Decellularization of Aortic Homografts: South American and European Current Experience
|
|
|
- Jemima Harvey
- 5 years ago
- Views:
Transcription



1 Department of Cardiac Surgery Instituto de Neurologia e Cardiologia de Curitiba (INC-Cardio) Decellularization of Aortic Homografts: South American and European Current Experience Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil
2 DISCLOSURES Ownership and patent license of the SDS decellularization technique (d-cell Allograft) Consultant and Member of the Advisory Board Tissue Regenix Ltd England


3 DECELLULARIZED HEART VALVE Decellularization Technique Fresh Allografts, no cryopreservation Storage at 4º C for up to 6 months


4 Fresh Aortic Cusp PRM 100x Descellularized Aortic Cusp PRM 100x

5 Decellularized Heart Valves Brazilian Experience ( ) Number of Implants = 1870 cases

6 Cryolife aortic valve replacement
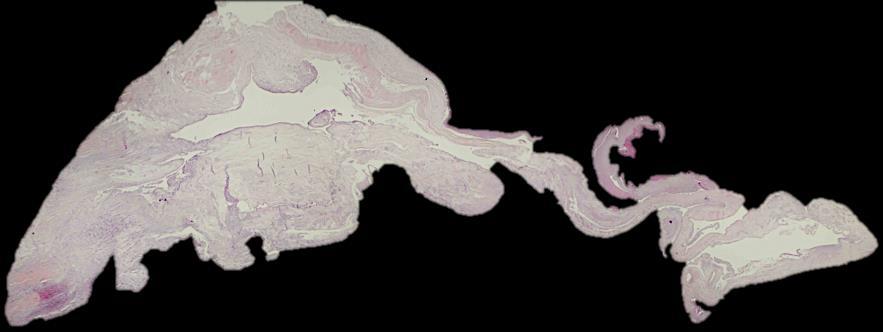
7 Synergraft aortic homograft study Reasons for reoperation in DAVA: endocarditis 26 % aortic stenosis 29 % aortic regurgitation 31 % Only 10 DAVA were available for histological analysis in 7 edematous degeneration and calcifications were found in 3 valves mild recellularisation was found adventitial fibrosis and neointimal fibrosis were identified in all 10 specimens

8 Long term follow up crucial Cusp Wall
9 CryoLife homograft processing Proprietary technique, details unknown such as strength testing after processing Homografts in the Helder report have been cryopreserved and radiated before implantation. Both of these procedures have been demonstrated to impact the ultrastructure. Sarathchandra P, Smolenski RT, Yuen AH, Chester AH, Goldstein S, Heacox AE, Yacoub MH, Taylor PM. Impact of γ-irradiation on extracellular matrix of porcine pulmonary valves. J Surg Res Aug;176(2): In contrast, the ARISE trial is evaluating fresh, non-cryopreserved and nonradiated DAH for AVR. Courtesy of Prof Samir Sarikouch - Hannover



10 The ARISE Study Group Hospitals Tissue Banks Processing A. Haverich J. Pepper J.L. Pomar Biobank M. Hazekamp G. Stellin B. Meyns M. Hübler G. Laufer A. Lichtenberg Administration Courtesy of Prof Samir Sarikouch - Hannover
11 Current status clinical trial Calculated sample size patients ARISE - Homografts Inclusion stopped Courtesy of Prof Samir Sarikouch - Hannover


12 Current status clinical trial Courtesy of Prof Samir Sarikouch - Hannover

13 Hospitals Tissue Banks Processing Biobank
14 Hospitals Tissue Banks Processing Biobank
15 Courtesy of Prof Samir Sarikouch - Hannover Overview cell-free homografts 9/2018 Aortic valve Period 02/ /2018 Diameter Patients Mean age Age range Follow-up 22.4 ± 3.0 mm 180 (210 total) 27.0 ± 20.0 yrs., (in >40 % as a redo operation) yrs. 100% (1313 exams) Patient years total Mean follow-up years 2.0 ± 2.1 (max. 9.5) Max. gradient (mmhg) 16.2 ± 18.0 Regurgitation (Grad 0-3) 0.5 ± 0.6 Freedom from explantation 94.3 % (n=12/210)
16 Freedom from Explantation (%) Freedom from explantation Age group: 1: <10 2: > Number at risk Time Group: 1: < Group: 2: Group: 3- > Courtesy of Prof Samir Sarikouch - Hannover

17
18 DECELLULARIZED AORTIC VALVE ALLOGRAFTS CLINICAL DATA Study Period: Nov 2005 Sep 2018 Patients: n= 125 (High Risk Profile] Age: 47 ± 18,6 (min=0,1 max=81) Sex: Males = 82, Females =43 27 Concomitant Mitral Valve Disease ( Multiple Reoperations] 20 Ascending Aorta / Hemiarch Aneurysm 27 Bacterial Endocarditis 8 Coronary Artery Disease
19 Data n % Valvular Lesion Aortic Stenosis 46 36,8 Aortic Insufficiency Mixed Lesion 29 23,2 Etiology Rheumatic 18 14,4 Congenital 32 25,6 Degenerative 24 19,2 Prosthetic Valve Dysfunction 21 16,8 Endocarditis 28 22,4 Acute Aortic Dissection 1 0,8 Unknown 1 0,8 NYHA Classe Funcional I 9 7,2 II 69 55,2 III 39 31,2 IV 8 6,4 Operation Primary Reoperation 55 44
20 DECELLULARIZED AORTIC VALVE ALLOGRAFTS OPERATIVE DATA Surgical Technique Aortic Root Replacement in all patients Allograft Diameter 21,6 ±2,5 mm (min=6, max=28) Cross-Clamp Time 110,7±26,1min (min=60, max=215) Extracorporeal Circulation Time 141,4±45,4min (min=80, max=270)
21 DECELLULARIZED AORTIC VALVE ALLOGRAFTS POSTOPERATIVE EVALUATION Clinical Examination Echocardiography Before hospital discharge 6/12 months PO, annualy thereafter CT Scan MRI Follow-up Clinical Follow-up 106 patients (90,1% complete) Mean clinical follow-up time = 4,9 years (0,1 12,4)
22 DECELLULARIZED AORTIC VALVE ALLOGRAFTS RESULTS Early Mortality = 6.4% ( 8/125) Low Cardiac Output...4 Sepsis and Multiorgan Failure.. 2 Cardiogenic Shock...2
23 AVR WITH DECELLULARIZED AORTIC VALVE ALLOGRAFTS LATE SURVIVAL Survival (%) Early Death = 8 Late Death = % at 10 Years CI95% = (66.9% %) Time (Years) Patients at Risk (117) (93) (68) (50) (31) (13) (1)
24 DECELLULARIZED AORTIC VALVE ALLOGRAFTS CAUSES OF LATE DEATH (N=16) Sudden Death. 2 Pneumonia.2 Cancer....2 Brain Stroke..1 Acute Myocardial Infarction.. 2 Reoperation for CABG... 2 DVP Pulmonary Embolism Trauma Unknown.....3
25 RESULTS CLINICAL FOLLOW-UP Late Functional Status NYHA I - 91 patients NYHA II - 14 patients NYHA III - 1 patient NYHA IV 0 patient 2 cases of Thromboembolism No case of Bleeding 1 case of Bacterial Endocarditis Department of Cardiovascular Surgery Santa Casa de Curitiba- PUCPR
26 Peak Gradients (mmhg) DECELLULARIZED AOTIC VALVE ALLOGRAFTS EARLY AND LATE MAX INSTANTANEOUS GRADIENTS Mean Early Peak Gradients 11.6 ± 10.3 Mean Late Peak Gradients 9.6 ± 7, Time (Years)
27 Aortic Regurgitation (Number of Observations) DECELLULARIZED AORTIC VALVE ALLOGRAFTS AORTIC REGURGITATION None/Trivial Mild Moderate Severe Time (Years)
28 DECELLULARIZED AORTIC VALVE ALLOGRAFTS FREEDOM FROM MODERATE AR Freedom from > Moderate AR Events 1 Bacterial Endocardites 3 Cusps Prolapse * Time (years) Patients at Risk (108) (93) (68) (50) (31) (13) (1) 92.4% at 10 Years CI95% = (64.4% %)
29 DECELLULARIZED AORTIC VALVE ALLOGRAFTS REOPERATIONS(N=5) AR due to Healed Bacterial Endocarditis 1 Primary Cusp Prolapse *..3 Patient Outgrowth....1 * 1 PATIENT REOPERATED ELSEWHERE NO ECHO AVAILABLE SURGEON REPORT ONLY
30 DECELLULARIZED AORTIC VALVE ALLOGRAFTS FREEDOM FROM REOPERATION ON THE ALLOGRAFT Freedom from Reoperation Patients at Risk % at 10 Years CI95% = (75,9% %) Time (years) (117) (93) (68) (50) (31) (13) (1)

31



32 EXPLANTED AORTIC ALLOGRAFT 8 YEARS OF FOLLOW-UP AORTIC WALL Íntima Well preserved aortic wall Elastic fibers intact in vivo repopulation Endothelization Minimal Intimal Hyperplasia
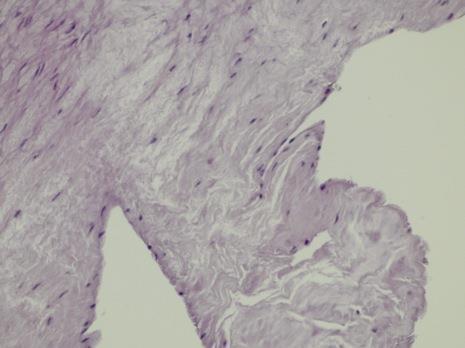
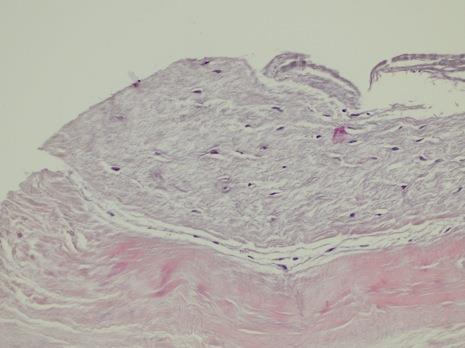
33 CUSP B VENTRICULARIS FREE MARGIN A FIBROSA CUSP INSERTION A B

34 Calcium Score (A) Decellularized Ao Allografts Calcium Score Time (years)


35 DECELLULARIZED AO VALVE ALLOGRAFTS CT SCAN EVALUATION CALCIUM SCORES - ABSENT OR MINIMAL CALCIFICATION ON CUSPS AND CONDUITS AT 8 YEARS OF FOLLOW-UP!!!!!


36 DECELLULARIZED AO VALVE ALLOGRAFTS CT SCAN EVALUATION CALCIUM SCORES - ABSENT OR MINIMAL CALCIFICATION ON CUSPS AND CONDUITS AT 7 YEARS OF FOLLOW-UP!!!!!

37 CT SCAN EVALUATION CALCIUM SCORES - DECELLULARIZED AO VALVE ALLOGRAFTS More Intense Calcification on the Aortic Wall Only at 9Years of Follow-up
38 CONCLUSIONS Decellularized Allografts have shown very promising results up to 12 years of follow-up. They are well incorporated to the host, with minimal inflammation and negligible immune reaction. They do not retract in the pulmonary circulation and do not dilate in the systemic side. Occasional biopsies have demonstrated partial repopulation of these grafts and minimal or absent calcification, even in children under the age of 12 years. These data demonstrate that decellularized allografts have, at least up to 10 years, better performance than conventional cryopreserved allografts and they are currently our graft of choice for patients at any age.

39 Contact: Francisco Diniz Affonso da Costa Phone: (55) / (55)
The Role Of Decellularized Valve Prostheses In The Young Patient
 The Role Of Decellularized Valve Prostheses In The Young Patient Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil Disclosures Ownership and patent license of the SDS decellularization
The Role Of Decellularized Valve Prostheses In The Young Patient Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil Disclosures Ownership and patent license of the SDS decellularization
Long-term results (22 years) of the Ross Operation a single institutional experience
 of the Ross Operation a single institutional experience") Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart van Putte, Nabil Saouti. St. Antonius Hospital, Nieuwegein, The Netherlands
 Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
Aortic root reconstructive surgery - new created technique for aortic stenosis
 Aortic root reconstructive surgery - new created technique for aortic stenosis Reconstructive surgery of the aortic root Academician d-r Zan Mitrev, T.Anguseva, E.Stoicovski, E Idoski Special hospital
Aortic root reconstructive surgery - new created technique for aortic stenosis Reconstructive surgery of the aortic root Academician d-r Zan Mitrev, T.Anguseva, E.Stoicovski, E Idoski Special hospital
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Outcome of elderly patients with severe but asymptomatic aortic stenosis
 Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S.
 CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
Unusual Causes of Aortic Regurgitation. Case 1
 Unusual Causes of Aortic Regurgitation Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA No Disclosures Case 1 54 year old female with h/o cerebral aneurysm and vascular malformation
Unusual Causes of Aortic Regurgitation Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA No Disclosures Case 1 54 year old female with h/o cerebral aneurysm and vascular malformation
Lessons From The Computer Model and How We Do Root Replacement
 Lessons From The Computer Model and How We Do Root Replacement Ehud Raanani, MD Cardiac Surgery Leviev Cardiothoracic and Vascular Center Sheba Medical Center Sackler School of Medicine, Tel Aviv University
Lessons From The Computer Model and How We Do Root Replacement Ehud Raanani, MD Cardiac Surgery Leviev Cardiothoracic and Vascular Center Sheba Medical Center Sackler School of Medicine, Tel Aviv University
Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension?
 Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension? Y d Udekem, J Siddiqui, C Seaman, I Konstantinov, J Galati, M Cheung, C Brizard Royal
Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension? Y d Udekem, J Siddiqui, C Seaman, I Konstantinov, J Galati, M Cheung, C Brizard Royal
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic,
 Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
Role of Sutureless Valves in the Surgeon s Armamentarium Prof. Dr Malakh Shrestha Vice Chair, Director of Aortic Surgery Cardiothoracic, transplantation and Vascular Surgery Hannover Medical School, Germany
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Indications and Late Results of Aortic Valve Repair
 Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Results of Aortic Valve Preservation and Repair
 Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval?
 Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Reconstructive surgery of the aortic root
 Reconstructive surgery of the aortic root Reconstructive surgery of the aortic root Academician d-r Zan Mitrev MDFETCS Special hospital for surgery Fillip II Skopje - Macedonia february, 2011 Reconstructive
Reconstructive surgery of the aortic root Reconstructive surgery of the aortic root Academician d-r Zan Mitrev MDFETCS Special hospital for surgery Fillip II Skopje - Macedonia february, 2011 Reconstructive
CLINICAL COMMUNIQUE 16 YEAR RESULTS
 CLINICAL COMMUNIQUE 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900 Introduction The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 6900, was introduced
CLINICAL COMMUNIQUE 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900 Introduction The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 6900, was introduced
Aortic valve repair: When and how to employ this novel approach?
 Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
The Early and Midterm Function of Decellularized Aortic Valve Allografts
 The Early and Midterm Function of Decellularized Aortic Valve Allografts Francisco D. A. da Costa, MD, Ana Claudia B. A. Costa, Roberta Prestes, Ana Carolina Domanski, MD, Eduardo Mendel Balbi, MD, Andreia
The Early and Midterm Function of Decellularized Aortic Valve Allografts Francisco D. A. da Costa, MD, Ana Claudia B. A. Costa, Roberta Prestes, Ana Carolina Domanski, MD, Eduardo Mendel Balbi, MD, Andreia
Clinical material and methods. Copyright by ICR Publishers 2003
 Fourteen Years Experience with the CarboMedics Valve in Young Adults with Aortic Valve Disease Jan Aagaard 1, Jens Tingleff 2, Per V. Andersen 1, Christel N. Hansen 2 1 Department of Cardio-Thoracic and
Fourteen Years Experience with the CarboMedics Valve in Young Adults with Aortic Valve Disease Jan Aagaard 1, Jens Tingleff 2, Per V. Andersen 1, Christel N. Hansen 2 1 Department of Cardio-Thoracic and
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
16 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900
 CLINICAL COMMUNIQUé 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 69 The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 69, was introduced into clinical
CLINICAL COMMUNIQUé 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 69 The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 69, was introduced into clinical
How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D.
 How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D. AATS International Cardiovascular Symposium 2017 Session 6: Technical Aspects of Open Surgery on the Aortic Valve Sao Paulo, Brazil
How to Perform a Valve Sparing Root Replacement Joseph S. Coselli, M.D. AATS International Cardiovascular Symposium 2017 Session 6: Technical Aspects of Open Surgery on the Aortic Valve Sao Paulo, Brazil
Autologous Pulmonary Valve Replacement of the Diseased Aortic Valve
 Autologous Pulmonary Valve Replacement of the Diseased Aortic Valve By L. GONZALEZ-LAvIN, M.D., M. GEENS. M.D., J. SOMERVILLE, M.D., M.R.C.P., ANm D. N. Ross, M.B., CH.B., F.R.C.S. SUMMARY Living tissue
Autologous Pulmonary Valve Replacement of the Diseased Aortic Valve By L. GONZALEZ-LAvIN, M.D., M. GEENS. M.D., J. SOMERVILLE, M.D., M.R.C.P., ANm D. N. Ross, M.B., CH.B., F.R.C.S. SUMMARY Living tissue
Update on the CoreValve Experience
 TCT Asia Pacific April 22-24, 2009 Update on the CoreValve Experience Eberhard Grube HELIOS Klinikum, Germany Instituto Dante Pazzanese de Cardiología, São Paulo, Brazil Stanford University, Palo Alto,
TCT Asia Pacific April 22-24, 2009 Update on the CoreValve Experience Eberhard Grube HELIOS Klinikum, Germany Instituto Dante Pazzanese de Cardiología, São Paulo, Brazil Stanford University, Palo Alto,
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
The Bicuspid AV Surgical Conisiderations
 The Bicuspid AV Surgical Conisiderations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University MAY 15, 2014 Homburg BAV Repair Congenital variations
The Bicuspid AV Surgical Conisiderations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University MAY 15, 2014 Homburg BAV Repair Congenital variations
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
RV- PA Surgical Valve Choices in Adults longevity and risks
 RV- PA Surgical Valve Choices in Adults longevity and risks ACHD, Queenstown, 2017 Adult Congenital Heart Surgery 1991 8/3/2017 Total = 751 Patients 200 180 160 140 120 100 80 60 40 20 0 Primary Diagnosis
RV- PA Surgical Valve Choices in Adults longevity and risks ACHD, Queenstown, 2017 Adult Congenital Heart Surgery 1991 8/3/2017 Total = 751 Patients 200 180 160 140 120 100 80 60 40 20 0 Primary Diagnosis
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Presenter Disclosure. Patrick O. Myers, M.D. No Relationships to Disclose
 Presenter Disclosure Patrick O. Myers, M.D. No Relationships to Disclose Aortic Valve Repair by Cusp Extension for Rheumatic Aortic Insufficiency in Children Long term Results and Impact of Extension Material
Presenter Disclosure Patrick O. Myers, M.D. No Relationships to Disclose Aortic Valve Repair by Cusp Extension for Rheumatic Aortic Insufficiency in Children Long term Results and Impact of Extension Material
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Aortic Valve Repair - Alternative to Replacement
 Aortic Valve Repair - Alternative to Replacement Seite 1 Dept. of Thoracic and Cardiovascular Surgery University Hospital of Saarland Homburg/ Saar Germany Seite 2 Aortic Valve - Historic Repair Attempts
Aortic Valve Repair - Alternative to Replacement Seite 1 Dept. of Thoracic and Cardiovascular Surgery University Hospital of Saarland Homburg/ Saar Germany Seite 2 Aortic Valve - Historic Repair Attempts
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504
 Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD
 2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve. Diana Aicher. September 16 th - 18 th 2015
 Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve Diana Aicher September 16 th - 18 th 2015 Why repair the aortic valve? Aortic Valve Replacement
Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve Diana Aicher September 16 th - 18 th 2015 Why repair the aortic valve? Aortic Valve Replacement
Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients
 Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients A Prospective, Multi-Center, Comparative Study Joseph S. Coselli, Irina V. Volguina, Scott A. LeMaire, Thoralf M. Sundt, Elizabeth
Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients A Prospective, Multi-Center, Comparative Study Joseph S. Coselli, Irina V. Volguina, Scott A. LeMaire, Thoralf M. Sundt, Elizabeth
The Bicuspid AV Surgical Considerations
 The Bicuspid AV Surgical Considerations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University September 12, 2014 Homburg BAV Repair Congenital variations
The Bicuspid AV Surgical Considerations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University September 12, 2014 Homburg BAV Repair Congenital variations
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes
 Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications
 24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Aortic Valve Repair a Modular and Geometric Approach. H.-J. Schäfers Dept. of Thoracic and Cardiovascular Surgery University Hospital of Saarland
 Aortic Valve Repair a Modular and Geometric Approach H.-J. Schäfers Dept. of Thoracic and Cardiovascular Surgery University Hospital of Saarland 12.09.2018 Limitations: Purely echocardiographic, does not
Aortic Valve Repair a Modular and Geometric Approach H.-J. Schäfers Dept. of Thoracic and Cardiovascular Surgery University Hospital of Saarland 12.09.2018 Limitations: Purely echocardiographic, does not
Results of Transapical Valves. A.P. Kappetein Dept Cardio-thoracic surgery
 Results of Transapical Valves A.P. Kappetein Dept Cardio-thoracic surgery Rotterda am, The Netherlands 2002 FIM 2003 2005 2006 2010 THV THV Cribier-Edwards Edwards Edwards Sapien Sapien XT Bovine pericardium
Results of Transapical Valves A.P. Kappetein Dept Cardio-thoracic surgery Rotterda am, The Netherlands 2002 FIM 2003 2005 2006 2010 THV THV Cribier-Edwards Edwards Edwards Sapien Sapien XT Bovine pericardium
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Valve Disease. Valve Surgery. Total Volume. In 2016, Cleveland Clinic surgeons performed 3039 valve surgeries.
 Valve Surgery Total Volume 1 1 Volume 35 3 5 15 1 5 1 13 1 N = 773 5 79 15 93 1 339 In 1, surgeons performed 339 valve surgeries. surgeons have implanted more than 1, bioprosthetic aortic valves since
Valve Surgery Total Volume 1 1 Volume 35 3 5 15 1 5 1 13 1 N = 773 5 79 15 93 1 339 In 1, surgeons performed 339 valve surgeries. surgeons have implanted more than 1, bioprosthetic aortic valves since
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
The Dilated Pulmonary Artery: Is there a risk of Dissection?
 The Dilated Pulmonary Artery: Is there a risk of Dissection? Pastora Gallego, MD, PhD Inter-center Adult Congenital Heart Disease Unit Area del Corazón Seville, Spain No conflict of interest to disclose
The Dilated Pulmonary Artery: Is there a risk of Dissection? Pastora Gallego, MD, PhD Inter-center Adult Congenital Heart Disease Unit Area del Corazón Seville, Spain No conflict of interest to disclose
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
ρ = 4(νp)2 Scale -200 to 200 V = m/s Grad = 34 mmhg V = 1.9 m/s Grad = 14 mmhg Types
2 Scale -200 to 200 V = m/s Grad = 34 mmhg V = 1.9 m/s Grad = 14 mmhg Types") Pre and Post Operative Evaluation of the Aorta and Aortic Valve Andrew J. Bierhals, MD The Pre and Post-Operative Evaluation of the Aorta and Aortic Valve Andrew Bierhals, MD, MPH Mallinckrodt Institute
Pre and Post Operative Evaluation of the Aorta and Aortic Valve Andrew J. Bierhals, MD The Pre and Post-Operative Evaluation of the Aorta and Aortic Valve Andrew Bierhals, MD, MPH Mallinckrodt Institute
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
A Loeys-Dietz Patient with a Trans-Atlantic Odyssey. Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4
 1 2 3 A Loeys-Dietz Patient with a Trans-Atlantic Odyssey Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4 5 6 7 8 9 Thierry Carrel 1, Florian Schoenhoff 1 and Duke Cameron
1 2 3 A Loeys-Dietz Patient with a Trans-Atlantic Odyssey Repeated Aortic Root Surgery ending with a Huge Left Main Coronary Aneurysm 4 5 6 7 8 9 Thierry Carrel 1, Florian Schoenhoff 1 and Duke Cameron
Iatrogenic pathology of the heart:
 Iatrogenic pathology of the heart: Complications of mitral valve plasty and replacement Patrick Bruneval D pt of Pathology Hôpital Européen Georges Pompidou Enterprise Interest None Mitral valve surgery
Iatrogenic pathology of the heart: Complications of mitral valve plasty and replacement Patrick Bruneval D pt of Pathology Hôpital Européen Georges Pompidou Enterprise Interest None Mitral valve surgery
DECLARATION OF CONFLICT OF INTEREST. No disclosures
 DECLARATION OF CONFLICT OF INTEREST No disclosures Congenital Aortic Valve Disease and Aortopathy: Recent Advances Sub- and Supravalvular Aortic Stenosis Westfälische Wilhelms-Universität Münster Helmut
DECLARATION OF CONFLICT OF INTEREST No disclosures Congenital Aortic Valve Disease and Aortopathy: Recent Advances Sub- and Supravalvular Aortic Stenosis Westfälische Wilhelms-Universität Münster Helmut
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kang D-H, Kim Y-J, Kim S-H, et al. Early surgery versus conventional
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kang D-H, Kim Y-J, Kim S-H, et al. Early surgery versus conventional
THE FOLDING LEAFLET. Rafael García Fuster. Cardiac Surgery Department University General Hospital of Valencia
 THE FOLDING LEAFLET Rafael García Fuster Cardiac Surgery Department University General Hospital of Valencia School of Medicine Catholic University of Valencia San Vicente Mártir SPAIN Carpentier s principles
THE FOLDING LEAFLET Rafael García Fuster Cardiac Surgery Department University General Hospital of Valencia School of Medicine Catholic University of Valencia San Vicente Mártir SPAIN Carpentier s principles
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Aortic valve reconstruction using the Ozaki technique, when and in whom? Mr Cesare Quarto MD PhD Consultant Cardiac Surgeon Royal Brompton Hospital
 Aortic valve reconstruction using the Ozaki technique, when and in whom? Mr Cesare Quarto MD PhD Consultant Cardiac Surgeon Royal Brompton Hospital London Disclosure of Interest Cesare Quarto I have the
Aortic valve reconstruction using the Ozaki technique, when and in whom? Mr Cesare Quarto MD PhD Consultant Cardiac Surgeon Royal Brompton Hospital London Disclosure of Interest Cesare Quarto I have the
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
Dr.ssa Loredana Iannetta. Centro Cardiologico Monzino
 Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Department of Cardiothoracic Surgery, Heart and Lung Center, Lund University Hospital, Lund, Sweden
 Long-Term Outcome of the Mitroflow Pericardial Bioprosthesis in the Elderly after Aortic Valve Replacement Johan Sjögren, Tomas Gudbjartsson, Lars I. Thulin Department of Cardiothoracic Surgery, Heart
Long-Term Outcome of the Mitroflow Pericardial Bioprosthesis in the Elderly after Aortic Valve Replacement Johan Sjögren, Tomas Gudbjartsson, Lars I. Thulin Department of Cardiothoracic Surgery, Heart
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
Transcatheter aortic valve implantation and pre-procedural risk assesment
 Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
VALVULAR HEART DISEASE
 VALVULAR HEART DISEASE Stenosis: failure of a valve to open completely, obstructing forward flow. - almost always due to a chronic process (e.g., calcification or valve scarring). Insufficiency : failure
VALVULAR HEART DISEASE Stenosis: failure of a valve to open completely, obstructing forward flow. - almost always due to a chronic process (e.g., calcification or valve scarring). Insufficiency : failure
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Quantitation of Aortic Regurgitation ASCeXAM / ReASCE Review Course
 Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Death is a Distant Rumor to the Young: The Bicuspid Aortic Valve. Hector I. Michelena, MD Assistant Professor of Medicine NO DISCLOSURES
 Death is a Distant Rumor to the Young: The Bicuspid Aortic Valve Hector I. Michelena, MD Assistant Professor of Medicine NO DISCLOSURES Leonardo s notes Royal collection, Queen Elizabeth II Leonardo s
Death is a Distant Rumor to the Young: The Bicuspid Aortic Valve Hector I. Michelena, MD Assistant Professor of Medicine NO DISCLOSURES Leonardo s notes Royal collection, Queen Elizabeth II Leonardo s
EACTS Adult Cardiac Database
 EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
Ascending Thoracic Aorta: Postsurgical CT Evaluation
 Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martinez Jimenez, MD GOALS Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martínez MD smartinez-jimenez@saint-lukes.org Saint
Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martinez Jimenez, MD GOALS Ascending Thoracic Aorta: Postsurgical CT Evaluation Santiago Martínez MD smartinez-jimenez@saint-lukes.org Saint
Hypoplasia of the aortic root1 The problem of aortic valve replacement
 Hypoplasia of the aortic root1 The problem of aortic valve replacement ROWAN NICKS, T. CARTMILL, and L. BERNSTEIN Department of Cardio-thoracic Surgery and the Hallstrom Institute of Cardiology, the Royal
Hypoplasia of the aortic root1 The problem of aortic valve replacement ROWAN NICKS, T. CARTMILL, and L. BERNSTEIN Department of Cardio-thoracic Surgery and the Hallstrom Institute of Cardiology, the Royal
Aortic Regurgitation in Connective Tissue Disorders Special precautions? Carlos A. Mestres MD PhD FETCS
 Aortic Regurgitation in Connective Tissue Disorders Special precautions? Carlos A. Mestres MD PhD FETCS Senior Consultant Department of Cardiovascular Surgery University Hospital Zürich (Switzerland) Extraordinary
Aortic Regurgitation in Connective Tissue Disorders Special precautions? Carlos A. Mestres MD PhD FETCS Senior Consultant Department of Cardiovascular Surgery University Hospital Zürich (Switzerland) Extraordinary
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
In contrast to aortic stenosis, which essentially has 3
 Valvular Heart Disease Causes of Pure Aortic Regurgitation in Patients Having Isolated Aortic Valve Replacement at a Single US Tertiary Hospital (1993 to 2005) William Clifford Roberts, MD; Jong Mi Ko,
Valvular Heart Disease Causes of Pure Aortic Regurgitation in Patients Having Isolated Aortic Valve Replacement at a Single US Tertiary Hospital (1993 to 2005) William Clifford Roberts, MD; Jong Mi Ko,
Bicuspid Aortic Valve: Only Valvular Disease? Artur Evangelista
 Bicuspid Aortic Valve: Only Valvular Disease? Artur Evangelista Bicuspid aortic valve BAV is not only a valvulogenesis disorder but also represent coexisting aspects of a genetic disorder of the aorta
Bicuspid Aortic Valve: Only Valvular Disease? Artur Evangelista Bicuspid aortic valve BAV is not only a valvulogenesis disorder but also represent coexisting aspects of a genetic disorder of the aorta
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular