First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy"
|
|
|
- Shana Cooper
- 5 years ago
- Views:
Transcription
1
2 Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive degeneration of dopaminergic neurons located in the substantia nigra pars compacta (SNc)
3 Epidemiology Worldwide prevalence of PD is approximately 0.3 percent in the general population 40 years of age and older Estimates of the incidence of PD range from 8 to 18.6 per 100,000 person-years A global prevalence of 6.1 million people with PD in the year 2016
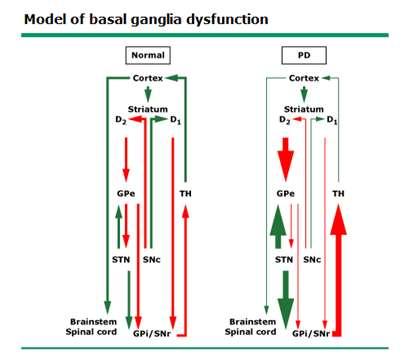
4 Pathophysiology The cortical input to the basal ganglia is excitatory, mediated by the neurotransmitter glutamate Neurons in the substantia nigra pars compacta (SNc) provide major dopaminergic input to the striatum and exert both excitatory and inhibitory influences on the striatal output neurons. The striatal output system is mediated by the inhibitory neurotransmitter gamma-aminobutyric acid (GABA).
5 The connection between the STN and the internal (medial) globus pallidus (GPi) and between STN and the lateral (or external) globus pallidus (GPe) is excitatory, mediated by glutamate.
6
7
8 Risk factors Older age and family history of PD are associated with an increased risk of developing PD Cigarette smoking is associated with a decreased risk
9 PD and Smoking There is an inverse correlation between PD and smoking A neuroprotective effect of nicotine has been proposed as one possible explanation for these observations An alternative hypothesis is that patients who develop PD are less likely to smoke in the first place, or more likely to quit smoking than those who do not develop PD. This alternative explanation posits that since dopamine is an integral component of the brain's reward system, people who will later develop signs of PD do not engage in rewardseeking behaviors, such as smoking, because dopamine is significantly depleted in the basal ganglia years before symptoms of PD appear
10 CARDINAL MANIFESTATIONS Tremor Bradykinesia Rigidity Postural instability
11 Other features Hypomimia (masked facial expression) Hypophonia Sialorrhea Micrographia Stooped posture Difficulty turning in bed Gait: Shuffling, short-stepped gait Freezing
12 Non motor manifestations Cognitive dysfunction Psychosis Mood disorders Sleep disturbances Fatigue Autonomic dysfunction Olfactory dysfunction
13 Dopamine metbolism
14 Treatment Drug therapy: L-dopa and dopa decarboxylase inbhibitor MAO B inhibitors Dopamine agonists Amantidine Anticholenergic drugs Stereotactic thalamotomy Deep brain Stimulation
15
16 Huntington disease It is an inherited progressive neurodegenerative disorder characterized by: choreiform movements, psychiatric problems, dementia. It is caused by a cytosine-adenine-guanine (CAG) trinucleotide repeat expansion in the huntingtin (HTT) gene on chromosome 4p and inherited in an autosomal-dominant pattern.
17 Huntingtin is present in a large number of tissues throughout the body. However, pathology mainly involves the central nervous system, with atrophy of the caudate and putamen (the neostriatum) being most prominent. In the early stages, Dopamine neurotransmission is increased leading to hyperkinetic movements. In contrast, in the late stages, Dopamone deficits produce hypokinesia
18 The main determinant of age of onset is the number of CAG repeats in the HTT gene. The normal number of repeats is 28 or less will not develop symptoms but the next generation is at a small risk to develop expansion are incompletely penetrant equal or greater than 40, the disease is fully penetrant and symptoms of the disease will occur.
19 CLINICAL PROGRESSION Regardless of age of onset, HD is a chronic, slowly progressive disease. The average length of survival after clinical onset ranges from 10 to 20 years, and some affected individuals live for 30 to 40 years
20 Anticipation Expansion of the repeat number between successive generations, which causes an earlier and more severe phenotype
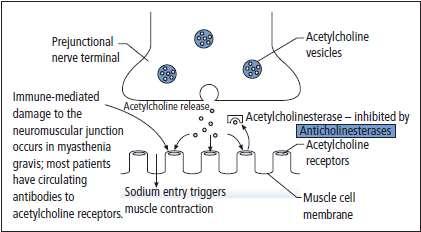
21 Myasthenia Gravis Myasthenia gravis is an acquired autoimmune disorder of the neuromuscular junction characterized by weakness and fatigability of skeletal muscles It is the most common disorder of neuromuscular transmission.
22
23 AChR antibodies cause dysfunction at the neuromuscular junction by blocking ACh binding to the AChR, cross-linking and internalizing AChRs, and activating complement-mediated AChR destruction.
24 The thymus and the origin of autoimmunity The majority of patients with AChR antibody-positive myasthenia gravis have thymic abnormalities: hyperplasia in 60 to 70 percent thymoma in 10 to 12 percent. Furthermore, the disease often improves or disappears after thymectomy
25 The thymus contains a small number of "myoid" cells. These cells are distinguished by striations and the presence of AChR on their surface and are the only known cells to express intact AChR outside of muscle.
26 Clinical manifestations: The cardinal feature of myasthenia gravis is fluctuating skeletal muscle weakness, often with true muscle fatigue. The fatigue is manifest by worsening contractile force of the muscle, not a sensation of tiredness The weakness may fluctuate throughout the day, but it is most commonly worse later in the day or evening, or after exercise
27 There are two clinical forms of myasthenia gravis: Ocular myasthenia: the weakness is limited to the eyelids and extraocular muscles. Generalized disease: the weakness commonly affects ocular muscles, but it also involves a variable combination of bulbar, limb, and respiratory muscles.
28 Ocular symptoms: Weakness of the eyelid muscles can lead to ptosis Weakness of extraocular muscles produces binocular diplopia that disappears when the patient closes or occludes one eye. Bulbar muscles : Fatigable chewing Dysarthria and dysphagia Nasal speech Facial muscles Patient appear expressionless.
29 Neck and limb muscles Neck extensor and flexor muscles are commonly affected. Involvement of the limbs in myasthenia produces predominantly proximal weakness similar to other muscle diseases. Respiratory muscles Involvement of the muscles of respiration produces the most serious symptoms in myasthenia gravis. Respiratory muscle weakness that leads to respiratory insufficiency and pending respiratory failure is a lifethreatening situation called "myasthenic crisis."
30 There are four basic therapies used to treat myasthenia gravis (MG): Smptomatic treatments (anticholinesterase agents) Chronic immunomodulating treatments (glucocorticoids and other immunosuppressive drugs) Rapid immunomodulating treatments (plasmapheresis and intravenous immune globulin) Surgical treatment (thymectomy)
31 Alzheimer disease AD is the most common cause of dementia in all age groups, occurring with markedly increased frequency in the elderly. It is a neurodegenerative disorder characterized pathologically by intracellular neurofibrillary tangles composed of paired helical filaments, and extracellular neuritic plaques containing an amyloid core, along with neuronal loss
32 The cholinergic system is involved in critical physiological processes, such as attention, learning, memory, stress response, wakefulness and sleep, and sensory information Cholinergic neurones are particularly affected in AD, providing a rationale for the use of cholinergic-enhancing drugs to improve memory in this disease. The concentration of ammo acid transmitters, particularly of glutamate, is also reduced in cortical and subcortical areas
33 Risk factors Age Family history Hypertension Dyslipidemia Cerebrovascular disease Peripheral atherosclerosis Type 2 diabetes and obesity Lifestyle and activity
34 Clinical features Early in the course of the illness, memory loss is apparent, particularly for recent events. Patients have difficulty learning and retaining new information. Later, the impairment of memory, along with attention deficits, leads to disorientation in time. There are word-finding difficulties and loss of general knowledge. Finally, there is severe global loss of cognitive function: amnesia, dysphasia, dyspraxia and agnosia. Death within 5 10 years.
35 Other symptoms Apraxia Dyspraxia, or difficulty performing learned motor tasks Olfactory dysfunction Sleep disturbances Seizures Motor signs
36 Treatment Various cholinergic-enhancing drugs have been used to improve memory early in the disease, albeit for only a few months, most notably the cholinesterase inhibitors Memantine affects glutamate transmission and is licensed for use in moderate to severe AD
37 Thank you
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
A. General features of the basal ganglia, one of our 3 major motor control centers:
 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. March 1, 2012 THE BASAL GANGLIA Objectives: 1. What are the main
Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. March 1, 2012 THE BASAL GANGLIA Objectives: 1. What are the main
A. General features of the basal ganglia, one of our 3 major motor control centers:
 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. April 22, 2010 THE BASAL GANGLIA Objectives: 1. What are the
Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. April 22, 2010 THE BASAL GANGLIA Objectives: 1. What are the
Basal Ganglia. Steven McLoon Department of Neuroscience University of Minnesota
 Basal Ganglia Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Graduate School Discussion Wednesday, Nov 1, 11:00am MoosT 2-690 with Paul Mermelstein (invite your friends)
Basal Ganglia Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Graduate School Discussion Wednesday, Nov 1, 11:00am MoosT 2-690 with Paul Mermelstein (invite your friends)
Basal ganglia Sujata Sofat, class of 2009
 Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Cheyenne 11/28 Neurological Disorders II. Transmissible Spongiform Encephalopathy
 Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Damage on one side.. (Notes) Just remember: Unilateral damage to basal ganglia causes contralateral symptoms.
 Just remember: Unilateral damage to basal ganglia causes contralateral symptoms.") Lecture 20 - Basal Ganglia Basal Ganglia (Nolte 5 th Ed pp 464) Damage to the basal ganglia produces involuntary movements. Although the basal ganglia do not influence LMN directly (to cause this involuntary
Lecture 20 - Basal Ganglia Basal Ganglia (Nolte 5 th Ed pp 464) Damage to the basal ganglia produces involuntary movements. Although the basal ganglia do not influence LMN directly (to cause this involuntary
Myasthenia Gravis. Mike Gilchrist 10/30/06
 Myasthenia Gravis Mike Gilchrist 10/30/06 Overview Background Pathogenesis Clinical Manifestations Diagnosis Treatment Associated Conditions Background Severe muscle disease Most common disorder of neuromuscular
Myasthenia Gravis Mike Gilchrist 10/30/06 Overview Background Pathogenesis Clinical Manifestations Diagnosis Treatment Associated Conditions Background Severe muscle disease Most common disorder of neuromuscular
Basal Ganglia George R. Leichnetz, Ph.D.
 Basal Ganglia George R. Leichnetz, Ph.D. OBJECTIVES 1. To understand the brain structures which constitute the basal ganglia, and their interconnections 2. To understand the consequences (clinical manifestations)
Basal Ganglia George R. Leichnetz, Ph.D. OBJECTIVES 1. To understand the brain structures which constitute the basal ganglia, and their interconnections 2. To understand the consequences (clinical manifestations)
Visualization and simulated animations of pathology and symptoms of Parkinson s disease
 Visualization and simulated animations of pathology and symptoms of Parkinson s disease Prof. Yifan HAN Email: bctycan@ust.hk 1. Introduction 2. Biochemistry of Parkinson s disease 3. Course Design 4.
Visualization and simulated animations of pathology and symptoms of Parkinson s disease Prof. Yifan HAN Email: bctycan@ust.hk 1. Introduction 2. Biochemistry of Parkinson s disease 3. Course Design 4.
The motor regulator. 1) Basal ganglia/nucleus
 Basal ganglia/nucleus") The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
Anatomy of the basal ganglia. Dana Cohen Gonda Brain Research Center, room 410
 Anatomy of the basal ganglia Dana Cohen Gonda Brain Research Center, room 410 danacoh@gmail.com The basal ganglia The nuclei form a small minority of the brain s neuronal population. Little is known about
Anatomy of the basal ganglia Dana Cohen Gonda Brain Research Center, room 410 danacoh@gmail.com The basal ganglia The nuclei form a small minority of the brain s neuronal population. Little is known about
Making Things Happen 2: Motor Disorders
 Making Things Happen 2: Motor Disorders How Your Brain Works Prof. Jan Schnupp wschnupp@cityu.edu.hk HowYourBrainWorks.net On the Menu in This Lecture In the previous lecture we saw how motor cortex and
Making Things Happen 2: Motor Disorders How Your Brain Works Prof. Jan Schnupp wschnupp@cityu.edu.hk HowYourBrainWorks.net On the Menu in This Lecture In the previous lecture we saw how motor cortex and
COGNITIVE SCIENCE 107A. Motor Systems: Basal Ganglia. Jaime A. Pineda, Ph.D.
 COGNITIVE SCIENCE 107A Motor Systems: Basal Ganglia Jaime A. Pineda, Ph.D. Two major descending s Pyramidal vs. extrapyramidal Motor cortex Pyramidal system Pathway for voluntary movement Most fibers originate
COGNITIVE SCIENCE 107A Motor Systems: Basal Ganglia Jaime A. Pineda, Ph.D. Two major descending s Pyramidal vs. extrapyramidal Motor cortex Pyramidal system Pathway for voluntary movement Most fibers originate
Chapter 8. Control of movement
 Chapter 8 Control of movement 1st Type: Skeletal Muscle Skeletal Muscle: Ones that moves us Muscles contract, limb flex Flexion: a movement of a limb that tends to bend its joints, contraction of a flexor
Chapter 8 Control of movement 1st Type: Skeletal Muscle Skeletal Muscle: Ones that moves us Muscles contract, limb flex Flexion: a movement of a limb that tends to bend its joints, contraction of a flexor
MYASTHENIA GRAVIS. Mr. D.Raju, M.pharm, Lecturer
 MYASTHENIA GRAVIS Mr. D.Raju, M.pharm, Lecturer OUTLINE Background Anatomy Pathophysiology Clinical Presentation Treatment BACKGROUND Acquired autoimmune disorder Clinically characterized by: Weakness
MYASTHENIA GRAVIS Mr. D.Raju, M.pharm, Lecturer OUTLINE Background Anatomy Pathophysiology Clinical Presentation Treatment BACKGROUND Acquired autoimmune disorder Clinically characterized by: Weakness
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
GBME graduate course. Chapter 43. The Basal Ganglia
 GBME graduate course Chapter 43. The Basal Ganglia Basal ganglia in history Parkinson s disease Huntington s disease Parkinson s disease 1817 Parkinson's disease (PD) is a degenerative disorder of the
GBME graduate course Chapter 43. The Basal Ganglia Basal ganglia in history Parkinson s disease Huntington s disease Parkinson s disease 1817 Parkinson's disease (PD) is a degenerative disorder of the
Dr. Farah Nabil Abbas. MBChB, MSc, PhD
 Dr. Farah Nabil Abbas MBChB, MSc, PhD The Basal Ganglia *Functions in association with motor cortex and corticospinal pathways. *Regarded as accessory motor system besides cerebellum. *Receive most of
Dr. Farah Nabil Abbas MBChB, MSc, PhD The Basal Ganglia *Functions in association with motor cortex and corticospinal pathways. *Regarded as accessory motor system besides cerebellum. *Receive most of
Basal Ganglia General Info
 Basal Ganglia General Info Neural clusters in peripheral nervous system are ganglia. In the central nervous system, they are called nuclei. Should be called Basal Nuclei but usually called Basal Ganglia.
Basal Ganglia General Info Neural clusters in peripheral nervous system are ganglia. In the central nervous system, they are called nuclei. Should be called Basal Nuclei but usually called Basal Ganglia.
UNDERSTANDING PARKINSON S DISEASE
 UNDERSTANDING PARKINSON S DISEASE WHAT IS PARKINSON S DISEASE? A progressive disease of the nervous system marked by tremor, muscular rigidity, and slow, imprecise movement, chiefly affecting middleaged
UNDERSTANDING PARKINSON S DISEASE WHAT IS PARKINSON S DISEASE? A progressive disease of the nervous system marked by tremor, muscular rigidity, and slow, imprecise movement, chiefly affecting middleaged
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
MOVEMENT OUTLINE. The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement
 MOVEMENT 2 Dr. Steinmetz 3 OUTLINE The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement Parkinson s Disease Huntington s Disease 1 4 TYPES
MOVEMENT 2 Dr. Steinmetz 3 OUTLINE The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement Parkinson s Disease Huntington s Disease 1 4 TYPES
Kinematic Modeling in Parkinson s Disease
 Kinematic Modeling in Parkinson s Disease Alexander Hui Department of Bioengineering University of California, San Diego La Jolla, CA 92093 alexhui@ucsd.edu Abstract Parkinson s disease is a slowly progressing
Kinematic Modeling in Parkinson s Disease Alexander Hui Department of Bioengineering University of California, San Diego La Jolla, CA 92093 alexhui@ucsd.edu Abstract Parkinson s disease is a slowly progressing
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
DRUG TREATMENT OF PARKINSON S DISEASE. Mr. D.Raju, M.pharm, Lecturer
 DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
Connections of basal ganglia
 Connections of basal ganglia Introduction The basal ganglia, or basal nuclei, are areas of subcortical grey matter that play a prominent role in modulating movement, as well as cognitive and emotional
Connections of basal ganglia Introduction The basal ganglia, or basal nuclei, are areas of subcortical grey matter that play a prominent role in modulating movement, as well as cognitive and emotional
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Strick Lecture 4 March 29, 2006 Page 1
 Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Part 1 Parkinson s Disease. COGS 172: Brain Disorders and Cogni5on
 Part 1 Parkinson s Disease COGS 172: Brain Disorders and Cogni5on Background: Neuroanatomy of the motor system Note: Given short time to the final the details of the anatomy will not be in the exam, but
Part 1 Parkinson s Disease COGS 172: Brain Disorders and Cogni5on Background: Neuroanatomy of the motor system Note: Given short time to the final the details of the anatomy will not be in the exam, but
Lecture XIII. Brain Diseases I - Parkinsonism! Brain Diseases I!
 Lecture XIII. Brain Diseases I - Parkinsonism! Bio 3411! Wednesday!! Lecture XIII. Brain Diseases - I.! 1! Brain Diseases I! NEUROSCIENCE 5 th ed! Page!!Figure!!Feature! 408 18.9 A!!Substantia Nigra in
Lecture XIII. Brain Diseases I - Parkinsonism! Bio 3411! Wednesday!! Lecture XIII. Brain Diseases - I.! 1! Brain Diseases I! NEUROSCIENCE 5 th ed! Page!!Figure!!Feature! 408 18.9 A!!Substantia Nigra in
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
symptoms of Parkinson s disease EXCEPT.
 M. Angele Theard, M.D Asst. Professor, Washington University, St. Louis, MO Quiz team; Shobana Rajan, M.D; Suneeta Gollapudy, MD; Verghese Cherian, M.D, M. Angele Theard, MD This quiz is being published
M. Angele Theard, M.D Asst. Professor, Washington University, St. Louis, MO Quiz team; Shobana Rajan, M.D; Suneeta Gollapudy, MD; Verghese Cherian, M.D, M. Angele Theard, MD This quiz is being published
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Biological Bases of Behavior. 8: Control of Movement
 Biological Bases of Behavior 8: Control of Movement m d Skeletal Muscle Movements of our body are accomplished by contraction of the skeletal muscles Flexion: contraction of a flexor muscle draws in a
Biological Bases of Behavior 8: Control of Movement m d Skeletal Muscle Movements of our body are accomplished by contraction of the skeletal muscles Flexion: contraction of a flexor muscle draws in a
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014
 Spring, 2014") UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 11 th edition 2006 Eman Al-Khateeb,
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 11 th edition 2006 Eman Al-Khateeb,
DISORDERS OF THE MOTOR SYSTEM. Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817.
 Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817. Four (4) hallmark clinical signs: 1) Tremor: (Note -
Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817. Four (4) hallmark clinical signs: 1) Tremor: (Note -
Parts of the motor circuits
 MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
Teach-SHEET Basal Ganglia
 Teach-SHEET Basal Ganglia Purves D, et al. Neuroscience, 5 th Ed., Sinauer Associates, 2012 Common organizational principles Basic Circuits or Loops: Motor loop concerned with learned movements (scaling
Teach-SHEET Basal Ganglia Purves D, et al. Neuroscience, 5 th Ed., Sinauer Associates, 2012 Common organizational principles Basic Circuits or Loops: Motor loop concerned with learned movements (scaling
PSY 315 Lecture 11 (2/23/2011) (Motor Control) Dr. Achtman PSY 215. Lecture 11 Topic: Motor System Chapter 8, pages
 (Motor Control) Dr. Achtman PSY 215. Lecture 11 Topic: Motor System Chapter 8, pages") Corrections: No Corrections Announcements: Exam #2 next Wednesday, March 2, 2011 Monday February 28, 2011 we will be going over the somatosensory system, and there will be time left in class to review
Corrections: No Corrections Announcements: Exam #2 next Wednesday, March 2, 2011 Monday February 28, 2011 we will be going over the somatosensory system, and there will be time left in class to review
EMERGING TREATMENTS FOR PARKINSON S DISEASE
 EMERGING TREATMENTS FOR PARKINSON S DISEASE Katerina Markopoulou, MD, PhD Director Neurodegenerative Diseases Program Department of Neurology NorthShore University HealthSystem Clinical Assistant Professor
EMERGING TREATMENTS FOR PARKINSON S DISEASE Katerina Markopoulou, MD, PhD Director Neurodegenerative Diseases Program Department of Neurology NorthShore University HealthSystem Clinical Assistant Professor
8/28/2017. Behind the Scenes of Parkinson s Disease
 BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Chapter 20. Media Directory. Amyotrophic Lateral Sclerosis. Alzheimer s Disease. Huntington s Chorea. Multiple Sclerosis
 Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Classes of Neurotransmitters. Neurotransmitters
 1 Drugs Outline 2 Neurotransmitters Agonists and Antagonists Cocaine & other dopamine agonists Alcohol & its effects / Marijuana & its effects Synthetic & Designer Drugs: Ecstasy 1 Classes of Neurotransmitters
1 Drugs Outline 2 Neurotransmitters Agonists and Antagonists Cocaine & other dopamine agonists Alcohol & its effects / Marijuana & its effects Synthetic & Designer Drugs: Ecstasy 1 Classes of Neurotransmitters
Basal Ganglia. Introduction. Basal Ganglia at a Glance. Role of the BG
 Basal Ganglia Shepherd (2004) Chapter 9 Charles J. Wilson Instructor: Yoonsuck Choe; CPSC 644 Cortical Networks Introduction A set of nuclei in the forebrain and midbrain area in mammals, birds, and reptiles.
Basal Ganglia Shepherd (2004) Chapter 9 Charles J. Wilson Instructor: Yoonsuck Choe; CPSC 644 Cortical Networks Introduction A set of nuclei in the forebrain and midbrain area in mammals, birds, and reptiles.
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
CLINICAL PRESENTATION
 MYASTHENIA GRAVIS INTRODUCTION Most common primary disorder of neuromuscular transmission Usually due to acquired immunological abnormality Also due to genetic abnormalities at neuromuscular junction.
MYASTHENIA GRAVIS INTRODUCTION Most common primary disorder of neuromuscular transmission Usually due to acquired immunological abnormality Also due to genetic abnormalities at neuromuscular junction.
Subthalamic Nucleus Deep Brain Stimulation (STN-DBS)
") Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) A Neurosurgical Treatment for Parkinson s Disease Parkinson s Disease Parkinson s disease is a common neurodegenerative disorder that affects about
Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) A Neurosurgical Treatment for Parkinson s Disease Parkinson s Disease Parkinson s disease is a common neurodegenerative disorder that affects about
A Parkinson s Disease and related disorders
 A 3.5.2 Parkinson s Disease and related disorders 10 November 2016 Marinela Vavla marinela.vavla@kcl.ac.uk Learning objectives Basal ganglia: components and localization (inter)connections and functions
A 3.5.2 Parkinson s Disease and related disorders 10 November 2016 Marinela Vavla marinela.vavla@kcl.ac.uk Learning objectives Basal ganglia: components and localization (inter)connections and functions
Diseases of Muscle and Neuromuscular Junction
 Diseases of Muscle and Neuromuscular Junction Diseases of Muscle and Neuromuscular Junction Neuromuscular Junction Muscle Myastenia Gravis Eaton-Lambert Syndrome Toxic Infllammatory Denervation Atrophy
Diseases of Muscle and Neuromuscular Junction Diseases of Muscle and Neuromuscular Junction Neuromuscular Junction Muscle Myastenia Gravis Eaton-Lambert Syndrome Toxic Infllammatory Denervation Atrophy
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Extrapyramidal Motor System. Basal Ganglia or Striatum. Basal Ganglia or Striatum 3/3/2010
 Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Huntington s Disease COGS 172
 Huntington s Disease COGS 172 Overview Part I: What is HD? - Clinical description and features - Genetic basis and neuropathology - Cell biology, mouse models and therapeutics Part II: HD as a model in
Huntington s Disease COGS 172 Overview Part I: What is HD? - Clinical description and features - Genetic basis and neuropathology - Cell biology, mouse models and therapeutics Part II: HD as a model in
Exam 2 PSYC Fall (2 points) Match a brain structure that is located closest to the following portions of the ventricular system
 Match a brain structure that is located closest to the following portions of the ventricular system") Exam 2 PSYC 2022 Fall 1998 (2 points) What 2 nuclei are collectively called the striatum? (2 points) Match a brain structure that is located closest to the following portions of the ventricular system
Exam 2 PSYC 2022 Fall 1998 (2 points) What 2 nuclei are collectively called the striatum? (2 points) Match a brain structure that is located closest to the following portions of the ventricular system
Study Guide Unit 2 Psych 2022, Fall 2003
 Study Guide Unit 2 Psych 2022, Fall 2003 Subcortical Anatomy 1. Be able to locate the following structures and be able to indicate whether they are located in the forebrain, diencephalon, midbrain, pons,
Study Guide Unit 2 Psych 2022, Fall 2003 Subcortical Anatomy 1. Be able to locate the following structures and be able to indicate whether they are located in the forebrain, diencephalon, midbrain, pons,
Basal Ganglia. Today s lecture is about Basal Ganglia and it covers:
 Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Impact of the Secretome of Human Mesenchymal Stem Cells on Brain Structure and Animal Behavior in a Rat Model of Parkinson s Disease
 Impact of the Secretome of Human Mesenchymal Stem Cells on Brain Structure and Animal Behavior in a Rat Model of Parkinson s Disease FABIO G. TEIXEIRA,MIGUEL M.CARVALHO KRISHNA M. PANCHALINGAM ANA J.RODRIGUES
Impact of the Secretome of Human Mesenchymal Stem Cells on Brain Structure and Animal Behavior in a Rat Model of Parkinson s Disease FABIO G. TEIXEIRA,MIGUEL M.CARVALHO KRISHNA M. PANCHALINGAM ANA J.RODRIGUES
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Chapter 8. Parkinsonism. M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University.
 Chapter 8 Parkinsonism M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University. Definition of Parkinson s Disease Parkinson's disease is a progressive, neurodegenerative disease
Chapter 8 Parkinsonism M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM University. Definition of Parkinson s Disease Parkinson's disease is a progressive, neurodegenerative disease
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
Neuroscience 410 Huntington Disease - Clinical. March 18, 2008
 Neuroscience 410 March 20, 2007 W. R. Wayne Martin, MD, FRCPC Division of Neurology University of Alberta inherited neurodegenerative disorder autosomal dominant 100% penetrance age of onset: 35-45 yr
Neuroscience 410 March 20, 2007 W. R. Wayne Martin, MD, FRCPC Division of Neurology University of Alberta inherited neurodegenerative disorder autosomal dominant 100% penetrance age of onset: 35-45 yr
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
How to Effectively Manage the Motor Symptoms of HD
 How to Effectively Manage the Motor Symptoms of HD Yvette Bordelon, MD, PhD Associate Clinical Professor of Neurology David Geffen School of Medicine at UCLA The information provided by speakers in workshops,
How to Effectively Manage the Motor Symptoms of HD Yvette Bordelon, MD, PhD Associate Clinical Professor of Neurology David Geffen School of Medicine at UCLA The information provided by speakers in workshops,
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz. Parkinson s Disease. A Guide to Medical Treatment
 M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Disorders of the Nervous System. Disorders of the Neurological System. General Endpoints of CNS Disease. General Endpoints of CNS Disease
 HD in Nursing-Pathophysiology Disorders of the Nervous System What are some disorders of the nervous system? Disorders of the Neurological System Dr. C.H. Lai The nervous system is vulnerable to various
HD in Nursing-Pathophysiology Disorders of the Nervous System What are some disorders of the nervous system? Disorders of the Neurological System Dr. C.H. Lai The nervous system is vulnerable to various
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology
 Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
STRUCTURE AND CIRCUITS OF THE BASAL GANGLIA
 STRUCTURE AND CIRCUITS OF THE BASAL GANGLIA Rastislav Druga Department of Anatomy, Second Faculty of Medicine 2017 Basal ganglia Nucleus caudatus, putamen, globus pallidus (medialis et lateralis), ncl.
STRUCTURE AND CIRCUITS OF THE BASAL GANGLIA Rastislav Druga Department of Anatomy, Second Faculty of Medicine 2017 Basal ganglia Nucleus caudatus, putamen, globus pallidus (medialis et lateralis), ncl.
Deep Brain Stimulation: Indications and Ethical Applications
 Deep Brain Stimulation Overview Kara D. Beasley, DO, MBe, FACOS Boulder Neurosurgical and Spine Associates (303) 562-1372 Deep Brain Stimulation: Indications and Ethical Applications Instrument of Change
Deep Brain Stimulation Overview Kara D. Beasley, DO, MBe, FACOS Boulder Neurosurgical and Spine Associates (303) 562-1372 Deep Brain Stimulation: Indications and Ethical Applications Instrument of Change
Case Study 2: Neurological Degenerative Disease FDA Regulatory and Clinical Background
 Case Study 2: Neurological Degenerative Disease FDA Regulatory and Clinical Background Heather Benz, Ph.D. FDA Center for Devices and Radiological Health Neurological Degenerative Diseases Neurodegenerative
Case Study 2: Neurological Degenerative Disease FDA Regulatory and Clinical Background Heather Benz, Ph.D. FDA Center for Devices and Radiological Health Neurological Degenerative Diseases Neurodegenerative
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinson's Disease. Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology
 Parkinson's Disease Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology 18 February 2002 Parkinson Disease Neurological disease affecting over four million patients
Parkinson's Disease Robert L. Copeland, Ph.D. Howard University College of Medicine Department of Pharmacology 18 February 2002 Parkinson Disease Neurological disease affecting over four million patients
Palladotomy and Pallidal Deep Brain Stimulation
 Palladotomy and Pallidal Deep Brain Stimulation Parkinson s disease Parkinson s Disease is a common neurodegenerative disorder that affects about 1:100 individuals over the age of 60. In a small percentage
Palladotomy and Pallidal Deep Brain Stimulation Parkinson s disease Parkinson s Disease is a common neurodegenerative disorder that affects about 1:100 individuals over the age of 60. In a small percentage
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Deep Brain Stimulation Surgery for Parkinson s Disease
 Deep Brain Stimulation Surgery for Parkinson s Disease Demystifying Medicine 24 January 2012 Kareem A. Zaghloul, MD, PhD Staff Physician, Surgical Neurology Branch NINDS Surgery for Parkinson s Disease
Deep Brain Stimulation Surgery for Parkinson s Disease Demystifying Medicine 24 January 2012 Kareem A. Zaghloul, MD, PhD Staff Physician, Surgical Neurology Branch NINDS Surgery for Parkinson s Disease
Making Every Little Bit Count: Parkinson s Disease. SHP Neurobiology of Development and Disease
 Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Dystonia: Title. A real pain in the neck. in All the Wrong Places
 Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Global Myasthenia Gravis Market: Size, Trends & Forecasts ( ) August 2017
 August 2017") Global Myasthenia Gravis Market: Size, Trends & Forecasts (2017-2021) August 2017 Global Myasthenia Gravis Market Scope of the Report The report titled Global Myasthenia Gravis Market: Size, Trends & Forecasts
Global Myasthenia Gravis Market: Size, Trends & Forecasts (2017-2021) August 2017 Global Myasthenia Gravis Market Scope of the Report The report titled Global Myasthenia Gravis Market: Size, Trends & Forecasts
Parkinson's Disease KP Update
 Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
WELCOME. Parkinson s 101 for the Newly Diagnosed. Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW
 WELCOME Parkinson s 101 for the Newly Diagnosed Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW Parkinson s Disease 101 Presenter for Today Cari Friedman, LCSW Patient and Family Service
WELCOME Parkinson s 101 for the Newly Diagnosed Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW Parkinson s Disease 101 Presenter for Today Cari Friedman, LCSW Patient and Family Service
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts