Evidence Base for Child Abuse Fractures
|
|
|
- Agnes Barker
- 5 years ago
- Views:
Transcription
1 Evidence Base for Child Abuse Fractures SPR Sunrise Session May 17, 2018 Megan B. Marine, MD, FAAP Assistant Professor of Clinical Radiology, Pediatric Division Co-Director, Pediatric Radiology Fellowship Indiana University School of Medicine Riley Hospital for Children, Indianapolis, IN
2 No Disclosures
3 Childhood Fractures Fractures are a common childhood injury Consider history, age and developmental stage of child, fracture type and associated mechanism, as well as identification of other injuries In infants and toddlers, physical abuse is the cause of 12-20% of fractures (1) Any fracture can be caused by child abuse
4 History HPI: Details important Children able should be interviewed apart and by a professional skilled in forensic interviewing One study showed caregivers either provided no history or a history of a low-energy event in cases of abuse, whereas 29% of caregivers of those with accidental injury provided a high-energy event (2) PMH, FH, PE and lab evaluation important in consideration of differential diagnosis
5 Age 80% of all fractures from abuse were seen in children under 18 months in large review (3) In children <1yo, 25% fractures caused by child abuse (4)
6 Developmental Stage Children who are not yet mobile are more likely to have fractures caused by abuse (1) In nonambulatory patients, physical abuse is the more likely cause of humeral and femoral fractures than those who are walking (2) % of fractures caused by abuse declines sharply after child begins to walk (1)
7 *High Specificity CMLs Rib Fractures Scapular Fractures Spinous Process Fractures Sternal Fractures Moderate Specificity Multiple Fractures Vertebral Body Fractures Epiphyseal Separations Fractures Differing Ages Digit Fractures Complex Skull Fractures Low Specificity Subperiosteal New Bone Formation Clavicle Fractures Long-bone Shaft Fractures Linear Skull Fractures *Highest Specificity in Infants (5)Flaherty EG, et al. Pediatrics 2014;133:
8 Classic Metaphyseal Lesion Planar fracture through primary spongiosa of the metaphysis (6) Corner or bucket handle appearance Most common in distal femur, proximal and distal tibia, and proximal humeri Acute fractures difficult to visualize and commonly heal without new subperiosteal bone formation or sclerosis (7) Heal quickly and undetectable in up to 4 weeks (7)
9 Classic Metaphyseal Lesion High specificity for physical abuse, particularly in the first year life (6,8) Mechanism: Torsional and tractional shearing strains applied across metaphysis as in pulling or twisting of an extremity (7) Supported by similar lesions in breech and armling obstetric deliveries (9) CMLs are the most common long bone fracture found in infants who die of inflicted injury (10)







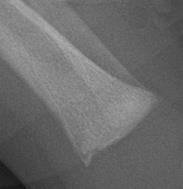
10 Classic Metaphyseal Lesions






11 Classic Metaphyseal Lesions
12 Rib Fractures Rib fractures, particularly posterior rib fractures, in young children are highly specific for abuse (3,5) Positive predictive value of rib fractures for child abuse in children <3yo has been reported up to 95% (11) A child with multiple rib fractures has a 7 in 10 chance of having been abused (3)

13 Rib Fractures Mechanism: Most caused by anterior-posterior compression as in an infant who is held around the chest, squeezed, and shaken (12)
14 Posterior Rib Fractures


15 Posterior Rib Fractures


16 CT Chest in 70 do Female



17 CT Chest in 70 do Female
18 Long-bone Shaft Fractures Low specificity but important as the single long bone diaphyseal fracture is the most common fracture pattern identified in abused children (4) Fracture pattern itself cannot clearly distinguish between abuse and nonabuse (2) Important for injury mechanism described by caregiver to match the extent and type of load required (13)

19 Long Bone Fracture Mechanism Transverse fracture Bending load applied perpendicular to bone
")
20 Long Bone Fracture Mechanism Spiral fracture Torsion or twisting of bone along its long axis Accidental spiral femur fracture reported in stairway falls with specific circumstances (14)

21 Long Bone Fracture Mechanism Oblique fracture Bending and torsion combination Accidental oblique femur fracture reported in stationary activity center as in an Exersaucer (15)

22 Long Bone Fracture Mechanism Buckle/impacted fracture Axial loading along length of bone Accidental buckle femur fractures reported in short fall to the knee (13)
23 Femoral Shaft Fractures A child with a femoral fractures has a 1 in 3-4 chance of having been abused (3) Key discriminator is the motor developmental level of the child Femoral fractures resulting from abuse are more commonly seen in children who are not yet walking
24 Humeral Shaft Fractures In a child less than 18 mo, humeral shaft fractures have a high likelihood of abuse (3) Supracondylar fractures are more likely to have non-abusive causes Case reported of infant rolling from prone to supine while child s arm was extended causing a spiraloblique midshaft humerus fracture (16)
25 Skull Fractures Majority of linear skull fractures are not inflicted (17) A short fall from several feet onto a hard surface can cause a linear, nondiastatic skull fracture (18, 19) Complex or bilateral skull fractures are typical of NAT (5)



26 3D Skull Reformats: 6 mo female


27 3D Skull Reformats: 21 mo male
28 Skeletal Survey ACR imaging recommendations available by age and presentation Child <24mo with suspicion for abuse should have skeletal survey (20) Additional fractures are found in 10%, with higher rates in infants (21) 2 week follow up skeletal survey provides additional information in up to one third of patients (20)
29 When is a Fracture Suspicious for Child Abuse? No history of injury Mechanism provided not consistent with type of fracture Inconsistent or changing histories Fracture in nonambulatory child Fracture of high specificity for abuse Multiple fractures Fractures of different ages Other injuries suspicious for abuse Delay in seeking care for an injury (5) Flaherty EG, et al. Pediatrics 2014;133:
30 References 1. Leventhal JM, Martin KD, Asnes AG. Incidence of fractures attributable to abuse in young hospitalized children: results rom analysis of a US database. Pediatrics. 2008;122(3): Hui C, Joughin E, Goldstein S, et al. Femoral fractures in children younger than three years: the role of nonaccidental injury. J Pediatr Orthop. 2008;28(3): Kemp AM, Dunstan F, Harrison S, et al. Patterns of skeletal fractures in child abuse: systematic review. BMJ. 2008;337:a Loder RT, Feinberg JR. Orthopaedic injuroes in children with nonaccidental trauma: demographics and incidence from the 2000 kids inpatient database. J Pediatr Orthop. 2008:28(6): Flaherty EG, Perez-Rossello JM, Levine MA et al. Evaluating children with fractures for child physical abuse. Pediatrics 2014;133: Kleinman PK. Diagnostic Imaging of Child Abuse. 2 nd ed. St. Louis, MO: Mosby; Kleinman PK. Problems in the diagnosis of metaphyseal fractures. Pediatr Radiol. 2008;38(suppl 3):S388-S Kleinman PK, Perez-Rossello JM, Newton AW, Feldman HA, Kleinmain PL. Prevalence of the classic metaphyseal lesion in infants at low versus high risk for abuse. AJR AM J Roentgenol. 2011;197(4): Ekengren K, Bergdahl S, Ekstrom G. Birth injuries to the epiphyseal cartilage. Acta Radiol Diagn (stockh) 1978;19:
31 10. Kleinman PK, Marks SC, Jr, Richmond JM, et al. Inflicted skeletal injury: a postmortem radiologic-histopathologic study in 31 infants. AJR Am J Roentgenol. 1995;165(3): Barsness KA, Cha E-S, Bensard DD, et al. The positive predictive value of rib fractures as an indicator of nonaccidental trauma in children. J Trauma. 2003;54(6): Kleinman PK, Marks, SC, Spevak MR, et al. Fractures of the rib heads in abused infants. Radiology 1992; Oct:185(1): Pierce MC, Bertocci G. Injury bio-mechanics and child abuse. Annu Rev Biomed Eng. 2008;10: Pierce MC, Bertocci GE, Janosky JE, et al. Femur fractures resulting from stair falls among children: an injury plausibility model. Pediatrics. 2005;115(6): Grant P, Mata MB, Tidwell M. Femur fractures in infants: a possible accidental etiology. Pedaitrics. 2001;108(4): Hymel KP, Jenny C. Abusive spiral fracture of the humerus: a videotaped exception. Arch Pediatr Adolesc Med. 1996;150(2): Wood JN, Christian CW, Adams, CM, et al. Skeletal surveys in infants with isolated skull fractures. Pediatrics. 2009;123(2)
32 18. Kleinman PK. The spectrum of nonaccidental injuries (child abuse) and its imitators. In: Hodler J, Zollikofer CL, Schulthess GK, eds. Musculoskeletal Disease Milan, Italy: Springer Italia; 2009: Laskey AL, Stump TE, Hicks RA, Smith JL. Yield of skeletal surveys in children,18months of age presenting with isolated skull fractures. J Pediatr. 2013;162(1): ACR appropriateness criteria: suspected physical child abuse. American College of Radiology Expert Panel on Pediatric Imaging: Sandra L Wooton-Gorges, Bruno P Soares, Adina L Alazraki, et. al. J Am Coll Radiol. 2017; 14: S338-S Duffy SO, Squires J, Fromkin JB et al. Use of skeletal surveys to evaluate for physical abuse: analysis of 703 consecutive skeletal surveys. Pediatrics 2011;127:e47 e52
33 Thank You
Common Abusive Skeletal Injuries
 Common Abusive Skeletal Injuries Paul Kleinman, M.D. Children s Hospital Harvard Medical School Boston, Ma. Rib fractures, especially posteromedial Rib fractures, especially posteromedial Kemp AM et. Al.
Common Abusive Skeletal Injuries Paul Kleinman, M.D. Children s Hospital Harvard Medical School Boston, Ma. Rib fractures, especially posteromedial Rib fractures, especially posteromedial Kemp AM et. Al.
Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics
 Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics Disclosure I have nothing to disclose Objectives Describe common accidental injuries which can be confused with child abuse Describe
Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics Disclosure I have nothing to disclose Objectives Describe common accidental injuries which can be confused with child abuse Describe
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Bilateral rib fractures 2 on right and 1 on left In different stages of healing, with left fracture older than right fractures
 More history: Seen by PCP yesterday because of vomiting and fussinesss. Called by ED today because Mom presents with same complaints. ED found nothing but got an abdominal x ray. ED now wants kid admitted
More history: Seen by PCP yesterday because of vomiting and fussinesss. Called by ED today because Mom presents with same complaints. ED found nothing but got an abdominal x ray. ED now wants kid admitted
Evaluation of a Pediatric Patient
 September 2005 Evaluation of a Pediatric Patient Percy Ballard, Harvard Medical School Year III Our Little Man: 6mo old male transferred to Children s from hospital in the Philippines 3mo history of meningitis,
September 2005 Evaluation of a Pediatric Patient Percy Ballard, Harvard Medical School Year III Our Little Man: 6mo old male transferred to Children s from hospital in the Philippines 3mo history of meningitis,
Radiologic Assessment of Child Abuse in Infants: A Focus on Plain Film Analysis of Highly Specific Fractures
 July 2006 Radiologic Assessment of Child Abuse in Infants: A Focus on Plain Film Analysis of Highly Specific Fractures Denise De Las Nueces, Harvard Medical School Year IV General Overview Introduction
July 2006 Radiologic Assessment of Child Abuse in Infants: A Focus on Plain Film Analysis of Highly Specific Fractures Denise De Las Nueces, Harvard Medical School Year IV General Overview Introduction
CORE-INFO: fractures in children
 CORE-INFO: fractures in children This leaflet summarises what is currently known about the relationship between fractures and physical abuse and will be of particular interest to paediatricians, general
CORE-INFO: fractures in children This leaflet summarises what is currently known about the relationship between fractures and physical abuse and will be of particular interest to paediatricians, general
10/8/17. I have no disclosures. What are they? Upper extremity fractures Lower extremity fractures Non accidental trauma
 I have no disclosures Upper extremity fractures Lower extremity fractures Non accidental trauma What are they? Fractures of the radius, ulna and/or humerus Who gets them? Active children usually after
I have no disclosures Upper extremity fractures Lower extremity fractures Non accidental trauma What are they? Fractures of the radius, ulna and/or humerus Who gets them? Active children usually after
Stair falls: caregiver s missed step as a source of childhood fractures
 J Child Orthop (2014) 8:77 81 DOI 10.1007/s11832-014-0551-x ORIGINAL CLINICAL ARTICLE Stair falls: caregiver s missed step as a source of childhood fractures Andrew T. Pennock George D. Gantsoudes Jennifer
J Child Orthop (2014) 8:77 81 DOI 10.1007/s11832-014-0551-x ORIGINAL CLINICAL ARTICLE Stair falls: caregiver s missed step as a source of childhood fractures Andrew T. Pennock George D. Gantsoudes Jennifer
Radiological investigations
 Nita Jain, MD, FRCPC The role of diagnostic imaging in the evaluation of child abuse Radiologists experienced in pediatric imaging can provide invaluable assistance to health care teams working to identify
Nita Jain, MD, FRCPC The role of diagnostic imaging in the evaluation of child abuse Radiologists experienced in pediatric imaging can provide invaluable assistance to health care teams working to identify
High Specificity Features on Plain Film of Non-Accidental Injury
 High Specificity Features on Plain Film of Non-Accidental Injury Adam A Dmytriw 1,2, Kota Talla 1, Munire Gündogan 2 1 Department of Medical Imaging, University of Toronto 2 Department of Diagnostic Radiology,
High Specificity Features on Plain Film of Non-Accidental Injury Adam A Dmytriw 1,2, Kota Talla 1, Munire Gündogan 2 1 Department of Medical Imaging, University of Toronto 2 Department of Diagnostic Radiology,
Childhood Fractures. Incomplete fractures more common. Ligaments stronger than bone. Tendons stronger than bone. Fractures may be pathologic
 Childhood Fractures Incomplete fractures more common Plastic bowing Torus / Buckle Greenstick Ligaments stronger than bone Fracture patterns different Physeal injury, not dislocation Tendons stronger than
Childhood Fractures Incomplete fractures more common Plastic bowing Torus / Buckle Greenstick Ligaments stronger than bone Fracture patterns different Physeal injury, not dislocation Tendons stronger than
OVERVIEW OF CHILD PHYSICAL ABUSE
 2011 MFMER slide-1 OVERVIEW OF CHILD PHYSICAL ABUSE Mark S. Mannenbach, MD Mayo Medical Center Rochester, MN 2011 MFMER slide-2 Objectives At the conclusion of this session, the participant will be able
2011 MFMER slide-1 OVERVIEW OF CHILD PHYSICAL ABUSE Mark S. Mannenbach, MD Mayo Medical Center Rochester, MN 2011 MFMER slide-2 Objectives At the conclusion of this session, the participant will be able
Forensic pediatric radiology: studies in living and deceased children Hoogendoorn, T.
 UvA-DARE (Digital Academic Repository) Forensic pediatric radiology: studies in living and deceased children Hoogendoorn, T. Link to publication Citation for published version (APA): Hoogendoorn, T. (2014).
UvA-DARE (Digital Academic Repository) Forensic pediatric radiology: studies in living and deceased children Hoogendoorn, T. Link to publication Citation for published version (APA): Hoogendoorn, T. (2014).
Pattern of Fractures in Non-Accidental Injuries in the Pediatric Population in Singapore
 Original Article Clinics in Orthopedic Surgery 2014;6:432-438 http://dx.doi.org/10.4055/cios.2014.6.4.432 Pattern of Fractures in Non-Accidental Injuries in the Pediatric Population in Singapore Sumanth
Original Article Clinics in Orthopedic Surgery 2014;6:432-438 http://dx.doi.org/10.4055/cios.2014.6.4.432 Pattern of Fractures in Non-Accidental Injuries in the Pediatric Population in Singapore Sumanth
5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains
 5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains Kristen Reeder, MD Child Abuse Pediatrician, REACH Program Children s Health SM Children s Medical Center Dallas Assistant Professor
5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains Kristen Reeder, MD Child Abuse Pediatrician, REACH Program Children s Health SM Children s Medical Center Dallas Assistant Professor
12/13/16. Jamie Hoffman-Rosenfeld, MD Medical Director, Queens CAC December 14, 2016
 Jamie Hoffman-Rosenfeld, MD Medical Director, Queens CAC December 14, 2016 Jamie Hoffman-Rosenfeld, MD, has no financial relationships with any commercial interests. The learner will be able to:! Articulate
Jamie Hoffman-Rosenfeld, MD Medical Director, Queens CAC December 14, 2016 Jamie Hoffman-Rosenfeld, MD, has no financial relationships with any commercial interests. The learner will be able to:! Articulate
Femur Shaft Fractures Under 10 years old
 1 Femur Shaft Fractures Under 10 years old Richard M Schwend MD Professor Orthopaedics and Pediatrics Director of Research Children s Mercy Hospital Kansas City MO, USA rmschwend@cmh.edu 5 th Annual SLAOTI
1 Femur Shaft Fractures Under 10 years old Richard M Schwend MD Professor Orthopaedics and Pediatrics Director of Research Children s Mercy Hospital Kansas City MO, USA rmschwend@cmh.edu 5 th Annual SLAOTI
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
6/23/2017. What do you see? skull fracture
 What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
Common Orthopaedic Injuries in Children
 Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
They re not little adults, but they are little humans. Pearls for your next pediatric trauma patient. Children are little humans
 They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
CHILD MALTREATMENT- GUIDELINES FOR SUSPICION and INITIAL MEDICAL EVALUATION DRAFT May Leslie M. Quinn M.D.
 CHILD MALTREATMENT- GUIDELINES FOR SUSPICION and INITIAL MEDICAL EVALUATION DRAFT May 2012 - Leslie M. Quinn M.D. PHYSICAL ABUSE: For any child presenting with signs and or symptoms of an injury consider
CHILD MALTREATMENT- GUIDELINES FOR SUSPICION and INITIAL MEDICAL EVALUATION DRAFT May 2012 - Leslie M. Quinn M.D. PHYSICAL ABUSE: For any child presenting with signs and or symptoms of an injury consider
Disclosure. Physical Abuse. Objectives. What is the Mechanism of the Injury?
 Disclosure Abuse or Not Abuse: What is the Answer? Natalie Kissoon, MD Assistant Professor Division of Child Abuse Pediatrics University of Texas Health Science Natalie Kissoon, MD has no relationships
Disclosure Abuse or Not Abuse: What is the Answer? Natalie Kissoon, MD Assistant Professor Division of Child Abuse Pediatrics University of Texas Health Science Natalie Kissoon, MD has no relationships
Trauma Center Practice Management Guideline Blank Children s Hospital (BCH) Des Moines
 Des Moines") Trauma Center Practice Management Guideline Blank Children s Hospital (BCH) Des Moines Non-Accidental Trauma (NAT) PEDIATRIC Practice Management Guideline Contact: Trauma Center Medical Director/ Trauma
Trauma Center Practice Management Guideline Blank Children s Hospital (BCH) Des Moines Non-Accidental Trauma (NAT) PEDIATRIC Practice Management Guideline Contact: Trauma Center Medical Director/ Trauma
Fractures in Abused Children What tests? When?
 Fractures in Abused Children What tests? When? VFPMS Seminar Anne Smith, Medical Director VFPMS Background What do we want to know? Does bone injury exist? What pattern/type of injury is this? Are there
Fractures in Abused Children What tests? When? VFPMS Seminar Anne Smith, Medical Director VFPMS Background What do we want to know? Does bone injury exist? What pattern/type of injury is this? Are there
The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast
 The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast September 27, 2018 Introduction: Hello everyone, my name is Dominique Piché
The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast September 27, 2018 Introduction: Hello everyone, my name is Dominique Piché
Lower Extremity Alignment: Genu Varum / Valgum
 Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Pediatric Orthopedics
 Pediatric Orthopedics Alexander Rogers, MD Associate Professor Emergency Medicine and Pediatrics Michigan Medicine/University of Michigan Disclosures I have no conflicts of interest to disclose I will
Pediatric Orthopedics Alexander Rogers, MD Associate Professor Emergency Medicine and Pediatrics Michigan Medicine/University of Michigan Disclosures I have no conflicts of interest to disclose I will
Downloaded from by on 12/24/17 from IP address Copyright ARRS. For personal use only; all rights reserved
 Pediatric Imaging Prosser et al. Radiologic Dating of Pediatric Fractures Ingrid Prosser 1 Sabine Maguire 1 Sara K. Harrison 2 Mala Mann 3 Jonathan R. Sibert 1 Alison M. Kemp 1 Welsh Child Protection Systematic
Pediatric Imaging Prosser et al. Radiologic Dating of Pediatric Fractures Ingrid Prosser 1 Sabine Maguire 1 Sara K. Harrison 2 Mala Mann 3 Jonathan R. Sibert 1 Alison M. Kemp 1 Welsh Child Protection Systematic
Pediatric Injuries/Fractures. Rena Heathcote
 Pediatric Injuries/Fractures Rena Heathcote INTRODUCTION Incidence Anatomy of the Growing Bone Injury Patterns What can we X-ray PEDIATRIC FRACTURES INCIDENCE What makes children susceptible to fractures?
Pediatric Injuries/Fractures Rena Heathcote INTRODUCTION Incidence Anatomy of the Growing Bone Injury Patterns What can we X-ray PEDIATRIC FRACTURES INCIDENCE What makes children susceptible to fractures?
UvA-DARE (Digital Academic Repository)
") UvA-DARE (Digital Academic Repository) Skeletal imaging of child abuse (non-accidental injury) Offiah, A.; van Rijn, R.R.; Perez-Rossello, J.M.; Kleinman, P.K. Published in: Pediatric radiology DOI: 10.1007/s00247-009-1157-1
UvA-DARE (Digital Academic Repository) Skeletal imaging of child abuse (non-accidental injury) Offiah, A.; van Rijn, R.R.; Perez-Rossello, J.M.; Kleinman, P.K. Published in: Pediatric radiology DOI: 10.1007/s00247-009-1157-1
Imaging of non-accidental injury; what is clinical best practice?
 REVIEW ARTICLE Imaging of non-accidental injury; what is clinical best practice? Amy Nguyen, BRadMedImag (Hons), & Robin Hart, PhD Department of Medical Imaging and Radiation Sciences, Faculty of Medicine,
REVIEW ARTICLE Imaging of non-accidental injury; what is clinical best practice? Amy Nguyen, BRadMedImag (Hons), & Robin Hart, PhD Department of Medical Imaging and Radiation Sciences, Faculty of Medicine,
7/23/2018 DESCRIBING THE FRACTURE. Pattern Open vs closed Location BASIC PRINCIPLES OF FRACTURE MANAGEMENT. Anjan R. Shah MD July 21, 2018.
 BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles. Striated Skeletal. Smooth
 1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles
 1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
Pediatric Elbow Radiology. Seema Awatramani, MD Friday, April 5, 2018 ACOEP Spring Seminar
 Pediatric Elbow Radiology Seema Awatramani, MD Friday, April 5, 2018 ACOEP Spring Seminar Disclosure I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or
Pediatric Elbow Radiology Seema Awatramani, MD Friday, April 5, 2018 ACOEP Spring Seminar Disclosure I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or
Multicentre study of physical abuse and limb fractures in young children in the East Anglia Region, UK
 1 Department of Orthopaedics, Peterborough City Hospital, Peterborough, UK 2 Department of Paediatrics, Peterborough City Hospital, Peterborough, UK 3 Statistical Laboratory, University of Cambridge, Cambridge,
1 Department of Orthopaedics, Peterborough City Hospital, Peterborough, UK 2 Department of Paediatrics, Peterborough City Hospital, Peterborough, UK 3 Statistical Laboratory, University of Cambridge, Cambridge,
Guide to the Medical Evaluation in Suspected Physical Abuse
 Guide to the Medical Evaluation in Suspected Physical Abuse Introduction Every year more than 3 million referrals are made to child protective services for concerns of child abuse and neglect with almost
Guide to the Medical Evaluation in Suspected Physical Abuse Introduction Every year more than 3 million referrals are made to child protective services for concerns of child abuse and neglect with almost
PHYSICAL ABUSE: INITIAL EVALUATION AND MANAGEMENT **Child Protection MD is available by pager for questions or formal consultation **
 PHYSICAL ABUSE: INITIAL EVALUATION AND MANAGEMENT **Child Protection MD is available by pager for questions or formal consultation ** I. RECOGNITION A. History 1. Unexplained or un-witnessed injury 2.
PHYSICAL ABUSE: INITIAL EVALUATION AND MANAGEMENT **Child Protection MD is available by pager for questions or formal consultation ** I. RECOGNITION A. History 1. Unexplained or un-witnessed injury 2.
5/31/2018. Ipsilateral Femoral Neck And Shaft Fractures. Ipsilateral Neck-Shaft Fractures Introduction. Ipsilateral Neck-Shaft Fractures Introduction
 Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
11/4/2018 SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING SPEAKER DISCLOSURES
 SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING Charles S. Resnik, M.D. Professor of Radiology University of Maryland School of Medicine Upon completion of this presentation, participants will be better able
SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING Charles S. Resnik, M.D. Professor of Radiology University of Maryland School of Medicine Upon completion of this presentation, participants will be better able
ORTHOPEDIC ASPECTS CHILD ABUSE. A summary of the physical, metaphysical, psychological, and sociological aspects of Non-
 ORTHOPEDIC ASPECTS OF CHILD ABUSE A summary of the physical, metaphysical, psychological, and sociological aspects of Non- Accidental Injury with specific references to both the perpetrator and victim
ORTHOPEDIC ASPECTS OF CHILD ABUSE A summary of the physical, metaphysical, psychological, and sociological aspects of Non- Accidental Injury with specific references to both the perpetrator and victim
Orthopedics in Motion Tristan Hartzell, MD January 27, 2016
 Orthopedics in Motion 2016 Tristan Hartzell, MD January 27, 2016 Humerus fractures Proximal Shaft Distal Objectives 1) Understand the anatomy 2) Epidemiology and mechanisms of injury 3) Types of fractures
Orthopedics in Motion 2016 Tristan Hartzell, MD January 27, 2016 Humerus fractures Proximal Shaft Distal Objectives 1) Understand the anatomy 2) Epidemiology and mechanisms of injury 3) Types of fractures
ACR Appropriateness Criteria Suspected Physical Abuse Child EVIDENCE TABLE
 6. Merten DF, Carpenter BL. Radiologic imaging of inflicted injury in the child abuse syndrome. Pediatr Clin North Am. 1990;7():815-87. 7. Servaes S, Brown SD, Choudhary AK, et al. The etiology and significance
6. Merten DF, Carpenter BL. Radiologic imaging of inflicted injury in the child abuse syndrome. Pediatr Clin North Am. 1990;7():815-87. 7. Servaes S, Brown SD, Choudhary AK, et al. The etiology and significance
A Timetable for the Radiologic Features of Fracture Healing in Young Children
 Pediatric Imaging Original Research Prosser et al. Imaging Signs of Fracture Healing in Young Children Pediatric Imaging Original Research Downloaded from www.ajronline.org by 37.44.23.165 on 12/12/17
Pediatric Imaging Original Research Prosser et al. Imaging Signs of Fracture Healing in Young Children Pediatric Imaging Original Research Downloaded from www.ajronline.org by 37.44.23.165 on 12/12/17
THE NANCY NAIL. The End Caps ADVANTAGES OF NANCY NAIL
 NANCY NAIL THE NANCY NAIL Nancy nails are manufactured from a specific titanyum alloy with proprietary surface treatment, which provides increased fatigue resistance. Six nail diameters (1.5 mm 2.0 mm
NANCY NAIL THE NANCY NAIL Nancy nails are manufactured from a specific titanyum alloy with proprietary surface treatment, which provides increased fatigue resistance. Six nail diameters (1.5 mm 2.0 mm
A Probable Case of Child Abuse from Historic Gloucester
 A Probable Case of Child Abuse from Historic Gloucester Bernadette M Manifold Department of Archaeology, School of Human and Environmental Sciences, University of Reading, Whiteknights, Reading Address
A Probable Case of Child Abuse from Historic Gloucester Bernadette M Manifold Department of Archaeology, School of Human and Environmental Sciences, University of Reading, Whiteknights, Reading Address
Distal Femur Fractures in The Elderly The Ideal Construct
 Distal Femur Fractures in The Elderly The Ideal Construct Tak-Wing Lau Department of Orthopaedics and Traumatology Queen Mary Hospital The University of Hong Kong Singapore Trauma 2015 Trauma Through the
Distal Femur Fractures in The Elderly The Ideal Construct Tak-Wing Lau Department of Orthopaedics and Traumatology Queen Mary Hospital The University of Hong Kong Singapore Trauma 2015 Trauma Through the
The Shoulder Complex. Anatomy. Articulations 12/11/2017. Oak Ridge High School Conroe, Texas. Clavicle Collar Bone Scapula Shoulder Blade Humerus
 The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne
 Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne FRACTURE MANAGEMENT I Simple closed fracture : Complete or Incomplete Stable or unstable II Open fracture III Multiple fracture IV Polytrauma Fractures
Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne FRACTURE MANAGEMENT I Simple closed fracture : Complete or Incomplete Stable or unstable II Open fracture III Multiple fracture IV Polytrauma Fractures
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA. Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009
 EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
Non-Accidental Trauma (NAT) Protocol
 Protocol") Non-Accidental Trauma (NAT) Protocol All children suspected of non-accidental trauma will have a complete work-up including a complete history and physical exam with a focus on injuries and explanation
Non-Accidental Trauma (NAT) Protocol All children suspected of non-accidental trauma will have a complete work-up including a complete history and physical exam with a focus on injuries and explanation
Screening for and Assessment of Osteonecrosis in Oncology Patients. Sue C. Kaste, DO SPR Postgraduate Course 2015
 Screening for and Assessment of Osteonecrosis in Oncology Patients Sue C. Kaste, DO SPR Postgraduate Course 2015 The author declares no potential conflicts of interest or financial disclosures Osteonecrosis
Screening for and Assessment of Osteonecrosis in Oncology Patients Sue C. Kaste, DO SPR Postgraduate Course 2015 The author declares no potential conflicts of interest or financial disclosures Osteonecrosis
PEDIATRIC UPPER EXTREMITY FRACTURE MANAGEMENT JULIA RAWLINGS, MD SPORTS MEDICINE SYMPOSIUM: THE PEDIATRIC ATHLETE 2 MARCH 2018
 PEDIATRIC UPPER EXTREMITY FRACTURE MANAGEMENT JULIA RAWLINGS, MD SPORTS MEDICINE SYMPOSIUM: THE PEDIATRIC ATHLETE 2 MARCH 2018 DISCLOSURE I have nothing to disclose. 2 OBJECTIVES Discuss the diagnosis,
PEDIATRIC UPPER EXTREMITY FRACTURE MANAGEMENT JULIA RAWLINGS, MD SPORTS MEDICINE SYMPOSIUM: THE PEDIATRIC ATHLETE 2 MARCH 2018 DISCLOSURE I have nothing to disclose. 2 OBJECTIVES Discuss the diagnosis,
LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia.
 LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia. LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia.
LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia. LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia.
Fractures of the shoulder girdle, elbow and fractures of the humerus. H. Sithebe 2012
 Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Proteus XR/f Patient positioning guide
 Proteus XR/f Patient positioning guide PROTEUS XR/F Now a single digital x-ray room accommodates nearly all your radiographic studies. With extended tube coverage and wireless detectors, Proteus XR/f gives
Proteus XR/f Patient positioning guide PROTEUS XR/F Now a single digital x-ray room accommodates nearly all your radiographic studies. With extended tube coverage and wireless detectors, Proteus XR/f gives
1/19/2018. Winter injuries to the shoulder and elbow. Highgate Private Hospital (Whittington Health NHS Trust)
") Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Disclosure. Learning ObjecAves. A Quick Review. Pediatric Fractures. The Developing Bone
 How to Bend but not Break Managing Pediatric Orthopedic Injuries in the Emergency Department Disclosure Nothing to disclosure No conflict of interest related to this topic Adam Cheng, MD, FRCPC Division
How to Bend but not Break Managing Pediatric Orthopedic Injuries in the Emergency Department Disclosure Nothing to disclosure No conflict of interest related to this topic Adam Cheng, MD, FRCPC Division
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh
 Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions
 54 Questions") Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What is caused by overexerting or tearing of a muscle? p. 375 A.) Dislocation B.) Sprain C.) Fracture *D.)
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What is caused by overexerting or tearing of a muscle? p. 375 A.) Dislocation B.) Sprain C.) Fracture *D.)
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
SPR 2017 General Pediatric Radiology Categorical Course: Musculoskeletal May 16, 2017 SAM References
 Elbow: Don't be a FOOL Kiery Braithwaite, MD SPR 2017 General Pediatric Radiology Categorical Course: Musculoskeletal May 16, 2017 SAM 1. Which pediatric elbow fracture is most commonly seen in the absence
Elbow: Don't be a FOOL Kiery Braithwaite, MD SPR 2017 General Pediatric Radiology Categorical Course: Musculoskeletal May 16, 2017 SAM 1. Which pediatric elbow fracture is most commonly seen in the absence
Children diagnosed with skull fractures are often. Transfer of children with isolated linear skull fractures: is it worth the cost?
 clinical article J Neurosurg Pediatr 17:602 606, 2016 Transfer of children with isolated linear skull fractures: is it worth the cost? Ian K. White, MD, 1 Ecaterina Pestereva, BS, 1 Kashif A. Shaikh, MD,
clinical article J Neurosurg Pediatr 17:602 606, 2016 Transfer of children with isolated linear skull fractures: is it worth the cost? Ian K. White, MD, 1 Ecaterina Pestereva, BS, 1 Kashif A. Shaikh, MD,
LOCKING TEP LOCKING TITANIUM ELASTIC PIN INTRAMEDULLARY NAIL
 LOCKING TEP LOCKING TITANIUM ELASTIC PIN INTRAMEDULLARY NAIL ... Index -3 3-8 8 9 9 0 7 Introduction Features Indicatiıons Surgical Technique Femoral Surgical Technique Tibial Surgical Technique Ulna Radius
LOCKING TEP LOCKING TITANIUM ELASTIC PIN INTRAMEDULLARY NAIL ... Index -3 3-8 8 9 9 0 7 Introduction Features Indicatiıons Surgical Technique Femoral Surgical Technique Tibial Surgical Technique Ulna Radius
Disclosures. Fracture vs. Break: Is There a Difference? Jennifer Weiner, MS, RN, CPNP AC/PC March 21, Fracture vs. Break. Learning Objectives
 39 th National Conference on Pediatric Health Care Fracture vs. Break: Is There a Difference? Jennifer Weiner, MS, RN, CPNP AC/PC March 21, 2018 March 19-22, 2018 CHICAGO Disclosures I have no conflicts
39 th National Conference on Pediatric Health Care Fracture vs. Break: Is There a Difference? Jennifer Weiner, MS, RN, CPNP AC/PC March 21, 2018 March 19-22, 2018 CHICAGO Disclosures I have no conflicts
OUTLINE FRACTURES OUTLINE. PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT. Mohammad Diab M.D. UCSF FRACTURE
 PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT FRACTURE Mohammad Diab M.D. UCSF FRACTURE articular displacement < 2 mm. accept FRACTURES routine imaging S-H 3 S-H 4 displacement > 2 mm. ORIF
PÆDIATRIC ORTHOPÆDIC CHALLENGES in the EMERGENCY DEPARTMENT FRACTURE Mohammad Diab M.D. UCSF FRACTURE articular displacement < 2 mm. accept FRACTURES routine imaging S-H 3 S-H 4 displacement > 2 mm. ORIF
Country Health SA Medical Imaging
 Country Health SA Medical Imaging REMOTE OPERATORS POSITIONING GUIDE Contents Image Evaluation Page 4 Positioning Guides Section 1 - THORAX 1.1 Chest Page 5 1.2 Bedside Chest Page 7 1.3 Ribs Page 8 Section
Country Health SA Medical Imaging REMOTE OPERATORS POSITIONING GUIDE Contents Image Evaluation Page 4 Positioning Guides Section 1 - THORAX 1.1 Chest Page 5 1.2 Bedside Chest Page 7 1.3 Ribs Page 8 Section
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
Introduction to Fractures. Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3
 Introduction to Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3 Definitions A fracture is an interruption in the continuity of bone Fracture = Break Fracture: mechanical damage produced in a
Introduction to Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3 Definitions A fracture is an interruption in the continuity of bone Fracture = Break Fracture: mechanical damage produced in a
Basic Radiographic Principles Part II
 Basic Radiographic Principles Part II Kristopher Avant, D.O. October 19 th, 2016 I have no disclosures relevant to the material presented in this discussion. Good Stuff!!! 1 Really? Really! Musculoskeletal
Basic Radiographic Principles Part II Kristopher Avant, D.O. October 19 th, 2016 I have no disclosures relevant to the material presented in this discussion. Good Stuff!!! 1 Really? Really! Musculoskeletal
Long bones manifestations of congenital syphilis
 Long bones manifestations of congenital syphilis Poster No.: C-0139 Congress: ECR 2011 Type: Educational Exhibit Authors: T. F. de Souza 1, P. P. Collier 1, E. J. M. Bronzatto 1, G. L. P. Keywords: DOI:
Long bones manifestations of congenital syphilis Poster No.: C-0139 Congress: ECR 2011 Type: Educational Exhibit Authors: T. F. de Souza 1, P. P. Collier 1, E. J. M. Bronzatto 1, G. L. P. Keywords: DOI:
RADIOGRAPHY OF THE KNEE, PATELLA, and FEMUR
 RADIOGRAPHY OF THE KNEE, PATELLA, and FEMUR KNEE AP Projection Patient Position: Part Position: Leg in Center Femoral condyles Central Ray: - Asthenic patient - if ASIS to tabletop is < 19 cm Sthenic patient
RADIOGRAPHY OF THE KNEE, PATELLA, and FEMUR KNEE AP Projection Patient Position: Part Position: Leg in Center Femoral condyles Central Ray: - Asthenic patient - if ASIS to tabletop is < 19 cm Sthenic patient
The differential diagnosis for a young child with 1 or more fractures is
 Advances in Pediatrics 57 (2010) 63 83 ADVANCES IN PEDIATRICS Controversies in the Evaluation of Young Children with Fractures Melissa K. Egge, MD a, *, Carol D. Berkowitz, MD b,c a Department of Pediatrics,
Advances in Pediatrics 57 (2010) 63 83 ADVANCES IN PEDIATRICS Controversies in the Evaluation of Young Children with Fractures Melissa K. Egge, MD a, *, Carol D. Berkowitz, MD b,c a Department of Pediatrics,
FOOSH It sounded like a fun thing at the time!
 FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
Physeal Fractures and Growth Arrest
 Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Routine Guide EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION. 14x17 CW* 14x17LW 14x17LW. 14x17LW 14x17LW 14x17LW
 EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION A-C Joints without weights with weights 14x17 CW* One 14x17 divided; both shoulders on one exposure. *If part does not fit, do 10x12s CW. Both
EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION A-C Joints without weights with weights 14x17 CW* One 14x17 divided; both shoulders on one exposure. *If part does not fit, do 10x12s CW. Both
Since the publication of The Battered-Child Syndrome in 1962,1
 The new england journal of medicine Clinical Practice Caren G. Solomon, M.D., M.P.H., Editor Physical Abuse of Children Carol D. Berkowitz, M.D. This Journal feature begins with a case vignette highlighting
The new england journal of medicine Clinical Practice Caren G. Solomon, M.D., M.P.H., Editor Physical Abuse of Children Carol D. Berkowitz, M.D. This Journal feature begins with a case vignette highlighting
Overview of Abusive Head Trauma: What Everyone Needs to Know. 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012
 Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
---Start of Pediatric and Adolescent Upper Extremity Fractures---
 Presented by: Mary Lloyd Ireland Professor Dept. of Orthopaedic Surgery and Sports Medicine University of Kentucky Lexington KY www.marylloydireland.com ---Start of Pediatric and Adolescent Upper Extremity
Presented by: Mary Lloyd Ireland Professor Dept. of Orthopaedic Surgery and Sports Medicine University of Kentucky Lexington KY www.marylloydireland.com ---Start of Pediatric and Adolescent Upper Extremity
Relationship between the Apex of Flexible Nail and the Level of Fracture: A Biomechanical Study Ahmed N* 1, Gakhar H 2, Cheung G 3, Sharma A 4
 Relationship between the Apex of Flexible Nail and the Level of Fracture: A Biomechanical Study Ahmed N* 1, Gakhar H 2, Cheung G 3, Sharma A 4 Abstract Background Centre of Orthopaedic biomechanics, Bath
Relationship between the Apex of Flexible Nail and the Level of Fracture: A Biomechanical Study Ahmed N* 1, Gakhar H 2, Cheung G 3, Sharma A 4 Abstract Background Centre of Orthopaedic biomechanics, Bath
Treatment of delayed union or non-union of the tibial shaft with partial fibulectomy and an Ilizarov frame
 Acta Orthop. Belg., 2007, 73, 630-634 ORIGINAL STUDY Treatment of delayed union or non-union of the tibial shaft with partial fibulectomy and an Ilizarov frame Jo DUJARDYN, Johan LAMMENS From the University
Acta Orthop. Belg., 2007, 73, 630-634 ORIGINAL STUDY Treatment of delayed union or non-union of the tibial shaft with partial fibulectomy and an Ilizarov frame Jo DUJARDYN, Johan LAMMENS From the University
FOOSH It sounded like a fun thing at the time!
 FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
A jump park is an interconnected network of trampolines designed for entertainment purposes
 A jump park is an interconnected network of trampolines designed for entertainment purposes One of fastest growing recreational-entertainment businesses in the U.S. Approximately 350 operating jump parks
A jump park is an interconnected network of trampolines designed for entertainment purposes One of fastest growing recreational-entertainment businesses in the U.S. Approximately 350 operating jump parks
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
Society for Pediatric Radiology 2015 Hands on Session. DDH: Pitfalls and Practical Tips
 Society for Pediatric Radiology 2015 Hands on Session DDH: Pitfalls and Practical Tips Michael A. DiPietro, M.D. John F. Holt Collegiate Professor of Radiology Professor of Pediatrics and Communicable
Society for Pediatric Radiology 2015 Hands on Session DDH: Pitfalls and Practical Tips Michael A. DiPietro, M.D. John F. Holt Collegiate Professor of Radiology Professor of Pediatrics and Communicable
Principles of Musculoskeletal Injuries
 Principles of Musculoskeletal Injuries Wiroon Laupattarakasem, M.D. Professor in Orthopaedics Faculty of Medicine Khon Kaen University Contents: Fractures and Dislocations Mechanisms of injuries Description
Principles of Musculoskeletal Injuries Wiroon Laupattarakasem, M.D. Professor in Orthopaedics Faculty of Medicine Khon Kaen University Contents: Fractures and Dislocations Mechanisms of injuries Description
Lecture (10) Bone Fractures. Resources: - Lecture by dr.alboukai - Diagnostic imaging book
 Bone Fractures. Resources: - Lecture by dr.alboukai - Diagnostic imaging book") Lecture (10) Bone Fractures Hanan Alsalman Hanan Alrabiah Reem Aljurayyad Ayshah Almahboob Ghadeer Alwuhyad Khawlah AlOthman Dalal Alqadi Suliman Alshammari Maha AlKubaidan Rawabi Alghamdi Resources: -
Lecture (10) Bone Fractures Hanan Alsalman Hanan Alrabiah Reem Aljurayyad Ayshah Almahboob Ghadeer Alwuhyad Khawlah AlOthman Dalal Alqadi Suliman Alshammari Maha AlKubaidan Rawabi Alghamdi Resources: -
FIRST DESCRIBED RETROGRADE TECHNIQUE USING MEDIAL EPICONDYLE 6/5/2018. RETROGRADE vs. ANTEGRADE FEMORAL NAILING
 What do I do? ISSUES ANTEGRADE vs. RETROGRADE PIRIFORMIS vs. TROCHANTER FLAT vs. FRACTURE TABLE SWIONTKOWSKI, 1984 FIRST DESCRIBED RETROGRADE TECHNIQUE USING MEDIAL EPICONDYLE 1 RETROGRADE NAILING SANDERS
What do I do? ISSUES ANTEGRADE vs. RETROGRADE PIRIFORMIS vs. TROCHANTER FLAT vs. FRACTURE TABLE SWIONTKOWSKI, 1984 FIRST DESCRIBED RETROGRADE TECHNIQUE USING MEDIAL EPICONDYLE 1 RETROGRADE NAILING SANDERS
Chapter XIX.1. Fractures May 2002
 Case Based Pediatrics For Medical Students and Residents Department of Pediatrics, University of Hawaii John A. Burns School of Medicine Chapter XIX.1. Fractures May 2002 Annemarie Uliasz The skeletal
Case Based Pediatrics For Medical Students and Residents Department of Pediatrics, University of Hawaii John A. Burns School of Medicine Chapter XIX.1. Fractures May 2002 Annemarie Uliasz The skeletal
11/25/2012. Chapter 7 Part 2: Bones! Skeletal Organization. The Skull. Skull Bones to Know Cranium
 Chapter 7 Part 2: Bones! 5) Distinguish between the axial and appendicular skeletons and name the major parts of each 6) Locate and identify the bones and the major features of the bones that compose the
Chapter 7 Part 2: Bones! 5) Distinguish between the axial and appendicular skeletons and name the major parts of each 6) Locate and identify the bones and the major features of the bones that compose the
Suspected Physical Abuse Clinical Practice Guideline
 Suspected Physical Abuse Clinical Practice Guideline WHEN TO CONSIDER ABUSE Consider abuse on the differential Injuries to multiple organ systems Injuries in different stages of healing Patterned injuries
Suspected Physical Abuse Clinical Practice Guideline WHEN TO CONSIDER ABUSE Consider abuse on the differential Injuries to multiple organ systems Injuries in different stages of healing Patterned injuries
Fracture fixation. Types. Mechanical considerations. Biomechanics of fracture fixation. External fixation. Internal fixation
 Fracture fixation Biomechanics of fracture fixation Types External fixation Mechanical considerations Internal fixation Mechanical considerations in treatment of 1. In the external fixation: fracture When
Fracture fixation Biomechanics of fracture fixation Types External fixation Mechanical considerations Internal fixation Mechanical considerations in treatment of 1. In the external fixation: fracture When
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Clinical Practice Guidelines: Can I Learn to Live With Them? What s in the News These Days 2/11/2016. Excessive Costs of Medical Care
 Orthopaedic Trauma Fracture Care: Pushing the Envelope San Diego Clinical Practice Guidelines: Can I Learn to Live With Them? Andrew H. Schmidt, MD What s in the News These Days Excessive Costs of Medical
Orthopaedic Trauma Fracture Care: Pushing the Envelope San Diego Clinical Practice Guidelines: Can I Learn to Live With Them? Andrew H. Schmidt, MD What s in the News These Days Excessive Costs of Medical
DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT
 P.O. Box 6743 New Albany, IN 47151-6743 (812) 945-5515 (812) 945-5632 Fax WWW.KMX.CC DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT Patient Name: Lubna Ibriham Date of Digitization and
P.O. Box 6743 New Albany, IN 47151-6743 (812) 945-5515 (812) 945-5632 Fax WWW.KMX.CC DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT Patient Name: Lubna Ibriham Date of Digitization and
Bone Marrow Changes on MRI: Self-Assessment Module
 1.5 CME 1.0 SAM AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Bone Marrow Changes on MRI: Self-Assessment Module Catherine C. Roberts 1, William B. Morrison 2, Laura W. Bancroft 3,4, Felix S.
1.5 CME 1.0 SAM AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Bone Marrow Changes on MRI: Self-Assessment Module Catherine C. Roberts 1, William B. Morrison 2, Laura W. Bancroft 3,4, Felix S.