Disclosures Nothing to disclose
|
|
|
- Silvia Harrell
- 6 years ago
- Views:
Transcription


1 Aortic Valve Disease Illustrative Cases December 8, 2009 David Stultz, MD, FACC Southwest Cardiology, Inc Handout available at
2 Disclosures Nothing to disclose
3 Objectives Understand the use of echocardiography to assess aortic valve disease Apply clinical guidelines to management of aortic valve disease


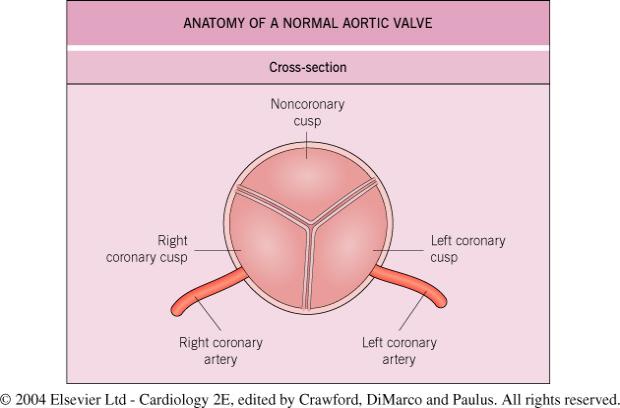
4 Aortic Valve Anatomy Hurst 12 th ed.
5 Selected Abnormalities of Aortic Valve Aortic Stenosis Narrowing of the valve orifice Aortic Regurgitation Incompetence of the valve Blood leaks from aorta to left ventricle in ventricular diastole Bicuspid Aortic Valve Endocarditis
6 How to Assess the Aortic Valve Clinical History Physical Examination Echocardiography Transthoracic Transesophageal Angiography Cardiac CT (not regurgitation, though) MRI
7 Why do aortic valves become Valvular Stenosis stenotic? Bicuspid valve with calcification Age-related calcific aortic stenosis Rheumatic Rare causes: Congenital, Rheumatoid, Severe atherosclerosis (Hyperlipidemia), alkaptonuria Supravalvular Stenosis Subvalvular Stenosis Discrete Hypertrophic Cardiomyopathy Braunwald 8th ed.

8 Normal aortic valve Bicuspid aortic stenosis Rheumatic aortic stenosis Age related aortic stenosis Braunwald 8th ed.

9 Normal trileaflet aortic valve echo 2009 David Stultz, MD
10
11 How to assess aortic stenosis by echo 2-DD echo Planimetry measure the valve orifice Doppler Hemodynamics Continuity equation Peak/Mean pressure gradient

12 Planimetry Transthoracic Transesophageal Technically difficult, may overestimate valve area
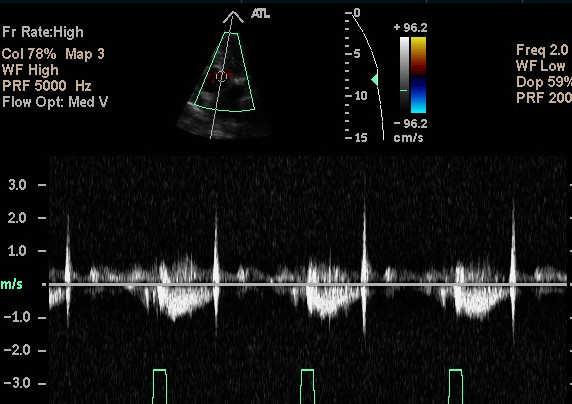
13 Echo Doppler Echo probe generates sound wave Sound wave reflects off tissue/blood Echo probe has a time window to listen for these reflections Moving targets (blood) will create a frequency shift in the sound wave This frequency shift can be translated into a velocity Can measure the velocity of blood flow
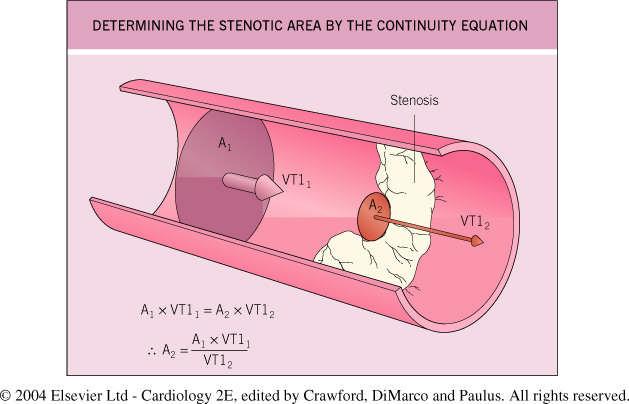
14 Continuity equation Without a nozzle, the water velocity inside the hose (1/2 ) ) is the same as after the hose
15 Continuity equation With a nozzle, the water velocity inside the hose (1/2 ) ) is lower than after the nozzle Nozzle reduces the orifice area Know diameter of hose (1/2 ) Can measure velocity of water in the hose Can measure the velocity of water after the nozzle What is the effective orifice created by the nozzle?
16 Continuity equation Conservation of mass Flow before nozzle = Flow after nozzle Area of hose * velocity of water in hose = Orifice area * velocity of water after hose Area = (½( * diameter) 2 * 3.14(π) Can solve equation for orifice area
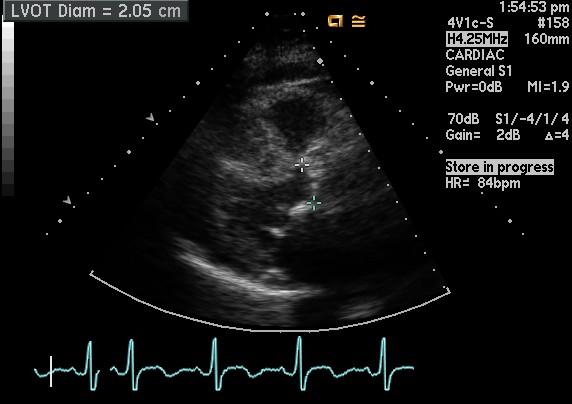
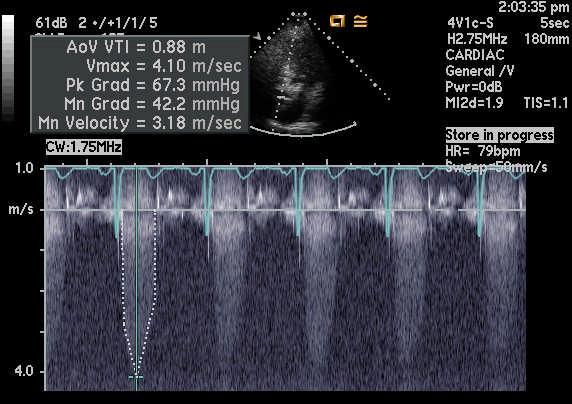
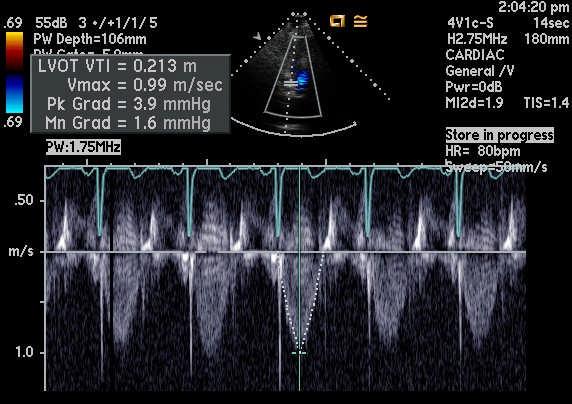
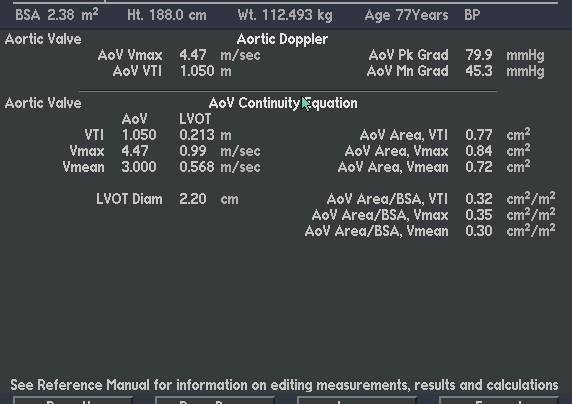
17 Continuity equation Now think of the aortic valve Can measure LVOT diameter Can measure LVOT velocity (or TVI) Can measure velocity (or TVI) after aortic valve Can solve for aortic valve orifice Simplified Bernoulli equation 4v 2 = mmhg pressure gradient
18
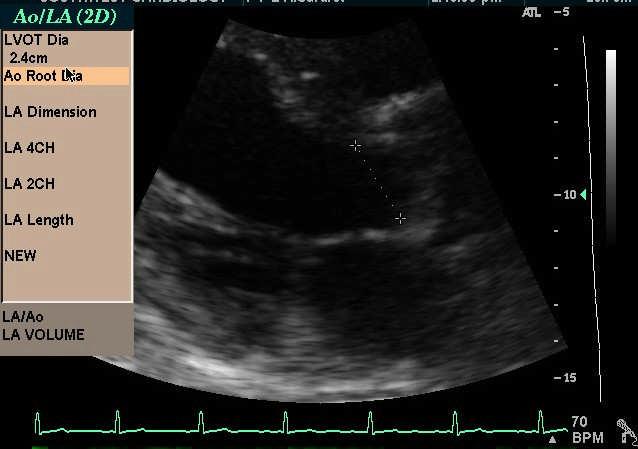
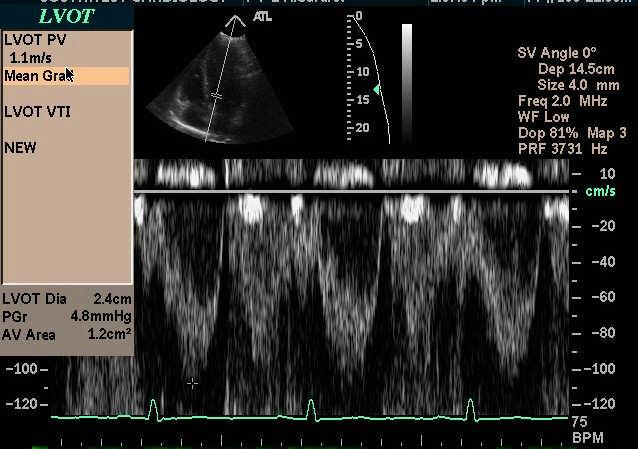
19 Case 1 77 year old African American Male Referred for evaluation of murmur Medical history: HTN Asymptomatic, able to walk up and down stairs, shovel snow BP 146/86 Crescendo/Descrescendo 3/6 systolic murmur at left lower sternal border
20
21
22
23

24
25
26 Severe aortic stenosis Aortic valve area <1.0cm 2 Peak aortic velocity >4.0m 2 Mean aortic valve gradient >40 mmhg
27 Pathphysiology of Aortic Stenosis Previously felt to occur as a normal process of aging, related to mechnical stress on normal valve Current theory involves inflammatory process with T lymphocyte and macrophage infiltration with lipid accumulation, resulting in bone formation (calcification) Braunwald 8th ed.
28 Prevalence of Aortic Stenosis At age 65 29% have aortic sclerosis Irregular thickening of leaflets Mild/early form of stenosis 2% have aortic stenosis Braunwald 8th ed.
29 Risk factors for AS Genetic familial clustering noted in some cases Elevated LDL Elevated Lp(a) Diabetes Smoking Hypertension Braunwald 8th ed.
30 Pathphysiology of Aortic Stenosis Valve orifice area slowly declines over time Symptoms progress gradually LV pressure overload results in concentric hypertrophy Increased LV wall mass, diastolic dysfunction Braunwald 8th ed.
31 Symptoms of AS (Severe) Exertional Dyspnea/Heart failure Chest pain 50% with significant coronary atherosclerosis Syncope Vasodilation with fixed cardiac output
32 Physical Examination of AS Palpation of the carotid upstroke Parvus et tardus Systolic murmur Crescendo-decrescendo decrescendo Heart failure Crackles in lung fields Jugular venous distension Edema

33
34 Management of Asymptomatic Severe Aortic Stenosis Up to 33% remain asymptomatic for 5 years Without symptoms, prognosis is generally good Risk of sudden death 1-2%/year1 Consider exercise testing under direct cardiologist supervision Verify asymptomatic Assess for fall in blood pressure Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111: Rafique AM, Biner S, Ray I, Forrester JS, Tolstrup K, Siegel RJ. Meta-analysis of prognostic value of stress testing in patients with asymptomatic severe aortic stenosis. Am J Cardiol Oct 1;104(7):972-7.
35 Does statin treatment affect AS? Retrospective studies show slowing of progression Prospective (atorvastatin( atorvastatin) ) study showed no benefit in advanced calcific aortic stenosis Prospective (rosuvastatin( rosuvastatin) ) study showed slowing of progression in less severe aortic stenosis Ongoing prospective trial using ezetimide (Zetia) Cowell SJ, Newby DE, Prescott RJ, et al: A randomized trial of intensive lipid-lowering therapy in calcific aortic stenosis. N Engl J Med 2005; 352:2389. Moura LM, Ramos SF, Zamorano JL, et al: Rosuvastatin Affective Aortic Valve Endothelium to slow the progression of aortic stenosis. J Am Coll Cardiol 2007; 49:554.
36 Case 1 management Exercised for 9 minutes on treadmill Manual modified protocol 6.8 METS 83% maximum predicted heart rate Good rise in blood pressure Mild shortness of breath symptoms Started on Beta blocker
37 Case 1 Plan Remains asymptomatic 1 year later Plan for clinical follow-up every 6 months If other heart surgery (CABG) indicated, valve will be replaced
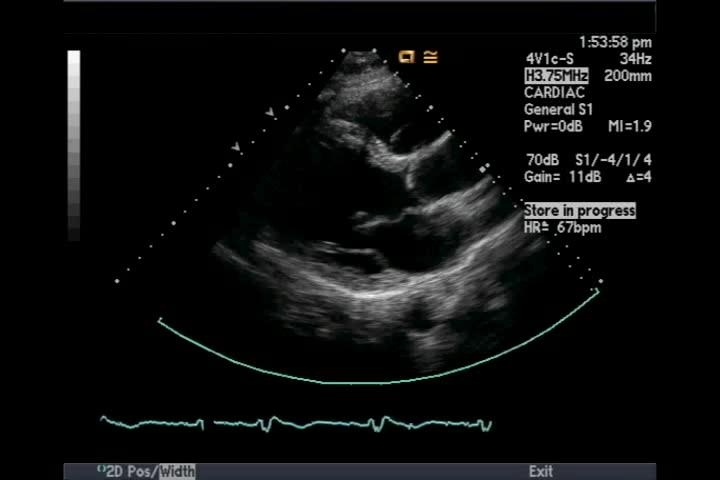
38 Case 2 48 year old male Heart murmur appreciated on physical examination Mild shortness of breath with exertion Climbing 3 flights of stairs No Chest pain Overweight, quit smoking recently DM, HTN, HLP

39 Echocardiogram


40 2009 David A Stultz, closer MD look at the aortic valve
41
42

43
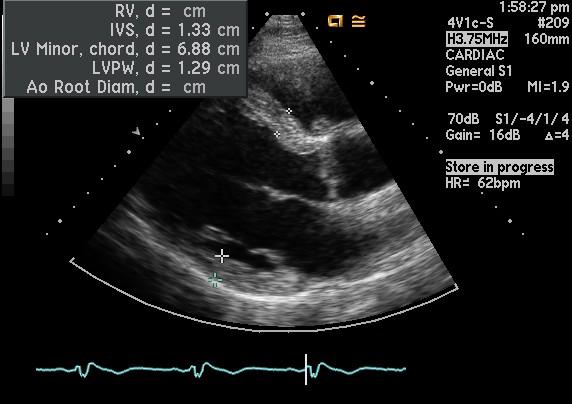
44 Bicuspid Aortic Valve Moderate to severe aortic stenosis Aortic valve area 1.1 cm 2 Mean pressure gradient 44.5 mmhg Peak velocity 4.4 m/s Mild aortic valve regurgitation Dilated of aortic root (4.3 cm)
45 Bicuspid aortic valve 1-2% Incidence in live births Male predominance (up to 80%) Association with disorders of aorta Coarctation Dilitation/aneurysm Dissection Symptomatic stenosis develops around age 50 Familial form with autosomal dominant inheritance (NOTCH1 gene mutation) Carabello BA, Paulus WJ. Aortic stenosis. Lancet Mar 14;373(9667): Epub 2009 Feb 21. Braunwald 8 th ed.
46 Management of Moderate Bicuspid Aortic Stenosis If there is aortic dilatation (>4.0cm) Beta Blockers unless contraindicated Moderate to severe regurgitation Echo every year Surgery if aortic root >5.0cm or >0.5cm/1 year Without aortic dilatation No specific medical therapy Echo every years or if clinical change Bonow RO, Carabello BA, Chatterjee K, de Leon A C Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanew ise JS; American College of Cardiology/American Heart Association Task Force on Practice Guidelines focused update incorporated into the ACC/A HA 2006 guidelines for the management of patients w ith valvular heart disease: a report of the American College of Cardiology/Amer ican Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients w ith valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol Sep 23;52(13):e1-142
47 Case 2 plan of care On statin for hyperlipidemia Treatment of DM, HTN (ARB) Aspirin 81mg daily Followup office and echo in 6 months

48 2009 David Another Stultz, MD example of Bicuspid Aortic Valve
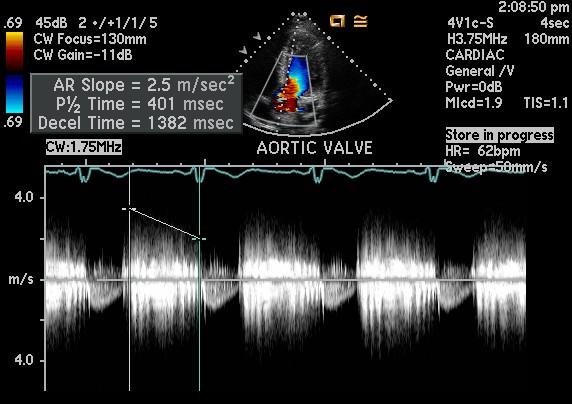
49 Case 3 44 year old white male Referred for loud murmur Spouse started hearing his heart at night about 1 month ago Asymptomatic, physically active, able to climb stairs No smoking, DM, HTN 6/6 loud holodiastolic murmur
50 Transthoracic Echo
51
52
53
54 Indications for Valve replacement in Aortic regurgitation Connective tissue disease with aortic root dilitation (25%) Congenital, including bicuspid (13%) Infective endocarditis (10%) Age-related calcific degeneration (7%) Other/Unknown/Idiopathic (35%) Trauma, rheumatic, syphillis,, aortic dissection, fenfluramine + phentermine, Antiphospholipid syndrome Crawford & DiMarco, 2 nd ed Borer JS, Hochreiter C, Herrold EM, Supino P, Aschermann M, Wencker D, Devereux RB, Roman MJ, Szulc M, Kligfield P, Isom OW. Prediction of indications for valve replacement among asymptomatic or minimally symptomatic patients with chronic aortic regurgitation and normal left ventricular performance. Circulation Feb 17;97(6):
55 How to assess aortic regurgitation History Physical Echocardiogram Angiography MRI
56 Echocardiographic evaluation of Color Doppler Jet area Jet height PISA ERO aortic regurgitation Pressure ½ time Regurgitant fraction, volume Descending thoracic aortic flow reversal Left ventricular EF and dimensions No single criteria is perfect Eccentric jets are often worse than calculated/estimated

57 Color doppler Mild Moderate Severe Visual inspection Also Jet area and jet height Feigenbaum 6 th ed
( ) left ventricular")

58 Pressure ½ time Measurement of time it takes for aortic pressure to equalize to (½)( ) left ventricular pressure Variable thresholds in literature! <300ms consistent with severe regurgitation ms moderate >500ms mild

59 Flow reversal in descending thoracic aorta
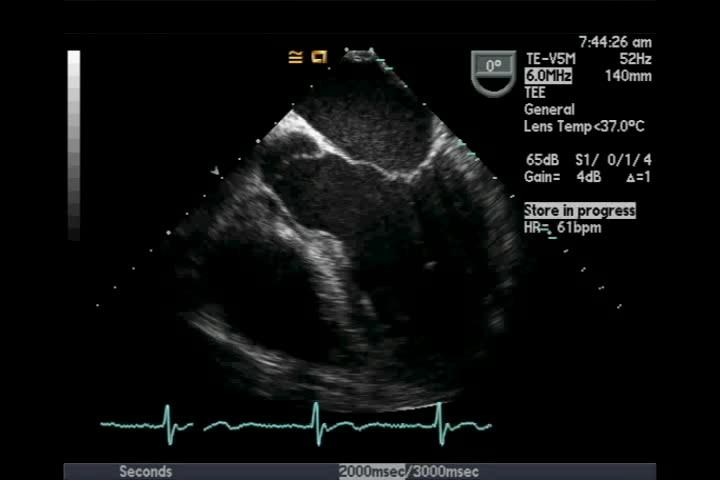
60 Transesophageal Echo
61 Case 3 management Severe posteriorly eccentric aortic regurgitation LV diastolic dimension 6.9cm EF 60-65% 65% No clear etiology Blood cultures obtained 2 of 2 initially positive gram + cocci 1 of 4 subsequently positive gram + cocci Initially admitted, treated with IV antibiotics Blood cultures staph, all different species Antibiotics stopped, no symptoms
62 Criteria for Surgery? Asymptomatic Severe Aortic regurgitation EF <50% Systolic dimension >5.5cm Diastolic dimension >7.5cm Guidelines are complicated, but become more vigilant about surveillance when Systolic dimension >5.0cm Diastolic dimension >7.0cm
63 Issues not addressed in guidelines Noncoronary cusp prolapse with severe eccentric jet hitting anterior leaflet of the mitral valve? Possibility to distort Mitral valve architecture Unclear etiology Lifestyle Both patient and spouse hear the murmur
64 Referred for elective surgery Mechanical or bioprosthetic valve? Intraoperatively,, torn noncoronary cusp noted Overall stable postoperative course
65 Case 4 Male in mid 40 s History of automobile accident with orthopedic trauma Several years afterward, noted to have murmur Echo showed aortic regurgitation Overall asymptomatic Does not want to take medications

66 Echo 8 years later
67 Management LV diastolic dimension 7.6cm EF 55-60% Class 2A indication for surgery by guidelines Vasodilator therapy (Nifedipine( Nifedipine,, ACE inhibitors) are a Class 2B indication Pt declines surgery and medications 6-12 month clinical and echo followup Bonow RO, Carabello BA, Chatterjee K, de Leon A C Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanew ise JS; American College of Cardiology/American Heart Association Task Force on Practice Guidelines focused update incorporated into the ACC/A HA 2006 guidelines for the management of patients w ith valvular heart disease: a report of the American College of Cardiology/Amer ican Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients w ith valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol Sep 23;52(13):e1-142

68 2009 David Stultz, 5 MD years later after last echo


69 As time passes Initial 5 Years Later LVH decreases LV diastolic dimension decreases



70 As time passes Initial 5 Years Later Pressure ½ Time decreases Correlating with worse regurgitation


71 As time passes Initial 5 Years Later
72 Variable natural history Asymptomatic patients with normal LV function <6%/year have symptoms and/or LV dysfunction <3.5%/year progress to asymptomatic LV dysfunction <0.2%/year have sudden cardiac death Asymptomatic patients with LV dysfunction >25%/year progress to have symptoms Symptomatic Severe Aortic Regurgitation >10%/year mortality rate Bonow RO, Carabello BA, Chatterjee K, de Leon A C Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanew ise JS; American College of Cardiology/American Heart Association Task Force on Practice Guidelines focused update incorporated into the ACC/A HA 2006 guidelines for the management of patients w ith valvular heart disease: a report of the American College of Cardiology/Amer ican Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients w ith valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol Sep 23;52(13):e1-142
73 Conclusion Case illustrations of decision making for Asymptomatic severe aortic stenosis Moderate bicuspid aortic stenosis with aortic root dilatation Asymptomatic severe aortic regurgitation Symptoms + Severe AS or AR = Surgery No clear medical management Consider Beta blockers for aortic root dilatation Statins for mild-moderate moderate aortic stenosis?
74 References Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS; American College of Cardiology/American Heart Association Task Force on Practice Guidelines focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol Sep 23;52(13):e Borer JS, Hochreiter C, Herrold EM, Supino P, Aschermann M, Wencker D, Devereux RB, Roman MJ, Szulc M, Kligfield P, Isom OW. Prediction of indications for valve replacement among asymptomatic or minimally symptomatic patients with chronic aortic regurgitation and normal left ventricular performance. Circulation Feb 17;97(6): Cowell SJ, Newby DE, Prescott RJ, et al: A randomized trial of intensive lipid-lowering therapy in calcific aortic stenosis. N Engl J Med 2005; 352:2389. Moura LM, Ramos SF, Zamorano JL, et al: Rosuvastatin Affective Aortic Valve Endothelium to slow the progression of aortic stenosis. J Am Coll Cardiol 2007; 49:554. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111: Rafique AM, Biner S, Ray I, Forrester JS, Tolstrup K, Siegel RJ. Meta-analysis of prognostic value of stress testing in patients with asymptomatic severe aortic stenosis. Am J Cardiol Oct 1;104(7):972-7.
Valvular Heart Disease
 Valvular Heart Disease Roman M. Sniecinski, MD, FASE Associate Professor of Anesthesiology Emory University School of Medicine Learning Objectives Review the major pathophysiology of the most common heart
Valvular Heart Disease Roman M. Sniecinski, MD, FASE Associate Professor of Anesthesiology Emory University School of Medicine Learning Objectives Review the major pathophysiology of the most common heart
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Management of Aortic Valve Disease: Review Questions
 S e l f - A s s e s s m e n t i n C a r d i o l o g y Management of Aortic Valve Disease: Review Questions Josh Leitner, MD Wen-Chih Wu, MD QUESTIONS Choose the single best answer for each question. Questions
S e l f - A s s e s s m e n t i n C a r d i o l o g y Management of Aortic Valve Disease: Review Questions Josh Leitner, MD Wen-Chih Wu, MD QUESTIONS Choose the single best answer for each question. Questions
Aortic Regurgitation & Aorta Evaluation
 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
A Health Care Professional s Guide Aortic Stenosis in Seniors
 A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
: mm 86 mm EF mm
 37 Vol. 35, pp. 37 42, 2007 2 3 : 9 6 22 68 40 2003 4 Ejection fraction: EF44 IV 70 mm 86 mm EF46 6 24 mm 4 mm EF 80 60 mm 70 mm Aortic Regurgitation: AR 2 3 AR Aortic Valve Replacement: AVR AR 38 : 68
37 Vol. 35, pp. 37 42, 2007 2 3 : 9 6 22 68 40 2003 4 Ejection fraction: EF44 IV 70 mm 86 mm EF46 6 24 mm 4 mm EF 80 60 mm 70 mm Aortic Regurgitation: AR 2 3 AR Aortic Valve Replacement: AVR AR 38 : 68
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
TAVI and Valve Replacement Thromboprophylaxis. Warren Prokopiw Pharmacy Resident
 TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
G. AORTIC STENOSIS (AS)
") G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
CARDIAC PHYSIOLOGIST LED AORTIC STENOSIS SURVEILLANCE CLINIC
 CARDIAC PHYSIOLOGIST LED AORTIC STENOSIS SURVEILLANCE CLINIC Background Aortic stenosis is the commonest form of valvular heart disease in the UK Asymptomatic patients with mild AS make up a significant
CARDIAC PHYSIOLOGIST LED AORTIC STENOSIS SURVEILLANCE CLINIC Background Aortic stenosis is the commonest form of valvular heart disease in the UK Asymptomatic patients with mild AS make up a significant
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
My Heart Will Go on: ANTICOAGULATION NO LONGER STOPS AT VALVULAR HEART DISEASE
 Disclosures My Heart Will Go on: ANTICOAGULATION NO LONGER STOPS AT VALVULAR HEART DISEASE Nicholas Boemio, PharmD- No potential or actual conflicts of interest to disclose Kim L. Daley, PharmD, BCGP,
Disclosures My Heart Will Go on: ANTICOAGULATION NO LONGER STOPS AT VALVULAR HEART DISEASE Nicholas Boemio, PharmD- No potential or actual conflicts of interest to disclose Kim L. Daley, PharmD, BCGP,
My Heart Will Go on: Disclosures 3/2/2018
 My Heart Will Go on: ANTICOAGULATION NO LONGER STOPS AT VALVULAR HEART DISEASE Nicholas Boemio, PharmD PGY-1 Pharmacy Practice Resident VA Connecticut Healthcare System Kim L. Daley, PharmD, BCGP, CDP
My Heart Will Go on: ANTICOAGULATION NO LONGER STOPS AT VALVULAR HEART DISEASE Nicholas Boemio, PharmD PGY-1 Pharmacy Practice Resident VA Connecticut Healthcare System Kim L. Daley, PharmD, BCGP, CDP
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Tricuspid and Pulmonic Valve Disease
 Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Aortic stenosis (AS) is common with the aging population.
 is common with the aging population.") New Insights Into the Progression of Aortic Stenosis Implications for Secondary Prevention Sanjeev Palta, MD; Anita M. Pai, MD; Kanwaljit S. Gill, MD; Ramdas G. Pai, MD Background The risk factors affecting
New Insights Into the Progression of Aortic Stenosis Implications for Secondary Prevention Sanjeev Palta, MD; Anita M. Pai, MD; Kanwaljit S. Gill, MD; Ramdas G. Pai, MD Background The risk factors affecting
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
 Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Aortic valve disease. Acknowledgement for slides. Heart Valves 4/28/2018. Adopted from
 Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
MATRIX VHD FORM. State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form.
 for whom you are providing the information contained in this form.") MATRIX VHD FORM A. Patient Information State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form. (First Name) (Middle Initial) (Last Name) (Date
MATRIX VHD FORM A. Patient Information State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form. (First Name) (Middle Initial) (Last Name) (Date
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Circulation Cardiovascular Case Series
 Circulation Cardiovascular Case Series Asymptomatic Severe Aortic Stenosis Silence of the Lambs? Ravi V. Shah, MD; Nihar R. Desai, MD, MPH; Patrick T. O Gara, MD Forward Information about a real patient
Circulation Cardiovascular Case Series Asymptomatic Severe Aortic Stenosis Silence of the Lambs? Ravi V. Shah, MD; Nihar R. Desai, MD, MPH; Patrick T. O Gara, MD Forward Information about a real patient
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Valvular Heart Disease: Recognition and Management in the Outpatient Setting
 Valvular Heart Disease: Recognition and Management in the Outpatient Setting Ian S. Harris UCSF Division of Cardiology Case 1: 80 year old man with a history of hypertension, complaining of exertional
Valvular Heart Disease: Recognition and Management in the Outpatient Setting Ian S. Harris UCSF Division of Cardiology Case 1: 80 year old man with a history of hypertension, complaining of exertional
WRITING COMMITTEE MEMBERS
 Journal of the American College of Cardiology Vol. 48, No. 3, 2006 2006 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/06/$32.00 Published by Elsevier
Journal of the American College of Cardiology Vol. 48, No. 3, 2006 2006 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/06/$32.00 Published by Elsevier
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Left Ventricular Outflow Tract Obstruction
 Left Ventricular Outflow Tract Obstruction Department of Paediatrics Left Ventricular Outflow Tract Obstruction Subvalvular aortic stenosis Aortic Stenosis Supravalvular aortic stenosis Aortic Coarctation
Left Ventricular Outflow Tract Obstruction Department of Paediatrics Left Ventricular Outflow Tract Obstruction Subvalvular aortic stenosis Aortic Stenosis Supravalvular aortic stenosis Aortic Coarctation
Mitral Valve Disease. Prof. Sirchak Yelizaveta Stepanovna
 Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy
 Mædica - a Journal of Clinical Medicine STATE TE-OF OF-THE THE-AR ART Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy Roxana Cristina SISU MD, Fellow in cardiology;
Mædica - a Journal of Clinical Medicine STATE TE-OF OF-THE THE-AR ART Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy Roxana Cristina SISU MD, Fellow in cardiology;
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should.
 What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
VALVULO-METABOLIC RISK IN AORTIC STENOSIS
 January 2008 (Vol. 1, Issue 1, pages 21-25) VALVULO-METABOLIC RISK IN AORTIC STENOSIS By Philippe Pibarot, DVM, PhD, FACC, FAHA Groupe de Recherche en Valvulopathies (GRV), Hôpital Laval Research Centre
January 2008 (Vol. 1, Issue 1, pages 21-25) VALVULO-METABOLIC RISK IN AORTIC STENOSIS By Philippe Pibarot, DVM, PhD, FACC, FAHA Groupe de Recherche en Valvulopathies (GRV), Hôpital Laval Research Centre
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Regurgitant Lesions. Bicol Hospital, Legazpi City, Philippines July Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA
 Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Valve Disease Board Review Questions
 Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Which one of the following echocardiographic profiles most strongly indicates the need for aortic valve replacement? FS [
 Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
Aortic regurgitation. Physiopathology. Dr Pilar Tornos Hospital Vall d Hebron. Barcelona Eurovalve 2014
 Aortic regurgitation. Physiopathology Dr Pilar Tornos Hospital Vall d Hebron. Barcelona Eurovalve 2014 Faculty disclosure Pilar Tornos I have no financial relationships to disclose. Acute AR Etiology:
Aortic regurgitation. Physiopathology Dr Pilar Tornos Hospital Vall d Hebron. Barcelona Eurovalve 2014 Faculty disclosure Pilar Tornos I have no financial relationships to disclose. Acute AR Etiology:
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis
 Page 1 of 5 Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis Authors Athina Chasapi, Adam Hobbs, Theodore Velissaris & Benoy N Shah. Wessex Cardiac &
Page 1 of 5 Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis Authors Athina Chasapi, Adam Hobbs, Theodore Velissaris & Benoy N Shah. Wessex Cardiac &
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications
 24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
SAUDI FELLOWSHIP TRAINING PROGRAM. Adult Cardiology. Final Written Examination 2019
 SAUDI FELLOWSHIP TRAINING PROGRAM Adult Cardiology Final Written Examination 2019 Objectives 1. Determine the trainee has sufficient competency related to the required specialty. 2. Determine the eligibility
SAUDI FELLOWSHIP TRAINING PROGRAM Adult Cardiology Final Written Examination 2019 Objectives 1. Determine the trainee has sufficient competency related to the required specialty. 2. Determine the eligibility
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Mitral Valve Disease. Chapter 29
 Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
For unclear reasons, only about 40% of patients with calcific aortic stenosis also have coronary
 Αθηροσκλήρωση και ασβεστοποιός στένωση της αορτικής βαλβίδας. Οµοιότητες και διαφορές Ν. Μεζίλης Κλινική «Άγιος Λουκάς» Ασβεστοποιός στένωση της αορτικής βαλβίδας: Μία ακόµα µορφή αθηρωµάτωσης; Some observations
Αθηροσκλήρωση και ασβεστοποιός στένωση της αορτικής βαλβίδας. Οµοιότητες και διαφορές Ν. Μεζίλης Κλινική «Άγιος Λουκάς» Ασβεστοποιός στένωση της αορτικής βαλβίδας: Μία ακόµα µορφή αθηρωµάτωσης; Some observations
Welcome 17 Michigan TAVR Participating Hospitals!
 Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Coronary Anomalies & Hemodynamic Identification
 Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Section V VALVULAR HEART T DISEASE. Chapter 27 Aortic Stenosis Chapter 28 Aortic Insufficiency Chapter 29 Mitral Valve Disease...
 Section V VALVULAR HEART T DISEASE Chapter 27 Aortic Stenosis........................... 256 Chapter 28 Aortic Insufficiency....................... 265 Chapter 29 Mitral Valve Disease......................
Section V VALVULAR HEART T DISEASE Chapter 27 Aortic Stenosis........................... 256 Chapter 28 Aortic Insufficiency....................... 265 Chapter 29 Mitral Valve Disease......................
Physical Exam Part II
 Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Valvular Heart Disease
 Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
The timing of aortic valve surgery is
 Heart 2000;84:211 218 VALVE DISEASE the prudent physician will evaluate and treat conventional coronary risk factors. Timing of aortic valve surgery Catherine M Otto Division of Cardiology, University
Heart 2000;84:211 218 VALVE DISEASE the prudent physician will evaluate and treat conventional coronary risk factors. Timing of aortic valve surgery Catherine M Otto Division of Cardiology, University
For more information about how to cite these materials visit
 Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Cardiac Ausculation in the Elderly
 Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications