The Management of Septic Shock
|
|
|
- Darcy Lynch
- 5 years ago
- Views:
Transcription
1 The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine
2 No conflicts No disclosures Conflicts & Disclosures
3 Overview and Objectives Definitions and clinical criteria for diagnosis Epidemiology Recognition Early Goal Directed Therapy Recent sepsis resuscitation trials Surviving Sepsis Guidelines
4 Overview of Surviving Sepsis Guidelines Initial Resuscitation Fluid Therapy Vasopressor Therapy Inotropic Therapy Antibiotics & Other Therapies Source Control
5 Definitions & Clinical Criteria
6 Definitions of Sepsis A clinical syndrome not a specific disease with a single specific cause e.g. Flu-like syndrome vs actual influenza virus infection We use syndromes to more easily recognize and prevent morbidity and mortality with common illness, e.g. asthma, hypertension, flu and sepsis Infection-induced systemic inflammatory response Recognition of sepsis syndrome severity is also important Bone RC et al, Chest 1992;101:1644
7 Systemic Inflammatory Response Syndrome (SIRS) Criteria Temperature > 38 C or < 36 C Heart rate > 90 Respiratory rate > 20 PaCO2 < 32 mm Hg WBC > 12 or < 4 > 10% Bands/Immature Segs THeRe are CO2WBoyS mnemonic

8 Definitions of Sepsis Severity Possible Sepsis 2 or more SIRS criteria Confirmed Sepsis OR suspected infection Severe Sepsis ANY organ dysfunction Septic Shock Refractory Septic Shock Annane et al, Lancet 2005;365:63 After initial fluid bolus High-dose vasopressors

9 Sepsis = SIRS + Infection BACTEREMIA TRAUMA INFECTION FUNGEMIA SEPSIS SIRS BURNS PARASITEMIA VIREMIA OTHER OTHER PANCREATITIS Bone RC et al, Chest 1992;101:1644
10 SIRS vs Sepsis Severity-Mortality Sepsis severity is more than just numbers! Martin et al, NEJM 2003; 348:
11 SIRS vs Sepsis Severity-Mortality NEJM 2015: ANZICS group: You don t have to meet 2 SIRS criteria to die of sepsis! Kaukonen et al, NEJM 2015; 327:
12 Epidemiology
13 Epidemiology of Sepsis-Incidence It s Not Just the Years, but the Miles Age Male sex African American Acute organ failure Renal Cardiovascular Neurological Respiratory Co-morbidities Diabetes Malignancy Alcoholism HIV infection Immunosuppression Chronic organ failure CHF Chronic liver disease Martin et al, NEJM 2003; 348:
14 Recognition Always begins with the ABCs And a high index of suspicion Sepsis-Induced Organ Dysfunction

15 Always start at the beginning A: Airway: Independent life is impossible without it B: Breathing: 53% of both arms of the Early Goal- Directed Therapy landmark RCT were intubated within 6 hours Circulation: Assess organ perfusion & IV access: BP, skin, mental status, elevated lactate levels (>2 mmol/l)
.")
16 Early NMB in Severe Sepsis with MV Cohort In 3,518 patients matched on the propensity for treatment, receipt of a neuromuscular blocking agent was associated with a reduced risk of inhospital mortality (risk ratio, 0.88; 95% CI, 0.80, 0.96). Steingrub et al Crit Care Med 2014 Steingrub et al Crit Care Med 2014
17 Sepsis Induced Organ Dysfunction Vascular: Relative IVVD Hypotension Cardiac: Sepsis cardiomyopathy Pulmonary: Noncardiogenic pulmonary edema ARDS Renal: Intravascular volume depletion Hypoperfusion Acute Kidney Injury (AKI) Acute tubular necrosis (ATN) GI: Stress ulceration, hypoalbuminemia, gut bacterial translocation
18 Sepsis Induced Organ Dysfunction Blood: Decreased RBC deformability Hemolysis and microthrombi Impaired microcirculation Global tissue hypoxia Platelets: Nonspecific tissue activation Microthrombi; platelet consumption DIC with bleeding and clotting risks Leukocyte & Compliment : Activation Indiscriminate organ injury Brain: Encephalopathy, confusion, agitation are NOT benign (e.g. CURB-65 mortality indicator in pneumonia)
19 Sepsis Induced Organ Dysfunction Skin: EARLY: Vasodilated, high cardiac output WARM LATE: Intravascular hypovolemia, poor cardiac output, shunting to vital organs, microthrombi COLD Mottling Petechiae and purpura with DIC

20 Skin Mottling Predicts Sepsis Mortality
 In meningococcemia called purpura")
21 Disseminated Intravascular Coagulation (DIC) In meningococcemia called purpura fulminans
22 Early Goal-Directed Therapy A revolution in the care of septic shock
23 Early Goal-Directed Therapy Randomized, prospective, single center trial treatment 260 patients randomized 2/4 SIRS criteria and SBP < 90 mmhg or lactate > 4 mmol/l Patients randomized to 6 hours of goal-directed therapy vs standard therapy Rivers et al, NEJM 2001
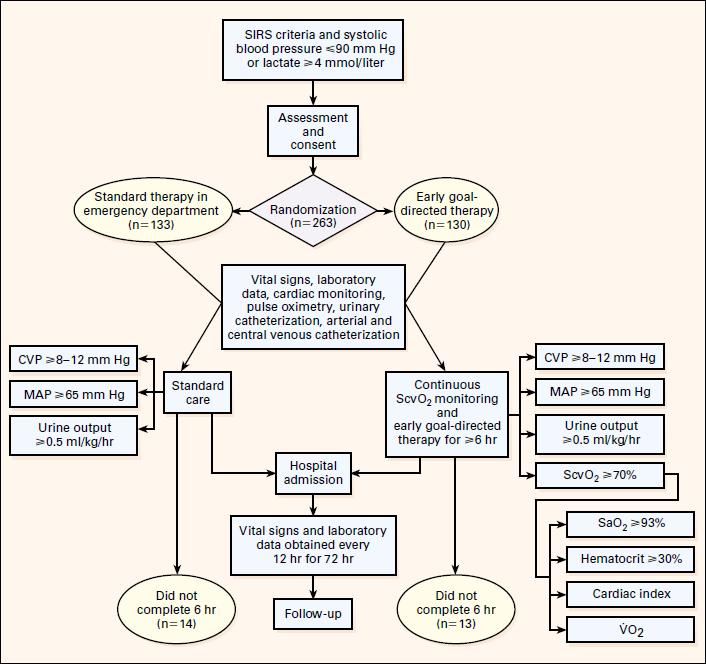
24 Randomization 6 hours

25 EGDT- Protocol In Depth IF good findings move down; IF bad turn right! mm if MV 53% Prior to EGDT all pts received a cc/kg bolus of 0.9% saline 500 cc every 30 min NE/Epi/Dopa/PE RBCs Dobutamine


26 EGDT: Results ARR Death = = 16% NNT = 7
27 EGDT: Results EGDT Treatment Group Differences in the first 6 hrs: 1. More IVF 2. More PRBC 3. More ionotrope <100 cc At 72 hrs the total IVF difference between groups?


28 ARISE the PROMISE of a new PROCESS

29 Surviving Sepsis Guidelines for the Management of Severe Sepsis & Septic Shock And some of the supporting evidence Formed in 2002

30 The Surviving Sepsis Guidelines
31 Recommendation #1: Initial Resuscitation We recommend the protocolized, quantitative resuscitation of patients with sepsis-induced tissue hypoperfusion (defined as hypotension persisting after initial fluid challenge or lactate 4 mmol/l). This protocol should be initiated as soon as hypoperfusion is recognized and should not be delayed pending ICU admission. We suggest, in patients with elevated lactate levels as a marker of tissue hypoperfusion, targeting resuscitation to normalize lactate as rapidly as possible. (Grade 2C)

32 Recommendation #1: Initial Resuscitation GOALS
33 The Surviving Sepsis Guidelines
 Jones A. JAMA.")
34 The Evidence: Lactate Clearance Mortality (%) Jones A. JAMA. 2010;303:
35 The Evidence: Lactate Clearance Adjusted HR= 0.61; adjusted 95% CI, ; HR= P= 0.61; % CI, ; P= Lactate vs Control 348 patients: decrease in lactate levels of 20% or more in the first 8 hours, in addition to ScvO 2 target achievement, and was associated with a 9.6% absolute reduction in mortality Jansen TC. Am J Respir Crit Care Med. 2010;182:
36 Recommendation #2: Fluid Therapy We recommend crystalloids be used as the initial fluid of choice in the resuscitation of severe sepsis and septic shock. (Grade 1B) We recommend against the use of hydroxy- ethyl starches for fluid resuscitation of severe sepsis and septic shock. (Grade 1B) We recommend an initial fluid challenge in patients with sepsis-induced tissue hypoperfusion with suspicion of hypovolemia to achieve a minimum of 30 ml/kg of crystalloids (a portion of this may be albumin equivalent). More rapid administration and greater amounts of fluid may be needed in some patients. (Grade 1C)
37 Recommendation #2: Fluid Therapy We recommend that a fluid challenge technique be applied wherein fluid administration is continued as long as there is hemodynamic improvement either based on dynamic (eg, change in pulse pressure, stroke volume variation) or static (eg, arterial pressure, heart rate) variables (Ungraded). My favorite quote A fluid bolus is a liter or more in thirty minutes or less and more may need to be given R. Phillip Dellinger, Surviving Sepsis Guidelines
38 The Evidence: Albumin vs. Crystalloid ALBIOS Study Caironi et al, N Engl J Med 2014; 370:
39 The Evidence: Albumin vs. Crystalloid Albumin recommended in severe sepsis and septic shock when significant crystalloid has been given Christian J. Wiedermann, et al, Meta-analysis of pooled data from the three large trials.
40 Recommendation #3: Vasopressors We recommend that vasopressor therapy initially target a mean arterial pressure (MAP) of 65 mm Hg. (Grade 1C) We recommend norepinephrine as the first- choice vasopressor. (Grade 1B) We suggest epinephrine (added to and potentially substituted for norepinephrine) when an additional agent is needed to maintain adequate blood pressure. (Grade 2B)
41 Recommendation #3: Vasopressors Vasopressin up to 0.03 units/minute can be added to norepinephrine with the intent of raising MAP to target or decreasing norepinephrine dosage. Low-dose vasopressin is not recommended as the single initial vasopressor for treatment of sepsis-induced hypotension, and vasopressin doses higher than units/minute should be reserved for salvage therapy (failure to achieve adequate MAP with other vasopressor agents). We suggest dopamine as an alternative vasopressor agent to norepinephrine only in highly selected patients (eg, patients with low risk of arrhythmias and/or low heart rate). (Grade 2C)
. Meta-analysis performed by Djillali Annane for Surviving Sepsis Campaign, using following publications: Annane D et al. Lancet.")
42 The Evidence: NE vs Dopamine Meta-Analysis Information from 4 randomized trials (n=540) comparing norepinephrine to epinephrine found no evidence for differences in the risk of dying (RR=0.96; 0.77 to 1.21; fixed effect; I 2 =0%). Meta-analysis performed by Djillali Annane for Surviving Sepsis Campaign, using following publications: Annane D et al. Lancet. 2007;370:
 comparing norepinephrine to epinephrine found no evidence for differences in the risk of dying (RR=0.96; 0.")
43 The Evidence: NE vs. Epinephrine Information from 4 randomized trials (n=540) comparing norepinephrine to epinephrine found no evidence for differences in the risk of dying (RR=0.96; 0.77 to 1.21; fixed effect; I 2 =0%). Meta-analysis performed by Djillali Annane for Surviving Sepsis Campaign, using Annane D et al. Lancet. 2007;370:
44 Recommendation #5: Ionotropes We recommend that a trial of dobutamine infusion up to 20 μg/kg/min be administered or added to vasopressor (if in use) in the presence of: (Down-graded in response to PROCESS, ARISE and PROMISE trials) myocardial dysfunction as suggested by elevated cardiac filling pressures and low cardiac output, or ongoing signs of hypoperfusion, despite achieving adequate intravascular volume and adequate mean arterial pressure. (Grade 1C) We recommend against the use of a strategy to increase cardiac index to predetermined supranormal levels. (Grade 1B) The Schumaker paradigm previously shown to increase mortality!
45 Recommendation #6: Diagnostics We recommend obtaining appropriate cultures before antimicrobial therapy is initiated if such cultures do not cause significant delay (>45 minutes) in the start of antimicrobial(s) administration (Grade 1C). To optimize identification of causative organisms, we recommend obtaining at least two sets of blood cultures (both aerobic and anaerobic bottles) before antimicrobial therapy, with at least one drawn percutaneously and one drawn through each vascular access device, unless the device was recently (<48 hours) inserted. Blood cultures can be drawn at the same time if from a different anatomic site (Grade 1C).
46 Recommendation #6: Diagnostics Cultures of other sites (preferably quantitative where appropriate), such as urine, cerebrospinal fluid, wounds, respiratory secretions, or other body fluids that may be the source of infection, should also be obtained before antimicrobial therapy if doing so does not cause significant delay in antibiotic administration (Grade 1C). We recommend that imaging studies be performed promptly in attempts to confirm a potential source of infection. Potential sources of infection should be sampled as they are identified and in consideration of patient risk for transport and invasive procedures (eg, careful coordination and aggressive monitoring if the decision is made to transport for a CT-guided needle aspiration). Bedside studies, such as ultrasound, may avoid patient transport (Ungraded).
47 Recommendation #7: Antibiotics The administration of effective intravenous antimicrobials within the first hour of recognition of septic shock (Grade 1B) and severe sepsis without septic shock (Grade 1C) should be the goal of therapy. Disclaimer: Although the weight of the evidence supports prompt administration of antibiotics following the recognition of severe sepsis and septic shock, the feasibility with which clinicians may achieve this ideal state has not been scientifically evaluated.

48 Recommendation #7: Antibiotics Dellinger RP. Crit Care Med 2013;41:

49 Hospital Mortality by Time to Antibiotics
50 Recommendation #7: Antibiotics We recommend that initial empiric anti-infective therapy include one or more drugs that have activity against all likely pathogens (bacterial and/or fungal or viral) and that penetrate in adequate concentrations into the tissues presumed to be the source of sepsis (Grade 1B). The antimicrobial regimen should be reassessed daily for potential deescalation to prevent the development of resistance, to reduce toxicity, and to reduce costs (Grade 1B). Empiric therapy should attempt to provide antimicrobial activity against the most likely pathogens based upon each patient s presenting illness and local patterns of infection. We suggest combination empiric therapy for neutropenic patients with severe sepsis (Grade 2B) and for patients with difficult-to-treat, multidrug-resistant bacterial pathogens such as Acinetobacter and Pseudomonas spp. (Grade 2B).
51 Recommendation #8: Procalcitonin We suggest the use of low procalcitonin levels or similar biomarkers to assist the clinician in the discontinuation of empiric antibiotics in patients who appeared septic, but have no subsequent evidence of infection (Grade 2C). Procalcitonin levels are NOT recommended as a biomarker for the diagnosis of sepsis.
52 Recommendation #8: Procalcitonin Meta-Analysis Meta-analysis: 7 studies; 1075 pts with severe sepsis or septic shock No difference in hospital mortality and 28-day mortality Duration of antimicrobial therapy was significantly reduced in favor of procalcitonin-guided therapy (HR 1.27 [ ], p<0.05) Prkno et al, Critical Care 2013; 17: R291
53 Recommendation #9: Source Control We recommend that a specific anatomical diagnosis of infection requiring consideration for emergent source control (eg, necrotizing soft tissue infection, peritonitis, cholangitis, intestinal infarction) be sought and diagnosed or excluded as rapidly as possible, and intervention be undertaken for source control within the first 12 hours after the diagnosis is made, if feasible (Grade 1C). We suggest that when infected peripancreatic necrosis is identified as a potential source of infection, definitive intervention is best delayed until adequate demarcation of viable and nonviable tissues has occurred (Grade 2B). The two Danish trials.
54 Recommendation #9: Source Control When source control in a severely septic patient is required, the effective intervention associated with the least physiologic insult should be used (eg, percutaneous rather than surgical drainage of an abscess) (Ungraded). If intravascular access devices are a possible source of severe sepsis or septic shock, they should be removed promptly after other vascular access has been established (Ungraded).
55 Recommendation #10: Corticosteroids Corticosteroids only for vasopressor refractory shock Hydrocortisone 200 mg daily +/- fludrocortisone CORTICUS no difference in 28-day mortality Earlier reversal of shock with hydrocortisone Sprung et al. N Engl J Med. 2008;358: No adrenal axis testing recommended Taper steroids upon discontinuation of pressors Do NOT give steroids in the absense of shock
56 Recommendation #11: Blood Products PRBCs for Hg < 7 g/dl No FFP to correct INR unless procedures to be done No anti-thrombin III Platelets only if <10K, or <20K with significant risk of bleeding, or >50K for invasive procedures
57 Recommendation #12: Glucose Control We recommend protocolized approach to blood glucose management, commencing insulin dosing when two consecutive blood glucose levels are >180 mg/dl. This protocolized approach should target upper blood glucose <180 mg/dl rather than <110 mg/dl (Grade 1A). Great lesson in knowing patient population being studied and not making broad application! NICE-SUGAR Investigators. N Engl J Med. 2009;360: van den Berghe et al. N Engl J Med. 2001;345: Dellinger et al. Crit Care Med. 2013;41: Dellinger et al. Intensive Care Med. 2013;39:
58 Glycemic Control: The van den Berghe Studies at a glance
59 Excess mortality with intensive therapy due to cardiac death Glycemic Control: NICE SUGARS Mortality rates were 27.5% in the intensive-control group and 24.9% in the conventional-control group. Conventional <180 g/dl vs. Intensive g/dl
60 Recommendation #13: Bicarbonate We recommend against the use of sodium bicarbonate therapy for the purpose of improving hemodynamics or reducing vasopressor requirements in patients with hypoperfusion-induced lactic acidemia with ph 7.15 (Grade 2B). For me, I would choose to paralyze a patient with cisatracurium BEFORE using bicarbonate therapy to decrease CO2 production
61 Compliance with Guidelines - Outcomes Levy et al; Intensive Care Med (2014) 40:
62 Least invasive source control within 12 hours Conclusions: Keys to Management Early identification with high index of suspicion Aggressive fluid resuscitation EARLY Don t stop even after starting vasopressors if fluid responsive! Best standard resuscitation directed towards restoration of perfusion and lactate clearance is equivalent to EGDT Early, appropriate and broad antimicrobial therapy ONLY error is not to give them (assuming no allergies)
63 Conclusions: Keys to Management Use procalcitonin to guide de-escalation and NOT to diagnose severe sepsis/septic shock Low dose corticosteroids ONLY with vasopressor refractory shock Avoid intensive glycemic control; keep glucose <180 g/dl ARDS Net Ventilation
64 QUESTIONS?
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
 Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2012
 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2012 Definition Sepsis the presence of infection with
本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2012 Definition Sepsis the presence of infection with
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
EBM EGDT 每次都是RCT.有點煩 本來想簡單處理 那些年我們曾經打拼過的~~ By Maxy Lu 這次想要放鬆一下~~ EGDT (Early goal-directed therapy) Early go to ICU
 Early go to ICU") EBM 2014.03.24 By Maxy Lu 每次都是RCT.有點煩 這次想要放鬆一下~~ 本來想簡單處理 EGDT (Early goal-directed therapy) 那些年我們曾經打拼過的~~ EGDT Early go to ICU 想說這下開心了 Best practice Not Standard of care Screening and practice improvement
EBM 2014.03.24 By Maxy Lu 每次都是RCT.有點煩 這次想要放鬆一下~~ 本來想簡單處理 EGDT (Early goal-directed therapy) 那些年我們曾經打拼過的~~ EGDT Early go to ICU 想說這下開心了 Best practice Not Standard of care Screening and practice improvement
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of
 Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Sepsis Review. Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center
 Sepsis Review Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org Discuss the Updated International Guidelines Discuss how you
Sepsis Review Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org Discuss the Updated International Guidelines Discuss how you
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis and septic shock: can we win the battle against this hidden crisis?
 REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Why does it matter? Sepsis
 Sepsis 2015 Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University Providence, RI Sepsis Why does it matter?
Sepsis 2015 Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University Providence, RI Sepsis Why does it matter?
Chapter 5: Sepsis Stephen Lo
 Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
9/9/15. Sepsis Update: Early identification and management. Objectives. Incidence & Mortality. Blaizie Goveas, MS, APRN, AGACNP- BC
 Sepsis Update: Early identification and management Blaizie Goveas, MS, APRN, AGACNP- BC Objectives Understanding what is sepsis and the severity of the disease process. Epidemiology of sepsis Identifying
Sepsis Update: Early identification and management Blaizie Goveas, MS, APRN, AGACNP- BC Objectives Understanding what is sepsis and the severity of the disease process. Epidemiology of sepsis Identifying
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
SEPSIS MANAGEMENT. Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah
 Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah") SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center
 UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX
 Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
SEPSIS RAPID RESPONSE
 SEPSIS RAPID RESPONSE Sepsis kills up to 50% of those infected. How many deaths will you prevent this year? 1 SEPSIS Back ground: According to the Institute for Health Improvement and the Surviving Sepsis
SEPSIS RAPID RESPONSE Sepsis kills up to 50% of those infected. How many deaths will you prevent this year? 1 SEPSIS Back ground: According to the Institute for Health Improvement and the Surviving Sepsis
Practical. Septic shock resuscitation ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล
 Practical Septic shock resuscitation ไ ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล ประช มว ชาการ 101 ป อาย รศาสตร ศ ร ราช 6 ก มภาพ นธ 2561 Early recognition Early resuscitation Early
Practical Septic shock resuscitation ไ ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล ประช มว ชาการ 101 ป อาย รศาสตร ศ ร ราช 6 ก มภาพ นธ 2561 Early recognition Early resuscitation Early
4/4/2014. Of patients diagnosed with sepsis 50% will develop severe sepsis 25% will develop shock. SIRS Sepsis Severe Septic Sepsis Shock.
 A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Inflammation. Sepsis Ladder
 Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
 Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Billion
 Surviving : Are we? The 7th National Emergency Medicine Congress Antalya, Turkey Alexander L. Eastman, MD, MPH Department of Surgery UTSW Severe : A Significant Healthcare Challenge Major cause of morbidity
Surviving : Are we? The 7th National Emergency Medicine Congress Antalya, Turkey Alexander L. Eastman, MD, MPH Department of Surgery UTSW Severe : A Significant Healthcare Challenge Major cause of morbidity
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand