Vol. 84, No. 2, December: 301-306, 2016 www.medicaljournalofcairouniversity.net Effect of Therapeutic Lumbar Puncture on the Visual Outcome and the Further Need for Surgery in Patients
Med. J. Cairo Univ., Vol. 84, No. 2, December: 301-306, 2016 www.medicaljournalofcairouniversity.net Effect of Therapeutic Lumbar Puncture on the Visual Outcome and the Further Need for Surgery in Patients
The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery
 The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery The Case: Upon awakening from anesthesia, he is blind in both eyes After Non-Ocular Surgeries Nancy J. Newman,
The Case: A 64 yo man with chronic back pain has elective multilevel lumbar spinal surgery The Case: Upon awakening from anesthesia, he is blind in both eyes After Non-Ocular Surgeries Nancy J. Newman,
I have nothing to disclose but I
 OPTIC NEUROPATHIES Robert L. Tomsak MD PhD Professor of Ophthalmology and Neurology Wayne State t University it Sh School of Mdii Medicine I have nothing to disclose but I wish I did. dd Road map for this
OPTIC NEUROPATHIES Robert L. Tomsak MD PhD Professor of Ophthalmology and Neurology Wayne State t University it Sh School of Mdii Medicine I have nothing to disclose but I wish I did. dd Road map for this
Carotid Cavernous Fistula
 Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
DISCLOSURE: What to do? 2/22/2016
 DISCLOSURE: Dr. Joseph Sowka is a member of the Speakers Bureau for Alcon Laboratories, and Carl Zeiss Meditec. He is on the advisory boards for Alcon, Zeiss, and Allergan. He is a consultant for Alcon.
DISCLOSURE: Dr. Joseph Sowka is a member of the Speakers Bureau for Alcon Laboratories, and Carl Zeiss Meditec. He is on the advisory boards for Alcon, Zeiss, and Allergan. He is a consultant for Alcon.
Retinal Complications of Obstructive Sleep Apnea A Growing Concern!
 Retinal Complications of Obstructive Sleep Apnea A Growing Concern! Jay M. Haynie, OD, FAAO Financial Disclosure I have received honoraria or am on the advisory board for the following companies: Carl
Retinal Complications of Obstructive Sleep Apnea A Growing Concern! Jay M. Haynie, OD, FAAO Financial Disclosure I have received honoraria or am on the advisory board for the following companies: Carl
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
9/11/11. Temporal Arteritis. Background. Background. Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service
 Temporal Arteritis Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service 1 Background Giant Cell Arteritis Temporal Arteritis Cranial Arteritis Granulomatous Arteritis
Temporal Arteritis Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service 1 Background Giant Cell Arteritis Temporal Arteritis Cranial Arteritis Granulomatous Arteritis
3/16/2018. Optic Nerve Examination. Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital
 Air Force Hospital") Optic Nerve Examination Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital 1 Examination Structure ( optic disc) Function Examination of the optic disc The only cranial nerve (brain tract) which
Optic Nerve Examination Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital 1 Examination Structure ( optic disc) Function Examination of the optic disc The only cranial nerve (brain tract) which
OBSTRUCTIVE sleep apnea
 CLINICAL SCIENCES Papilledema and Obstructive Sleep Apnea Syndrome Valerie A. Purvin, MD; Aki Kawasaki, MD; Robert D. Yee, MD Objectives: To characterize the pathogenesis and clinical features of optic
CLINICAL SCIENCES Papilledema and Obstructive Sleep Apnea Syndrome Valerie A. Purvin, MD; Aki Kawasaki, MD; Robert D. Yee, MD Objectives: To characterize the pathogenesis and clinical features of optic
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
ACTIVATED OR NOT? RETINAL CASE PRESENTATION Shorye Payne, MD Medical Retinal Specialist Robley Rex VA Eye Clinic
 ACTIVATED OR NOT? RETINAL CASE PRESENTATION Shorye Payne, MD Medical Retinal Specialist Robley Rex VA Eye Clinic C We anticipate that the future management of posterior uveal melanoma (PUM) will focus
ACTIVATED OR NOT? RETINAL CASE PRESENTATION Shorye Payne, MD Medical Retinal Specialist Robley Rex VA Eye Clinic C We anticipate that the future management of posterior uveal melanoma (PUM) will focus
Neurological Dilemmas in Primary Care
 Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Idiopathic Intracranial Hypertension Update
 Idiopathic Intracranial Hypertension Update Chris Borgman, OD, FAAO Southern College of Optometry Memphis, TN COPE Disclosures: I do not have any relevant financial relationships to disclose. The content
Idiopathic Intracranial Hypertension Update Chris Borgman, OD, FAAO Southern College of Optometry Memphis, TN COPE Disclosures: I do not have any relevant financial relationships to disclose. The content
Neuro-ophthalmologyophthalmology. Marek Michalec, MD.
 Neuro-ophthalmologyophthalmology Marek Michalec, MD. Neuro-ophthalmology Study integrating ophthalmology and neurology Disorders affecting parts of CNS devoted to vision or eye: Afferent system (visual
Neuro-ophthalmologyophthalmology Marek Michalec, MD. Neuro-ophthalmology Study integrating ophthalmology and neurology Disorders affecting parts of CNS devoted to vision or eye: Afferent system (visual
Incorporating OCT Angiography Into Patient Care
 Incorporating OCT Angiography Into Patient Care Beth A. Steele, OD, FAAO OCT A: Introduction Isolates microvascular circulation from OCT image data Axial resolution = 5 microns (i.e. fine capillaries visible)
Incorporating OCT Angiography Into Patient Care Beth A. Steele, OD, FAAO OCT A: Introduction Isolates microvascular circulation from OCT image data Axial resolution = 5 microns (i.e. fine capillaries visible)
41 year old female with headache. Elena G. Violari MD and Leo Wolansky MD
 41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
IMAGE OF THE MOMENT PRACTICAL NEUROLOGY
 178 PRACTICAL NEUROLOGY IMAGE OF THE MOMENT Gawn G. McIlwaine*, James H. Vallance* and Christian J. Lueck *Princess Alexandra Eye Pavilion, Chalmers Street, Edinburgh UK; The Canberra Hospital, P.O. Box
178 PRACTICAL NEUROLOGY IMAGE OF THE MOMENT Gawn G. McIlwaine*, James H. Vallance* and Christian J. Lueck *Princess Alexandra Eye Pavilion, Chalmers Street, Edinburgh UK; The Canberra Hospital, P.O. Box
Abstract title: Vision loss from myelinated retinal nerve fiber layer with maculopathy. Authors: Man Kin (Eric) Chow, OD Lori Vollmer, OD, FAAO
 Chow, OD Lori Vollmer, OD, FAAO") Abstract title: Vision loss from myelinated retinal nerve fiber layer with maculopathy. Authors: Man Kin (Eric) Chow, OD Lori Vollmer, OD, FAAO Joseph Sowka, OD, FAAO General Topic: Ocular Disease Primary
Abstract title: Vision loss from myelinated retinal nerve fiber layer with maculopathy. Authors: Man Kin (Eric) Chow, OD Lori Vollmer, OD, FAAO Joseph Sowka, OD, FAAO General Topic: Ocular Disease Primary
Intro to Glaucoma/2006
 Intro to Glaucoma/2006 Managing Patients with Glaucoma is Exciting Interesting Challenging But can often be frustrating! Clinical Challenges To identify patients with risk factors for possible glaucoma.
Intro to Glaucoma/2006 Managing Patients with Glaucoma is Exciting Interesting Challenging But can often be frustrating! Clinical Challenges To identify patients with risk factors for possible glaucoma.
Idiopathic Intracranial Hypertension in Pregnant Women
 Azza A. Ghali et al. Idiopathic Intracranial Hypertension in Pregnant Women Azza Abass Ghali, Ehab El-Seidy, Tarek Ragaiey Hussein 2, Manal Mostfa 3 Departments of Neuropsychiatry, Ophthalmology 2, Obstetrics
Azza A. Ghali et al. Idiopathic Intracranial Hypertension in Pregnant Women Azza Abass Ghali, Ehab El-Seidy, Tarek Ragaiey Hussein 2, Manal Mostfa 3 Departments of Neuropsychiatry, Ophthalmology 2, Obstetrics
Optical coherence tomography of the retinal nerve fibre layer in mild papilloedema and pseudopapilloedema
 294 SCIENTIFIC REPORT Optical coherence tomography of the retinal nerve fibre layer in mild papilloedema and pseudopapilloedema E Z Karam, T R Hedges... Aims: To determine the degree to which optical coherence
294 SCIENTIFIC REPORT Optical coherence tomography of the retinal nerve fibre layer in mild papilloedema and pseudopapilloedema E Z Karam, T R Hedges... Aims: To determine the degree to which optical coherence
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation