DECLARATION OF CONFLICT OF INTEREST. No disclosures
|
|
|
- Ilene Robertson
- 5 years ago
- Views:
Transcription
1 DECLARATION OF CONFLICT OF INTEREST No disclosures





2 Congenital Aortic Valve Disease and Aortopathy: Recent Advances Sub- and Supravalvular Aortic Stenosis Westfälische Wilhelms-Universität Münster Helmut Baumgartner Adult Congenital and Valvular Heart Disease Center University of Muenster Germany
3 Subaortic Stenosis Operated or unoperated - up to 6% of pts. seen in ACHD clinics Frequently (up to 60%) associated with other lesions: VSD AVSD Coarctation of the aorta Shone syndrome (coarctation, parachute MV, supravalv. mitral ring)
4 Subaortic Stenosis - Pediatric Considerations Acquired heart disease usually not present at birth but appears after first year of life (anatomic precursor + genetic?) Observation of rapid progression and increasing presence and severity of AR Early surgery even in mild disease? Brauner R at al J Am Coll Cardiol 1997;30:1835 However, progression varies widely and in particular mild disease frequently progresses slowly; less effect of surgery on AV disease than originally thought Coleman DM et al J Am Coll Cardiol 1994;24:1558 More conservative in mild subaortic stenosis (gradient < 30mmHg) Gersony WM J Am Coll Cardiol 2001
5 Subaortic Stenosis - Recurrence After Surgery Overall recurrence rate 15-27% More frequent in fibromuscular than in discrete (membranous) SAS Re-operation rate 12-20% Recurrence rate depends on Surgical technique Extent of obstruction relief at operation Residual gradient 30mmHg -> high risk of recurrence
6 Subaortic Stenosis - Recurrence After Surgery Risk factors for reoperation after repair for discrete subaortic stenosis Geva A et al J Am Coll Cardiol 2007;50: < 6mm distance between AoV and obstruction HR 5.1 Peak gradient by Doppler 60mmHg HR 4.2 Peeling of membrane from Ao or MV
7 Adult Patients with Subaortic Stenosis Not diagnosed during childhood Recognized but not operated on during childhood Residual obstruction after surgery during childhood Recurrent obstruction after surgery during childhood Aortic valve disease (regurgitation)

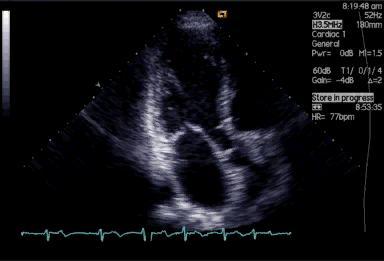
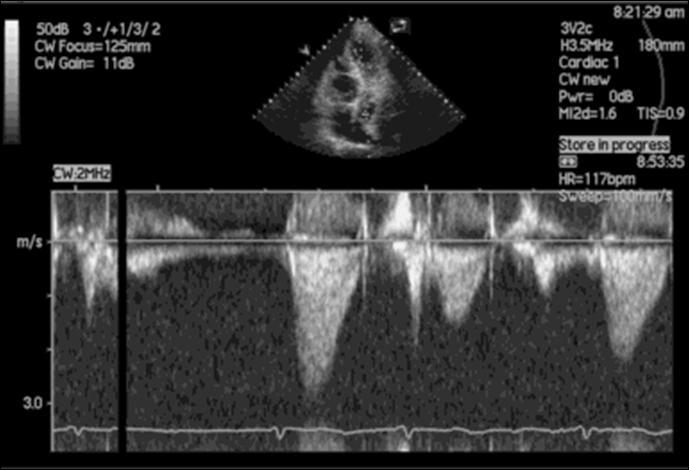
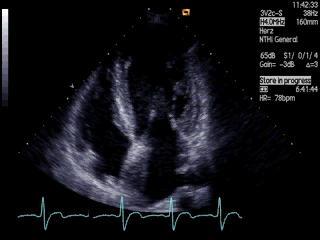
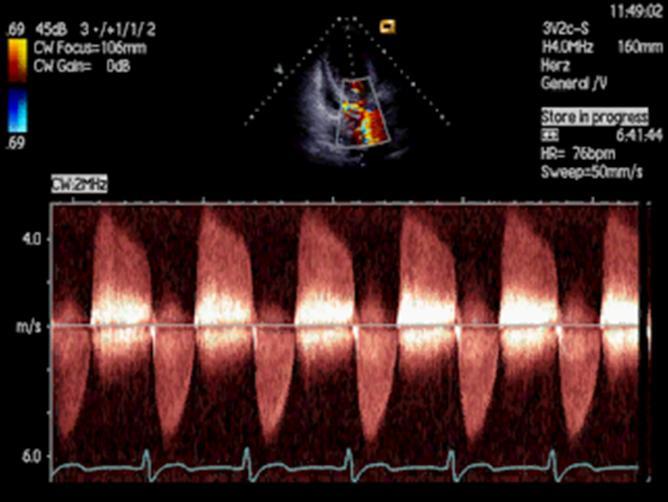
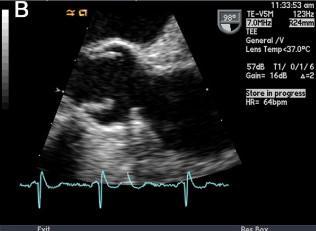
8 Echo Diagnosis
9 Subaortic Stenosis - When to (re)-intervene? Symptoms related to (re)stenosis -> mean gradient expected > 50mmHg reduced exercise capacity shortness of breath angina diziness, syncope Severe aortic valve disease (AR) Surgery in symptomatic pts. and asymptomatic pts. + LV enlargement and/or LVEF < 50%
10 Subaortic Stenosis - When to (re)-intervene? Asymptomatic pt. (without severe AR) - PROGNOSTIC CONSIDERATIONS Consequences for aortic valve (AR) Consequences of LVOT obstruction with pressure load for LV LVH LV myocardial fibrosis Arrhythmias LV dysfunction Sudden death

11 Subaortic Stenosis - When to (re)-intervene? Consequences of LVOT obstruction with pressure load for LV LVH LV myocardial fibrosis Arrhythmias LV-dysfunction Sudden death Pts. with unusually profound LVH (unproportional to stenosis cardiomyopathy?) LVH regression after surgery

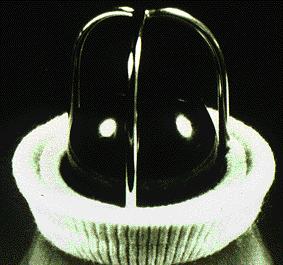
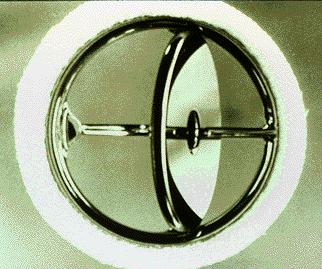

12 HEART VALVE PROSTHESES
13 Subaortic Stenosis - When to (re)-intervene? (Re)-intervention in asymptomatic patients: AV considerations (AR)



14 JET DAMAGE
15 Subaortic Stenosis - When to (re)-intervene? (Re)-intervention in asymptomatic patients: AV considerations (AR)
16 Discrete Subaortic Stenosis in Adults Oliver JM et al J Am Coll Cardiol 2001;38: pts. (31 ± 17yrs, 64 females) 6.5% of pts. with CHD at study period Group A (N=29) surgery during adult life Group B (N=64) unoperated Group C (N=41) surgery < 15 years of age Age A: 56±15 yrs B: 27±13 yrs C: 21±4 yrs Associated lesions (VSD, AVSD, CoA a.o.) A: 7% B: 64% C: 44%
17 LVOTO (mmhg) Discrete Subaortic Stenosis in Adults Oliver JM et al J Am Coll Cardiol 2001;38: pts. with 2 exams, average interval 4.8±1.8 yrs Gradient increase 7.6±14mmHg; 2.3±4.7mmHg/yr Age 50 yrs Age < 50 yrs P = 0.01 Initial Follow-up P = NS Initial Follow-up
18 AR (Percent) AR Degree Mean ± SD Discrete Subaortic Stenosis in Adults Oliver JM et al J Am Coll Cardiol 2001;38: Presence and degree of AR in with (C) and without surgery during childhood (A+B) P = Group C Group A+B Group C Group A+B N=41 N=93 N=41 N=93 trace to mild mild to moderate moderate to severe 0 -
19 AR Degree Discrete Subaortic Stenosis in Adults Oliver JM et al J Am Coll Cardiol 2001;38: pts. with 2 exams, average interval 4.8±1.8 yrs Change in AR degree over time 1.3±.8 1.5± P = = trace to mild 2 = mild to moderate 3 = moderate to severe ± 0.8 Baseline 1.5± 0.9 Follow-up AR degree sign. related to LVOTO (p <.001) but not age (p =.055) 4 pts. with endocarditis!
20 Discrete Subaortic Stenosis in Adults Oliver JM et al J Am Coll Cardiol 2001;38: Prevalence is increasing (greater number of repaired CHD) LVOTO increases but very slowly, particularly at age < 50 years Average age for surgical repair > 50 years AR is very common but rarely hemodynamically significant AR shows usually little progression over time AR is more prominent in pts. after surgery
21 Subaortic Stenosis and AR Surgical relief of LVOTO improves AR Serraf A et al J Thrac Cardiovasc Surg 1999;117:669 Progression in severtiy of AR not significantly different in surgical and nonsurgical groups Giuffre RM et al Adv Ther 2004;21:322-8 No substantial change in AR during follow-up after surgery Stassano P et al Thorac Cardiov Surg 2005 Late worsening of AR related to initial gradient (>30mmHg) Karamlou T et al Ann Thorac Surg 2007:84 Predictors: small distance to AV, higher gradient, peeling of the membrane from the AV Geva A et al J Am Coll Cardiol 2007:50 Surgery did not have impact on the incidence and severity of AR Drolet Ch et al Can J Cardiol 2011:27

22 Baumgartner H et al Eur Heart J 2011
23



24 Patel B et al J Am Coll Cardiol 2010;56

25 Salahuddin S et al Heart 2010;96:1808


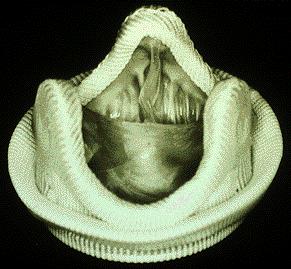
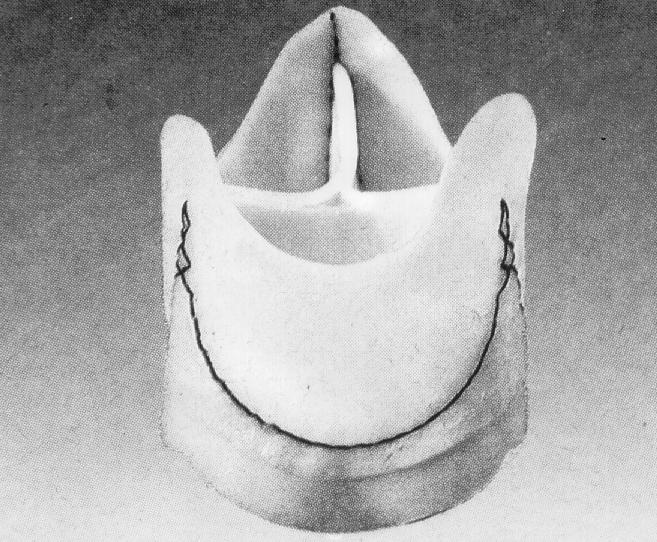
26 Supravalvular AS By far rarest obstructive lesion of the LVOT Histology: diseased media with an increased collagen content and reduced elastic tissue in the form of broken and disorganized elastin fibers (elastin arteriopathy) normal Aorta thickening irregular arrangement of elastic lamellae Stamm C et al Eur J Cardio-thoracic Surg
27 Supravalvular AS (SVAS) SVAS associated with Williams syndrome SVAS as inherited, autosomal dominant familial form without the nonvascular features of Williams syndrome -> elastin gene deleted or disrupted ± neighboring genes Sporadic cases of isolated SVAS hemizygous microdeletion on chromosome 7q11.23 identified in all three



28 Supravalvular AS (SVAS) Abnormalities of the AV in up to 50% In appr. 30% entire ascendig aorta, sometimes arch Obstruction of the pulmonary vasculature in up to 83% (all three forms of SVAS) Coronary arteries: - adhesion of the cusp leaflet edge to the narrowed STJ - obstr. by thickened aortic wall - high pressure -> premature arteriosclerosis Stamm C et al Eur J Cardio-thoracic Surg
29 Supravalvular AS (SVAS) Other Associated Lesions Aortic coarctation Patent ductus arteriosus Atrial septal defect Ventricular septal defect Tetralogy of Fallot Mitral valve abnormalities (elastin defect??)



30 Stamm C et al Eur J Cardio-thoracic Surg Aortic Regurgitation Kaushal et al Ann Thorac Surg 2010
31 Cardiac Outcomes in Adults With Supravalvular Aortic Stenosis (SVAS) Greutmann M, Tobler D, Sharma NC, Mebus S, Schuler P, Beauchesne L, Salehian O, Hoffmann A, Oechslin EN, Silversides CK. ESC ACHD centers N = 113 >18yrs Cardiac Events: CV death, SVT/VT >30s, ACS, Stroke, new onset CHF, endocarditis Surgery during adulthood Age at 1 st visit: 20 ± 4 yrs Williams-Beuren Syndrome 55% SVAS surgry during childhood 67% Multiple operations 34% NYHA II 8% RBBB 11% 16mmHg residual peak P 45% 50mmHg residua peak P 6% > mild AS / > mild AR 10/10% > mild MS / > mild MR 3/4%
32 Cardiac Outcomes in Adults With Supravalvular Aortic Stenosis (SVAS) Greutmann M, Tobler D, Sharma NC, Mebus S, Schuler P, Beauchesne L, Salehian O, Hoffmann A, Oechslin EN, Silversides CK. ESC ACHD centers N = 113 >18yrs Cardiac Events: CV death, SVT/VT >30s, ACS, Stroke, new onset CHF, endocarditis Surgery during adulthood Age at 1 st visit: 20 ± 4 yrs Williams-Beuren Syndrome 55% SVAS surgry during childhood 67% Multiple operations 34% NYHA II 8% RBBB 11% 16mmHg residual peak P 45% 50mmHg residua peak P 6% > mild AS / > mild AR 10/10% > mild MS / > mild MR 3/4% (more likely in WBS) (less likely in WBS)
33 Cardiac Outcomes in Adults With Supravalvular Aortic Stenosis (SVAS) Greutmann M, Tobler D, Sharma NC, Mebus S, Schuler P, Beauchesne L, Salehian O, Hoffmann A, Oechslin EN, Silversides CK. ESC 2011 Follow-up of 96 pts. median FU 6 yrs (0.1 30yrs) 20 events: - death 2 - SVT / VT 8 (7/3) - new onset CHF 7 - endocarditis 2 - stroke 1 Surgery - AVR 5 - SVAS repair 4 - PVI 1 - LV assist device 1 Predictors of events: multiple surgery, NYHA II, sign. MV disease Predictors of surgery: BWS, RBBB, >50mmHg gradient

34 Baumgartner H et al Eur Heart J 2011
35
36 Balloon Dilatation in Discrete Subaortic Stenosis Feasibilty shown (gradient reduction, no increase in AR) Very small patient numbers Residual gradient of concern No sufficient follow-up Rao PS et al J Invasive Cardiol 1990;2:65-71 Sharma S et al J Interv Cardiol 1991;4:105-9 Moskowitz WB et al J Invasive Cardiol 1999;11:116-20
The Bicuspid Aortic Valve: New Frontiers in Genetics and Interventions
 The Bicuspid Aortic Valve: New Frontiers in Genetics and Interventions Westfälische Wilhelms-Universität Münster Helmut Baumgartner Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
The Bicuspid Aortic Valve: New Frontiers in Genetics and Interventions Westfälische Wilhelms-Universität Münster Helmut Baumgartner Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
RVOTO adult and post-op
 Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Left Ventricular Outflow Tract Obstruction
 Left Ventricular Outflow Tract Obstruction Department of Paediatrics Left Ventricular Outflow Tract Obstruction Subvalvular aortic stenosis Aortic Stenosis Supravalvular aortic stenosis Aortic Coarctation
Left Ventricular Outflow Tract Obstruction Department of Paediatrics Left Ventricular Outflow Tract Obstruction Subvalvular aortic stenosis Aortic Stenosis Supravalvular aortic stenosis Aortic Coarctation
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Pulmonary Hypertension: Follow-up in adolescence and adults
 Pulmonary Hypertension: Follow-up in adolescence and adults Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of Muenster Germany
Pulmonary Hypertension: Follow-up in adolescence and adults Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of Muenster Germany
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT
 LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT 10-13 March 2017 Ritz Carlton, Riyadh, Saudi Arabia Zohair AlHalees, MD Consultant, Cardiac Surgery Heart Centre LEFT VENTRICULAR
LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT 10-13 March 2017 Ritz Carlton, Riyadh, Saudi Arabia Zohair AlHalees, MD Consultant, Cardiac Surgery Heart Centre LEFT VENTRICULAR
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Adult Congenital Heart Disease T S U N ` A M I!
 Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
Adult Congenital Heart Disease
 Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
MEDICAL SCIENCES Vol.I -Adult Congenital Heart Disease: A Challenging Population - Khalid Aly Sorour
 ADULT CONGENITAL HEART DISEASE: A CHALLENGING POPULATION Khalid Aly Sorour Cairo University, Kasr elaini Hospital, Egypt Keywords: Congenital heart disease, adult survival, specialized care centers. Contents
ADULT CONGENITAL HEART DISEASE: A CHALLENGING POPULATION Khalid Aly Sorour Cairo University, Kasr elaini Hospital, Egypt Keywords: Congenital heart disease, adult survival, specialized care centers. Contents
Unusual Causes of Aortic Regurgitation. Case 1
 Unusual Causes of Aortic Regurgitation Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA No Disclosures Case 1 54 year old female with h/o cerebral aneurysm and vascular malformation
Unusual Causes of Aortic Regurgitation Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA No Disclosures Case 1 54 year old female with h/o cerebral aneurysm and vascular malformation
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
Management of Heart Failure in Adult with Congenital Heart Disease
 Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Most common fetal cardiac anomalies
 Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Arterial Switch Operation Long-term outcomes - all good? Daniel Tobler Adult congenital heart disease University Hospital Basel
 Arterial Switch Operation Long-term outcomes - all good? Daniel Tobler Adult congenital heart disease University Hospital Basel www.chd-diagrams.com Arterial Switch Operation Long-term outcomes - all good?
Arterial Switch Operation Long-term outcomes - all good? Daniel Tobler Adult congenital heart disease University Hospital Basel www.chd-diagrams.com Arterial Switch Operation Long-term outcomes - all good?
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
When should we intervene surgically in pediatric patient with MR?
 When should we intervene surgically in pediatric patient with MR? DR.SAUD A. BAHAIDARAH CONSULTANT, PEDIATRIC CARDIOLOGY ASSISTANT PROFESSOR OF PEDIATRICS HEAD OF CARDIOLOGY AND CARDIAC SURGERY UNIT KAUH
When should we intervene surgically in pediatric patient with MR? DR.SAUD A. BAHAIDARAH CONSULTANT, PEDIATRIC CARDIOLOGY ASSISTANT PROFESSOR OF PEDIATRICS HEAD OF CARDIOLOGY AND CARDIAC SURGERY UNIT KAUH
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
The Role of Imaging in Transcatheter Aortic Valve Implantation
 The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
TGA, VSD, and LVOTO. Cheul Lee, MD. Department of Thoracic and Cardiovascular Surgery Sejong General Hospital
 Surgical Management of TGA, VSD, and LVOTO Cheul Lee, MD Department of Thoracic and Cardiovascular Surgery Sejong General Hospital TGA, VSD, and LVOTO Incidence : 0.7% of all CHD 20% of TGA with VSD 4%
Surgical Management of TGA, VSD, and LVOTO Cheul Lee, MD Department of Thoracic and Cardiovascular Surgery Sejong General Hospital TGA, VSD, and LVOTO Incidence : 0.7% of all CHD 20% of TGA with VSD 4%
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Transposition of the great arteries
 EuroEcho 2010 - Teaching course on CHD Transposition of the great arteries - Follow-up after the arterial switch Gertjan Tj. Sieswerda, MD PhD Nothing to disclose Interuniversitary Institute for Congenital
EuroEcho 2010 - Teaching course on CHD Transposition of the great arteries - Follow-up after the arterial switch Gertjan Tj. Sieswerda, MD PhD Nothing to disclose Interuniversitary Institute for Congenital
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Arrhythmias in Adult Congenital Heart Disease
 Arrhythmias in Adult Congenital Heart Disease NAAMA s 24 th International Medical Convention Beirut, Lebanon June 26 July 2, 2010 Naser Ammash, MD Mayo School of Medicine Rochester, Minnesota CP1212391-1
Arrhythmias in Adult Congenital Heart Disease NAAMA s 24 th International Medical Convention Beirut, Lebanon June 26 July 2, 2010 Naser Ammash, MD Mayo School of Medicine Rochester, Minnesota CP1212391-1
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
The Dilated Pulmonary Artery: Is there a risk of Dissection?
 The Dilated Pulmonary Artery: Is there a risk of Dissection? Pastora Gallego, MD, PhD Inter-center Adult Congenital Heart Disease Unit Area del Corazón Seville, Spain No conflict of interest to disclose
The Dilated Pulmonary Artery: Is there a risk of Dissection? Pastora Gallego, MD, PhD Inter-center Adult Congenital Heart Disease Unit Area del Corazón Seville, Spain No conflict of interest to disclose
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
What is the Definition of Small Systemic Ventricle. Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University
 What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Debate in CHD - When Should We
 Debate in CHD - When Should We Replace Pulmonary Valve? Lee, Jae Young Dept. of Pediatrics, Seoul Saint Mary s Hospital The Catholic University of Korea 14 yr/m, TOF repair (1yr) FC I PR Fraction - 48
Debate in CHD - When Should We Replace Pulmonary Valve? Lee, Jae Young Dept. of Pediatrics, Seoul Saint Mary s Hospital The Catholic University of Korea 14 yr/m, TOF repair (1yr) FC I PR Fraction - 48
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Reoperation for Left Ventricular Outflow Tract Obstruction After Repair of Atrioventricular Septal Defect
 Reoperation for Left Ventricular Outflow Tract Obstruction After Repair of Atrioventricular Septal Defect David M. Overman Division of Pediatric Cardiac Surgery The Children s Heart Clinic Chief, Division
Reoperation for Left Ventricular Outflow Tract Obstruction After Repair of Atrioventricular Septal Defect David M. Overman Division of Pediatric Cardiac Surgery The Children s Heart Clinic Chief, Division
What is the Role of Surgical Repair in 2012
 What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Surgical Management of TOF in Adults. Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital
 Surgical Management of TOF in Adults Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital Tetralogy of Fallot (TOF) in Adults Most common cyanotic congenital heart
Surgical Management of TOF in Adults Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital Tetralogy of Fallot (TOF) in Adults Most common cyanotic congenital heart
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Management of complex CHD in adults
 Management of complex CHD in adults Victor Tsang Society of Thoracic Surgeons of Thailand 2016 The impact of infant cardiac surgery Over 90 % of infants born with CHD will reach adulthood By 2010, adults
Management of complex CHD in adults Victor Tsang Society of Thoracic Surgeons of Thailand 2016 The impact of infant cardiac surgery Over 90 % of infants born with CHD will reach adulthood By 2010, adults
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
LOW-FLOW LOW-GRADIENT PULMONARY STENOSIS IN REPAIRED TOF: FACT OR FICTION?
 LOW-FLOW LOW-GRADIENT PULMONARY STENOSIS IN REPAIRED TOF: FACT OR FICTION? Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Comgenital and Valvular Heart Disease Deptartment
LOW-FLOW LOW-GRADIENT PULMONARY STENOSIS IN REPAIRED TOF: FACT OR FICTION? Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Comgenital and Valvular Heart Disease Deptartment
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
Follow-up after VSD closure- what to look for?
 The 3rd Congress of Congenital heart disease Ventricular Septal Defect from A-Z January 9-11. 2013, Ho Chi Minh City, Vietnam Follow-up after VSD closure- what to look for? Nina Wunderlich University Hospital
The 3rd Congress of Congenital heart disease Ventricular Septal Defect from A-Z January 9-11. 2013, Ho Chi Minh City, Vietnam Follow-up after VSD closure- what to look for? Nina Wunderlich University Hospital
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve
 Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Management of HOCM: Non-Surgical Options
 Management of HOCM: Non-Surgical Options Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology Director,
Management of HOCM: Non-Surgical Options Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology Director,
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Research Presentation June 23, Nimish Muni Resident Internal Medicine
 Research Presentation June 23, 2009 Nimish Muni Resident Internal Medicine Research Question In adult patients with repaired Tetralogy of Fallot, how does Echocardiography compare to MRI in evaluating
Research Presentation June 23, 2009 Nimish Muni Resident Internal Medicine Research Question In adult patients with repaired Tetralogy of Fallot, how does Echocardiography compare to MRI in evaluating
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
Dr.ssa Loredana Iannetta. Centro Cardiologico Monzino
 Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Changing Profile of Adult Congenital Heart Disease
 Congenital Heart Disease New Developments for the General Cardiologist Changing Profile of Adult Congenital Heart Disease European Society of Cardiology August 27, 2012 Ariane Marelli MD, FRCP, FACC, MPH
Congenital Heart Disease New Developments for the General Cardiologist Changing Profile of Adult Congenital Heart Disease European Society of Cardiology August 27, 2012 Ariane Marelli MD, FRCP, FACC, MPH
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death
 Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
The Role Of Decellularized Valve Prostheses In The Young Patient
 The Role Of Decellularized Valve Prostheses In The Young Patient Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil Disclosures Ownership and patent license of the SDS decellularization
The Role Of Decellularized Valve Prostheses In The Young Patient Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil Disclosures Ownership and patent license of the SDS decellularization
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Coarctation of the Aorta
 Interventional Management of Coarctation of the Aorta Lee Benson MD Professor Pediatrics (Cardiology) Director, Cardiac Diagnostic & Interventional Unit The Hospital for Sick Children Toronto, Canada Outline
Interventional Management of Coarctation of the Aorta Lee Benson MD Professor Pediatrics (Cardiology) Director, Cardiac Diagnostic & Interventional Unit The Hospital for Sick Children Toronto, Canada Outline
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Aortic valve Stenosis: Insights in the evaluation of LV function. Erwan DONAL Cardiologie CHU Rennes
 Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Pulmonary Valve Replacement
 Pulmonary Valve Replacement Christian Kreutzer MD Hospital Nacional Alejandro Posadas Hospital Universitario Austral (No disclosures) Scope of the problem. CHD with PS or PA require a RVOT procedure. Tetralogy
Pulmonary Valve Replacement Christian Kreutzer MD Hospital Nacional Alejandro Posadas Hospital Universitario Austral (No disclosures) Scope of the problem. CHD with PS or PA require a RVOT procedure. Tetralogy
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
European CMR Certification: LIST OF PROCEDURES FORM
 European CMR Certification: LIST OF PROCEDURES FORM Application for: Level 2 Level 3 Candidate is requested to submit a list of 150 (Level 2) or 300 (Level 3) studies reported by her/him as detailed in
European CMR Certification: LIST OF PROCEDURES FORM Application for: Level 2 Level 3 Candidate is requested to submit a list of 150 (Level 2) or 300 (Level 3) studies reported by her/him as detailed in
Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension?
 Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension? Y d Udekem, J Siddiqui, C Seaman, I Konstantinov, J Galati, M Cheung, C Brizard Royal
Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension? Y d Udekem, J Siddiqui, C Seaman, I Konstantinov, J Galati, M Cheung, C Brizard Royal