ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
|
|
|
- Georgina Walsh
- 5 years ago
- Views:
Transcription
1 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
2 Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10% jejunum, 5 % colon Dominant symptoms: 75% intraabdominal hemorrhage, 25% peritonitis
3 Mechanisms of trauma Deceleration: tears, disruptions Crashing: solid organs External compression: hollowed organs: stomach, bowels, bladder Low energy penetration: stab wounds High energy (high velocity) penetrations: shot wounds, mechanism of cavitation
4 Action at the site of accident 1. Primary examination: open or close trauma 2. Patient's general condition stable vs unstable hemodynamically 3. Venous access 4. Short-acting analgetics 5. Treatment of hypovolemia (rule of 100) 6. What about penetrating items? 7. Wet dresing if evisceration (do not retract) 8. Every significant AT transport to the hospital 9. Continous and repeated monitoring during transport 10. Warning to the target hospital
5 Accident and Emergency Room Patient stable 1. Continous patient monitoring 2. Blood group and #match 3. Medical history closed trauma type of trauma, inensivity, place in the car, position during accident, speed of the car penetrating trauma object (type, size, direction) shot wounds (type of gun, distance, calliber)
6 Accident and Emergency Room Patient stable Wywiad (cd) umiejscowienie bólu nasilenie, zalezność od pozycji, ruchu promieniowanie krwiomocz Badanie przedmiotowe Chory rozebrany Badanie ściany przedniej, bocznych, pleców i krocza Zewnętrzne ślady urazów Napięcie i bolesność powłok Perystaltyka Per rectum Rany kłute sondowanie niewskazane Rany postrzałowe na salę operacyjną
7 1. Combined trauma team 2. Intubation Accident and Emergency Room Patient in deep shock 3. Blod for blood group and #-match, possibly blood gasses. All ather lab tests waste of time 4. Fast fluid transfusion 5. Diagnosis FAST (Focused Assesment with Sonography for Trauma -free fluid-injury to the solid organs in 80-90% cases -sensitivity 44-65% in diagnosis of the retroperitoneal injury -underestimates the extent of the injury 5. Damage Control
8 Damage control RYC 13.3 Kulig J, Nowak W, Ostry Brzuch, PZWL 2009
9 Imaging 1. Chest X-ray 3. Abdominal X-ray - questionable usefulness
10
11 Imaging 1. Chest X-ray 2. Abdominal X-ray 3. FAST 4. CT with contrast or angio CT (vascular trauma) 5. DPL (Diagnostic Peritoneal Lavage) 6. GI Endoscopy DECISION conservative or operative treatment Conservative continous observation Operative preparation for surgery

12 Stomach traumas -Stab and shot wounds -Rarely blunt trauma -Operative treatment
13 Duodenal traumas 2-5% of all abdominal traumas - stab and shot wounds double wall penetration Symptoms Operative treatment difficult to repair high mortality -Blunt trauma posterior wall, retroperitoneal leak
14
15 Small bowel traumas grade description I Wall contusion, haematona, no perforation II III Full thickness wall damage <50% or multiple part thickness Full thickness wall damage >50%, without desruption of the continuity IV desruption of the continuity V desruption of the continuity, ischaemia, segmental necrosis Organ Injury Scaling wg Moore

16
17 20% of all abdominal traumas 80% blunt More frequently right lobe Liver traumas grade description I Subcapsular hematoma <10 cm, tear <1 cm II Subcapsular hematoma <50% surface, intralobar < 10 cm, tear <10 cm dł, <1 cm depth. III Subcapsular hematoma >50% surface, intralobar >10 cm, tear >3 cm depth. IV V VI Damaged 25-75% of parenchyma, tear to 1-3 segments Damaged >75% of parenchyma, tear to >3 segments Separation from large vessels Organ Injury Scaling wg Moore

18 Symptoms -pain -shock -peritoneal symptoms Diagnosis -US Liver traumas Kulig J, Nowak W, Ostry Brzuch, PZWL 2009

19 Diagnosis, cont. CT Kulig J, Nowak W, Ostry Brzuch, PZWL 2009

20 Liver traumas - treatment Kulig J, Nowak W, Ostry Brzuch, PZWL 2009
21 Mechanism blunt trauma penetrating trauma Grading Spleen traumas grade I description Subcapsular hematoma <10 cm, tear <1 cm II Subcapsular hematoma <50% surface, intraparenchymal < 5 cm, tear <1 cm depth. III Subcapsular hematoma >50% surface, intraparenchymal > 5 cm, tear <3 cm depth. IV V Damaged 25-75% of parenchyma Disruption of parenchyma resulting in ischemia Organ Injury Scaling wg Moore

22
23
24 Pancreatic traumas <3% of all abdominal traumas Mostly blunt trauma Combined with injury to other organs grade I II III IV description Small hematoma, pancreatic duct intact Large hematoma, pancreatic duct intact Peripherial disruption of pancreas, pancreatic duct disrupted Head of the pancreas disrupted, pancreatic duct disrupted V Pancreas crushed into multiple fragments Organ Injury Scaling wg Moore
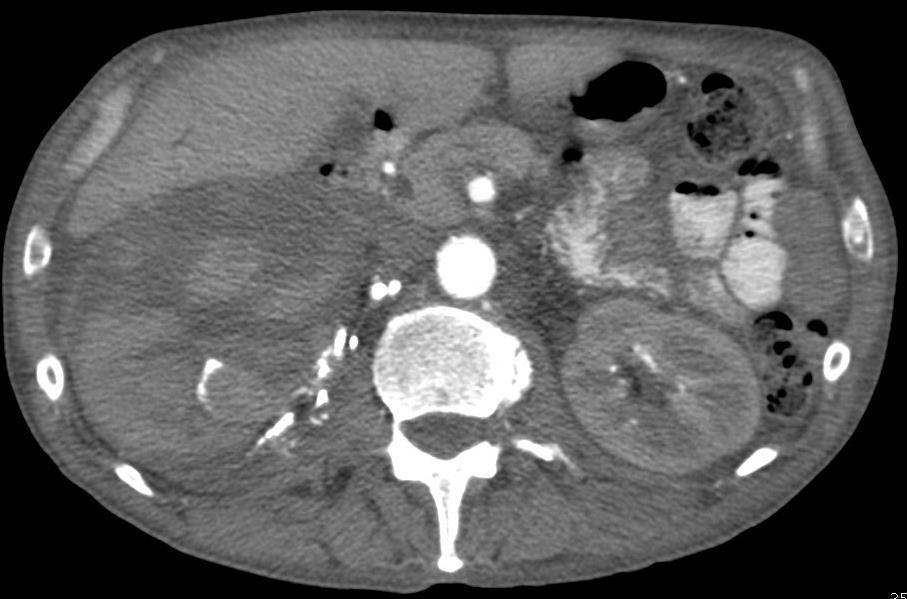
25 Urinary tract traumas -relatively common in abdominal traumas -present in 3-10% -mostly blunt traumas (80-90%) car accidents -deceleration mechanism -penetrating traumas (ca 10%) mostly iatrogenic -isolated kidney injuries -severe injuries combined with other intraabdominal organ injuries -requires surgical treatment in 5-10% cases
26 Symptoms of kidney injury - degree of hematuria and shok related to the severity of the trauma - hematuria absent: disruption of the ureter, renal vessels torn off - indications for CT macroscopic hematuria microscopic hematuria and shock (< 90 mmhg) deceleration, fall, injury to the flank, fractions of the lower ribs or spine Th-L
27 Diagnostic imaging Angiography ia embolisation, stenting, X-Ray pelvic bones fractures, foreign bodies (objects) Urography one-shot intraoperative IVP if patient unstable 2 ml/kg bw and one X-ray shot after 10 min.
28 grade injury Description I II Contussion Hematoma Hematoma Kidney disruption Macro/microhematuria Subcapsular hematoma Perirenal hematoma superficial kidney disruption < 1cm, collection system intact III Kidney disruption Kidney disruption 1cm, collection system intact IV Kidney disruption Injury to the vessels Kidney disruption,collection system disrupted Injury to the renal artery or vein with intrarenal hematoma, segmental infarct without kidney disruption V Kidney disruption Injury to the vessels * grade I-III if affected bilaterally, increase the grade by 1. Kidney fragmented, ureter or renal vessels torn of Oderwanie szypuły lub zakrzepica z zawałem nerki


29
30

31
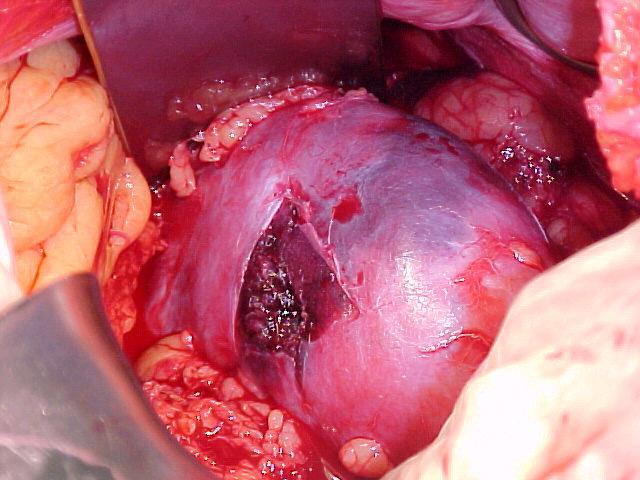
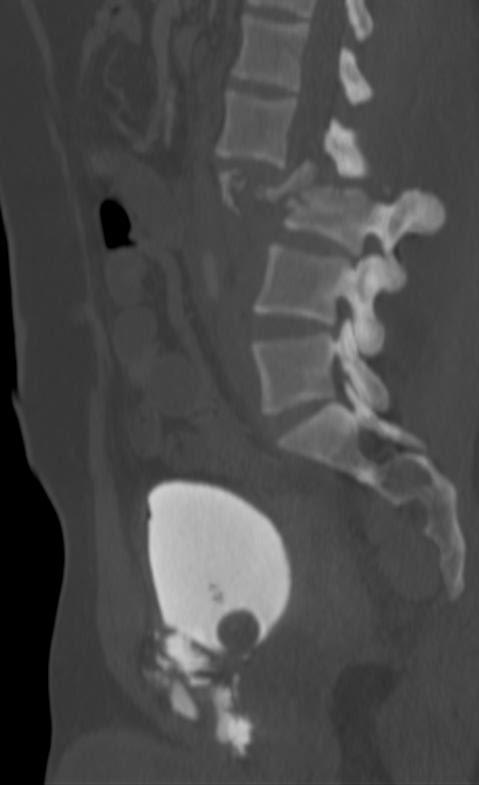
32 Urinary bladder traumas -car accidents, falls, significant trauma to the lower abdomen -in 60-90% combined with pelvic fractures -in 3-4% pelvic fractures combined with bladder injury -retroperitoneal perforation (80-90%) treatment conservative possible -intraperitoneal perforation (5-10%) surgical treatment -in 15% combined with urethral injury -CT cystography (imaging of choice)
33
34 Thank you for your attention
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Question 2. What percentage of abdominal trauma involve the kidney? a) 5 % b) 10% c) 15 % d) 20 %
 5 % b) 10% c) 15 % d) 20 %") Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Urogenital Injuries The role of radiology
 Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Role of Imaging in the evaluation of Renal Trauma
 Role of Imaging in the evaluation of Renal Trauma M. H. Ather,M.A. Noor ( Department of Surgery, The Aga Khan University, Karachi. ) Trauma is the leading cause of morbidity and mortality among young adults
Role of Imaging in the evaluation of Renal Trauma M. H. Ather,M.A. Noor ( Department of Surgery, The Aga Khan University, Karachi. ) Trauma is the leading cause of morbidity and mortality among young adults
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
TRAUMA CARE: ABDOMINAL TRAUMA
 TRAUMA CARE: ABDOMINAL TRAUMA Jassin M. Jouria, MD Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University School of Medicine and
TRAUMA CARE: ABDOMINAL TRAUMA Jassin M. Jouria, MD Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University School of Medicine and
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
UROLOGIC TRAUMA. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 UROLOGIC TRAUMA Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara UROLOGIC TRAUMA Renal trauma Ureteral injury Bladder injury Urethral injury Injury to external genitalia
UROLOGIC TRAUMA Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara UROLOGIC TRAUMA Renal trauma Ureteral injury Bladder injury Urethral injury Injury to external genitalia
TRAUMA SERIES: ABDOMINAL TRAUMA
 TRAUMA SERIES: ABDOMINAL TRAUMA Jassin M. Jouria, MD Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University School of Medicine and
TRAUMA SERIES: ABDOMINAL TRAUMA Jassin M. Jouria, MD Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University School of Medicine and
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS***
 Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
ABDOMINAL TRAUMA. Aurora Health Care EMS Continuing Education 2 nd Quarter 2011 Packet
 Aurora Health Care EMS Continuing Education 2 nd Quarter 2011 Packet ABDOMINAL TRAUMA Blunt and penetrating abdominal trauma are major causes of morbidity and mortality in the United States, particularly
Aurora Health Care EMS Continuing Education 2 nd Quarter 2011 Packet ABDOMINAL TRAUMA Blunt and penetrating abdominal trauma are major causes of morbidity and mortality in the United States, particularly
Urinary tract embolization
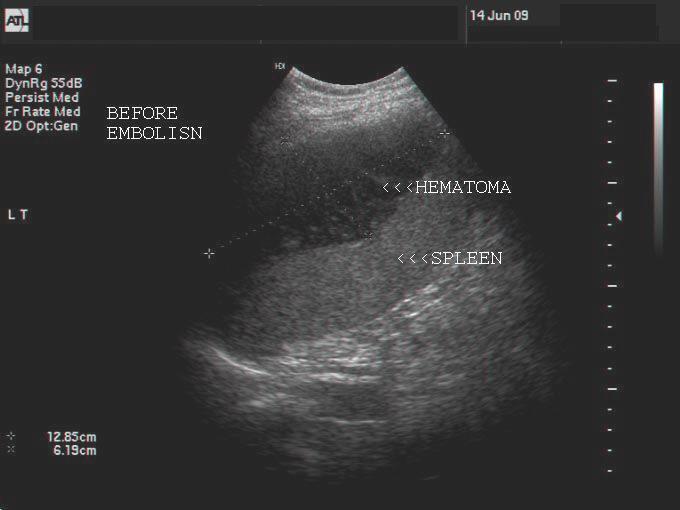
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
SSRG International Journal of Medical Science (SSRG-IJMS) volume 1 Issue 2 December 2014
 volume 1 Issue 2 December 2014") Blunt Abdominal Trauma: Making Decision of Management with Conventional and Ultrasonography Evaluation Dr.Naveen K G 1, Dr. Ravi N 2, Dr. Nagaraj B R 3 1(senior resident-department of radiology, Bangalore
Blunt Abdominal Trauma: Making Decision of Management with Conventional and Ultrasonography Evaluation Dr.Naveen K G 1, Dr. Ravi N 2, Dr. Nagaraj B R 3 1(senior resident-department of radiology, Bangalore
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
I have no financial disclosures.
 In the Belly of the Whale: Surviving Thoracoabdominal Trauma Debra Esernio Jenssen, MD, FAAP I have no financial disclosures. Objectives Review epidemiology of abusive chest and abdominal trauma. Identify
In the Belly of the Whale: Surviving Thoracoabdominal Trauma Debra Esernio Jenssen, MD, FAAP I have no financial disclosures. Objectives Review epidemiology of abusive chest and abdominal trauma. Identify
Genitourinary Tract Injuries
 Genitourinary Tract Injuries Chapter 18 Genitourinary Tract Injuries Introduction Genitourinary injuries constitute approximately 5% of the total injuries encountered in combat. Their treatment adheres
Genitourinary Tract Injuries Chapter 18 Genitourinary Tract Injuries Introduction Genitourinary injuries constitute approximately 5% of the total injuries encountered in combat. Their treatment adheres
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Uroradiology For Medical Students
 Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Review. 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach.
 Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to
 Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
If your patient is stable, perform a complete assessment using inspection, auscultation, percussion, and pal- By Cynthia Blank-Reid, RN, CEN, MSN
 Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
OP-10: ABDOMEN CT USE OF CONTRAST MATERIAL
 Description of Measure OP-10: ABDOMEN CT USE OF CONTRAST MATERIAL This measure calculates the percentage of abdomen studies that are performed with and without contrast out of all abdomen studies performed
Description of Measure OP-10: ABDOMEN CT USE OF CONTRAST MATERIAL This measure calculates the percentage of abdomen studies that are performed with and without contrast out of all abdomen studies performed
CASPER CASPER. COVER Workshop - 13th March 2012 Berlin, Germany CHILD ADVANCED SAFETY PROJECT FOR EUROPEAN ROADS. Abdominal injuries
 CASPER CHILD ADVANCED SAFETY PROJECT FOR EUROPEAN ROADS COVER Workshop - 13th March 2012 Berlin, Germany Content Agenda Context Biomechanical aspects Analysis - per type of CRS - per impact type Influence
CASPER CHILD ADVANCED SAFETY PROJECT FOR EUROPEAN ROADS COVER Workshop - 13th March 2012 Berlin, Germany Content Agenda Context Biomechanical aspects Analysis - per type of CRS - per impact type Influence
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ABDOMINAL TRAUMA MODULE
 INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA. LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital
 MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital
 Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Internal Injury Documentation Guidelines
 Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011
 Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011 Reported: Analysis Summary for: Abdomen Examination Survey Dates 06/13/2011-06/26/2011 Invited Respondents 6,000 Surveys with Demographics
Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011 Reported: Analysis Summary for: Abdomen Examination Survey Dates 06/13/2011-06/26/2011 Invited Respondents 6,000 Surveys with Demographics
Liver lacerations in abdominal trauma management based on anatomical knowledge: A Case report
 American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
CT Images of Blunt Renal Trauma: Correlating the Degree of Hematuria, CT Classification, Treatment and Outcome
 Chin J Radiol 2002; 27: 157-163 157 CT Images of Blunt Renal Trauma: Correlating the Degree of Hematuria, CT Classification, Treatment and Outcome CHUN-JUNG JUAN 1 CHANG-HSIEN LIOU 1 CHUN-JEN HSUEH 1 HUENG-CHEUN
Chin J Radiol 2002; 27: 157-163 157 CT Images of Blunt Renal Trauma: Correlating the Degree of Hematuria, CT Classification, Treatment and Outcome CHUN-JUNG JUAN 1 CHANG-HSIEN LIOU 1 CHUN-JEN HSUEH 1 HUENG-CHEUN
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Guidelines on Urological Trauma
 Guidelines on Urological Trauma N. Djakovic, E. Plas, L. Martínez-Piñeiro, Th. Lynch, Y. Mor, R.A. Santucci, E. Serafetinidis, L.N. Turkeri, M. Hohenfellner European Association of Urology 2012 TABLE OF
Guidelines on Urological Trauma N. Djakovic, E. Plas, L. Martínez-Piñeiro, Th. Lynch, Y. Mor, R.A. Santucci, E. Serafetinidis, L.N. Turkeri, M. Hohenfellner European Association of Urology 2012 TABLE OF
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O
 ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning
 Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Multidetector CT of Blunt Abdominal Trauma 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Reviews and Commentary
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Reviews and Commentary
Review. A. abrasion B. contusion C. hematoma D. avulsion
 Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
Guideline for the Management of Blunt Liver and Spleen Injuries
 Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Office of the Chief Medical Examiner Persons Present
 Office of the Chief Medical Examiner CB # 7580 Chapel Hill, NC 27599-7580 Telephone 9199662253 REPORT OF AUTOPSY EXAMINATION DECEDENT Document Identifier Autopsy Type ME Autopsy Name Roberta Ann Lindsey
Office of the Chief Medical Examiner CB # 7580 Chapel Hill, NC 27599-7580 Telephone 9199662253 REPORT OF AUTOPSY EXAMINATION DECEDENT Document Identifier Autopsy Type ME Autopsy Name Roberta Ann Lindsey
Renal Trauma: Management Options
 Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Prevention of Surgical Injuries in Gynecology
 in Gynecology John K. Chan, M.D. Division of Gynecologic Oncology Overview Review anatomy, etiology, intraoperative, postoperative management, prevention of injuries to: 1. Urinary tract 2. Gastrointestinal
in Gynecology John K. Chan, M.D. Division of Gynecologic Oncology Overview Review anatomy, etiology, intraoperative, postoperative management, prevention of injuries to: 1. Urinary tract 2. Gastrointestinal
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
MDCT Findings of Renal Trauma
 MDT of Renal Trauma Genitourinary Imaging Pictorial Essay Downloaded from www.ajronline.org by 148.251.232.83 on 04/06/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights
MDT of Renal Trauma Genitourinary Imaging Pictorial Essay Downloaded from www.ajronline.org by 148.251.232.83 on 04/06/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
SAS Journal of Surgery ISSN SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p Available online at
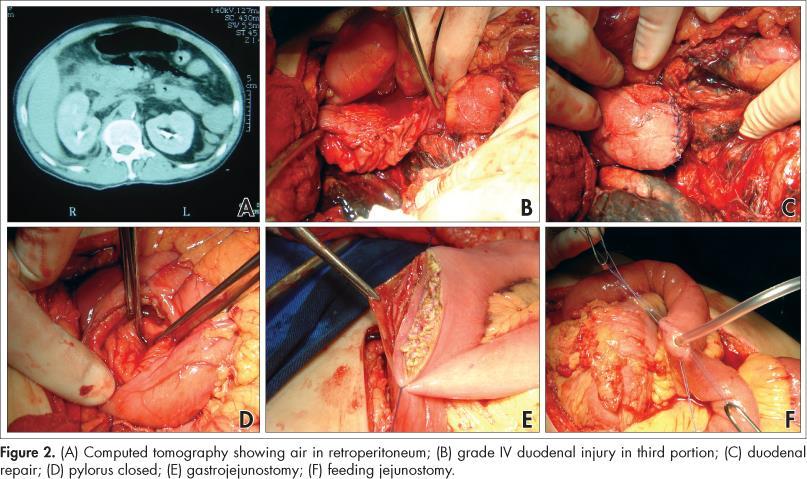
; p Available online at") SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience
 Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
FAST Focused Assessment with Sonography in Trauma
 FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
2018 RN.ORG, S.A., RN.ORG, LLC
 Abdominal Trauma WWW.RN.ORG Reviewed October, 2018, Expires October, 2020 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2018 RN.ORG, S.A., RN.ORG, LLC
Abdominal Trauma WWW.RN.ORG Reviewed October, 2018, Expires October, 2020 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2018 RN.ORG, S.A., RN.ORG, LLC
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
TitleRadiographic evaluation of blunt re. TSUJI, Akira; MATSUZAKI, Shouji; TA. Citation 泌尿器科紀要 (1989), 35(7):
, 35(7):") TitleRadiographic evaluation of blunt re TSUJI, Akira; MATSUZAKI, Shouji; TA Author(s) NAGAKURA, Kazuhiko; MURAI, Masaru; Hiroshi Citation 泌尿器科紀要 (1989), 35(7): 1119-1123 Issue Date 1989-07 URL http://hdl.handle.net/2433/116611
TitleRadiographic evaluation of blunt re TSUJI, Akira; MATSUZAKI, Shouji; TA Author(s) NAGAKURA, Kazuhiko; MURAI, Masaru; Hiroshi Citation 泌尿器科紀要 (1989), 35(7): 1119-1123 Issue Date 1989-07 URL http://hdl.handle.net/2433/116611
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific