Diagnosis of tuberculosis in children H Simon Schaaf
|
|
|
- George Alexander
- 5 years ago
- Views:
Transcription


1 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH)

2 Estimated TB incidence rates 2014 WHO Global TB Report 2015
3 Epidemiology ~ notified TB cases in South Africa/year ( % of population) Children make up 15-20% of the national TB burden The MDR-TB estimate (overall) for was of 2.8%; (95%CI: 2.0%-3.6%); remained stable from previous survey in of 2.9% (95% CI: 2.4%-3.5%). However, increase in RIF resistance as well as INH mono-resistance Of concern is a rising trend in both RIFmonoresistant and INH-monoresistant TB

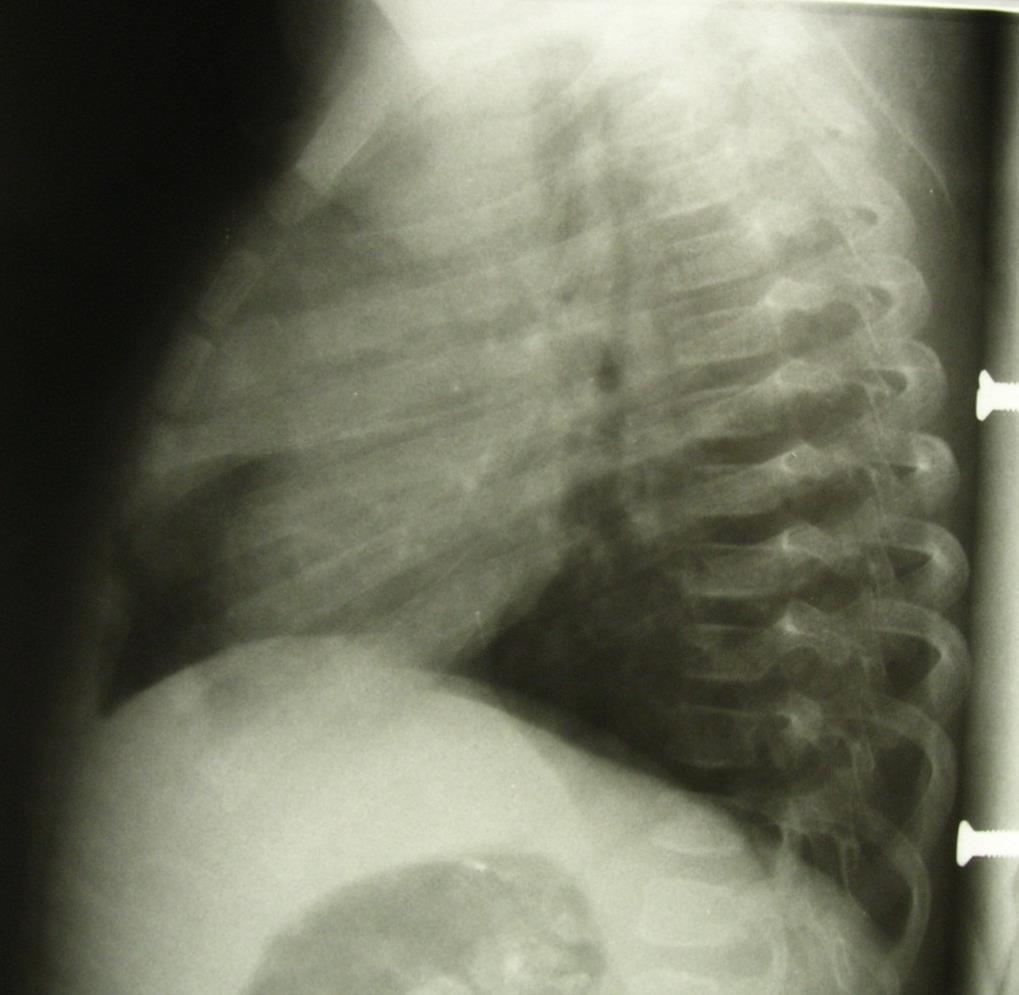
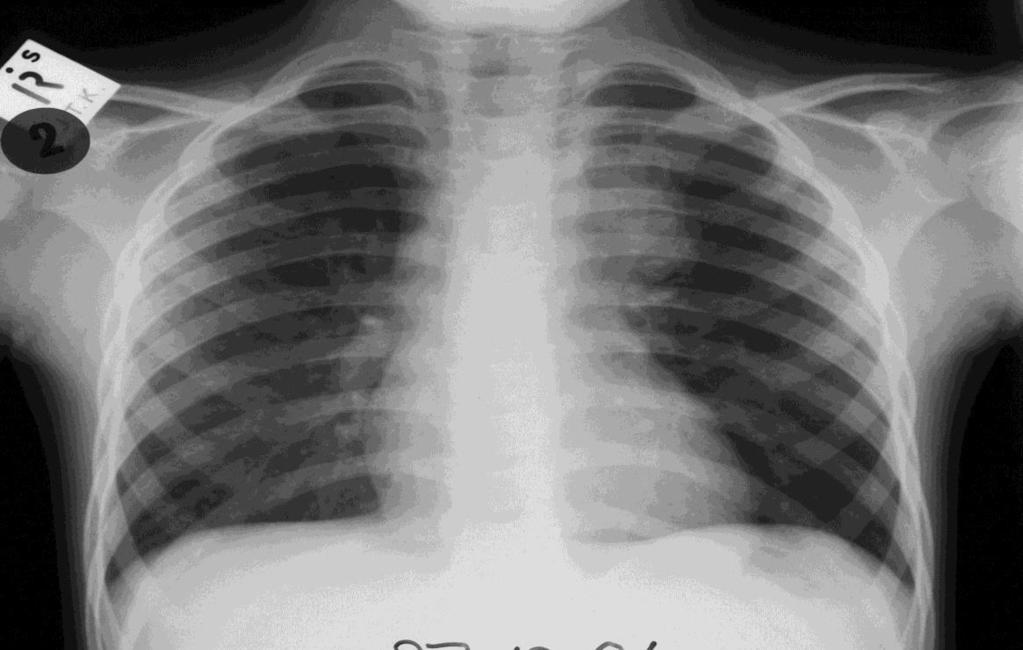
4 Is diagnosing TB in children difficult? Case 1: 3-year-old, coughing 3 weeks, LOW, fever Father recently diagnosed with smear-positive PTB, living in same house
5 Is diagnosing TB in children difficult? Case 2: Baby-girl 14 weeks cough >4 weeks. Coughing bouts turns red says mom. Was seen at clinic several times. Amoxicillin given. Mom told to stop smoking Fever for last two weeks. Unbooked mom: Baby born at home. Breastfed since birth, but on clinic card not thriving. No BCG given (out of stock) No-one known with TB at home. Mom says she has a normal cough O/E Decreased air entry LUL; hepatosplenomegaly Irritable baby, no neck stiffness or bulging fontanelle, bilateral femoral hernias and low grade fever

6
7
8 Case from dr S. Mukherjee Case 3: 7-year-old male, progressive swelling both lower limbs (pedal oedema), fatigue and occasional fever. HIVinfected on ART x 6 months. No history of TB contact. Severe pallor. No heart problem. No history of any decreased urine output or history of jaundice. Abdomen: hepatomegaly 7cm (non-tender, firm consistency, surface smooth, margins sharp) and splenomegaly of 4cm. Abdomen soft, non-tender. No ascitis. Generalized lymph-adenopathy. Mantoux TST 12mm. No AFB was isolated from the sputum or the gastric aspirate. Chest X-ray was normal. Hemoglobin of 5g/dL, WCC 7000 (N=55; L=42), LFT and renal function test was normal. U/S of abdomen - multiple intra-abdominal lymph nodes (mesenteric, para-aortic, retroperitoneal lymph nodes)
9 Answers to cases Case 1 = Hilar nodes, culture-confirmed TB Case 2 = Culture-confirmed TB. Mother cavitary TB 3+ smear positive INFECTION RISK in ward! Case 3 = A large lymph node (20mmx17mm) was compressing the IVC. Biopsy was taken from a retroperitoneal lymph node. It revealed histological features of non-hodgkin s lymphoma.
10 Conventional approach to TB diagnosis A constellation of the following: History of chronic symptoms and TB contact Clinical examination (incl. growth assessment) Tuberculin skin testing (or IGRAs?) Chest radiography Bacteriological confirmation Histology (especially EPTB) HIV testing (high prevalence areas or patients at risk) (Scoring systems and diagnostic algorithms)
11 Age-related risk Immune compromised % PTB Disseminated 10 0 <1 1to2 2to5 5to10 10to15 Age in years
12 History of symptoms of chronic disease Symptoms may overlap with other diseases, but welldefined symptoms give improved yield: - Chronic cough = unremitting cough >3 weeks - Fever = >7-14 days after excluding common causes - Weight loss or FTT = preferably documented on growth chart (RTHC) - Fatigue (tiredness) not keeping up with others In some children TB presents as an acute pneumonia; both in HIV-infected and -uninfected
 Persistent, non-remittent 1w 2w 3w 4w Duration in")
13 Symptom characteristics 1) Acute with delayed recovery 2) Recurrent Intensity of Cough 3) Persistent, non-remittent 1w 2w 3w 4w Duration in weeks
14 History of contact A close contact = living in the same household (or in frequent contact) with source case. Sputum smear-positive TB case > infectious than smear-negative source cases, but still infectious! Screen all children (especially <5 years or HIVinfected) in HH contact with PTB cases for TB Contact with source case is found in only 40-70% of cases. May be infected outside of household Often undiagnosed or other TB cases in the family - in infants, may be worthwhile to screen mother Find out about DST of adult source cases!
15 Clinical examination Pulmonary TB: No specific features on clinical examination to confirm that presenting illness is due to pulmonary TB Physical signs highly suggestive of EPTB: Gibbus, especially recent onset (spinal TB) Non-painful cervical lymphadenopathy (with/without fistula formation) Meningitis: with sub-acute onset (or not responding to AB) Pleural effusion older children Distended abdomen with ascites or abdominal masses Signs of tuberculin hypersensitivity (phlyctenular conjunctivitis, erythema nodosum, PNT) Painful joint(s)





16





17

 All other children: 10 mm Negative TST does")
18 Tuberculin skin test (TST) Useful to identify children infected with TB Mantoux TST the recommended test Read in mm induration after hours. Regarded as positive as follows: High-risk children: 5 mm (HIV-infected or severely malnourished children) All other children: 10 mm Negative TST does not rule out TB
19 Interferon-gamma release assays Based on release of IFN-γ produced by T-cells Two blood tests commercially available - T-Spot.TB (ELISPOT) - Quantiferon-TB Gold In-tube test Diagnose infection and not disease (as TST) More specific than TST not affected by BCG IGRAs possibly more sensitive than TST, but this has not been confirmed in high-burden areas Time to lab / amount of blood / cost are limitations May be specific indications for use such as young children (infants) after BCG
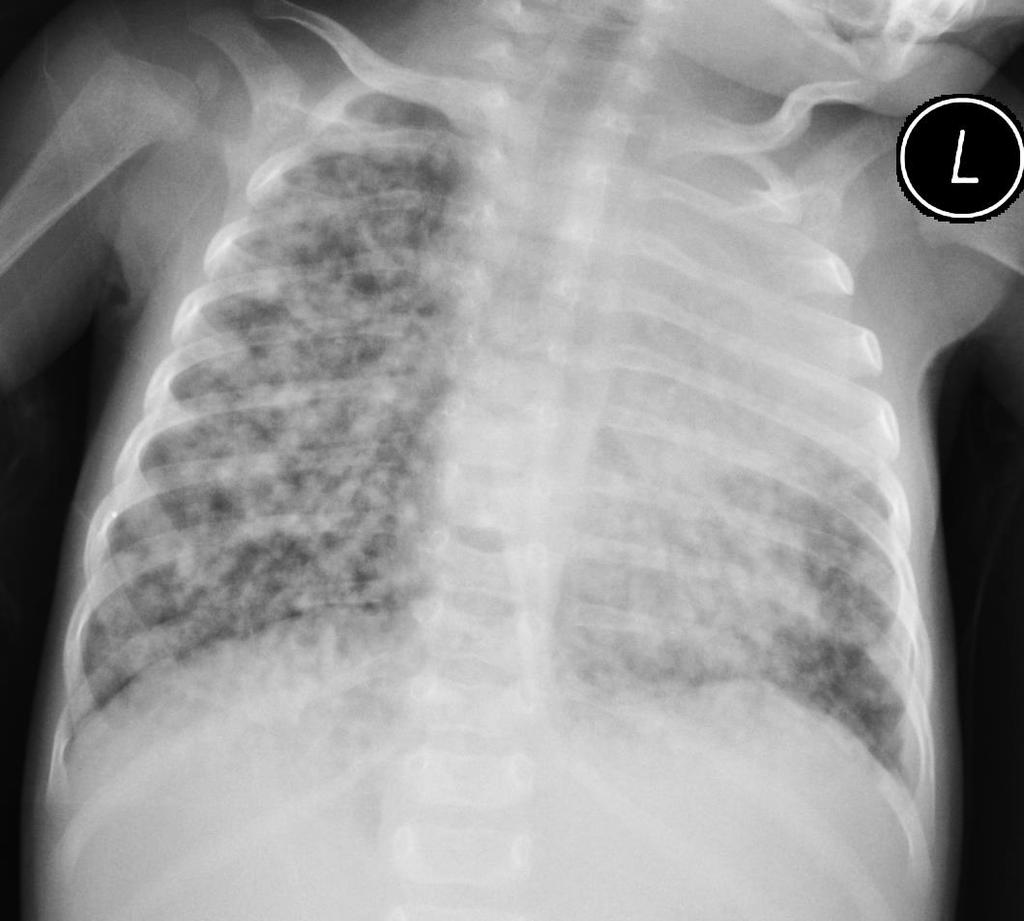
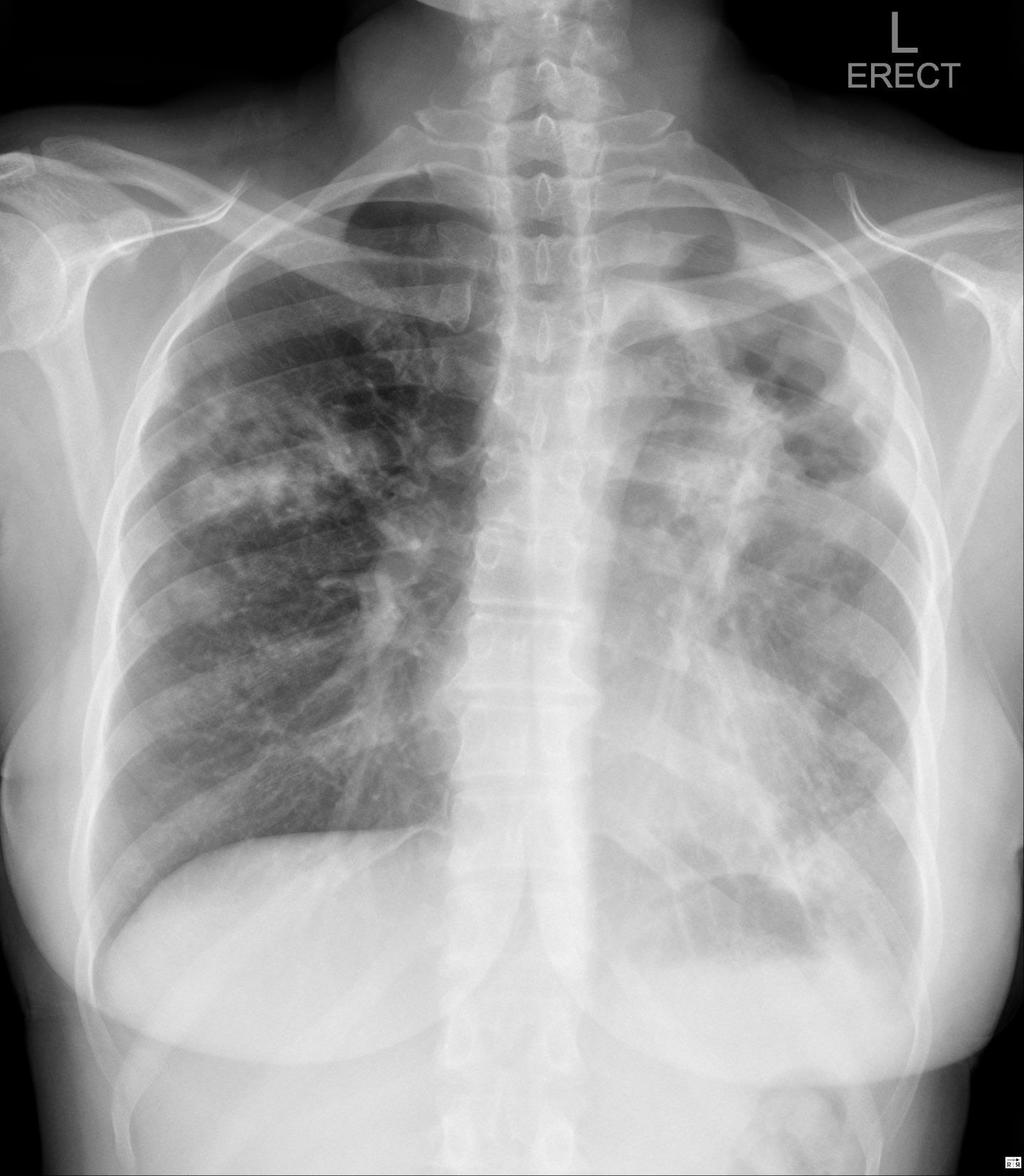
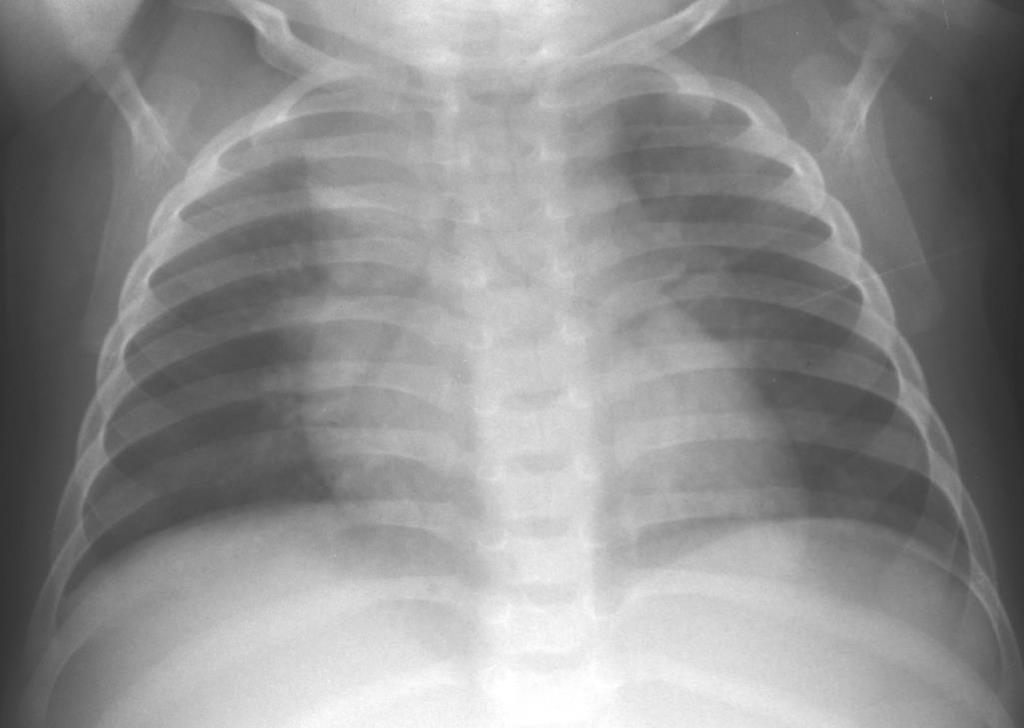
20 Chest Radiography Remains an important tool in diagnosis although: Quality of radiographs is important Chest radiographs often misread in children with TB. Intra- and inter-observer error for hilar lymphadenopathy common Suggestive pictures Enlarged hilar and/or mediastinal lymph nodes with or without (persistent) opacification in the lung Ghon focus/complex (uncommon) Miliary pattern in HIV-uninfected children Adolescents: adult type PTB or pleural effusion
21 HIV/TB: Chest Radiography Basic features the same. Often more difficult to interpret: HIV-associated lung conditions look similar to TB, e.g. bronchiectasis, recurrent pneumonias, LIP TB can occur concurrently with other diseases Reticulonodular (miliary) picture ± adenopathy could be miliary TB, LIP or other conditions Reports: (Madhi IJTLD 2000, Hesseling IJTLD 2002) more cavitation in HIV+ TB more miliary TB in HIV+ TB Most children with TB are not HIV-infected!


22 Hilar nodes / thymus?

23 Pulmonary vasculature

24

25 Subcarinal lymphnodes

26 Is this TB or lobar pneumonia?

27 Mother s CXR
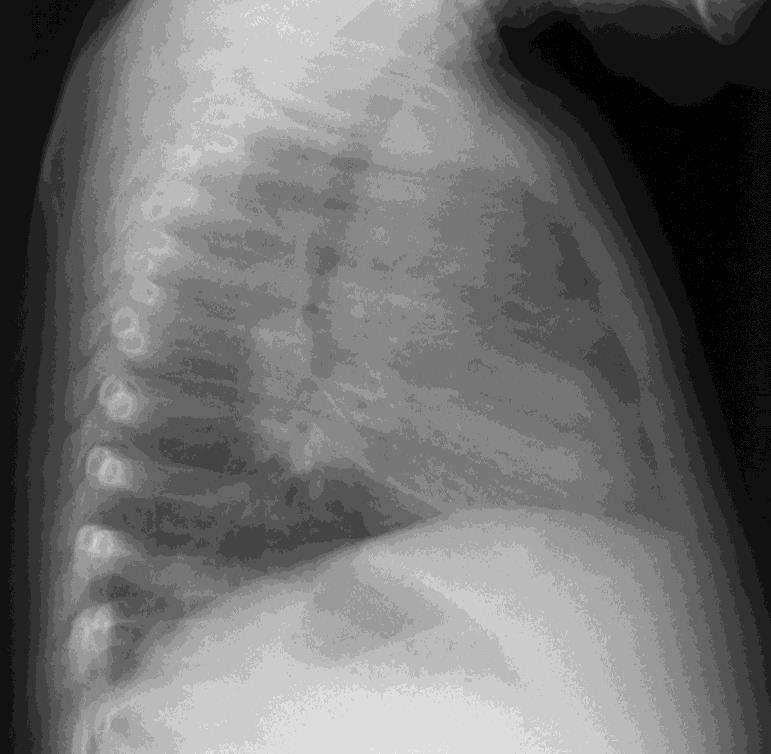
28 Other imaging (remember EPTB) Ultrasound: Abdominal TB, pleural and pericardial effusions CT scans: TBM, chest mainly MRI scans: Spinal TB, TBM Bronchoscopy: lymph nodes and its effects


29 Airways compression
30 HIV-infected vs. non-hiv-infected There are still many more HIV-uninfected children with TB than HIV-infected Treat HIV-infected children as a high-risk group (infection is as important as disease). As immune status deteriorates (lower CD4%), risk for TB increases Early HAART will reduce risk between 3-10 times, but risk remains higher than in HIVuninfected children
31 Point Scoring System Feature Score GENERAL Weeks ill < > 4 WFA > 80% 60 80% < 60% Family history Tuberculin Malnutrition Fever LOCAL None Reported Sputum + No response Positive Not improving Lymph ad. Bone / joint Abd. mass CNS sg / CSF Gibbus TOTAL
32 Scoring systems or diagnostic approaches Critical review of these approaches shows that few have been tested and sensitivity and specificity has not been calculated (A Hesseling et al. IJTLD 2002;6: ) In an area with high HIV prevalence the specifity was 25% (95% CI 16-37%) (P van Rheenen. Trop Med Int Health 2002;7:435-41) In developing countries scoring systems is all that is available stepwise approach more a screening tool than a diagnostic tool
33 Contact management algorithm Child close contact of infectious PTB case 0-59 months or HIV+ >60 months & HIV- Well Symptomatic Symptomatic Well 6H Consider TB* No treatment If becomes symptomatic If becomes symptomatic *Follow guidelines for diagnosis
34 How to investigate contacts Clinical assessment: History (Symptoms; closeness and duration of contact; drug resistance) Clinical examination Clinical assessment alone is sufficient to decide whether contact is well or symptomatic If available: TST (exposure prophylax even if TST negative) CXR (for diagnosis of disease)
35 Why do we need microbiological confirmation? The majority of child TB cases are diagnosed at primary care level without microbiological confirmation, as specimens from children are difficult to obtain and often those children have primary (paucibacillary) TB In >80% of culture-confirmed cases in hospital the diagnosis of TB was made before culture result was available If DST of adult source case is known, child contact should be treated according to adult isolate s DST result, as concordance between source case and child s isolates is between 78-90% in different studies
36 Why do we need microbiological confirmation? To confirm TB in difficult cases, e.g. uncertain lung pathology, HIV-infected children, extrapulmonary TB To determine drug susceptibility in children with unknown source cases, especially if they have poor response to first-line treatment To confirm drug resistance if a source case with DR-TB is identified in our experience 10-20% not the same DST pattern as source case, either because different source case or infected before amplification of resistance in the source case



37 Culture for M. tuberculosis Only 5-10% smear-positive yield in children Cultures positive in 30-40% of hospital-based cases; lower in community-based studies. Respiratory samples in children: Induced sputum ~ gastric aspirate NPA, tracheal aspirates or BAL FNA biopsies are useful for diagnosis of EPTB Any other body fluid/biopsy of tissue suspected of TB (e.g. CSF, bone/sinovial biopsy)

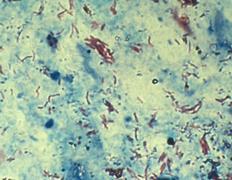
38 Robert Koch Discovered M. Tuberculosis 1882

39 GeneXpert MTB/RIF GXP PCR-based diagnosis of both M.tuberculosis complex as well as RIF resistance. Becoming more of point-of-care test and replacing sputum smear microscopy, but culture still needs to be done to confirm results and, in case of RIF resistance, to confirm MDR-TB and do second-line DST Mainly done on sputum samples, but several studies have shown its value also with other specimens, e.g. GA, FNA from lymph nodes, CSF and even stool Xpert MTB/RIF Ultra? Improved yield?





40 From LJ medium to MGIT Automated culture system
41 DST in children Culture & DST takes longer but provides best yield (30-70% in symptomatic children). Phenotypic or genotypic DST can be done, the latter providing more rapid results Xpert MTB/RIF should in children be followed by culture and DST, because children usually have smear-negative disease, and only ~60% of smear-neg, culture-pos cases will be identified. Xpert MTB/RIF also does not provide further DST results other than RIF (currently mainly sputum used) With increasing RIF-monoresistant TB cases in adults and Xpert MTB/RIFresults only, managing child contacts becomes a problem
42 Line Probe Assays Line-probe assays, a family of DNA strip-based tests that use PCR and reverse hybridization methods for the rapid detection of mutations associated with drug resistance, are available as commercial kits. Confirms M. tuberculosis complex and provides drug susceptibility test (DST) results for INH and RIF GenoType MTBDRplus INH and RIF mutations GenoType MTBDRsl second-line drugs now approved, but still need phenotypic DST Problems: Need laboratory set-up, risk of cross contamination Advantage: identifies the mutation conferring resistance to INH. This could assist with choosing the correct drugs, e.g. high-dose INH vs ethionamide

43 Line Probe Assay result
44 Conclusion of present data There is very little new data that has dramatically changed our ability to diagnose TB in children, but microbiological confirmation has become more rapid The more proof, the more certain the diagnosis Scoring systems, despite its shortcomings may still have a role to play as a screening tool in certain settings Younger children are at greater risk for complications e.g. disseminated TB and TBM, therefore treat earlier Role of culture/dst confirming diagnosis and identification & confirmation of drug resistance

45
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Algorithmic Approaches to Child TB Management in Resource-limited Settings
 Algorithmic Approaches to Child TB Management in Resource-limited Settings Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital
Algorithmic Approaches to Child TB Management in Resource-limited Settings Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS
 MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
TB in Children. The diagnostic challenge. Ralph Diedericks Red Cross Hospital
 TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
Pediatric Drug-Resistant TB in China
 Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
GUIDELINES FOR THE MANAGEMENT OF TUBERCULOSIS IN CHILDREN
 GUIDELINES FOR THE MANAGEMENT OF TUBERCULOSIS IN CHILDREN 2013 health Department: Health REPUBLIC OF SOUTH AFRICA GUIDELINES FOR THE MANAGEMENT OF TUBERCULOSIS IN CHILDREN 2013 Published by the Department
GUIDELINES FOR THE MANAGEMENT OF TUBERCULOSIS IN CHILDREN 2013 health Department: Health REPUBLIC OF SOUTH AFRICA GUIDELINES FOR THE MANAGEMENT OF TUBERCULOSIS IN CHILDREN 2013 Published by the Department
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
GENEXPERT: TOWARDS STANDARD EVALUATION OF A TB INDEX TEST IN CHILDREN
 GENEXPERT: TOWARDS STANDARD EVALUATION OF A TB INDEX TEST IN CHILDREN 29 June 2011 A collaborative NDWG Child Subgroup Protocol NIH Diagnostics Meeting Anneke C. Hesseling Desmond Tutu TB Centre Stellenbosch
GENEXPERT: TOWARDS STANDARD EVALUATION OF A TB INDEX TEST IN CHILDREN 29 June 2011 A collaborative NDWG Child Subgroup Protocol NIH Diagnostics Meeting Anneke C. Hesseling Desmond Tutu TB Centre Stellenbosch
Diagnosis of TB in Children. Dr Jacquie Narotso Oliwa
 Diagnosis of TB in Children Dr Jacquie Narotso Oliwa 1 Objectives To identify the common clinical presentations of TB in children Overview of diagnostic measures To understand a simplified approach to
Diagnosis of TB in Children Dr Jacquie Narotso Oliwa 1 Objectives To identify the common clinical presentations of TB in children Overview of diagnostic measures To understand a simplified approach to
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
The Origin of Swine Flu
 How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Introduction. Diagnosis of extrapulmonaryand paediatric tuberculosis. Extrapulmonary tuberculosis EPTB SASCM WORKSHOP 2014/05/24
 Diagnosis of extrapulmonaryand paediatric tuberculosis AW Dreyer Centre for Tuberculosis NICD Introduction Part of the global efforts to control tuberculosis (TB) include improving case detection, especially
Diagnosis of extrapulmonaryand paediatric tuberculosis AW Dreyer Centre for Tuberculosis NICD Introduction Part of the global efforts to control tuberculosis (TB) include improving case detection, especially
The SAARC Regional Programme Guidelines of Diagnosis & Management of Pediatric Tuberculosis (TB) 2017
 2017") The SAARC Regional Programme Guidelines of Diagnosis & Management of Pediatric Tuberculosis (TB) 2017 SAARC Tuberculosis and HIV/AIDS Centre (STAC) Thimi, Bhaktapur P.O.Box No.: 9517, Kathmandu, Nepal.
The SAARC Regional Programme Guidelines of Diagnosis & Management of Pediatric Tuberculosis (TB) 2017 SAARC Tuberculosis and HIV/AIDS Centre (STAC) Thimi, Bhaktapur P.O.Box No.: 9517, Kathmandu, Nepal.
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
When good genes go bad
 When good genes go bad Dr Kessendri Reddy NHLS Tygerberg Hospital Division of Clinical Microbiology Fakulteit Geneeskunde en Gesondheidswetenskappe Faculty of Medicine and Health Sciences Overview Cases
When good genes go bad Dr Kessendri Reddy NHLS Tygerberg Hospital Division of Clinical Microbiology Fakulteit Geneeskunde en Gesondheidswetenskappe Faculty of Medicine and Health Sciences Overview Cases
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
TB/HIV 2 sides of the same coin. Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai
 TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
DESK GUIDE FOR DIAGNOSIS AND MANAGEMENT OF TB IN CHILDREN
 DESK GUIDE FOR DIAGNOSIS AND MANAGEMENT OF TB IN CHILDREN Second edition, 2015 International Union Against Tuberculosis and Lung Disease (The Union) 68 Boulevard Saint-Michel, 75006 Paris, France Second
DESK GUIDE FOR DIAGNOSIS AND MANAGEMENT OF TB IN CHILDREN Second edition, 2015 International Union Against Tuberculosis and Lung Disease (The Union) 68 Boulevard Saint-Michel, 75006 Paris, France Second
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
New Standards for an Old Disease:
 New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
New Standards for an Old Disease: Practical Implications of the TB Standards TB Prevention and Control Saskatchewan September 16, 2015 Practical Implications of the TB Standards Learning Objectives At
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
TOG The Way Forward
 TOG 2016- The Way Forward Main Changes in Diagnostic algorithm Definition (Type, Classification, Outcome) Registration at the time of Diagnosis (PHI level Notification Register) Long term follow up (till
TOG 2016- The Way Forward Main Changes in Diagnostic algorithm Definition (Type, Classification, Outcome) Registration at the time of Diagnosis (PHI level Notification Register) Long term follow up (till
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis
 New approaches and the importance of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis Bahrmand.AR, Hadizadeh Tasbiti.AR, Saifi.M, Yari.SH, Karimi.A, Fateh.A, Tuberculosis Dept. Pasteur Institute
New approaches and the importance of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis Bahrmand.AR, Hadizadeh Tasbiti.AR, Saifi.M, Yari.SH, Karimi.A, Fateh.A, Tuberculosis Dept. Pasteur Institute
Prospective evaluation of World Health Organization criteria to assist diagnosis of tuberculosis in children
 Eur Respir J 99; : DOI:./99.9. Printed in UK - all rights reserved Copyright ERS Journals Ltd 99 European Respiratory Journal ISSN 9-9 Prospective evaluation of World Health Organization criteria to assist
Eur Respir J 99; : DOI:./99.9. Printed in UK - all rights reserved Copyright ERS Journals Ltd 99 European Respiratory Journal ISSN 9-9 Prospective evaluation of World Health Organization criteria to assist
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
TB Intensive San Antonio, Texas. TB/HIV Co-Infection. Lisa Armitige, MD, PhD has the following disclosures to make:
 TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB, or NOT TB? A Tough Question in Kids!
 TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
Pediatric TB Theresa Barton, MD
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Chapter 4 Diagnosis of Tuberculosis Disease
 Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
The Lancet Infectious Diseases
 Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study Susan E Dorman, Samuel G Schumacher, David Alland et al. 2017
Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study Susan E Dorman, Samuel G Schumacher, David Alland et al. 2017
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
INTENSIFIED TB CASE FINDING
 INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Global TB Burden
 Diagnosis of TB in HIV-infected persons and children: Challenges and Solutions Soumya Swaminathan, MD Coordinator, o WHO/TDR, Geneva ev Global TB Burden - 2009 9.4 million new TB cases, 1.7 million deaths
Diagnosis of TB in HIV-infected persons and children: Challenges and Solutions Soumya Swaminathan, MD Coordinator, o WHO/TDR, Geneva ev Global TB Burden - 2009 9.4 million new TB cases, 1.7 million deaths
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Tuberculosis in children: gaps and opportunities
 Tuberculosis in children: gaps and opportunities Mark Nicol Division of Medical Microbiology and Institute for Infectious Diseases and Molecular Medicine, University of Cape Town and National Health Laboratory
Tuberculosis in children: gaps and opportunities Mark Nicol Division of Medical Microbiology and Institute for Infectious Diseases and Molecular Medicine, University of Cape Town and National Health Laboratory
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
9 month old with stridor, cough, low-grade fever, mild hypoxia
 9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
Research Methods for TB Diagnostics. Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012
 Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Pulmonary TB Clinical Diagnosis
 Pulmonary TB Clinical Diagnosis Dr Onn Min Kon TB Clinics St Mary s Hospital + Hammersmith Hospital History back to basics Symptoms Ethnicity/ age Recent arrival/ travel history Contact history BCG history
Pulmonary TB Clinical Diagnosis Dr Onn Min Kon TB Clinics St Mary s Hospital + Hammersmith Hospital History back to basics Symptoms Ethnicity/ age Recent arrival/ travel history Contact history BCG history
Tuberculosis. Objectives. Tuberculosis in children is usually spead from an adult with untreated pulmonary tuberculosis.
 8 Tuberculosis Objectives When you have completed this unit you should be able to: Give reasons why tuberculosis is an important and dangerous disease. Describe primary tuberculous infection of the lung.
8 Tuberculosis Objectives When you have completed this unit you should be able to: Give reasons why tuberculosis is an important and dangerous disease. Describe primary tuberculous infection of the lung.
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Peripheral mycobacterial lymphadenitis (TB, NTM and BCG)
") Peripheral mycobacterial lymphadenitis (TB, NTM and BCG) H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Peripheral
Peripheral mycobacterial lymphadenitis (TB, NTM and BCG) H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Peripheral
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Report on WHO Policy Statements
 Report on WHO Policy Statements Christopher Gilpin TB Diagnostics and Laboratory Strengthening Unit Secretariat, Global Laboratory Initiative Stop TB Department, WHO Geneva New Diagnostics Working Group
Report on WHO Policy Statements Christopher Gilpin TB Diagnostics and Laboratory Strengthening Unit Secretariat, Global Laboratory Initiative Stop TB Department, WHO Geneva New Diagnostics Working Group
Pediatric Tuberculosis
 Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Case presentation. Dr REESAUL R
 Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
The need for new TB diagnostics in children and the way forward
 The need for new TB diagnostics in children and the way forward Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital Melbourne
The need for new TB diagnostics in children and the way forward Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital Melbourne
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
ORIGINAL ARTICLES Tuberculosis in children at Mbarara University Teaching Hospital, Uganda: diagnosis and outcome of treatment ABSTRACT Background:
 ORIGINAL ARTICLES Tuberculosis in children at Mbarara University Teaching Hospital, Uganda: diagnosis and outcome of treatment ABSTRACT Julius P. Kiwanuka 1 1 Department of Paediatrics, Mbarara University
ORIGINAL ARTICLES Tuberculosis in children at Mbarara University Teaching Hospital, Uganda: diagnosis and outcome of treatment ABSTRACT Julius P. Kiwanuka 1 1 Department of Paediatrics, Mbarara University