Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2012
|
|
|
- Erik Hampton
- 5 years ago
- Views:
Transcription
1 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2012
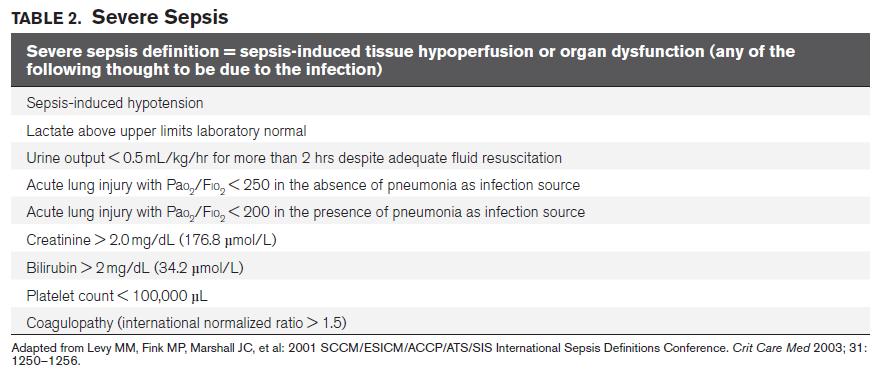
2 Definition Sepsis the presence of infection with systemic manifestations of infection Severe sepsis sepsis plus sepsis-induced organ dysfunction or tissue hypoperfusion Septic shock sepsis-induced hypotension persisting despite adequate fluid resuscitation
3 Definition Sepsis-induced hypotension systolic blood pressure (SBP) < 90 mm Hg mean arterial pressure (MAP) < 70 mm Hg SBP decrease > 40 mmhg or less than two standard deviations below normal for age absence of other causes of hypotension Sepsis-induced tissue hypoperfusion infection-induced hypotension elevated lactate oliguria
4
5
6 History of the Guidelines 2004 The initial SSC guidelines incorporated the evidence available through the end of publication analyzed evidence available through the end of The most current iteration is based on updated literature search incorporated into the evolving manuscript through fall 2012
7 Selection and Organization of Committee Members Appointed by the Society of Critical Care Medicine and European Society of Intensive Care Medicine Sepsis expertise Four clinicians with experience in the GRADE process application (referred to in this document as GRADE group or Evidence-Based Medicine [EBM] group)
8 Search Techniques Search terms sepsis, severe sepsis, septic shock, and sepsis syndrome All questions used in the previous guidelines publications were searched Database MEDLINE, EMBASE, Cochrane Library, ACP Journal Club, Evidence-Based Medicine Journal, Cochrane Registry of Controlled Clinical Trials, International Standard Randomized Controlled Trial Registry
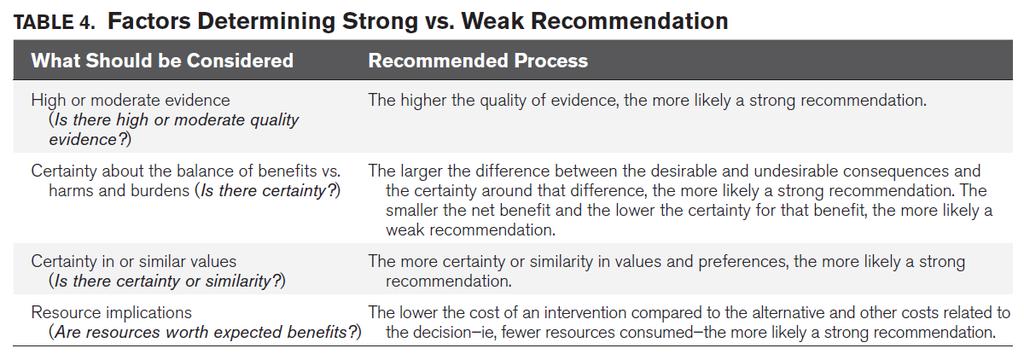
9 Grading Grading of Recommendations Assessment, Development and Evaluation (GRADE) system Quality of evidence High (grade A) Moderate (grade B) Low (grade C) Very low (grade D) Classification of recommendations Strong (grade 1) Weak (grade 2)
10 Grading Throughout the document are a number of statements that either follow graded recommendations or are listed as stand-alone numbered statements followed by ungraded in parentheses (UG).
11 MANAGEMENT OF SEVERE SEPSIS Initial Resuscitation and Infection Issues Hemodynamic Support and Adjunctive Therapy Supportive Therapy of Severe Sepsis
12 Initial Resuscitation and Infection Issues
13 Initial Resuscitation and Infection Issues A. Initial Resuscitation B. Screening for Sepsis and Performance Improvement (New) C. Diagnosis D. Antimicrobial Therapy E. Source Control F. Infection Prevention (New)
14 A. Initial Resuscitation

15 A. Initial Resuscitation 1. We recommend the protocolized, quantitative resuscitation of patients with sepsis-induced tissue hypoperfusion This protocol should be initiated as soon as hypoperfusion is recognized not be delayed pending ICU admission

16 A. Initial Resuscitation The first 6 hrs of resuscitation goals (grade 1C) (1C) : a) CVP 8 12 mm Hg b) MAP 65 mm Hg c) Urine output 0.5 ml/kg/hr d) Superior vena cava oxygenation saturation (ScvO2) 70% or mixed venous oxygen saturation (SvO2) 65%,
17 A. Initial Resuscitation 2. We suggest targeting resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion (grade 2C)
18 B. Screening for Sepsis and Performance Improvement (NEW)
19 B. Screening for Sepsis and Performance Improvement (NEW) 1. We recommend routine screening of potentially infected seriously ill patients for severe sepsis to increase the early identification of sepsis and allow implementation of early sepsis therapy (grade 1C). 2. Performance improvement efforts in severe sepsis should be used to improve patient outcomes (UG).
20 B. Screening for Sepsis and Performance Improvement The early identification of sepsis and implementation of early evidence-based therapies have been documented to improve outcomes and decrease sepsis-related mortality. -- Levy MM, Dellinger RP, Townsend SR, et al; Surviving Sepsis Campaign: The Surviving Sepsis Campaign: Results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med 2010; 38:
21 B. Screening for Sepsis and Performance Improvement Performance improvement efforts in sepsis have been associated with improved patient outcomes Kortgen A, Niederprüm P, Bauer M: implementation of an evidencebased standard operating procedure and outcome in septic shock. Crit Care Med 2006; 34: Rivers EP, Ahrens T: Improving outcomes for severe sepsis and septic shock: Tools for early identification of at-risk patients and treatment protocol implementation. Crit Care Clin 2008; 24(3 Suppl):S1 47 Gao F, Melody T, Daniels DF, et al: The impact of compliance with 6-hour and 24-hour sepsis bundles on hospital mortality in patients with severe sepsis: A prospective observational study. Crit Care 2005; 9:R764 R770 Schorr C: Performance improvement in the management of sepsis. Crit Care Clin 2009; 25: Girardis M, Rinaldi L, Donno L, et al; Sopravvivere alla Sepsi Group of the Modena-University Hospital: Effects on management and outcome of severe sepsis and septic shock patients admitted to the intensive care unit after implementation of a sepsis program: A pilot study. Crit Care 2009; 13:R143 Pestaña D, Espinosa E, Sangüesa-Molina JR, et al; REASEP Sepsis Study Group: Compliance with a sepsis bundle and its effect on intensive care unit mortality in surgical septic shock patients. J Trauma 2010; 69:
22 B. Screening for Sepsis and Performance Improvement Evaluation of process change requires Consistent education Protocol development and implementation Data collection Measurement of indicators Feedback to facilitate the continuous performance improvement
23 B. Screening for Sepsis and Performance Improvement Application of the SSC sepsis bundles led to sustained, continuous quality improvement in sepsis care and was associated with reduced mortality Analysis of the data from nearly 32,000 patient charts gathered from 239 hospitals in 17 countries through September 2011 as part of phase III of the campaign informed the revision of the bundles in conjunction with the 2012 guidelines

24 B. Screening for Sepsis and Performance Improvement In 2012 version the management bundle was dropped the resuscitation bundle was broken into two parts and modified
25 B. Screening for Sepsis and Performance Improvement
26 C. Diagnosis

27 C. Diagnosis 1.We recommend obtaining appropriate cultures before antimicrobial therapy is initiated if such cultures do not cause significant delay (> 45 minutes) in the start of antimicrobial(s) administration (grade 1C) (1C)
28 C. Diagnosis 2. We suggest the use of the 1,3 β-d-glucan assay (grade 2B), mannan and anti-mannan antibody assays (grade 2C) when invasive candidiasis is in the differential diagnosis of infection. (New)

29 C. Diagnosis 3. We recommend that imaging studies be performed promptly in attempts to confirm a potential source of infection (UG).
30 C. Diagnosis Blood culture Obtaining at least two sets of blood cultures (both aerobic and anaerobic bottles) before antimicrobial therapy, At least one drawn percutaneously and one drawn through each vascular access device, unless the device was recently (< 48 hours) inserted Can be drawn at the same time if they are obtained from different sites
31 C. Diagnosis Cultures of other sites should also be obtained before antimicrobial therapy if doing so does not cause significant delay in antibiotic administration (grade 1C). such as urine, cerebrospinal fluid, wounds, respiratory secretions, or other body fluids that may be the source of infection
32 C. Diagnosis The Gram stain can be useful in particular for respiratory tract specimens, to determine if inflammatory cells are present Rapid influenza antigen testing during periods of increased influenza activity in the community is also recommended
33 C. Diagnosis The potential role of biomarkers (PCT, CRP) for diagnosis of infection in patients presenting with severe sepsis remains undefined for distinguish between severe infection and other acute inflammatory states, no recommendation can be given for discriminate the acute inflammatory pattern of sepsis from other causes of generalized inflammation (eg, postoperative, other forms of shock) has not been demonstrated.
34 C. Diagnosis Imaging studies Potential sources of infection should be sampled as they are identified Consideration of patient risk for transport and invasive procedures (eg, careful coordination and aggressive monitoring if the decision is made to transport for a CTguided needle aspiration). Bedside studies, such as ultrasound, may avoid patient transport
35 D. Antimicrobial Therapy

 (1B) and severe sepsis without septic shock (grade 1C)")
36 D. Antimicrobial Therapy 1. The administration of effective intravenous antimicrobials within the first hour of recognition of septic shock (grade 1B) (1B) and severe sepsis without septic shock (grade 1C) (1D) should be the goal of therapy.

37 D. Antimicrobial Therapy 2a. We recommend that initial empiric anti-infective therapy include one or more drugs that have activity against all likely pathogens (bacterial and/or fungal or viral) that penetrate in adequate concentrations into the tissues presumed to be the source of sepsis (grade 1B) (1B)

38 D. Antimicrobial Therapy 2b. The antimicrobial regimen should be reassessed daily for potential de-escalation to prevent the development of resistance, to reduce toxicity, and to reduce costs (grade 1B) (1C).
39 D. Antimicrobial Therapy 3. We suggest the use of low procalcitonin levels or similar biomarkers to assist the clinician in the discontinuation of empiric antibiotics in patients who appeared septic, but have no subsequent evidence of infection (grade 2C).
40 D. Antimicrobial Therapy 4a. Empiric therapy should attempt to provide antimicrobial activity against the most likely pathogens We suggest combination empiric therapy for neutropenic patients with severe sepsis (grade 2B) (2D) difficult-to-treat, multidrug-resistant bacterial pathogens such as Acinetobacter and Pseudomonas spp. (grade 2B).
41 D. Antimicrobial Therapy 4a. For selected patients with severe infections associated with respiratory failure and septic shock for P. aeruginosa bacteremia combination therapy with an extended spectrum beta-lactam and either an aminoglycoside or a fluoroquinolone is suggested (grade 2B) (2D). for Streptococcus pneumoniae bacteremia a more complex combination of beta-lactam and a macrolide is suggested for patients with septic shock (grade 2B).
 (2D).")
42 D. Antimicrobial Therapy 4b. We suggest that combination therapy, when used empirically in patients with severe sepsis, should not be administered for longer than 3 to 5 days. De-escalation to the most appropriate single-agent therapy should be performed as soon as the susceptibility profile is known (grade 2B) (2D). Exceptions would include aminoglycoside monotherapy, which should be generally avoided, particularly for P. aeruginosa sepsis, and for selected forms of endocarditis, where prolonged courses of combinations of antibiotics are warranted
 (1D) Longer courses may be appropriate in patients who have a slow")
43 D. Antimicrobial Therapy 5. We suggest that the duration of therapy typically be 7 to 10 days if clinically indicated(grade 2C) (1D) Longer courses may be appropriate in patients who have a slow clinical response undrainable foci of infection bacteremia with S. aureus some fungal and viral infections immunologic deficiencies, including neutropenia
. 7.")
44 D. Antimicrobial Therapy 6. We suggest that antiviral therapy be initiated as early as possible in patients with severe sepsis or septic shock of viral origin (grade 2C). 7. We recommend that antimicrobial agents not be used in patients with severe inflammatory states determined to be of noninfectious cause (UG) (1D)
45 E. Source Control

46 E. Source Control 1. We recommend that a specific anatomical diagnosis of infection requiring consideration for emergent source control be sought and diagnosed or excluded as rapidly as possible intervention be undertaken for source control within the first 12 hr after the diagnosis is made, if feasible (grade 1C). (necrotizing soft tissue infection, peritonitis, cholangitis, intestinal infarction)

47 E. Source Control 2. We suggest that when infected peripancreatic necrosis is identified as a potential source of infection, definitive intervention is best delayed until adequate demarcation of viable and nonviable tissues has occurred (grade 2B) (2B).

48 E. Source Control 3. When source control in a severely septic patient is required, the effective intervention associated with the least physiologic insult should be used (eg, percutaneous rather than surgical drainage of an abscess) (UG) (1D).

49 E. Source Control 4. If intravascular access devices are a possible source of severe sepsis or septic shock, they should be removed promptly after other vascular access has been established (UG) (1C).
50 F. Infection Prevention (New)
51 F. Infection Prevention (New) 1a. We suggest that selective oral decontamination (SOD) and selective digestive decontamination (SDD) should be introduced and investigated as a method to reduce the incidence of ventilator-associated pneumonia (VAP); this infection control measure can then be instituted in healthcare settings and regions where this methodology is found to be effective (grade 2B).
52 F. Infection Prevention 1b. We suggest oral chlorhexidine gluconate (CHG) be used as a form of oropharyngeal decontamination to reduce the risk of VAP in ICU patients with severe sepsis (grade 2B).
53 F. Infection Prevention Careful infection control practices should be instituted during the care of septic patients as reviewed in the nursing considerations for the Surviving Sepsis Campaign hand washing expert nursing care, catheter care barrier precautions airway management elevation of the head of the bed subglottic suctioning
54 To Be Continue.Thank You
55
56
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
 Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Early Physical Rehabilitation in the ICU and Ventilator Liberation
 Early Physical Rehabilitation in the ICU and Ventilator Liberation 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Respiratory Care 2012 Oct Vol 57 No 10 Pedro A Mendez-Tellez MD and Dale M Needham MD PhD
Early Physical Rehabilitation in the ICU and Ventilator Liberation 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Respiratory Care 2012 Oct Vol 57 No 10 Pedro A Mendez-Tellez MD and Dale M Needham MD PhD
The clinical implication and prognostic predictors of Tigecycline treatment for pneumonia involving multidrug-resistant Acinetobacter baumannii
 Journal of Infection (2011) 63, 351e361 The clinical implication and prognostic predictors of Tigecycline treatment for pneumonia involving multidrug-resistant Acinetobacter baumannii R 陳南丞 VS 余文良醫師 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Journal of Infection (2011) 63, 351e361 The clinical implication and prognostic predictors of Tigecycline treatment for pneumonia involving multidrug-resistant Acinetobacter baumannii R 陳南丞 VS 余文良醫師 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Tracheostomy practice in adults with acute respiratory failure
 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Tracheostomy practice in adults with acute respiratory failure Bradley D. Freeman, MD, FACS; Peter E. Morris, MD, FCCP Crit Care Med 2012 Vol. 40, No. 10
本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Tracheostomy practice in adults with acute respiratory failure Bradley D. Freeman, MD, FACS; Peter E. Morris, MD, FCCP Crit Care Med 2012 Vol. 40, No. 10
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
PROTON PUMP INHIBITOR AND CLOPIDOGREL INTERACTION: Am J Gastroenterol Jan;105(1): Epub 2009 Nov 10.
: Epub 2009 Nov 10.") PROTON PUMP INHIBITOR AND CLOPIDOGREL INTERACTION: FACT OR FICTION? 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Am J Gastroenterol. 2010 Jan;105(1):34-41. Epub 2009 Nov 10. Introduction Current consensus
PROTON PUMP INHIBITOR AND CLOPIDOGREL INTERACTION: FACT OR FICTION? 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Am J Gastroenterol. 2010 Jan;105(1):34-41. Epub 2009 Nov 10. Introduction Current consensus
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Journal meeting. 時間 : Aug 4, 2014 地點 : ICU 討論室報告者 : 陳信宏主治醫師 : 楊俊杰醫師
 Journal meeting 時間 : Aug 4, 2014 地點 : ICU 討論室報告者 : 陳信宏主治醫師 : 楊俊杰醫師 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 What is the future of ARDS after the Berlin definition? Carmen S.V. Barbas, Alexandre M.
Journal meeting 時間 : Aug 4, 2014 地點 : ICU 討論室報告者 : 陳信宏主治醫師 : 楊俊杰醫師 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 What is the future of ARDS after the Berlin definition? Carmen S.V. Barbas, Alexandre M.
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of
 Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Management of Septic Shock
 The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
EBM EGDT 每次都是RCT.有點煩 本來想簡單處理 那些年我們曾經打拼過的~~ By Maxy Lu 這次想要放鬆一下~~ EGDT (Early goal-directed therapy) Early go to ICU
 Early go to ICU") EBM 2014.03.24 By Maxy Lu 每次都是RCT.有點煩 這次想要放鬆一下~~ 本來想簡單處理 EGDT (Early goal-directed therapy) 那些年我們曾經打拼過的~~ EGDT Early go to ICU 想說這下開心了 Best practice Not Standard of care Screening and practice improvement
EBM 2014.03.24 By Maxy Lu 每次都是RCT.有點煩 這次想要放鬆一下~~ 本來想簡單處理 EGDT (Early goal-directed therapy) 那些年我們曾經打拼過的~~ EGDT Early go to ICU 想說這下開心了 Best practice Not Standard of care Screening and practice improvement
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
TERMINOLOGY SIRS 10/30/2014 SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU
 Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
ISF criteria (International sepsis forum consensus conference of infection in the ICU) Secondary peritonitis
 Secondary peritonitis") Appendix with supplementary material. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Supplementary Tables Table S1. Definitions
Appendix with supplementary material. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Supplementary Tables Table S1. Definitions
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
SEPSIS MANAGEMENT. Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah
 Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah") SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Vocal cord dysfunction: what do we know? K. Kenn and R. Balkissoon European Respiratory Journal 2011; 37:
 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Vocal cord dysfunction: what do we know? K. Kenn and R. Balkissoon European Respiratory Journal 2011; 37: 194 200 Introduction Refractory or severe asthma
本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Vocal cord dysfunction: what do we know? K. Kenn and R. Balkissoon European Respiratory Journal 2011; 37: 194 200 Introduction Refractory or severe asthma
VAP Prevention bundles
 VAP Prevention bundles Dr. Shafiq A.Alimad MD Head of medical department at USTH YICID workshop, 15-12-2014 Care Bundles What are they & why use them? What are Care Bundles? Types of Care Bundles available
VAP Prevention bundles Dr. Shafiq A.Alimad MD Head of medical department at USTH YICID workshop, 15-12-2014 Care Bundles What are they & why use them? What are Care Bundles? Types of Care Bundles available
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock, 2012
 Intensive Care Med (2013) 39:165 228 DOI 10.1007/s00134-012-2769-8 GUIDELINES R. P. Dellinger Mitchell M. Levy Andrew Rhodes Djillali Annane Herwig Gerlach Steven M. Opal Jonathan E. Sevransky Charles
Intensive Care Med (2013) 39:165 228 DOI 10.1007/s00134-012-2769-8 GUIDELINES R. P. Dellinger Mitchell M. Levy Andrew Rhodes Djillali Annane Herwig Gerlach Steven M. Opal Jonathan E. Sevransky Charles
AN INTRODUCTION TO EXTRACORPOREAL BLOOD PURIFICATION IN CRITICAL ILLNESS. Proceedings of Singapore Healthcare Volume 21 Number
 AN INTRODUCTION TO EXTRACORPOREAL BLOOD PURIFICATION IN CRITICAL ILLNESS Proceedings of Singapore Healthcare Volume 21 Number 2 2012 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Mechanisms of Extracorporeal
AN INTRODUCTION TO EXTRACORPOREAL BLOOD PURIFICATION IN CRITICAL ILLNESS Proceedings of Singapore Healthcare Volume 21 Number 2 2012 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Mechanisms of Extracorporeal
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Sepsis Update: Early Identification and Management
 Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Sepsis Review. Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center
 Sepsis Review Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org Discuss the Updated International Guidelines Discuss how you
Sepsis Review Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org Discuss the Updated International Guidelines Discuss how you
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
5/1/2015 SEPSIS SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 INFECTION CAN BE CONFIRMED BY:
 SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Sepsis Update Disclosures. Definitions. Objectives. Diagnosis. Diagnosis 9/21/15
 Sepsis Update 2015 Nathaniel D. Curl, MD FACEP UnityPoint Health-Trinity Disclosures I received an all-expenses paid trip in March 2011 from Edwards, the manufacturer of the PreSep catheter, to attend
Sepsis Update 2015 Nathaniel D. Curl, MD FACEP UnityPoint Health-Trinity Disclosures I received an all-expenses paid trip in March 2011 from Edwards, the manufacturer of the PreSep catheter, to attend
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency
 BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency Medicine 1 NO CONFLICT OF INTEREST 2 We do not fully understand
BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency Medicine 1 NO CONFLICT OF INTEREST 2 We do not fully understand
Educational Workshop
 Educational Workshop EW02: Management of severe sepsis and septic shock anno 2015 Arranged with ESGBIS & International Sepsis Forum (ISF) Convenors: W. Joost Wiersinga, Amsterdam, NL Tom van der Poll,
Educational Workshop EW02: Management of severe sepsis and septic shock anno 2015 Arranged with ESGBIS & International Sepsis Forum (ISF) Convenors: W. Joost Wiersinga, Amsterdam, NL Tom van der Poll,
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
Bacteriemia and sepsis
 Bacteriemia and sepsis Case 1 An 80-year-old man is brought to the emergency room by his son, who noted that his father had become lethargic and has decreased urination over the past 4 days. The patient
Bacteriemia and sepsis Case 1 An 80-year-old man is brought to the emergency room by his son, who noted that his father had become lethargic and has decreased urination over the past 4 days. The patient
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center
 UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Guidebook for ED and Inpatient Sepsis Order Set Initiatives 2018
 Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Saving Lives: Focusing on Severe Sepsis and Septic Shock
 Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Jarisch A. Kreislauffragen, Dünser et al. Critical Care 2013, 17:326 Sunday, March 30, 14
 It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Sepsis - A Year in Transition
 Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis: Getting to ZERO Probable or Impossible?
 Sepsis: Getting to ZERO Probable or Impossible? Carol A Rauen, RN-BC, MS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant. Burn Trauma ICU, Sentara Norfolk General, VA Sepsis
Sepsis: Getting to ZERO Probable or Impossible? Carol A Rauen, RN-BC, MS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant. Burn Trauma ICU, Sentara Norfolk General, VA Sepsis
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Critical Care Medicine: Landmarks and Legends 1305 Matthew R. Rosengart
 CRITICAL CARE FOR THE GENERAL SURGEON Foreword Ronald F. Martin xiii Preface Juan Carlos Puyana and Matthew R. Rosengart xvii Critical Care Medicine: Landmarks and Legends 1305 Matthew R. Rosengart Critical
CRITICAL CARE FOR THE GENERAL SURGEON Foreword Ronald F. Martin xiii Preface Juan Carlos Puyana and Matthew R. Rosengart xvii Critical Care Medicine: Landmarks and Legends 1305 Matthew R. Rosengart Critical
The EM Educator Series
 The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP
 Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP Objectives Review the changes to the 2012 sepsis guidelines and the 2016 Sepsis Guidelines Discuss the literature impacting the sepsis
Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP Objectives Review the changes to the 2012 sepsis guidelines and the 2016 Sepsis Guidelines Discuss the literature impacting the sepsis
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Last frontier of infection in critically ill patients
 Last frontier of infection in critically ill patients Nick Beeching Tropical & Infectious Disease Unit Royal Liverpool University Hospital Liverpool School of Tropical Medicine Liverpool School of Tropical
Last frontier of infection in critically ill patients Nick Beeching Tropical & Infectious Disease Unit Royal Liverpool University Hospital Liverpool School of Tropical Medicine Liverpool School of Tropical
From Bench to Bedside: Reducing Sepsis Mortality
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/from-bench-to-bedside-reducing-sepsismortality/4009/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/from-bench-to-bedside-reducing-sepsismortality/4009/
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Potential Conflicts of Interests
 Potential Conflicts of Interests Research Grants Agency for Healthcare Research and Quality Akers Bioscience, Inc. Pfizer, Inc. Scientific Advisory Boards Pfizer, Inc. Cadence Pharmaceuticals Kimberly
Potential Conflicts of Interests Research Grants Agency for Healthcare Research and Quality Akers Bioscience, Inc. Pfizer, Inc. Scientific Advisory Boards Pfizer, Inc. Cadence Pharmaceuticals Kimberly
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Nosocomial Pneumonia. <5 Days: Non-Multidrug-Resistant Bacteria
 Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000