Bilateral rib fractures 2 on right and 1 on left In different stages of healing, with left fracture older than right fractures
|
|
|
- Emory Moore
- 5 years ago
- Views:
Transcription
1 More history: Seen by PCP yesterday because of vomiting and fussinesss. Called by ED today because Mom presents with same complaints. ED found nothing but got an abdominal x ray. ED now wants kid admitted for observation because kid seems really fussy and they can t find a reason. Bilateral rib fractures 2 on right and 1 on left In different stages of healing, with left fracture older than right fractures You suspect physical abuse 1

2 WHAT NOW? 2
3 GET A SKELETAL SURVEY 6 AP skull Right lateral skull Left lateral skull AP chest Right oblique ribs Left oblique ribs AP abdomen/pelvis AP right humerus Lateral right humerus AP left humerus Lateral left humerus AP right forearm Lateral right forearm AP left forearm Lateral left forearm PA right hand PA left hand AP right femur Lateral right femur AP left femur Lateral left femur AP right tibia/fibula Lateral right tibia AP left tibia/fibula Lateral left tibia/fibula AP right foot AP left foot Lateral C spine Lateral T L spine ACR Appropriateness Criteria Pediatric Topics Suspected physical abuse Urinary tract infection Vomiting in infants up to 3 months of age 3
4 What other imaging is needed? <24 months old, no neuro or visceral injuries suspected 9 Skeletal survey 6 MRI head without contrast 5 CT head without contrast 4 Whole body bone scan 2 MRI head with(out) contrast 1 CT head with contrast 1 CT head with(out) contrast >24 months old, no neuro or visceral injuries suspected 9 X ray area of interest 6 CT head without contrast 5 Skeletal survey 5 MRI head without contrast 4 Whole body bone scan 2 MRI head with(out) contrast 1 CT head with contrast 1 CT head with(out) contrast Adapted from Reference 6 What about the child with more complex injuries, with one or more of the following? Neurologic signs or symptoms Apnea Complex skull fracture Other fractures Injuries highly suspicious of child abuse NO SUSPECTED VISCERAL INJURIES 9 X ray skeletal survey 9 CT head without contrast 8 MRI head without contrast 8 MRI cervical spine without contrast 5 MRI complete spine without contrast 5 Whole body bone scan 3 MRI head with(out) contrast 2 MRI cervical spine with(out) contrast 2 MRI complete spine with(out) contrast 1 CT head with contrast 1 CT head with(out) contrast Adapted from Reference 6 4
5 What if child has suspected injury in thorax, abdomen or pelvis? Abdominal skin bruising Abdominal distention Abdominal tenderness Elevated liver or pancreatic enzymes 9 X ray skeletal survey 9 CT abdomen/pelvis with IV contrast 6 CT chest with contrast 6 CT head without contrast 6 MRI head without contrast 4 Whole body bone scan 3 CT chest without contrast 2 MRI head with(out) contrast 2 CT abdomen/pelvis without contrast 1 CT head with contrast 1 CT head with(out) contrast Adapted from Reference 6 Cases of abuse may not be straightforward ACR Appropriateness Criteria are very helpful in determining what studies are needed Don t forget to consult with your friendly neighborhood pediatric radiologist If possible, consult with a child abuse pediatrician 5
:67 74.")
6 Nonaccidental Trauma (NAT) 1 in 10 ALTE/BRUE If you don t suspect it, you will miss it TEN 4 Bruising of torso, ears, or neck in kids under 4 y.o. Any bruising under 4 m.o. Pierce MC, Kaczor K, Aldridge S, O'Flynn J, Lorenz DJ. Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics. 2010;125(1): Know how to refer a kid to CPS before you have to NAT: X Rays Look carefully at entire x ray If there is a rib fracture/suspicion of rib fracture within lower chest on an abdominal x ray, at a minimum, you will need chest, 2 views also bilateral oblique views of ribs 6

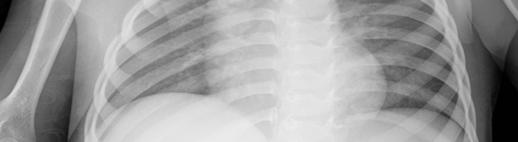
7 NONACCIDENTAL TRAUMA Rib fractures are common Can be difficult to see on x rays unless callus has formed 11 WEEK OLD MALE Posterior rib fractures, near costovertebral junction, are especially characteristic 7
8 NONACCIDENTAL TRAUMA Rib Fractures Fractures can occur anywhere on rib arc, from costochondral junction to costovertebral articulation NONACCIDENTAL TRAUMA Rib fractures are unusual unless child has experienced major thoracic trauma Typically due to AP thoracic compression 8
9 NONACCIDENTAL TRAUMA Rib Fractures May be single, multiple, unilateral, or bilateral Should raise suspicion of NAT NONACCIDENTAL TRAUMA Coexistence of two or more fractures: Moderately specific sign of NAT, especially if remote from each other and particularly if in different phases of healing 9
10 Skeletal Survey/Pediatric Trauma Survey 29 images! Do we need all 29 images? Typically, yes, unless very recent (within last day or two) image(s) of good quality Entire/Most of Extremity on 1 Image? Is it okay to try to get an entire extremity on one image? Usually not, depends on the patient May not be able to detect a very subtle acute or healing fracture 10
11 Often important DATING of FRACTURES Often discussed Often unsatisfying DATING FRACTURES* Timetable of Radiologic Changes in Children s Fractures** CATEGORY EARLY PEAK LATE 1. SPNBF 6 10 days days days 2. Loss of fracture line definition days days 3. Soft callus 9 15 days days 4. Hard callus days days days *Kleinman, P.K., ed. Diagnostic Imaging of Child Abuse, 3 rd edition. Cambridge University, Cambridge, UK, **Repetitive injuries may prolong all categories 11


12 3 ½ month old 12


13 13




14 14




15 15





16 What if subperiosteal new bone formation (SPNBF) is not symmetric, or is >2mm in thickness? Healing injury! Pediatric Trauma Survey 26 month old male 16








17 17





18 18





19 19







20 20








21 21

22 WHAT HAVE YOU SEEN? Burns 22
23 Frequency of Skeletal Injuries in Children with Inflicted Burns Kimberly E Fagen, Eglal Shalaby Rana, Allison M. Jackson Pediatric Radiology (2015) 45: nearly one third of those children with inflicted burns had associated skeletal injuries, most commonly healing rib fractures. Thus young children with concern for nonaccidental burns should undergo a skeletal survey. 23


24 So when there is concern for NAT, you need to consider getting a skeletal survey 24
25 What did you see? 25

26 Now what? Repeat after days! 26


27 27

28 What do you see? 1 st study 2 nd study, 16 days later 28

29 Follow up Skeletal Survey Ribs looked normal on 1 st Skeletal Survey no evidence of fracture then Obvious healing rib fractures on follow up skeletal survey When there is concern for NAT, follow up Skeletal Survey is mandatory 7 Month old Ex Premie Shortness of Breath 29
30 What do you see? 30

31 Bilateral healing rib fractures! 4 month old, transferred from OSH with ALTE 31



32 4 month old 4 month old, 3 days later, WOB 32


33 Later on same day What do you see? 33


34 34


35 Healing left rib fractures, consistent with NAT Next Patient He seems different 35
6/23/2017. What do you see? skull fracture
 What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
CHILD MALTREATMENT- GUIDELINES FOR SUSPICION and INITIAL MEDICAL EVALUATION DRAFT May Leslie M. Quinn M.D.
 CHILD MALTREATMENT- GUIDELINES FOR SUSPICION and INITIAL MEDICAL EVALUATION DRAFT May 2012 - Leslie M. Quinn M.D. PHYSICAL ABUSE: For any child presenting with signs and or symptoms of an injury consider
CHILD MALTREATMENT- GUIDELINES FOR SUSPICION and INITIAL MEDICAL EVALUATION DRAFT May 2012 - Leslie M. Quinn M.D. PHYSICAL ABUSE: For any child presenting with signs and or symptoms of an injury consider
Evaluation of a Pediatric Patient
 September 2005 Evaluation of a Pediatric Patient Percy Ballard, Harvard Medical School Year III Our Little Man: 6mo old male transferred to Children s from hospital in the Philippines 3mo history of meningitis,
September 2005 Evaluation of a Pediatric Patient Percy Ballard, Harvard Medical School Year III Our Little Man: 6mo old male transferred to Children s from hospital in the Philippines 3mo history of meningitis,
Suspected Physical Abuse Clinical Practice Guideline
 Suspected Physical Abuse Clinical Practice Guideline WHEN TO CONSIDER ABUSE Consider abuse on the differential Injuries to multiple organ systems Injuries in different stages of healing Patterned injuries
Suspected Physical Abuse Clinical Practice Guideline WHEN TO CONSIDER ABUSE Consider abuse on the differential Injuries to multiple organ systems Injuries in different stages of healing Patterned injuries
Radiological investigations
 Nita Jain, MD, FRCPC The role of diagnostic imaging in the evaluation of child abuse Radiologists experienced in pediatric imaging can provide invaluable assistance to health care teams working to identify
Nita Jain, MD, FRCPC The role of diagnostic imaging in the evaluation of child abuse Radiologists experienced in pediatric imaging can provide invaluable assistance to health care teams working to identify
Institution INSTRUCTIONS (I6) 1. This form is to be completed by a DESIGNATED STUDY NUCLEAR MEDICINE SPECIALIST
 1. This form is to be completed by a DESIGNATED STUDY NUCLEAR MEDICINE SPECIALIST") I6 ACRIN 6660 Whole Body MRI in the Evaluation of Pediatric Malignancies Conventional Scintigraphy Imaging Form If this is a revised or corrected form, indicate by checking box and fax to 215-717 - 0936.
I6 ACRIN 6660 Whole Body MRI in the Evaluation of Pediatric Malignancies Conventional Scintigraphy Imaging Form If this is a revised or corrected form, indicate by checking box and fax to 215-717 - 0936.
Disclosure. Physical Abuse. Objectives. What is the Mechanism of the Injury?
 Disclosure Abuse or Not Abuse: What is the Answer? Natalie Kissoon, MD Assistant Professor Division of Child Abuse Pediatrics University of Texas Health Science Natalie Kissoon, MD has no relationships
Disclosure Abuse or Not Abuse: What is the Answer? Natalie Kissoon, MD Assistant Professor Division of Child Abuse Pediatrics University of Texas Health Science Natalie Kissoon, MD has no relationships
Institution INSTRUCTIONS (M3) - All other imaging studies, including CT, CONVENTIONAL MRI, PET SCINTIGRAPHY, etc... AND
 - All other imaging studies, including CT, CONVENTIONAL MRI, PET SCINTIGRAPHY, etc... AND") M3 ACRIN 6660 Whole Body MRI in the Evaluation of Pediatric Malignancies Whole Body MRI Imaging Form No. Revised/corrected form, check box and fax to 215-717-0936 INSTRUCTIONS (M3) 1. This form is to be
M3 ACRIN 6660 Whole Body MRI in the Evaluation of Pediatric Malignancies Whole Body MRI Imaging Form No. Revised/corrected form, check box and fax to 215-717-0936 INSTRUCTIONS (M3) 1. This form is to be
CPT CODES. Ph: (307) Fax: (307) CATSCAN IV Contrast: 87.00
 Fax: (307) CATSCAN IV Contrast: 87.00") Ph: (307) 382-4282 Fax: (307) 382-4291 CPT CODES CATSCAN IV Contrast: 87.00 74150 Abdomen w/o contrast $ 809.00 74160 Abdomen w/ contrast $1175.00 w/ contrast: $1262.00 74170 Abdomen w_w/o contrast $1324.00
Ph: (307) 382-4282 Fax: (307) 382-4291 CPT CODES CATSCAN IV Contrast: 87.00 74150 Abdomen w/o contrast $ 809.00 74160 Abdomen w/ contrast $1175.00 w/ contrast: $1262.00 74170 Abdomen w_w/o contrast $1324.00
Evidence Base for Child Abuse Fractures
 Evidence Base for Child Abuse Fractures SPR Sunrise Session May 17, 2018 Megan B. Marine, MD, FAAP Assistant Professor of Clinical Radiology, Pediatric Division Co-Director, Pediatric Radiology Fellowship
Evidence Base for Child Abuse Fractures SPR Sunrise Session May 17, 2018 Megan B. Marine, MD, FAAP Assistant Professor of Clinical Radiology, Pediatric Division Co-Director, Pediatric Radiology Fellowship
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
10/8/17. I have no disclosures. What are they? Upper extremity fractures Lower extremity fractures Non accidental trauma
 I have no disclosures Upper extremity fractures Lower extremity fractures Non accidental trauma What are they? Fractures of the radius, ulna and/or humerus Who gets them? Active children usually after
I have no disclosures Upper extremity fractures Lower extremity fractures Non accidental trauma What are they? Fractures of the radius, ulna and/or humerus Who gets them? Active children usually after
Subtle Signs of Child Abuse Child s Protection Office MOH Presented by Dr.Fatoumah Alabdulrazzaq M.D,FRCPC,FAAP,PEM(C)
") Subtle Signs of Child Abuse Child s Protection Office MOH Presented by Dr.Fatoumah Alabdulrazzaq M.D,FRCPC,FAAP,PEM(C) Cutaneous Injuries Bruise : injury to soft tissues in which skin is not broken, characterized
Subtle Signs of Child Abuse Child s Protection Office MOH Presented by Dr.Fatoumah Alabdulrazzaq M.D,FRCPC,FAAP,PEM(C) Cutaneous Injuries Bruise : injury to soft tissues in which skin is not broken, characterized
OVERVIEW OF CHILD PHYSICAL ABUSE
 2011 MFMER slide-1 OVERVIEW OF CHILD PHYSICAL ABUSE Mark S. Mannenbach, MD Mayo Medical Center Rochester, MN 2011 MFMER slide-2 Objectives At the conclusion of this session, the participant will be able
2011 MFMER slide-1 OVERVIEW OF CHILD PHYSICAL ABUSE Mark S. Mannenbach, MD Mayo Medical Center Rochester, MN 2011 MFMER slide-2 Objectives At the conclusion of this session, the participant will be able
revised originals as separate pages on I://DX(all folders)/trauma X Manual and project
/trauma X Manual and project") 06-25-14 revised originals as separate pages on I://DX(all folders)/trauma X Manual and project Procedure for Suspected Child Abuse Imaging Trauma X GUIDELINES: Every effort should be made to request studies
06-25-14 revised originals as separate pages on I://DX(all folders)/trauma X Manual and project Procedure for Suspected Child Abuse Imaging Trauma X GUIDELINES: Every effort should be made to request studies
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Common Abusive Skeletal Injuries
 Common Abusive Skeletal Injuries Paul Kleinman, M.D. Children s Hospital Harvard Medical School Boston, Ma. Rib fractures, especially posteromedial Rib fractures, especially posteromedial Kemp AM et. Al.
Common Abusive Skeletal Injuries Paul Kleinman, M.D. Children s Hospital Harvard Medical School Boston, Ma. Rib fractures, especially posteromedial Rib fractures, especially posteromedial Kemp AM et. Al.
Overview of Abusive Head Trauma: What Everyone Needs to Know. 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012
 Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
RADIOLOGY REQUEST MANUAL. (615)
") RADIOLOGY REQUEST MANUAL www.vanderbiltchildrens.com RADIOLOGY REQUEST MANUAL EXAM PROTOCOL QUESTIONS? Please call: DIAGNOSTIC RADIOLOGY (X-RAY) Pager (615) 835-1714 CT (615) 936-4920 MRI (615) 936-4933
RADIOLOGY REQUEST MANUAL www.vanderbiltchildrens.com RADIOLOGY REQUEST MANUAL EXAM PROTOCOL QUESTIONS? Please call: DIAGNOSTIC RADIOLOGY (X-RAY) Pager (615) 835-1714 CT (615) 936-4920 MRI (615) 936-4933
CORE-INFO: fractures in children
 CORE-INFO: fractures in children This leaflet summarises what is currently known about the relationship between fractures and physical abuse and will be of particular interest to paediatricians, general
CORE-INFO: fractures in children This leaflet summarises what is currently known about the relationship between fractures and physical abuse and will be of particular interest to paediatricians, general
Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C.
 Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Routine Guide EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION. 14x17 CW* 14x17LW 14x17LW. 14x17LW 14x17LW 14x17LW
 EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION A-C Joints without weights with weights 14x17 CW* One 14x17 divided; both shoulders on one exposure. *If part does not fit, do 10x12s CW. Both
EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION A-C Joints without weights with weights 14x17 CW* One 14x17 divided; both shoulders on one exposure. *If part does not fit, do 10x12s CW. Both
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of multimodality supervised
Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of multimodality supervised
Trauma Center Practice Management Guideline Blank Children s Hospital (BCH) Des Moines
 Des Moines") Trauma Center Practice Management Guideline Blank Children s Hospital (BCH) Des Moines Non-Accidental Trauma (NAT) PEDIATRIC Practice Management Guideline Contact: Trauma Center Medical Director/ Trauma
Trauma Center Practice Management Guideline Blank Children s Hospital (BCH) Des Moines Non-Accidental Trauma (NAT) PEDIATRIC Practice Management Guideline Contact: Trauma Center Medical Director/ Trauma
Radiologic Assessment of Child Abuse in Infants: A Focus on Plain Film Analysis of Highly Specific Fractures
 July 2006 Radiologic Assessment of Child Abuse in Infants: A Focus on Plain Film Analysis of Highly Specific Fractures Denise De Las Nueces, Harvard Medical School Year IV General Overview Introduction
July 2006 Radiologic Assessment of Child Abuse in Infants: A Focus on Plain Film Analysis of Highly Specific Fractures Denise De Las Nueces, Harvard Medical School Year IV General Overview Introduction
The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast
 The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast September 27, 2018 Introduction: Hello everyone, my name is Dominique Piché
The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast September 27, 2018 Introduction: Hello everyone, my name is Dominique Piché
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Stair falls: caregiver s missed step as a source of childhood fractures
 J Child Orthop (2014) 8:77 81 DOI 10.1007/s11832-014-0551-x ORIGINAL CLINICAL ARTICLE Stair falls: caregiver s missed step as a source of childhood fractures Andrew T. Pennock George D. Gantsoudes Jennifer
J Child Orthop (2014) 8:77 81 DOI 10.1007/s11832-014-0551-x ORIGINAL CLINICAL ARTICLE Stair falls: caregiver s missed step as a source of childhood fractures Andrew T. Pennock George D. Gantsoudes Jennifer
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains
 5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains Kristen Reeder, MD Child Abuse Pediatrician, REACH Program Children s Health SM Children s Medical Center Dallas Assistant Professor
5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains Kristen Reeder, MD Child Abuse Pediatrician, REACH Program Children s Health SM Children s Medical Center Dallas Assistant Professor
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics
 Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics Disclosure I have nothing to disclose Objectives Describe common accidental injuries which can be confused with child abuse Describe
Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics Disclosure I have nothing to disclose Objectives Describe common accidental injuries which can be confused with child abuse Describe
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
NEUROSURGEON VS. HOSPITALIST Pediatric Hospital Medicine meeting Nashville, TN July 21, 2017*±
 NEUROSURGEON VS. HOSPITALIST Pediatric Hospital Medicine meeting Nashville, TN July 21, 2017*± *no pediatricians were harmed in the making of this presentation ±nonetheless, please do not try this at home
NEUROSURGEON VS. HOSPITALIST Pediatric Hospital Medicine meeting Nashville, TN July 21, 2017*± *no pediatricians were harmed in the making of this presentation ±nonetheless, please do not try this at home
Diagnostic Imaging Exams
 Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
What Not to Miss: Five Years' of Resident Discrepancies on Pediatric ED Exams. Project Overview
 What Not to Miss: Five Years' of Resident Discrepancies on Pediatric ED Exams Michael Baad MD, David Kromrey MD, Seng Ong MD, Mario Zaritzky MD, Kate A. Feinstein MD Project Overview Problem Residents
What Not to Miss: Five Years' of Resident Discrepancies on Pediatric ED Exams Michael Baad MD, David Kromrey MD, Seng Ong MD, Mario Zaritzky MD, Kate A. Feinstein MD Project Overview Problem Residents
COMPETENCY REQUIREMENTS for the CERTIFICATION EXAMINATION
 COMPETENCY REQUIREMENTS for the 10/2013 CERTIFICATION BOARD FOR RADIOLOGY PRACTITIONER ASSISTANTS CERTIFICATION EXAMINATION Note: The competency requirements contained in this document will be in effect
COMPETENCY REQUIREMENTS for the 10/2013 CERTIFICATION BOARD FOR RADIOLOGY PRACTITIONER ASSISTANTS CERTIFICATION EXAMINATION Note: The competency requirements contained in this document will be in effect
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
2/13/13. Ann S. Botash, MD SUNY Upstate Medical University
 Ann S. Botash, MD SUNY Upstate Medical University 3 month old, previously healthy infant, brought to the primary care physician due to a fall He was being carried by the father, who tripped over the family
Ann S. Botash, MD SUNY Upstate Medical University 3 month old, previously healthy infant, brought to the primary care physician due to a fall He was being carried by the father, who tripped over the family
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Radiography. 1. Introduction. 2. Documentation of Compliance. 3. Didactic Competency Requirements. 4. Clinical Competency Requirements
 PRIMARY CERTIFICATION AND REGISTRATION Radiography 1. Introduction Candidates for certification and registration are required to meet the Professional Education Requirements specified in the ARRT Rules
PRIMARY CERTIFICATION AND REGISTRATION Radiography 1. Introduction Candidates for certification and registration are required to meet the Professional Education Requirements specified in the ARRT Rules
Medica Health Plans. Minnesota Fee Schedule Revised 5/1/2016 NEW PATIENT EXAMS: MN Medicaid. Medicare
 Medica Health Plans Minnesota Fee Schedule Revised 5/1/2016 NEW PATIENT EXAMS: 99201 Problem focused history and examination --straightforward $23.48 100% of CMS $29.53 99201.25 Problem focused history
Medica Health Plans Minnesota Fee Schedule Revised 5/1/2016 NEW PATIENT EXAMS: 99201 Problem focused history and examination --straightforward $23.48 100% of CMS $29.53 99201.25 Problem focused history
W/ (2) (3) (4) (5) (5) (6) (6) CTA
 (3) (4) (5) (5) (6) (6) CTA") Index Abdomen W/ and W/Out (2) Abdomen Pelvis W/Out (3) Abdomen Pelvis W/ (4) Pelvis W/ (5) Chest W/Out (5) Chest/Abdomen/Pelvis W/ (6) Chest W/ (6) CTA ( 7-8) Neuro (8-9) Musculoskeletal (10) Trauma (11)
Index Abdomen W/ and W/Out (2) Abdomen Pelvis W/Out (3) Abdomen Pelvis W/ (4) Pelvis W/ (5) Chest W/Out (5) Chest/Abdomen/Pelvis W/ (6) Chest W/ (6) CTA ( 7-8) Neuro (8-9) Musculoskeletal (10) Trauma (11)
AIM 2014 CPT Radiology & Cardiac Codes Requiring Review
 AIM 2014 CPT Radiology & Cardiac Codes Requiring Review Modality Body Part CT Head 1 70480 CT orbit, sella or posterior fossa; w/o contrast 1 CT Head 1 70481 CT orbit, sella or posterior fossa; with CT
AIM 2014 CPT Radiology & Cardiac Codes Requiring Review Modality Body Part CT Head 1 70480 CT orbit, sella or posterior fossa; w/o contrast 1 CT Head 1 70481 CT orbit, sella or posterior fossa; with CT
MRI Non-Joint Extremity Questionnaire
 MRI n-joint Extremity Questionnaire INSTRUCTIONS FOR COMPLETING QUESTIONNAIRE: Answer all of the initial questions (Pages 1 and 2) Select the reason for imaging by answering question #6. Based on your
MRI n-joint Extremity Questionnaire INSTRUCTIONS FOR COMPLETING QUESTIONNAIRE: Answer all of the initial questions (Pages 1 and 2) Select the reason for imaging by answering question #6. Based on your
2012 CPT Radiology Codes Requiring Review Blue Cross and Blue Shield of Louisiana
 2012 CPT Radiology Codes Requiring Review Blue Cross and Blue Shield of Louisiana CT Head 70480 CT orbit, sella or posterior fossa; w/o CT Head 70481 CT orbit, sella or posterior fossa; with CT Head 70482
2012 CPT Radiology Codes Requiring Review Blue Cross and Blue Shield of Louisiana CT Head 70480 CT orbit, sella or posterior fossa; w/o CT Head 70481 CT orbit, sella or posterior fossa; with CT Head 70482
Pain Management. Medicine. without limits
 Pain Management Medicine without limits Minimally invasive therapies for chronic pain relief Thanks to advances in medicine, you don t have to live with the debilitating effects of chronic pain. The physicians
Pain Management Medicine without limits Minimally invasive therapies for chronic pain relief Thanks to advances in medicine, you don t have to live with the debilitating effects of chronic pain. The physicians
Pediatric Imaging Spine MRI and Spine CT Test Request Tip Sheet
 Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of ongoing back pain, six weeks of conservative
Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of ongoing back pain, six weeks of conservative
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
Pediatric Imaging Spine MRI and Spine CT Test Request Tip Sheet
 Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of
Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of
Contributors. Thanks to Peter Miller, MD; LCDR Kevin Preston, MD; and Keith Newbrough, MD for their generous contribution of images:
 Contributors Thanks to Peter Miller, MD; LCDR Kevin Preston, MD; and Keith Newbrough, MD for their generous contribution of images: Peter Miller, MD, Indiana University School of Medicine Chapter 1: Figure
Contributors Thanks to Peter Miller, MD; LCDR Kevin Preston, MD; and Keith Newbrough, MD for their generous contribution of images: Peter Miller, MD, Indiana University School of Medicine Chapter 1: Figure
RADIAL HEAD FRACTURES. It is far more common in adults than in children, (who more commonly fracture their neck of radius).
.") RADIAL HEAD FRACTURES Introduction Fractures of the head of the radius are relatively common. The injury can be subtle unless specifically looked for. It is far more common in adults than in children,
RADIAL HEAD FRACTURES Introduction Fractures of the head of the radius are relatively common. The injury can be subtle unless specifically looked for. It is far more common in adults than in children,
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
A N.S. Technologists Experiences
 A N.S. Technologists Experiences I have nothing to disclose What does appropriate imaging mean For radiologists? For technologists? How does this affect patients and technologists? Discuss ordering trends
A N.S. Technologists Experiences I have nothing to disclose What does appropriate imaging mean For radiologists? For technologists? How does this affect patients and technologists? Discuss ordering trends
screening; including image post processing CT, heart; without contrast material; with Requires authorization
 0042T Cerebral perfusion analysis using CT; with ; including of parametric maps with determination of cerebral blood flow, cerebral blood volume, and mean transit time 74263 Computed tomographic (CT) colonography,
0042T Cerebral perfusion analysis using CT; with ; including of parametric maps with determination of cerebral blood flow, cerebral blood volume, and mean transit time 74263 Computed tomographic (CT) colonography,
Pediatric Abusive Head Trauma
 Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Pediatric CT Protocols (18 years old or less)
") Pediatric CT Protocols (18 years old or less) Ped1: Head CT Ped2: Cervical spine CT Ped3: Sinus CT Ped4: Neck CT Ped5: Chest CT Ped6: Abdomen and pelvis CT Ped7: Thoracic or lumbar spine CT Ped8: Extremity
Pediatric CT Protocols (18 years old or less) Ped1: Head CT Ped2: Cervical spine CT Ped3: Sinus CT Ped4: Neck CT Ped5: Chest CT Ped6: Abdomen and pelvis CT Ped7: Thoracic or lumbar spine CT Ped8: Extremity
They re not little adults, but they are little humans. Pearls for your next pediatric trauma patient. Children are little humans
 They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
We Accept Care Credit
 We Accept Care Credit Standard Fee Schedule Valid 1-Jan-18 to 1-July-18 **Prices Subject to Change, Call 702-222-3544 For Verification** Exam CPT PAYMENT IN FULL AT TIME OF SERVICE EKG 93000 35 TREADMILL
We Accept Care Credit Standard Fee Schedule Valid 1-Jan-18 to 1-July-18 **Prices Subject to Change, Call 702-222-3544 For Verification** Exam CPT PAYMENT IN FULL AT TIME OF SERVICE EKG 93000 35 TREADMILL
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Practice Changes I Hope You Make
 Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
PREAMBLE GENERAL DIAGNOSTIC RADIOLOGY
 PREAMBLE The General Diagnostic Radiology category is intended to cover the body of knowledge a practicing board certified Diagnostic Radiologist should know. Since the range of content relevant to the
PREAMBLE The General Diagnostic Radiology category is intended to cover the body of knowledge a practicing board certified Diagnostic Radiologist should know. Since the range of content relevant to the
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Bones of Thorax (Rib Cage)
") Musculoskeletal System (Part A-2) Module 7 -Chapter 10 Overview Muscles Attachments Bones Bone types Surface features of bones Divisions of the skeletal system Joints or Articulations Susie Turner, M.D.
Musculoskeletal System (Part A-2) Module 7 -Chapter 10 Overview Muscles Attachments Bones Bone types Surface features of bones Divisions of the skeletal system Joints or Articulations Susie Turner, M.D.
The scapula is located on the back side of the ribcage and helps provide part of the shoulder joint and movement for the arms.
 The scapula is located on the back side of the ribcage and helps provide part of the shoulder joint and movement for the arms. Scapula Humerus (Upper Arm Bone) Radius and Ulna Radius on Top Ulna on Bottom
The scapula is located on the back side of the ribcage and helps provide part of the shoulder joint and movement for the arms. Scapula Humerus (Upper Arm Bone) Radius and Ulna Radius on Top Ulna on Bottom
12/13/16. Jamie Hoffman-Rosenfeld, MD Medical Director, Queens CAC December 14, 2016
 Jamie Hoffman-Rosenfeld, MD Medical Director, Queens CAC December 14, 2016 Jamie Hoffman-Rosenfeld, MD, has no financial relationships with any commercial interests. The learner will be able to:! Articulate
Jamie Hoffman-Rosenfeld, MD Medical Director, Queens CAC December 14, 2016 Jamie Hoffman-Rosenfeld, MD, has no financial relationships with any commercial interests. The learner will be able to:! Articulate
Abuse Or Not? Interactive Visual Clues in Child Abuse
 Abuse Or Not? Interactive Visual Clues in Child Abuse Amy Baxter MD FAAP FACEP Associate Clinical Professor Medical College of Georgia 4 month old sleepy vomiting Mom works nights Wouldn t feed well Shivering
Abuse Or Not? Interactive Visual Clues in Child Abuse Amy Baxter MD FAAP FACEP Associate Clinical Professor Medical College of Georgia 4 month old sleepy vomiting Mom works nights Wouldn t feed well Shivering
28/04/2016. I have nothing to declare and no financial. interest or relationship to disclose
 I have nothing to declare and no financial interest or relationship to disclose Skeletal Anomalies are diverse range of complexities which is NOT Easy to diagnose. It is NOT Difficult to detect-just be
I have nothing to declare and no financial interest or relationship to disclose Skeletal Anomalies are diverse range of complexities which is NOT Easy to diagnose. It is NOT Difficult to detect-just be
Case Studies: Low Back Pain in the Athlete. Jim Messerly DO
 Case Studies: Low Back Pain in the Athlete Jim Messerly DO Nothing to disclose Case #1 History 15 y/o male presents for evaluation of his low back pain. His pain has been present for several months. The
Case Studies: Low Back Pain in the Athlete Jim Messerly DO Nothing to disclose Case #1 History 15 y/o male presents for evaluation of his low back pain. His pain has been present for several months. The
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
Radiological / Imaging Services Fee Schedule Provider Specialty 093
 CODE MOD Description 70250 TC RADIOLOGIC EXAM SKULL $18.30 $18.30 7/1/2012 71010 TC RADIOLOGIC EXAM, CHEST $11.41 $11.41 7/1/2012 71020 TC RADILOGICAL EXAM CHEST TWO VIEWS FRONTAL/LATERAL $15.76 $15.76
CODE MOD Description 70250 TC RADIOLOGIC EXAM SKULL $18.30 $18.30 7/1/2012 71010 TC RADIOLOGIC EXAM, CHEST $11.41 $11.41 7/1/2012 71020 TC RADILOGICAL EXAM CHEST TWO VIEWS FRONTAL/LATERAL $15.76 $15.76
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions
 83 Questions") Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Name Date Score. Skeletal System. Indicate if the following statements are true or false. Correct false statements
 Name Date Score Skeletal System True/False Indicate if the following statements are true or false. Correct false statements 1. Bones surround vital organs to protect them. 2. Bones store most of the calcium
Name Date Score Skeletal System True/False Indicate if the following statements are true or false. Correct false statements 1. Bones surround vital organs to protect them. 2. Bones store most of the calcium
Paediatric Trauma. A/Prof Drew Richardson. The Canberra Hospital May MB BS (Hons) FACEM Grad CertHE MD
 FACEM Grad CertHE MD") Paediatric Trauma A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Identify unique anatomic and physiologic characteristics of injured children Describe
Paediatric Trauma A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Identify unique anatomic and physiologic characteristics of injured children Describe
Radiography Protocols
 Radiography Protocols Upper Limb Second through Fifth Digits (Standard 3 views) First Digit (Thumb) (Standard 3 views) Hand (Standard 3 views) Wrist (Standard 4 views) Forearm (Standard 2 views) Elbow
Radiography Protocols Upper Limb Second through Fifth Digits (Standard 3 views) First Digit (Thumb) (Standard 3 views) Hand (Standard 3 views) Wrist (Standard 4 views) Forearm (Standard 2 views) Elbow
Upper Cervical Spine - Occult Injury and Trigger for CT Exam
 Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
MANAGEMENT OF FRACTURE. Sudi maiteh (seminar 2 )
") MANAGEMENT OF FRACTURE Sudi maiteh (seminar 2 ) Management of fracture Subjects : _ general management of fractures & Orthopedic patient evaluation _ Closed and open fractures management (Conservative,
MANAGEMENT OF FRACTURE Sudi maiteh (seminar 2 ) Management of fracture Subjects : _ general management of fractures & Orthopedic patient evaluation _ Closed and open fractures management (Conservative,
The Skeletal System. Support Systems Unit 2
 The Skeletal System Support Systems Unit 2 The Basic Functions of the Skeletal System Hematopoiesis Structure Support Muscle Attachment and Movement Mineral Storage Axial vs. Appendicular The Axial Skeleton
The Skeletal System Support Systems Unit 2 The Basic Functions of the Skeletal System Hematopoiesis Structure Support Muscle Attachment and Movement Mineral Storage Axial vs. Appendicular The Axial Skeleton
RADIOLOGY (Management)
") ULTRASOUND BETA SCAN/ U/S ORBITAL 1600 Daily U/S WHOLE ABDOMEN (Abd + Pelvis) 1200 Daily U/S PELVIS 1200 Daily U/S ABDOMEN 1200 Daily U/S BREAST 1800 Daily U/S FOLLICULAR STUDY 3000 Daily U/S FOLLICULAR
ULTRASOUND BETA SCAN/ U/S ORBITAL 1600 Daily U/S WHOLE ABDOMEN (Abd + Pelvis) 1200 Daily U/S PELVIS 1200 Daily U/S ABDOMEN 1200 Daily U/S BREAST 1800 Daily U/S FOLLICULAR STUDY 3000 Daily U/S FOLLICULAR
Managing Patient Dose in Computed Tomography (CT) INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION
 INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION") Managing Patient Dose in Computed Tomography (CT) International Commission on Radiological Protection Information abstracted from ICRP Publication 87 Available at www.icrp.org Task Group: M.M. Rehani,
Managing Patient Dose in Computed Tomography (CT) International Commission on Radiological Protection Information abstracted from ICRP Publication 87 Available at www.icrp.org Task Group: M.M. Rehani,
Managed Physical Network, Inc.
 MPN DC FEE SCHEDULE EVALUATION AND MANAGEMENT 99201 New Patient Exam; Problem Focused $50.00 99202 New Patient Exam; Expanded $50.00 99203 New Patient Exam; Detailed $50.00 99204 New Patient Exam; Comprehensive
MPN DC FEE SCHEDULE EVALUATION AND MANAGEMENT 99201 New Patient Exam; Problem Focused $50.00 99202 New Patient Exam; Expanded $50.00 99203 New Patient Exam; Detailed $50.00 99204 New Patient Exam; Comprehensive
Special Instructions
 FDA and ACR guidelines are as follows: Special Instructions Safety concerning NSF and gadolinium-based contrast agents (GBCA) Prior to administering MRI contrast (GBCA), any patient who answers yes to
FDA and ACR guidelines are as follows: Special Instructions Safety concerning NSF and gadolinium-based contrast agents (GBCA) Prior to administering MRI contrast (GBCA), any patient who answers yes to
Indications for cervical spine immobilisation: -
 Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Journal reading. Introduction. Introduction. Ottawa Ankle Rules. Method
 Journal reading Presenter: PGY 林聖傑 Supervisor: Dr. 林俊龍 102.12.23 The accuracy of ultrasound evaluation in foot and ankle trauma Salih Ekinci, MD American Journal of Emergency Medicine 31 (2013) 1551 1555
Journal reading Presenter: PGY 林聖傑 Supervisor: Dr. 林俊龍 102.12.23 The accuracy of ultrasound evaluation in foot and ankle trauma Salih Ekinci, MD American Journal of Emergency Medicine 31 (2013) 1551 1555
FOLLICULAR / OVULATION STUDY USG HIP JOINT (LEFT) USG HIP JOINT (RIGHT) USG KNEE JOINT (LEFT) USG KNEE JOINT (RIGHT) USG KUB USG MUSKULOSKELETAL USG
 USG HIP JOINT (RIGHT) USG KNEE JOINT (LEFT) USG KNEE JOINT (RIGHT) USG KUB USG MUSKULOSKELETAL USG") RADIOLOGY TESTS SONOGRAPHY,COLOR DOPPLER 3D/4D ANAMOLY SCAN 3D/4D ANAMOLY SCAN TWINS 3D/4D USG PELVIS ABDOMEN & PELVIS USG ABDOMEN UPPER USG ANKLE JOINT (LEFT) USG ANKLE JOINT (RIGHT) USG B SCAN BREAST
RADIOLOGY TESTS SONOGRAPHY,COLOR DOPPLER 3D/4D ANAMOLY SCAN 3D/4D ANAMOLY SCAN TWINS 3D/4D USG PELVIS ABDOMEN & PELVIS USG ABDOMEN UPPER USG ANKLE JOINT (LEFT) USG ANKLE JOINT (RIGHT) USG B SCAN BREAST
After the Chest X-Ray:
 After the Chest X-Ray: What To Do Next Alan S. Brody Professor of Radiology and Pediatrics Chief of Thoracic Imaging Cincinnati Children s Hospital Cincinnati, Ohio USA What Should We Do Next? CT scan?
After the Chest X-Ray: What To Do Next Alan S. Brody Professor of Radiology and Pediatrics Chief of Thoracic Imaging Cincinnati Children s Hospital Cincinnati, Ohio USA What Should We Do Next? CT scan?
17. Imaging and interventional radiology
 17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
5/31/2018. Ipsilateral Femoral Neck And Shaft Fractures. Ipsilateral Neck-Shaft Fractures Introduction. Ipsilateral Neck-Shaft Fractures Introduction
 Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016
 PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016 Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Nupur Verma, MD University
PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016 Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Nupur Verma, MD University
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
GUIDELINES FOR. Advanced. Imaging Studies
 GUIDELINES FOR Advanced Imaging Studies Locations Herrin Hospital Memorial Hospital of Carbondale St. Joseph Memorial Hospital 201 S 14th Street Herrin, IL 62948 618.942.2171 ext 35400 General Radiography*
GUIDELINES FOR Advanced Imaging Studies Locations Herrin Hospital Memorial Hospital of Carbondale St. Joseph Memorial Hospital 201 S 14th Street Herrin, IL 62948 618.942.2171 ext 35400 General Radiography*
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Physical and Radiographic Examination of the Spine
 Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
2017 Patient Pricelist
 2017 Patient Pricelist Attached are the most frequent charges at St. Elizabeth Healthcare. All patients are charged the same irrespective of one s ability to pay. The patient s responsibility may vary
2017 Patient Pricelist Attached are the most frequent charges at St. Elizabeth Healthcare. All patients are charged the same irrespective of one s ability to pay. The patient s responsibility may vary
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
S.U.M.Ph. "Nicolae Testemitanu" Department of Forensic Medicine 2013/2014. Prelection by Vasile Șarpe MD, MS, PhD, Assoc.
 S.U.M.Ph. "Nicolae Testemitanu" Department of Forensic Medicine 2013/2014 Prelection by Vasile Șarpe MD, MS, PhD, Assoc. Professor Lecture items General concepts, classification Trauma due to fall down
S.U.M.Ph. "Nicolae Testemitanu" Department of Forensic Medicine 2013/2014 Prelection by Vasile Șarpe MD, MS, PhD, Assoc. Professor Lecture items General concepts, classification Trauma due to fall down