George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
|
|
|
- Magdalene Crawford
- 5 years ago
- Views:
Transcription




1 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR
2 Outline Epidemiology Mechanisms Initial Management Imaging Specific organ injuries: Liver and Spleen Renal Bowel Pancreas Follow up Role of minimally invasive surgery
3 Epidemiology: 1.5 million children/year involved in trauma 500,000 hospitalizations/year 20,000 deaths/year Blunt abdominal trauma 30% more common than thoracic trauma but 40% less fatal 8 12% of children with blunt abdominal trauma will have intra abdominal injuries Only 5 10% of these require surgery Mortality 10%
4 Mechanism: MVC without proper restraints: commonest Seat belt injuries: Lap belt Triad of abdominal wall contusion, Chance fracture & intestinal injuries Automobile versus pedestrian Falls ATV Handlebar injuries: bowel & pancreatic injuries Sports related (1%) Run over


5 Seatbelt Sign Handlebar Injury
6 Initial Evaluation LR or NS bolus at 20 cc/kg x2 if HD unstable Packed RBCS at 10 cc/kg if HD unstable Relevant History (if possible): Mononucleosis Bleeding tendency Developmental delay (CP, autism, etc ) Physical Examination: ABCDE Broselow tape Commonest cause of abdominal distension & tenderness is gastric distension with air Second most common cause is a full bladder
7 Initial Evaluation Physical Examination: Localized tenderness most predictive of IAI Abdominal wall bruises/echymosis highly suggestive Additional findings that help predict IAI: Femur fracture (OR 1.3) Low systolic BP (OR 4.8) GCS < 13 (OR 1.7) Challenges: The preverbal child The mentally challenged child Children with head injury
8 Lab studies: Type & cross Hemogram, LFTs and UA most useful Should not alter management but guide further studies CBC: Useful for f/u of solid organ injury Do not use to guide further imaging ALT & AST: Elevation is highly suggestive of liver injury If elevated & exam equivocal get a CT UA: ( >5 50 RBCs/hpf) Contraversial If +ve with an equivocal exam get act Coags: Only in those with head injury
9 Imaging: Plain films: Lateral C spine, CXR & pelvis CT abd/pelvis: Most accurate, noninvasive IV contrast a must Obtain CT head 1 st before contrast injection Not indicated if HD unstable Grades injury severity but does not correlate with outcome Contraversies: Contrast blush with solid organ injury Free fluid with no evidence of solid organ injury US: (FAST) Not well studied in the pediatric population May have a role in HD unstable patients
10 Adjuncts: DPL: May be useful to exclude bowel injury Largely replaced by CT & diagnostic laparoscopy Laparoscopy: Diagnostic & therapeutic Results in 53% reduction in Ex Laps (University of TN) Exclude serious head injury before OR
11 Liver & Spleen injury: Liver is the most common followed by spleen Hepatic injuries cause greatest number of fatalities (25% mortality) Associated abdominal injuries in 30 40% Liver injuries commonly involve right lobe (60 80%) and 10% of patients will arrive in shock Splenic injury often HD stable with less transfusion requirements Overwhelming postsplenectomy sepsis (OPSS): Lifetime risk 0.026% Mortality 50% Pneumococcal, meningococcal & H influenza vaccination + Penicillin for at least 2 years
12 Liver & Spleen injury:
13 Liver & Spleen injury:


14
15
16 Liver & Spleen Management: Paradigm shift to non operative management First reported by Simpson et al from Toronto in Twelve patients with clinical diagnosis of solid organ injury (NO CT or US) Hemodynamic stability is the sole determinant of management: No role for age No role for CT grading No role for contrast blush Even if intestinal injury suspected
17
18
19
20 Liver & Spleen Management: Success 90 95% Major concern is delayed Dx of intestinal injury: Occurs in only 2 3.6% of cases with solid organ injury No added morbididty or mortality with delayed diagnosis No justification for laparotomy to exclude it Other concerns: Postraumatic pseudoaneurysms: very low incidence Postraumatic biloma: Can be percutaneously drained Contrast blush on CT: may be associated with increased transfusion requirements but does not alter management Angiographic embolization not well studied and not recommended in pediatric patients Nonoperative management more likely used in pediatric trauma centers

21
22 Liver & Spleen Management: In case of HD instability despite fluids & blood: Splenic injury: Attempt splenic preservation unless spleen massively injured, associated abdominal injuries & HD instability Hepatic injury: Use compression, suture & topical hemostatics For exanguinating injuries (mortality 60 80%): Total hepatic vascular exclusion x 30 min Avoid lethal triad: ph<7.2, PT > 16 sec & temp < 35 c Early application of damage control: Control Hge & soiling, pack and temporary closure. Survival 60% for Grade 4 & 5 25% in Grade 5
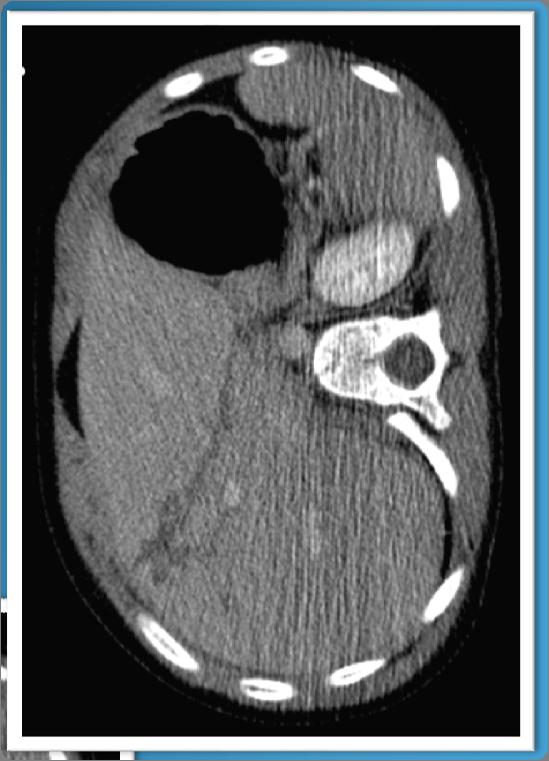
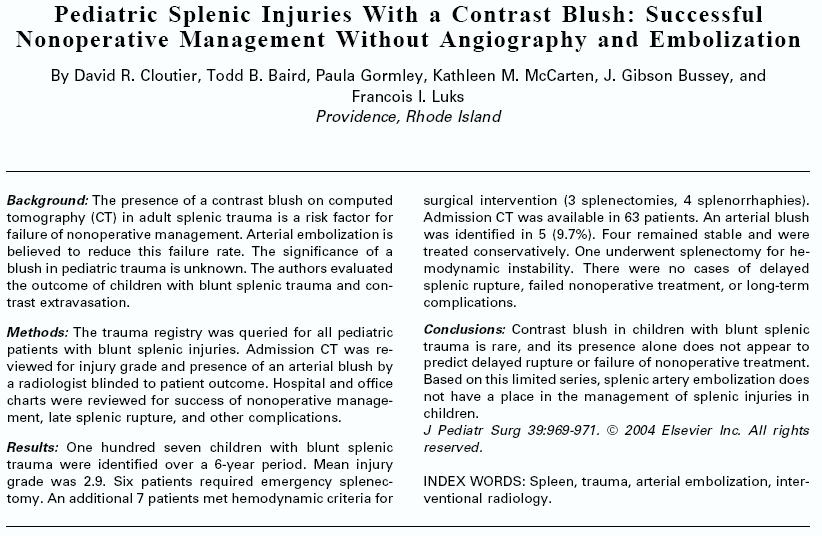
23 IH, 12 yo, slightly obese Fell face down in playground. Rt wrist and left shoulder pain Presented to PCP, X ray right wrist shows nondisplaced distal radial frx Abdominal exam benign in office, patient sent home Abdominal pain and left shoulder pain just outside the office urged mom to ask for a CT of the abdomen Patient sent to ED for CT HD stable Hct
24
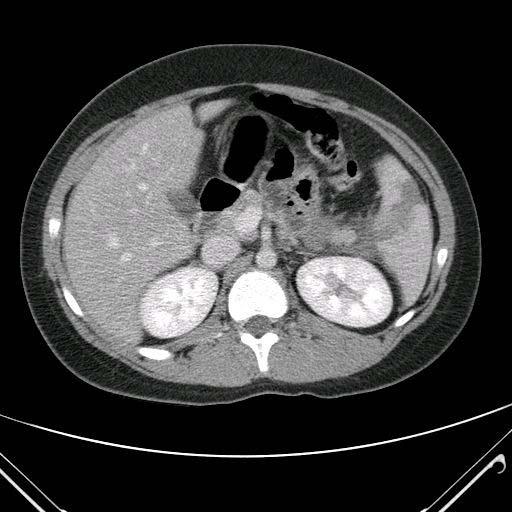
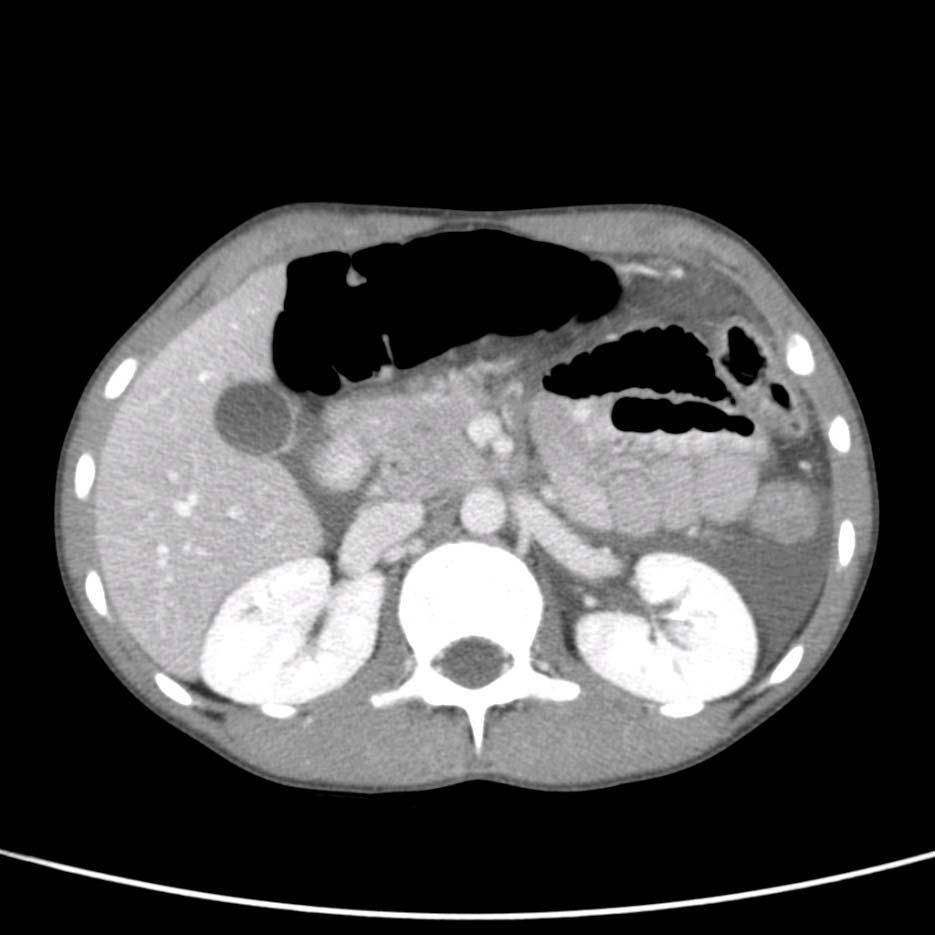
25 JW, 10 yo Riding bike, lost control with handlebar injury to Lt UQ Walked home, one episode of vomiting & some abdominal pain Presented to Urgent care. Exam benign & sent home More pain in AM. Family took him to ED CT obtained HD stable Hct


26

27 Renal injury: Commonest injured genitourinary organ In 10% of patients with blunt abdominal trauma Children more susceptible, particularly in the presence of underlying congenital renal anomalies
28 Renal injury: Hematuria is the most reliable indicator of injury Can be abscent in complete avulsion or thrombosis Microscopic hematuria < 50/HPF usually not associated with serious injury Microscopic hematuria > 50/HPF associated with serious renal injury 8% Gross hematuria associated with serious injury 32% of the time CT scan with IV contrast most useful
29 Renal injury: Only 5% will need surgery Management of Grade I III mostly conservative: Bed rest, abx & serial Hct till gross hematuria resolves Limited activity for 2 4 w till no hematuria Urinary extravasation tted by perc drainage & stenting Management of Grade IV V(10 15%) contraversial: Angio with embolization for persistent hematuria Extravasation treated by perc drainage & stenting Incidence of hypertension very low
30

31 Pancreatic injury: Rare (3 10%) Suspect in cases of handle bar injuries Elevated Amylase highly suggestive but cannot exclude if normal Early spiral CT with IV contrast essential
32 Pancreatic injury: Management contraversial: Aggressive intervention with early ERCP & surgery (San Diego) Non operative management even with complete duct disruption & perc drainage of pseudocyst if develops (Toronto) Conservative management is warranted in most cases Pseudocyst may develop in up to 60% but can be managed conservatively Ductal disruption to the left of the spine best managed by early splenic preserving distal pancreatectomy
33
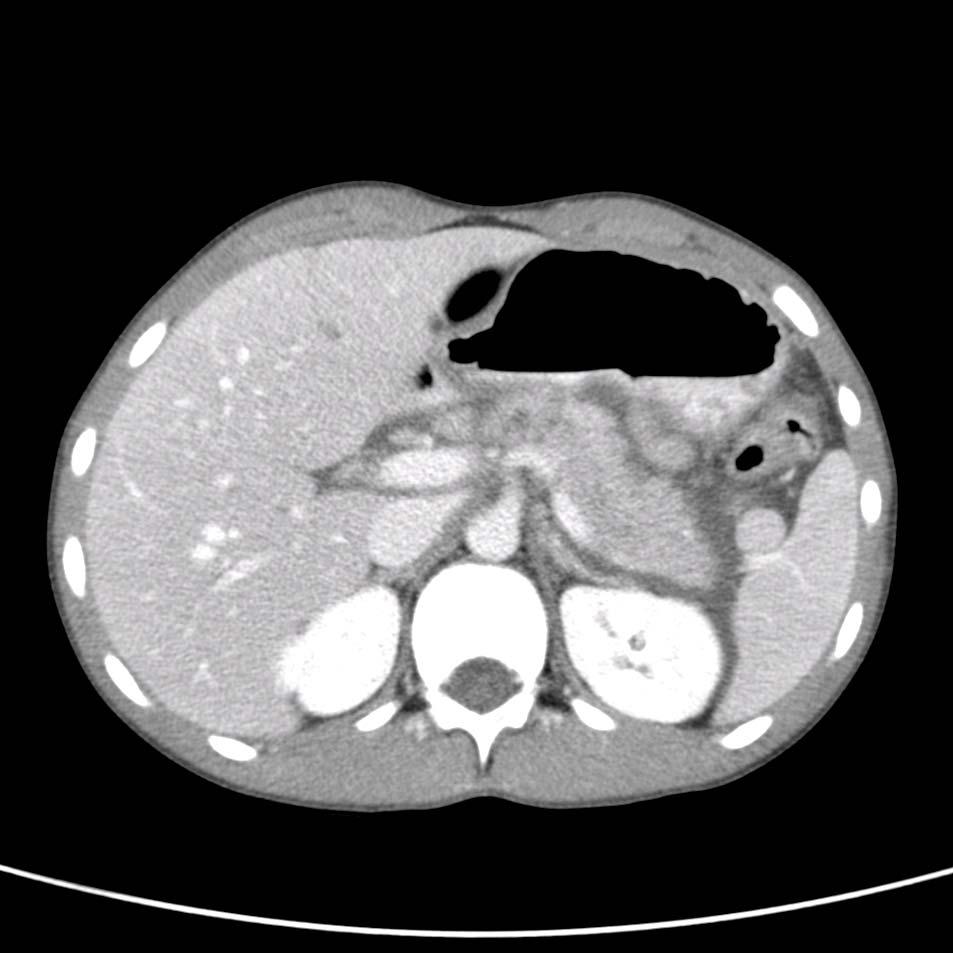
34 CM, 9 yo Vomiting and diffuse abd pain x 1 day. No fevers Presented to ED. WBCs 20.7K and Abd US shows slightly enlarged appendix and free fluid around Diagnosis of appendicitis possibly ruptured made & child admitted to hospital for surgery Exam shows tenderness in epigastrium and none in RT LQ CT obtained
35
36 Amylase 2083 and Lipase 1365 NPO, one dose of Zosyn (for appendicitis) & PICC for TPN Amylase 1259 in 24 h Amylase 237 on day 3, started PO Discharged day 5 tolerating low fat diet with Amylase 201
37 Intestinal injury: 2 3% of patients with blunt abdominal trauma Common with the seat belt complex : 10 15% have intestinal injuries CT scan mandatory Admission for at least 24 hours observation Perforation, hematoma or mesenteric tear with bleeding CT not sensitive unless shows pneumoperitoneum
38 Intestinal injury: More common with seat belt injuries, pancreatic injuries & multiple solid organ injuries Suspect if: Free fluid with no solid organ injury Localized bowel wall thickening Delayed diagnosis common but does not increase morbidity Maintain a high index of suspicion and if in doubt perform diagnostic laparoscopy
39
40 Thank You
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Evaluation of Children with Blunt Abdominal Trauma. James F. Holmes, MD, MPH UC Davis School of Medicine
 Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY
 NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Pediatric Solid Organ Injury
 Pediatric Solid Organ Injury Grand Rounds St. Charles Medical Center Bend, OR July 20, 2018 Disclosures Disclosure of relevant financial relationships in the past 12 months: I have had no relevant financial
Pediatric Solid Organ Injury Grand Rounds St. Charles Medical Center Bend, OR July 20, 2018 Disclosures Disclosure of relevant financial relationships in the past 12 months: I have had no relevant financial
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Pediatric Blunt Abdominal Trauma: Solid Organs, Seatbelts, and Sieverts. 23 March. The Plan. Tucker Redfern Symposium Ramin Jamshidi, MD FACS
 Pediatric Blunt Abdominal Trauma: Solid Organs, Seatbelts, and Sieverts Tucker Redfern Symposium 2018 23 March 1965: Gemini 3 launch 2001: Mir scrapped The Plan Solid Organ Injuries Seat-Belt Trauma Abdominal
Pediatric Blunt Abdominal Trauma: Solid Organs, Seatbelts, and Sieverts Tucker Redfern Symposium 2018 23 March 1965: Gemini 3 launch 2001: Mir scrapped The Plan Solid Organ Injuries Seat-Belt Trauma Abdominal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Pediatric Solid Organ Injuries: Waiting/Watching and Beyond
 Pediatric Solid Organ Injuries: Waiting/Watching and Beyond Ellen Reynolds, MSN, CRNP, CPNP AC/PC PNP, Trauma Clinical Services Children s Hospital of Pittsburgh of UPMC ABDOMINAL INJURIES The Cutting
Pediatric Solid Organ Injuries: Waiting/Watching and Beyond Ellen Reynolds, MSN, CRNP, CPNP AC/PC PNP, Trauma Clinical Services Children s Hospital of Pittsburgh of UPMC ABDOMINAL INJURIES The Cutting
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Pediatric Trauma Karim Rafaat, MD
 Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
Practice Variability in the Management of Pediatric Pancreatic Trauma
 Practice Variability in the Management of Pediatric Pancreatic Trauma Bindi Naik-Mathuria, MD and members of the Pediatric Trauma Study Group Falcone R Burd R Puapong D Mooney D Campbell B Kreyekes N Fenton
Practice Variability in the Management of Pediatric Pancreatic Trauma Bindi Naik-Mathuria, MD and members of the Pediatric Trauma Study Group Falcone R Burd R Puapong D Mooney D Campbell B Kreyekes N Fenton
Guideline for the Management of Blunt Liver and Spleen Injuries
 Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Trauma MedEd. Emphasis: Solid Organ - Spleen January 2012 T RAUMA C ALENDAR OF E VENTS WESTERN TRAUMA ASSOCIATION 42 ND ANNUAL MEETING
 The Trauma Professional s Blog Trauma MedEd Emphasis: Solid Organ - Spleen January 2012 Grading Spleen Injuries - Simplified Spleen injury grading is not as complicated as people think! The grading system
The Trauma Professional s Blog Trauma MedEd Emphasis: Solid Organ - Spleen January 2012 Grading Spleen Injuries - Simplified Spleen injury grading is not as complicated as people think! The grading system
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Nothing
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Nothing
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Question 2. What percentage of abdominal trauma involve the kidney? a) 5 % b) 10% c) 15 % d) 20 %
 5 % b) 10% c) 15 % d) 20 %") Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience
 Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE
 MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center
MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center
Pediatric Trauma. Sept 2nd, Patrick Murphy Neil Merritt
 Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Pediatric Trauma. July 27 th, Suzana Buac, PGY4. Dr. Neil Merritt
 Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
CLINICAL MANAGEMENT GUIDELINE PAGE 1 NO REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12
 CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Morning Report. Allison Haden, MD October 1, 2002
 Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
SAS Journal of Surgery ISSN SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p Available online at
; p Available online at") SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Medical - Clinical Research & Reviews
 Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
LIVER TRAUMA. Jonathan R. Hiatt, MD
 Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder
 Case Reports in Urology Volume 2012, Article ID 430746, 4 pages doi:10.1155/2012/430746 Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder Hazim H. Alhamzawi, 1 Husham
Case Reports in Urology Volume 2012, Article ID 430746, 4 pages doi:10.1155/2012/430746 Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder Hazim H. Alhamzawi, 1 Husham
Reinterventions belong to complications
 Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Objectives. Review ATLS from the pediatric perspective Convince you that children aren t simply little. Impress you with my Power Point mastery
 Pediatric Trauma Objectives Review ATLS from the pediatric perspective Convince you that children aren t simply little adults (especially when it comes to trauma) Impress you with my Power Point mastery
Pediatric Trauma Objectives Review ATLS from the pediatric perspective Convince you that children aren t simply little adults (especially when it comes to trauma) Impress you with my Power Point mastery
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm
 Overall Algorithm") Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
Non Operative Management of Perforated Duodenal Ulcers. Rabih Nemr M.D. Kings County Hospital Sept 2006
 Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS***
 Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
2/16/2019 EMRAM IN-SERVICE REVIEW: TRAUMA 3 ABDOMINAL TRAUMA OUTLINE BLUNT ABDOMINAL TRAUMA DIAPHRAGMATIC INJURIES HOLLOW VISCUS INJURIES
 OUTLINE EMRAM IN-SERVICE REVIEW: TRAUMA 3 ANGELA M. PUGLIESE MD DEPARTMENT OF EMERGENCY MEDICINE HENRY FORD HOSPITAL ABDOMINAL TRAUMA PUNCTURE WOUNDS SPECIAL (SENSITIVE LACERATIONS) LID LACERATIONS GLOBE
OUTLINE EMRAM IN-SERVICE REVIEW: TRAUMA 3 ANGELA M. PUGLIESE MD DEPARTMENT OF EMERGENCY MEDICINE HENRY FORD HOSPITAL ABDOMINAL TRAUMA PUNCTURE WOUNDS SPECIAL (SENSITIVE LACERATIONS) LID LACERATIONS GLOBE
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Scenario #4A: Geriatric Trauma Resuscitation Version-5
 Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
SEP-1 CHALLENGING CASES WITH DR. TOWNSEND
 UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018 OBJECTIVES 1. Summarize
UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018 OBJECTIVES 1. Summarize
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
I have no financial disclosures.
 In the Belly of the Whale: Surviving Thoracoabdominal Trauma Debra Esernio Jenssen, MD, FAAP I have no financial disclosures. Objectives Review epidemiology of abusive chest and abdominal trauma. Identify
In the Belly of the Whale: Surviving Thoracoabdominal Trauma Debra Esernio Jenssen, MD, FAAP I have no financial disclosures. Objectives Review epidemiology of abusive chest and abdominal trauma. Identify
If your patient is stable, perform a complete assessment using inspection, auscultation, percussion, and pal- By Cynthia Blank-Reid, RN, CEN, MSN
 Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Clinical Questions. Clinical Questions. Clinical Questions. Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen
 Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal