Near Infrared Spectroscopy in Medical Diagnostics
|
|
|
- Dortha Gilmore
- 6 years ago
- Views:
Transcription

1 Near Infrared Spectroscopy in Medical Diagnostics Michael D. Wider, PhD Vice President Of Technology Somanetics Corporation Adjunct Assistant Professor in Physiology Wayne State University School of Medicine
2 Presenter Disclosures The following relationships with commercial interest related to this presentation existed during the past 12 months: Full time employee of Somanetics Corporation. Shareholder of stock and options Somanetics Corporation. NIRS patent pending. The following FDA disclosures related to this presentation exist: All NIRS equipment referenced is FDA approved for use on all patients including neonates. Animal studies presented are investigational.
3 Near Infrared Spectroscopy NIR Spectroscopy What is it? What does it measure? How accurate is it? What are the limitations? Tissue Monitoring - Animal studies Clinical Evidence
4 Beer s Law
5 Near Infrared Spectroscopy - NIRS 700 to 1000 nm wavelength light Bond specific Few molecules absorb at this wavelength Iron containing heme ring H2O at >900 nm

6 Near Infrared
7 NIRS Specific Hb/HbO2 Accurate validation data in human subjects Sensitive extreme sensitivity to change in human subjects and animal model - R
8 What does it measure? rso 2 - regional hemoglobin oxygen saturation in tissue under the sensor - % saturation - Does NOT measure Hb concentration 25% arterial / 75% venous rso 2 venous weighted, no standard value SvO2 no standard value flow / metabolism coupled Tissue Hb saturation delivery / consumption Reflects perfusion distribution

9 Specific Overtone bands with extremely low molar absorptivity
10 Hemoglobin Molar Absorptivity
11 Analyte Specificity Lipids show minimal absorption by hydrocarbons at nm.
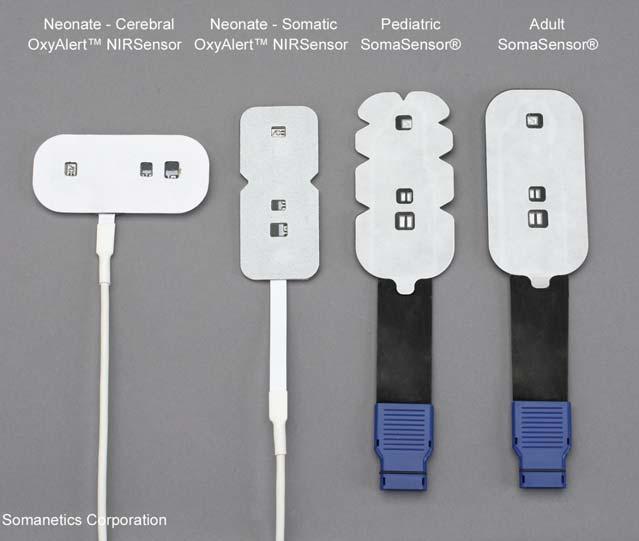
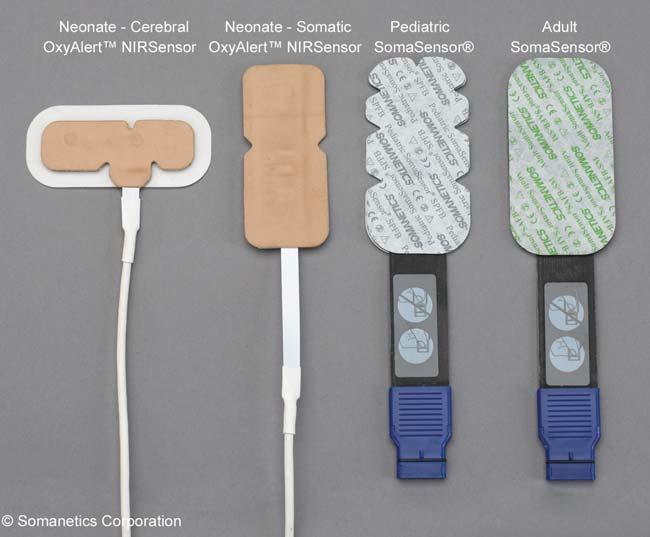
12 Sensors

13 Light Emitting Diode

14 Laser Diodes with Fiber Optics
15 Photodiode


16 Cerebral Oximetry Diffuse Reflectance Spectroscopy

 Hongo K et al.")
17 Spatial Resolution Spatially Resolved NIRS Multiple detectors spatially localize the measurement of brain oxygenation deep-shallow detector compensation isolates brain signals from scalp and surface matter External Carotid Artery Dye Injection Internal Carotid Artery Dye Injection Deep Signal Shallow Signal Deep-Shallow Difference (Represents Brain Signal) Hongo K et al Neurol Res 1995,17:89-93.
; 2000; 45; 328-32 Average age 4.")
18 Accurate - Validation Abdul-Kaliq H et al. Biomed Tech (Berl); 2000; 45; Average age 4.5 years (n=30)
19 Sensitive 50 % CrSO 2 Change Transitions, 22 Pts, 90 Points y = x R 2 = Bias = Std Dev = % fso 2 Change fso2 = field saturation (25% arterial:75% venous)
20 Measuring Oxygen Hb = hemoglobin (Hb) concentration in grams pre 100 ml blood PO 2 = partial pressure of oxygen (mm Hg) in air or liquid PaO 2 = Arterial partial pressure of dissolved oxygen in plasma (mm Hg) SO 2 = % saturation of Hb with oxygen SpO 2 = % saturation of Hb in arterial blood measured by pulse oximetry SaO 2 = % saturation of Hb in arterial blood SvO 2 = % saturation of Hb in mixed venous blood SjvO 2 = % saturation of Hb in jugular vein blood FiO 2 = fraction of oxygen in inspired air at sea level CaO2 = total Oxygen content of arterial blood DO 2 = Delivered oxygen rso 2 = amount of hemoglobin bound oxygen in tissue
21 Arterial vs Tissue HbO 2 Related but different issues - supply vs demand Clinical emphasis on O 2 supply blood gas, pulse ox Defined interventions for supply side SpO 2 fix the number and you fix the problem rso 2 perfusion balance / AV difference Arterial O 2 doesn t guarantee tissue O 2
22 Absolute Venous Saturation? While there is an absolute number or target saturation for arterial blood (SpO2 = 98%) there is no absolute number for venous saturation. SvO 2 depends on flow, ph, 2,3 DPG, Hb form, Hb concentration, vascular abnormalities, capillary exchange, tissue O2 demand, autoregulation, etc. Arterial Hb saturation does not guarantee sufficient O2 delivery.
23 Baselines Normal Cerebral rso 2 rso2 + SE Dark Sk in Light Skin Male Fem ale Total n=76 n=138 n=50 n=175 n=225 Normal, ambulatory adults (n=225)
24 Thresholds Following are the most recognized values published in the pediatric arena most often on congenital heart patients. Cerebral Typical range: 60-80; assuming SpO 2 is >90 < 50 rso 2 or 20% from rso 2 baseline < 45 rso 2 or 25% from rso 2 baseline is critical threshold Somatic Response to intervention Watch for drops 20% below patient baseline Hoffman GM, et al. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2005: Hoffman GM, et al. Anesthesiology 2005;103:A1327. Petrova A and Mehta R. Pediatr Crit Care Med 2006;7: Dent CL, et al. J Thorac Cardiovasc Surg Jan;131(1): Data on file.
25 Piglet Model Yorkshire- Duroc blend Michigan State University kg 1 to 30 days old Accepted model of human infant Very similar biology and anatomy 1-5 days old - very unstable Anesthetized vs unanesthetized



26 Piglet Model Fully Instrumented Temp Invasive BP HR SpO 2 SvO 2 co-oximeter SaO 2 co-oximeter ET-CO 2 Electrolytes Blood gases Lactate Glucose
27 Piglet Cerebral rso 2 Validation Cumulative CrSO2 vs SijvO 2 CrSO y = x R 2 = piglets 1.1 to 5.4 kg n = SijvO 2
28 Normal Piglet 100 Normal Piglet (Avg n=4) rso :00 0:20 0:40 1:00 1:20 1:40 2:00 2:20 2:40 3:00 3:20 3:40 4:00 Head Leg Kidney Gut
29 Cerebral Ischemia Carotid Occlusion bilateral occlusion unilateral occlusion 3.5 kg piglet rso Head Liver Kidney Gut Release 0 Time
30 Functional and Biochem Ischemic Thresholds FIG. 5. Logistic regression plot between near-infrared spectros-copy ScO2 and the percent of piglets without minor change in EEG activity or without major change in EEG activity compared with baseline. Data points indicate mean ± SD. Logistic regres-sion equation variables are presented in Table 2. FIG. 6. Logistic regression plot between near-infrared spectros-copy ScO2 and the percent of piglets with normal brain tissue lactate concentrations and normal brain tissue ATP concentra-tions. Data points indicate mean ± SD. Logistic regression equa-tion variables are presented in Table 2. Kurth CD, Levy WJ and McCann J J Cerebral Blood Flow and Metab 22;

31 Hou X et al Physiol Measures 28; Structural Ischemic Thresholds ~2.2 kg piglets >60% 40-50% 35-40% 30-35%
32 Renal Ischemia Renal Ischemia 2.7 kg piglet rso artery released Cerebral Gut Kidney Muscle renal artery occluded artery released 10 0 Time
33 Abdominal Ischemia am Ischemic Gut 1.9 kg piglet rso Right abdomen Right leg time
34 Hypovolemia Hypovolemia 3.5 kg piglet cc 40 cc 20 cc 10 cc 10 cc 8 cc 10 cc FA rso Head Liver Kidney Gut SpO 2 93 HR 181 MAP 66 SpO 2 9 HR 212 MAP 56 SpO 2 95 HR 241 MAP 50 Sf vo 2 35 Sf ao 2 93 SpO 2 93 HR 254 MAP 44 Sf vo 2 23 SpO 2 93 HR 277 MAP 62 SpO 2 92 HR 270 MAP 58 SpO 2 92 MAP 36 HR 246 Sf vo 2 30 Sf ao 2 94 SpO2 92 HR 279 MAP 42 SpO2 of f HR 231 MAP 25 Si j vo Time
35 Anemia Infant Sensor Anemia 1.4 kg piglet cc blood draw 60 cc LRS infused with each blood draw 25 cc blood draw 20 cc blood draw Euthanasia cc blood draw :19 13:30 13:41 13:52 14:03 14:14 14:26 14:37 14:48 14:59 15:10 15:21 15:32 15:43 rso2 6.0 Hb (gm/dl) 45 cc blood infused cc blood reinfused Head Leg Kidney Gut Hb
36 Anemia Baseline Shock Study Baseline 1.6 kg piglet rso /4 NS + D5W Total Hb 4.8 gm/dl 0 12:00 12:27 12:55 13:23 13:50 Time 14:18 14:46 15:13 15:41 16:09 Head Leg Kidney Gut
37 Using NIRS Look at the rso2 first Cerebral, perirenal and gut Perfusion distribution Then decide how the other clinical variables relate Decide on interventions based on all clinical data
38 Diagnostic Use Rule Out Perirenal rso 2 decline with acceptable cerebral rso 2 Reduced peripheral perfusion, autoregulation keeping up GA, Day of life, SpO 2, CHD (PDA, septal defect, FO) shunt, drugs, sepsis, FiO 2 Perirenal rso 2 decline with cerebral rso 2 decline Reduced global O 2 delivery GA, DOL, SpO 2, CHD, myocardial failure, drugs, sepsis, Cerebral rso 2 decline with minimal perirenal rso 2 change CO 2, cooling, sedation, drugs, brain death Cerebral and perirenal rso 2 stable abdominal rso 2 of Ominous sign of gut ischemia if prolonged Swelling, ascites, sepsis, drain, antibiotics, feeds,
39 MRI Brain Lesions and rso 2 Preop MRI (n =22) demonstrated ischemic lesions in 23% of patients. Postoperative (Norwood) MRI (n =15) demonstrated new or worsened ischemic lesions in 73% of patients Periventricular leukomalacia and focal ischemic lesions most common Prolonged low postoperative rso 2 (45% for 180 minutes) associated with the development of new or worsened ischemia on postoperative MRI (P =.029) Prolonged low postoperative rso2 was a more predictive indicator of neurologic damage than today s traditional OR and CICU measures...post-op cerebral oximetry seems to offer value as a standard of care following the Norwood procedure or other surgical interventions that may impair cardiac output. Dent CL et al J Thorac Cardiovasc Surg 131;
40 Post Norwood Outcome P < Adverse outcome was defined as hospital death, need for extracorporeal membrane oxygenation or cardiac intensive care unit length of stay greater than 30 days. Phelps HM et al Ann Thorac Surg 87;
41 Neonatal Baselines Vanderbilt University study Susannah McNeal et al premature neonates, wks GA First 21 days of life Cerebral, renal and gut mean daily avg rso 2 Cerebral and renal decline 10 pts over first 2 weeks of life vs wks GA - gut rso 2 p< Gut rso 2 variability decreases over first 2 weeks
42 Perirenal Tissue Ischemia Predicted Probabilities and 95% CI POD 3 Creatinine Doubling Somatic rso2 vs. Renal Function POD0 Somatic rso2 Predicted Value 95% CI Hoffman GM, et al. Anesthesiology 2005;103:A1327


43 Separation from ECMO rso 2 Underlying data and case notes on file ISC Data on file. Time

44 Pleural Effusion Following ASD/VSD Repair rso 2 Data on file. Time
45 Early Warning Neonate with Cardiac Defects - Early Indicator 100 Tetrology of Fallot, Pulmonary Atresia and Coarctation of the Aorta no change in map (37) map remains (37-40) cardiac arrest no wave form on art line 60 rso Pt. sx and assessed x ray Pt sx and assessed bilateral grade three-four head bleed 0 15 mcg/kg of dopamine, epinephrine and hydrocortisone for blood pressure support. 0:00 2:12 4:25 6:39 8:52 11:05 13:18 15:31 17:44 19:57 22:10 cerebral perirenal

46 NICU Statistics Kirkby S et al Advances in Neonatal Care 7; 80-87
47 R Nachar Hidalgo, M Wider, E Booth, S Drake, I Seri 2009 Cerebral rso 2 Drug Response (n=3) 100 Cerebral rso 2 Drug Response Dobutamine Dopamine Milrinone Epinephrine Norepinephrin e IV Drug Infusion :00 0:15 0:30 0:45 1:00 1:15 1:30 1:45 2:00 TIME
48 R Nachar Hidalgo, M Wider, E Booth, S Drake, I Seri 2009 Perirenal rso 2 Drug Response (n=3) 100 Perirenal rso 2 Drug Response Dobutamine Dopamine Milrinone Epinephrine Norepinephrin e IV Drug Infusion :00 0:15 0:30 0:45 1:00 1:15 1:30 1:45 2:00 TIME
49 R Nachar Hidalgo, M Wider, E Booth, S Drake, I Seri 2009 Gut rso 2 Drug Response (n=3) 100 Gut rso 2 Drug Response (n=3) Dobutamine Dopamine Milrinone Epinephrine Norepinephrin e IV Drug Infusion :00 0:15 0:30 0:45 1:00 1:15 1:30 1:45 2:00 TIME
50 R Nachar Hidalgo, M Wider, E Booth, S Drake, I Seri 2009 Gut rso 2 Drug Response (n=3) 100 Muscle rso 2 Drug Response (n=3) Dobutamine Dopamine Milrinone Epinephrine Norepinephrin e IV Drug Infusion :00 0:15 0:30 0:45 1:00 1:15 1:30 1:45 2:00 TIME
51 R Nachar Hidalgo, M Wider, E Booth, S Drake, I Seri 2009 Invasive BP Drug Response (n=3) 130 MAP Drug Response (n=3) Dobutamine Dopamine Milrinone Epinephrine Norepinephrin e IV Drug Infusion :00 0:15 0:30 0:45 1:00 1:15 1:30 1:45 2:00 TIME
Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology
 Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology") Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
Oximeters. Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan
 Oximeters Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan chanhl@mail.cgu.edu.tw Oxygen transport in blood Hemoglobin Oxygen O Deoxygen +O O Oximeters Arterial saturation
Oximeters Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan chanhl@mail.cgu.edu.tw Oxygen transport in blood Hemoglobin Oxygen O Deoxygen +O O Oximeters Arterial saturation
INVOS System Inservice Guide for Pediatric Use. INVOS System Inservice Guide for Pediatric Use
 INVOS System Inservice Guide for Pediatric Use INVOS System Inservice Guide for Pediatric Use The INVOS System: A Window to Perfusion Adequacy The noninvasive INVOS System reports the venous- weighted
INVOS System Inservice Guide for Pediatric Use INVOS System Inservice Guide for Pediatric Use The INVOS System: A Window to Perfusion Adequacy The noninvasive INVOS System reports the venous- weighted
Oximeters. Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan
 Oximeters Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan chanhl@mail.cgu.edu.tw Pulse oximeter Masimo pulse CO-oximeter http://www.masimo.com/produc ts/continuous/radical-7/
Oximeters Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan chanhl@mail.cgu.edu.tw Pulse oximeter Masimo pulse CO-oximeter http://www.masimo.com/produc ts/continuous/radical-7/
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Near-Infrared Monitoring of Brain and Tissue Oxygenation: Is the Monitor on the Right Person?
 Near-Infrared Monitoring of Brain and Tissue Oxygenation: Is the Monitor on the Right Person? Frank McGowan, MD, FAAP Professor of Anesthesiology and Critical Care Medicine University of Pennsylvania Perelman
Near-Infrared Monitoring of Brain and Tissue Oxygenation: Is the Monitor on the Right Person? Frank McGowan, MD, FAAP Professor of Anesthesiology and Critical Care Medicine University of Pennsylvania Perelman
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
NEONATAL MONITORING IN-SERVICE GUIDE
 NEONATAL MONITORING IN-SERVICE GUIDE INVOS cerebral/somatic oximetry system Key terms rso 2: regional oxygen saturation INVOS system: In vivo optical spectroscopy Cerebral application: brain area measurement
NEONATAL MONITORING IN-SERVICE GUIDE INVOS cerebral/somatic oximetry system Key terms rso 2: regional oxygen saturation INVOS system: In vivo optical spectroscopy Cerebral application: brain area measurement
How Does Pulse Oximetry Work? SpO2 Sensors Absorption at the Sensor Site Oxyhemoglobin Dissociation Curve
 SpO2 Monitoring Contents 1 Introduction 1 What is SpO 2? How Does Pulse Oximetry Work? SpO2 Sensors Absorption at the Sensor Site Oxyhemoglobin Dissociation Curve 5 How Do I Use SpO2? Choosing a Sensor
SpO2 Monitoring Contents 1 Introduction 1 What is SpO 2? How Does Pulse Oximetry Work? SpO2 Sensors Absorption at the Sensor Site Oxyhemoglobin Dissociation Curve 5 How Do I Use SpO2? Choosing a Sensor
NIRS of the brain new diagnostic tool
 NIRS of the brain new diagnostic tool Berndt Urlesberger Professor of Neonatology Head, Division of Neonatology, Department of Pediatrics Medical University Graz, Austria Email: berndt.urlesberger@medunigraz.at
NIRS of the brain new diagnostic tool Berndt Urlesberger Professor of Neonatology Head, Division of Neonatology, Department of Pediatrics Medical University Graz, Austria Email: berndt.urlesberger@medunigraz.at
Near Infrared Spectroscopy in Neonatal Intensive Care
 Near Infrared Spectroscopy in Neonatal Intensive Care Adré J. du Plessis, MBChB Fetal-Neonatal Neurology, Children s Hospital, Boston, MA Children s Hospital and Harvard Medical School Disclosure Statement
Near Infrared Spectroscopy in Neonatal Intensive Care Adré J. du Plessis, MBChB Fetal-Neonatal Neurology, Children s Hospital, Boston, MA Children s Hospital and Harvard Medical School Disclosure Statement
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Multimodal Brain Monitoring with NIRS and aeeg and their Clinical Significance
 Multimodal Brain Monitoring with NIRS and aeeg and their Clinical Significance The Best of IPOKRaTES: an Update in Neonatology September17-20, Leuven, Belgium What can we monitor to assess adequacy of
Multimodal Brain Monitoring with NIRS and aeeg and their Clinical Significance The Best of IPOKRaTES: an Update in Neonatology September17-20, Leuven, Belgium What can we monitor to assess adequacy of
How to maintain optimal perfusion during Cardiopulmonary By-pass. Herdono Poernomo, MD
 How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
Disclosures. Set up audience participation. Test question. Outline. Neuromonitoring What and When? IP for monitoring technology licensed to Medtronic
 Neuromonitoring What and When? Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set
Neuromonitoring What and When? Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set
Appendix E Choose the sign or symptom that best indicates severe respiratory distress.
 Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases
 Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
When Cyanosis is the Norm. Steven M. Schwartz, MD, FRCPC Cardiac Critical Care Medicine The Hospital for Sick Children Toronto
 When Cyanosis is the Norm Steven M. Schwartz, MD, FRCPC Cardiac Critical Care Medicine The Hospital for Sick Children Toronto No Disclosures When Cyanosis is the Norm Physiology of cyanotic congenital
When Cyanosis is the Norm Steven M. Schwartz, MD, FRCPC Cardiac Critical Care Medicine The Hospital for Sick Children Toronto No Disclosures When Cyanosis is the Norm Physiology of cyanotic congenital
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018
 CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018 OBJECTIVES 1. Understand how cerebral oximetry works 2. Understand how cerebral oximetry may guide intervention 3. Learn
CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018 OBJECTIVES 1. Understand how cerebral oximetry works 2. Understand how cerebral oximetry may guide intervention 3. Learn
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Biomedical Instrumentation D. The Photoplethysmogram
 Biomedical Instrumentation D. The Photoplethysmogram Dr Gari Clifford Based on slides by Prof. Lionel Tarassenko The need for real-time oxygen saturation monitoring Respiratory failure & pulmonary disease
Biomedical Instrumentation D. The Photoplethysmogram Dr Gari Clifford Based on slides by Prof. Lionel Tarassenko The need for real-time oxygen saturation monitoring Respiratory failure & pulmonary disease
Dr. Puntarica Suwanprathes. Version 2007
 Dr. Puntarica Suwanprathes Version 2007 O 2 and CO 2 transport in blood Oxyhemoglobin dissociation curve O 2 consumption (VO 2 ) CO 2 production (VCO 2 ) O 2 capacity O 2 content: CaO 2 or CvO 2 %saturation
Dr. Puntarica Suwanprathes Version 2007 O 2 and CO 2 transport in blood Oxyhemoglobin dissociation curve O 2 consumption (VO 2 ) CO 2 production (VCO 2 ) O 2 capacity O 2 content: CaO 2 or CvO 2 %saturation
Oxygen Saturation Monitors & Pulse Oximetry. D. J. McMahon rev cewood
 Oxygen Saturation Monitors & Pulse Oximetry D. J. McMahon 141105 rev cewood 2017-11-14 2 3 Key Points Oxygen Saturation Monitors & Pulse Oximetry : Role of hemoglobin in respiration Basic principle of
Oxygen Saturation Monitors & Pulse Oximetry D. J. McMahon 141105 rev cewood 2017-11-14 2 3 Key Points Oxygen Saturation Monitors & Pulse Oximetry : Role of hemoglobin in respiration Basic principle of
Transfusion Limbo How Low Will You Go? Safely. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
3. Which of the following would be inconsistent with respiratory alkalosis? A. ph = 7.57 B. PaCO = 30 mm Hg C. ph = 7.63 D.
 Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges
 Management: Decision Making & Challenges") Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges GEORGE JUSTISON CCP MANAGER PERFUSION SERVICES UNIVERSITY OF COLORADO HOSPITAL How do you define adequate perfusion?
Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges GEORGE JUSTISON CCP MANAGER PERFUSION SERVICES UNIVERSITY OF COLORADO HOSPITAL How do you define adequate perfusion?
ALCO Regulations. Protocol pg. 47
 For the EMT-Basic Objectives Understand ALCO regulations relative to monitoring pulse oximetry by the EMT-B Review the signs and symptoms of respiratory compromise. Understand the importance of adequate
For the EMT-Basic Objectives Understand ALCO regulations relative to monitoring pulse oximetry by the EMT-B Review the signs and symptoms of respiratory compromise. Understand the importance of adequate
ECMO Primer A View to the Future
 ECMO Primer A View to the Future Todd J. Kilbaugh Assistant Professor of Anesthesiology, Critical Care Medicine, and Pediatrics Director of The ECMO Center at the Children s Hospital of Philadelphia Disclosures
ECMO Primer A View to the Future Todd J. Kilbaugh Assistant Professor of Anesthesiology, Critical Care Medicine, and Pediatrics Director of The ECMO Center at the Children s Hospital of Philadelphia Disclosures
I have no relevant financial relationships with the manufacturers of any. commercial products and/or provider of commercial services discussed in
 I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this activity I do intend to discuss an unapproved/investigative
I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this activity I do intend to discuss an unapproved/investigative
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Module G: Oxygen Transport. Oxygen Transport. Dissolved Oxygen. Combined Oxygen. Topics to Cover
 Topics to Cover Module G: Oxygen Transport Oxygen Transport Oxygen Dissociation Curve Oxygen Transport Studies Tissue Hypoxia Cyanosis Polycythemia Oxygen Transport Oxygen is carried from the lungs to
Topics to Cover Module G: Oxygen Transport Oxygen Transport Oxygen Dissociation Curve Oxygen Transport Studies Tissue Hypoxia Cyanosis Polycythemia Oxygen Transport Oxygen is carried from the lungs to
Current bedside monitors of brain blood flow and oxygen delivery
 24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
Perioperative Management of TAPVC
 Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Cerebral Oximetry in Preterm Infants: Methods, Measurements and Evaluating Clinical Benefit
 Cerebral Oximetry in Preterm Infants: Methods, Measurements and Gorm Ole Greisen DrMedSci Professor and Consultant Neonatologist Department of Neonatology Rigshospitalet and Copenhagen University Copenhagen,
Cerebral Oximetry in Preterm Infants: Methods, Measurements and Gorm Ole Greisen DrMedSci Professor and Consultant Neonatologist Department of Neonatology Rigshospitalet and Copenhagen University Copenhagen,
Perioperative Management of DORV Case
 Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
Pediatric Septic Shock. Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee
 Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Why Old Blood is Bad. tales from the electronic perfusion record. Molly Marko, BS, BSE, CCP Geisinger Health System Danville, Pennsylvania
 Why Old Blood is Bad tales from the electronic perfusion record Molly Marko, BS, BSE, CCP Geisinger Health System Danville, Pennsylvania Disclosure I have no financial relationship with any of the companies
Why Old Blood is Bad tales from the electronic perfusion record Molly Marko, BS, BSE, CCP Geisinger Health System Danville, Pennsylvania Disclosure I have no financial relationship with any of the companies
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation?
 can help prevent Postoperative Cardiorespiratory instability following PDA ligation?") Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Near-Infrared Spectroscopy (NIRS) in the Neonatal Intensive Care Unit: Tissue Oxygenation Physiology and Monitoring Approaches
 in the Neonatal Intensive Care Unit: Tissue Oxygenation Physiology and Monitoring Approaches") Near-Infrared Spectroscopy (NIRS) in the Neonatal Intensive Care Unit: Tissue Oxygenation Physiology and Monitoring Approaches Jonathan P. Mintzer, MD, FAAP Assistant Professor of Pediatrics Stony Brook
Near-Infrared Spectroscopy (NIRS) in the Neonatal Intensive Care Unit: Tissue Oxygenation Physiology and Monitoring Approaches Jonathan P. Mintzer, MD, FAAP Assistant Professor of Pediatrics Stony Brook
ECLS Registry Form Extracorporeal Life Support Organization (ELSO)
") ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
(Peripheral) Temperature and microcirculation
 Temperature and microcirculation") (Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
(Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Heinz-Hermann Weitkemper, EBCP. 4th Joint Scandinavian Conference in Cardiothoracic Surgery 2012 Vilnius / Lithuania
 Heinz-Hermann Weitkemper, EBCP Everyone who earnestly practices perfusion is acting with the full belief that what they are doing is in the best interest of their patients. Perfusion can never be normal,
Heinz-Hermann Weitkemper, EBCP Everyone who earnestly practices perfusion is acting with the full belief that what they are doing is in the best interest of their patients. Perfusion can never be normal,
Muscle OxyGen monitor. The Science Behind Moxy
 Muscle OxyGen monitor The Science Behind Moxy How Does Moxy Monitor Work? Moxy Monitor works by shining near-infrared light onto the skin and detecting some of the light after it has travelled into the
Muscle OxyGen monitor The Science Behind Moxy How Does Moxy Monitor Work? Moxy Monitor works by shining near-infrared light onto the skin and detecting some of the light after it has travelled into the
Hybrid Stage I Palliation / Bilateral PAB
 Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
SUBJECT INFORMATION AND CONSENT FORM
 Title of Study: Department of Anesthesiology British Columbia s Children Hospital 4480 Oak Street Vancouver V6H 3V4 Tel 604 875 2711 Fax 604 875 3221 SUBJECT INFORMATION AND CONSENT FORM Mobile Health:
Title of Study: Department of Anesthesiology British Columbia s Children Hospital 4480 Oak Street Vancouver V6H 3V4 Tel 604 875 2711 Fax 604 875 3221 SUBJECT INFORMATION AND CONSENT FORM Mobile Health:
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
ECMO CPR. Ravi R. Thiagarajan MBBS, MPH. Cardiac Intensive Care Unit
 ECMO CPR Ravi R. Thiagarajan MBBS, MPH Staff Intensivist Cardiac Intensive Care Unit Children s Hospital Boston PCICS 2008, Miami, FL No disclosures Disclosures Outline Outcomes for Pediatric in-hospital
ECMO CPR Ravi R. Thiagarajan MBBS, MPH Staff Intensivist Cardiac Intensive Care Unit Children s Hospital Boston PCICS 2008, Miami, FL No disclosures Disclosures Outline Outcomes for Pediatric in-hospital
Defining Optimal Perfusion during CPB. Carlo Alberto Tassi Marketing Manager Eurosets Italy
 Defining Optimal Perfusion during CPB Carlo Alberto Tassi Marketing Manager Eurosets Italy It is a device able to monitor in a real time vital parameters and able to provide information regarding the transport
Defining Optimal Perfusion during CPB Carlo Alberto Tassi Marketing Manager Eurosets Italy It is a device able to monitor in a real time vital parameters and able to provide information regarding the transport
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Pulse. Assess for the following:
 Vital Signs Overview LOC = AVPU Pulse Respiration's Blood Pressure Lung Sounds Skin: Color, Texture, Temperature Pupils = Equal, Reactive to Light with Accomodation Pulse Assess for the following: Rate
Vital Signs Overview LOC = AVPU Pulse Respiration's Blood Pressure Lung Sounds Skin: Color, Texture, Temperature Pupils = Equal, Reactive to Light with Accomodation Pulse Assess for the following: Rate
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Failure of the circulation to maintain Tissue cellular. Tissue hypoperfusion Cellular hypoxia SHOCK. Perfusion
 Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Pulse oximetry revisited. Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital University of Pretoria
 Pulse oximetry revisited Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital University of Pretoria Topics that will be discussed and dissected: Revisiting physiology
Pulse oximetry revisited Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital University of Pretoria Topics that will be discussed and dissected: Revisiting physiology
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
NIRS utilization during first hours and days of life
 NIRS utilization during first hours and days of life Berndt Urlesberger, MD Professor of Neonatology Division of Neonatology, Department of Pediatrics Medical University Graz, Austria Email: berndt.urlesberger@medunigraz.at
NIRS utilization during first hours and days of life Berndt Urlesberger, MD Professor of Neonatology Division of Neonatology, Department of Pediatrics Medical University Graz, Austria Email: berndt.urlesberger@medunigraz.at
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Stabilization and Transportation guidelines for Neonates and infants with Heart disease:
 Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
The first oximetry system to put regional oximetry, pulse oximetry and ease of use at your fingertips.
 Model X-100 Universal Oximetry System for Pediatric Patients The first oximetry system to put regional oximetry, pulse oximetry and ease of use at your fingertips. NIRS [near-infrared spectroscopy] has
Model X-100 Universal Oximetry System for Pediatric Patients The first oximetry system to put regional oximetry, pulse oximetry and ease of use at your fingertips. NIRS [near-infrared spectroscopy] has
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Management of a Patient after the Bidirectional Glenn
 Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
The Hemodynamic Puzzle
 The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
Ajay Yadlapati, MD;* Tristan Grogan, MS; David Elashoff, PhD; Robert B. Kelly, MD
 The Journal of ExtraCorporeal Technology Correlation of a Novel Noninvasive Tissue Oxygen Saturation Monitor to Serum Central Venous Oxygen Saturation in Pediatric Patients with Postoperative Congenital
The Journal of ExtraCorporeal Technology Correlation of a Novel Noninvasive Tissue Oxygen Saturation Monitor to Serum Central Venous Oxygen Saturation in Pediatric Patients with Postoperative Congenital
Cardiovascular System. Blood Vessel anatomy Physiology & regulation
 Cardiovascular System Blood Vessel anatomy Physiology & regulation Path of blood flow Aorta Arteries Arterioles Capillaries Venules Veins Vena cava Vessel anatomy: 3 layers Tunica externa (adventitia):
Cardiovascular System Blood Vessel anatomy Physiology & regulation Path of blood flow Aorta Arteries Arterioles Capillaries Venules Veins Vena cava Vessel anatomy: 3 layers Tunica externa (adventitia):
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
I intend to discuss an unapproved/investigative use of a commercial product/device in my presentation
 Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
SenSmart Model X-100. The first oximetry system to put regional oximetry, pulse oximetry and ease of use at your fingertips.
 SenSmart Model X-100 Universal Oximetry (rso2 /SpO2 ) System for Pediatric Patients The first oximetry system to put regional oximetry, pulse oximetry and ease of use at your fingertips. NIRS [near-infrared
SenSmart Model X-100 Universal Oximetry (rso2 /SpO2 ) System for Pediatric Patients The first oximetry system to put regional oximetry, pulse oximetry and ease of use at your fingertips. NIRS [near-infrared
MANAGEMENT OF CIRCULATORY FAILURE
 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
Optical Sensor System for Hemoglobin Measurement
 International Journal of Computational Engineering Research Vol, 03 Issue, 7 Optical Sensor System for Hemoglobin Measurement Rajashree Doshi 1, Anagha Panditrao 2 1 Department of Instrumentation and Control,
International Journal of Computational Engineering Research Vol, 03 Issue, 7 Optical Sensor System for Hemoglobin Measurement Rajashree Doshi 1, Anagha Panditrao 2 1 Department of Instrumentation and Control,
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Oximetry. Jan Bakker. Grants Hutchinson Pulsion.
 Oximetry Jan Bakker jan.bakker@erasmusmc.nl www.erasmusmc.me Grants Hutchinson Pulsion Postgraduate Workshop on Hemodynamic Monitoring ISICEM 2012 - Brussels Oximetry arterial (pulse oximetry) central/mixed
Oximetry Jan Bakker jan.bakker@erasmusmc.nl www.erasmusmc.me Grants Hutchinson Pulsion Postgraduate Workshop on Hemodynamic Monitoring ISICEM 2012 - Brussels Oximetry arterial (pulse oximetry) central/mixed