Man, 65 years old, heavy smoker, cough, dyspnea and weight loss. AFB negative in sputum. Is TB possible?
|
|
|
- Melanie Alexia Collins
- 6 years ago
- Views:
Transcription
1 Chapter 10

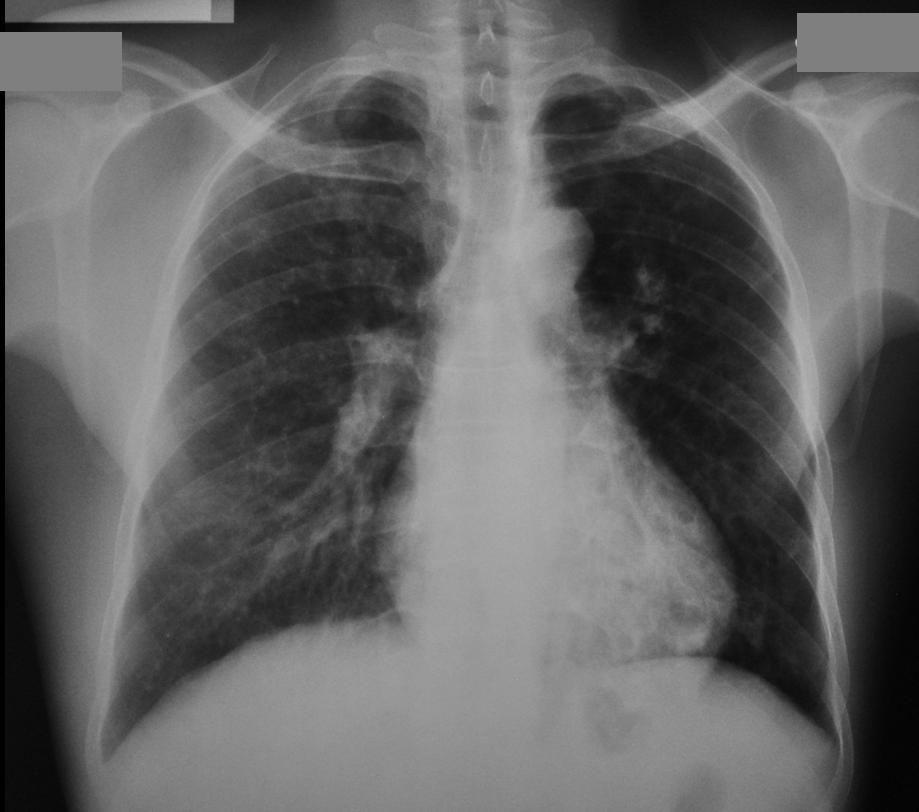
2 Man, 65 years old, heavy smoker, cough, dyspnea and weight loss. AFB negative in sputum. Is TB possible?
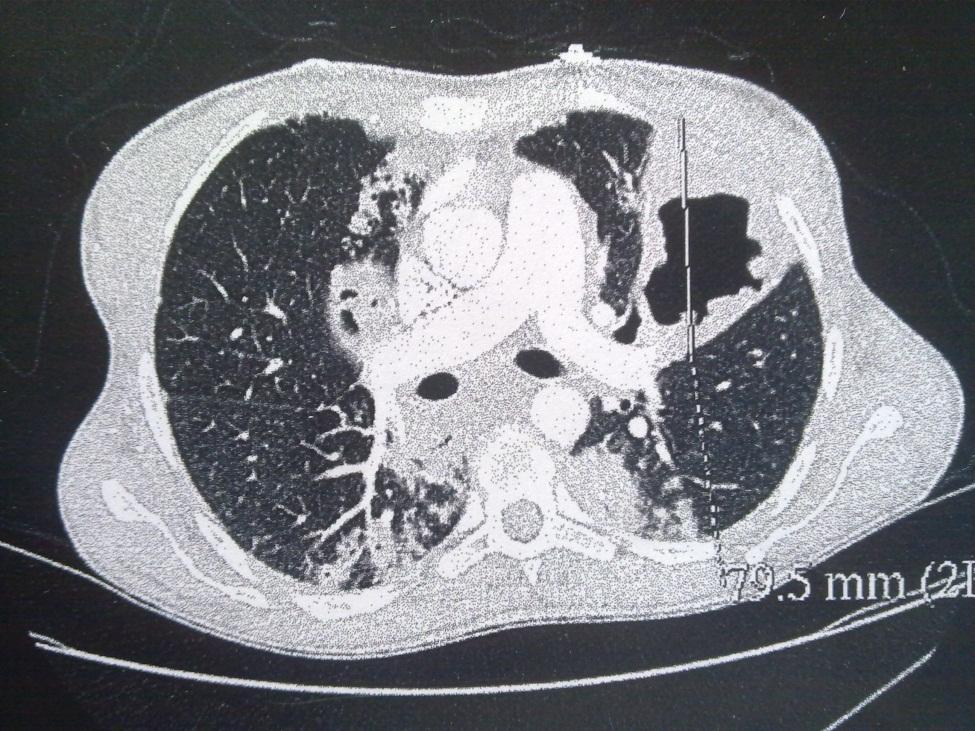
3 The opacity of the left upper lobe is not cavited and looks like a tissular mass, not alveolar picture, because of sharp limit and dense and homogenous aspect. There is a silhouette sign with aortic arch: mediastinal extension or adenopathies. The diagnosis of TB is improbable because no cavity in the opacity. It is a bronchial cancer with mediastinal adenopathies or mediastinal extension


4 Scan view of the previous case
5 2002: Young woman coming from Guinea, PLHIV (HIV2), cough and worsening condition AFB positive in sputum: Right superior lobe tuberculous pneumonia. Small left superior lobe infiltrate.



6 Radiological evolution after TB treatment : retraction and fibrosis 2009
7 June 2011: worsening condition and severe dyspnea. Producting cough: positive AFB

8 TB Recurence. 2 hypothesis: 1 endogen reinfection in case of incorrect or non complete treatment: in this case MDR TB must be suspected 2 Exogen reinfection: in this case probably no resistance to classical treatment. Specific PCR for research or resistance to anti TB drugs must be performed as soon as possible to decid adequat treatment. (genexpert)


9 Scan view of the previous case

10 Woman, 82 years old, non productive cough and chronic severe dyspnea.smear negative for AFB. Past history of lung disease but no more information.

11 Typical aspect of bilateral calcified pleural sequella, from old TB. Notice the «fishbone» aspect on the left side. No need of retreatment

12 Scan view of the previous case. Calcification of the left pleural wall.
13 Man, 80 years old, heavy smoker, right scapular pain and worsening condition
14 CXR: Right thoracic opacity with destruction of posterior arch of the 3rd 4th and 5th rib. This opacity is not a lung opacity neither pleural one : it is a parietal opacity: probable parietal extension of a bronchial cancer. In this case the diagnostic of TB is highly improbable: no cavity in this bulky opacity, rib destruction.. Notice 2 others round opacities in the inferior lobe suggesting metastasis.
15 Man, 58 years old non producting cough. Past history of pleural TB with monthes TB treatment. Crepitant rales on the right side at auscutation. No fever, chronic exercice dyspnea.
16 Non systematised opacity of the right inferior field with flatness of the diaphragm. Pleural sequella,, consequence of pleural effusion past history.. This picture is difiicult to distinguish from pneumonia. Lateral view his helpfull
17 Acute dyspnea non purulent sputum and no fever. Auscultation: bilateral crepitant rales.
18 Chest X ray: antero- posterior incidence. Bilateral alveolar pictures (notice he aeric bronchogram onthe left side). Clinical and radiological findings strongly suggest pulmonary cardiogenic oedema, even if the alveolar pictures are not symetric.
19 Woman, 54 years old, cough and anterior thoracic paint.

20 Left hilar opacity, with overlap sign. This opacity is anterior because positive silhouette sign with cardiac edge. On the lateral view the opacity fills the retro sternal clear space. Thymoma
21 Man, fever and cough for few monthes. Weight loss and recent severe hemoptisy
22 Cavity in right retractile upper lobe, associated with right latero hilar cavity, right inferior lobe infiltrate. Controlateral cavity in axillar area: TB cavities, AFB ++ in sputum


23 Woman, cough but no fever, no worsening condition. Diagnosis by radiologist and clinician: Right inferior lobe pneumonia Do you agree?
 / Do not make radiological")
24 Breast prosthesis superposition! (past history of breast cancer) / Do not make radiological diagnosis without clinical context

25 Woman, nurse, small cough. CXR considered as normal by radiologist. What do you think?
26 This CXR is not normal: see small infiltrate of the right upper lobe and, may be small cavity in the middle of the right lung

27 Same patient, 10 monthes after: infiltrate of the upper right lobe with cavern in the middle lobe.afb +++. This nurse has not been detected in time and had possibly contaminated a lot of patients
28 Case N 11 Woman, 26 years old, left thoracic pain with fever and chills.on productive cough. Quick onset of the symptoms. No past history of lung disease.
29 Chest X ray: technically perfect. Left alvolar opacity which erase cardiac silhouette on the left inferior arch, positive silhouette sign: the opacity is anterior,in the inferior part of the superior lobe (lingula segment). Clinical and radiological signs strongly suggests acute infectious pneumonia. Quick improvment with 3 g/ day of amoxicillin

30 Case N 12 Cough and hemoptisy. AFB neg. Smoking past history

31 Cavited bronchial cancer.. Thick and irregular wall. TB is possible but improbable because no bacilli in sputum, despite cavity in the opacity, and no associated nodules in the periphery of the mass
32 Case N 12 Man, 60 y, past history of TB treatment. Severe and repeted hemoptisy for many monthes.

33 Case N 12 Probable bulky aspergilloma in the left upper lobe, developped in tb sequela cavity.
34 Chapter 11
35 Case 1 Chronic productive cough and repeted infections for years Repeted smear negative

36 Left inferior lobe bronchectasis


37 Case 2 June 2010, 25 years old.nurse. As part of the recrutment examination: CXR considered as normal The radiologist has missed a small tb infiltrate in the right upper lobe


38 Case 2 3 years later: Productive cough. Smear ++++ for AFB TB cavity of the right upper lobe: very high risk of contamination in the houseold and also in the workplace
39 Case 3 Morning and chronic productive cough. Smear negative

40 Case 3 Bilateral inferior lobe bronchiectasis
.")
41 Case 4 Man 56 years old, asthenia cough and weight loss.smear -. Past history of smoking. Upper right bulky mass, with no cavitation (false picture of cavity due to rib superposition). TB is very improbable: no cavity and no associated nodules or infiltrate. Bronchial cancer.

42 Case 4 Scan view of the previous case. Confirmation of no cavity in the upper right lobe mass
43 Case 5 Fever, weight loss and cough smear (-)

44 Case 5 Right superior lobe infiltrate with right latero tracheal adenopathies: Smear negative Culture Positive: TB Cambodian National TB control program

45 Case 6 Man, 42 years old, severe dyspnea and worsening condition. Past history of nephrectomy for renal cancer The association of nodular and linear images suggests in this context a carcinomatous lymphangitis (renal origin)

46 Case 6 The association of nodular and linear and reticular pictures is much more visible on CT scan


47 Case N 7 Fever, dyspnea and headaches for 5 days Left superior lobe pneumonia. J1: beginning of treatment with amoxicillin.

48 Case N 7 J5: no improvment, Urine analysis positive for legionnella antigen. Modification of treatment with introduction of iv erythromicin

49 Case N 7 J12: signifianrt improvment with apyrexy and no more dyspnea. Residual asthenia

50 Case N 8 Man, 59 years old, hemoptisy with AFB negative in sputum. Good health condition. Past history of pulmonary tuberculosis, with a nine monthes treatment 4 years ago..
. New isolated hemoptisy.")
51 Case N 8 Same patient 2 years later (2006): possible «nodule» in the late retroclavicular area (always compar right and left for analysis of the retroclavicular area.). New isolated hemoptisy. Smear negative

52 Case N 8 Same patient, November Hemoptisy with spontaneous improvment. Smear negative. Always good health condition. Notice that the retroclavicular picture seems bigger than 2006 WHAT IS YOUR DIAGNOSIS?
 Notice on the chest X ray before surgery the enlargment of the retroclavicular opacity, inside the TB sequella cavity. Clinical and radiological evolution is highly suggesting of aspergilloma.")
53 Case N 8 Same patient, june 2009: very severe hemoptisy, life threatening situation. Improvment with IV glypressine treatment before emergency thoracic surgery surgery ( left superior lobectomy.) Notice on the chest X ray before surgery the enlargment of the retroclavicular opacity, inside the TB sequella cavity. Clinical and radiological evolution is highly suggesting of aspergilloma.

54 Case N 8 Same patient:typical aspect of aspergilloma on scannographic view



55 Case N
56 Case N 9 Men, 45 years old. Asthenia et weight loss. Nocturnal sweat and chronic cough. Smear negative

57 Case N 9 CXR: middle lobe opacity with retraction on the right side and enlargment of the mediastinum and right hilus: probable adenopathies. In this clinical context TB must be suspected.


58 Case N 9 Mediastinoscopy: positive for TB lesion. If no mediastinoscopy possible TB treatment must be nethertheless instaured on clinical and radiological argument
: regression of mediastinum enlargment and middle lobe pneumonia")
59 Case N 9 25/01/ /02/2011 Same patient after Tb treatment (right side): regression of mediastinum enlargment and middle lobe pneumonia





60 Case N 9 Before and after treatment. Notice the decrease of volume of the lymphe nodes
61 Case N 10 Cough an thoracic paint for few weeks. Smear negative CXR library for TB Diagnosis.- Cambodian National TB control program
62 Case N 10 Pleural encysted effusion. Possible pleural TB but others etiologies are possible (non tb infection..) Exploratory thoracentesis is necessary, if possible after ultrasound tracking CXR library for TB Diagnosis.- Cambodian National TB control program
63 Case N 11 Young women. Fever, weight loss and non productive cough for 2 monthes. CXR library for TB Diagnosis.- Cambodian National TB control program
64 Case N 11 Well limited opacity which does not erase aortic arch,and push the trachea. Notice also that the external limit is sharp under the clavicle and blurred over: So, this opacity is in the anterior mediastinum middle tier. The most probable diagnosis is thymoma or more probably LYMPHOMA. Tb adenopathies are less probable CXR library for TB Diagnosis.- Cambodian National TB control program
65 Case N 12 Man, 6 years old,heavy smoker. Left thoracic paint, cough, asthenia and weight loss. Smear negative


66 Case N 12 Notice the retraction and blur of the superior part of the left lung. On the profil view you see the retracted systematised opacity: lest superior lung atelectasis. In this clinical context you must suspect a bronchial cancer and, if possible propose a bronchoscopy for diagnosis confirmation
67 Chapter 12
68 Case N 1 Man, fever and cough. Mild hemoptisy. Smear negative an culture negative CXR library for TB Diagnosis.- Cambodian National TB control programman, f

69 Case N 1 Right latero tracheal adenopathy with probable hilar mass. TB is possible. But bronchial cancer with mediastinum associated adenopathies is more probable. Bronchoscopy and, if possible, TDM is required for diagnosis confirmation. CXR library for TB Diagnosis.- Cambodian National TB control programman,
70 Case N 2 Woman, acute dyspnea and non productive cough, worsening condition CXR library for TB Diagnosis.- Cambodian National TB control program

71 Case N 2 Diffuse, alveolar and interstitial pneumonia. Bacterial or viral pneumonia is possible. In case of HIV context, the most likely diagnosis is pneumocystosis CXR library for TB Diagnosis.- Cambodian National TB control program
72 Case N 3 Chronic productive cough with repeted bonchial infections CXR library for TB Diagnosis.- Cambodian National TB control program

73 Case N 3 Multiple cavities in the retro cardiac area. Probable left inferior lobe bronchiectasis CXR library for TB Diagnosis.- Cambodian National TB control program
74 Case N 4 Cough and left thoracic paint. Smear negative. TB treatment or not?

75 Case N 4 Left pleural effusion with right axillar and bilateral retro clavicular infiltrates. Mediastinum enlargment (probable adenopathies) Culture positive : Tuberculosis
76 Case N 5 Slight fever and cough. Smear negative TB treatment or not?.- Cambodian National TB control program

77 Case N 5 Right superior lobe infiltrate. Culture positive Tuberculosis.- Cambodian National TB control program

78 Case N 6 Man, 65 years old. Heavy smoker. Worsening condition and severe left shoulder and dorsal thoracic paint. Smear negative. TB treatment or not?


79 Case N 6 Left superior lobe mass with thoracic wall exrtension.: Bronchial cancer. Notice the false picture of cavity which is the consequency of rib superpositions. No need of tb treatment..
80 Case N 7 Cough fever and weight loss for 3 monthes Smear negative Do you initiate tb treatment or not?

81 Case N 7 Left superior lobar pneumonia (with aeric bronchogram) and right superior lobe infiltrate. Calcified left hilus adenopathies: The association of these different pictures strongly suggests TB. gene expert or Culture should be positive if available In this case TB treatment is mandatory because of clinical and radiological context
82 Case N 8 Man, chronic dyspnea and chronic productive cough with frequent bronchial infections. Past history of TB in house hold and TB treatment in childhood. Do you think tb retreatment is necessary or not?.-cambodian National TB control program
.")
83 Case N 8 Diffuse bronchiectasis of the left lung, which is restracted and distroyed. Typical of TB important sequella. No need of retreatment (smear and culture negative).-cambodian National TB control program
84 Case N 9 Men,57 years old, weight loss and hemoptisy. Past history of smoking. Smear negative
.")
85 Case N 9 Overlap of the left hilus by a mass. (notice that vessels are visible through the mass. It is an anterior overlap, because the mass is in contact with heart: (positive silhouette sign). Notice that left lung is slightly retracted with attraction of the trachea and ascension of the left diaphragm Final diagnosis is bronchial cancer with partial left superior lobe atelectasis
86 Case N 10 Woman78 years old, past history of hypertension, increasing dyspnea, with cough. Smear negative

87 Case N 10 Notice cardiac enlargment, blur and enlargment of the hili with vascular convergence : probable cardiac failure on the begining.

88 Spontaneous evolution: severe dyspnea with hypoxemia, bilateral crepitant rales: CXR bilateral alveolar patern acute pulmonary oedema
89 Case N 11 Woman, 37 years old.chronic cough with,sometimes hemoptoïc sputum. Repeted bronchial infections. Repeted smear negative for AFB

90 Case N 11 Right inferior lobe bronchiectasis. Look at the magnified view in the following slide

91 Typical rail pictures highly suggestive of cylindric bronchiectasis
92 Case N 12 Woman, 54 years old, bad clinical condition, weight loss, cough. Sputum negative for AFB.

93 Case N 12 Mediastinum elargment highly indicative of adenopathies, with macronodules, left side predominant, and probable partial right inferior lobe atelectasis. This radiological features highly suggest neoplasic process with pulmonary and node dissemination. Primitive tumor could be pulmonary, or extra pulmonary.
Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum.
 Chapter 7 Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum. Auscultation: crepitant bilateral rales. Chest Xray: cardiomegaly
Chapter 7 Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum. Auscultation: crepitant bilateral rales. Chest Xray: cardiomegaly
Case N 1. Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds. Courtesy Dr Van den Homberg-Tanzania
 Case N 1 Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds Courtesy Dr Van den Homberg-Tanzania Case N 1 Enlargment of cardiac silhouette. Notice the symetry
Case N 1 Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds Courtesy Dr Van den Homberg-Tanzania Case N 1 Enlargment of cardiac silhouette. Notice the symetry
Case N 1. Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available. Courtesy Dr Van Den Homberg
 Case N 1 Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available Courtesy Dr Van Den Homberg Case N 1 CXR: Right abundant pleural effusion. Notice the typical concave aspect of the superior
Case N 1 Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available Courtesy Dr Van Den Homberg Case N 1 CXR: Right abundant pleural effusion. Notice the typical concave aspect of the superior
Pulmonary TB aspects
 Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
I particularly want to thank: -Pr Pierre L Her who has been my nearest partner in this adventure which began in Cambodia many years ago.
 Introduction and advices for users: CXR interpretation in TB/HIV high burden settings Clinical and radiological cases for training to positive and differential diagnosis Here are collected 144 clinical
Introduction and advices for users: CXR interpretation in TB/HIV high burden settings Clinical and radiological cases for training to positive and differential diagnosis Here are collected 144 clinical
Key messages. CXR interpretation in TB/HIV setting. Training course
 Key messages CXR interpretation in TB/HIV setting Training course Normal CXR Front view and lateral view Good notions of technical conditions to obtain a good CXR Good knowledge of criteria for quality
Key messages CXR interpretation in TB/HIV setting Training course Normal CXR Front view and lateral view Good notions of technical conditions to obtain a good CXR Good knowledge of criteria for quality
Interstitial syndrome
 Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Radiological syndroms. Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome
 Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images
 Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Pleural syndrome. Tubercular pleurisy
 Pleural syndrome. Tubercular pleurisy Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Pleurisy: Findings of fluid between visceral
Pleural syndrome. Tubercular pleurisy Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Pleurisy: Findings of fluid between visceral
Pleural syndrome Tuberculous pleurisy
 Pleural syndrome Tuberculous pleurisy Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Pleural effusion: Findings of fluid between
Pleural syndrome Tuberculous pleurisy Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Pleural effusion: Findings of fluid between
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Alveolar condensation syndrome
 Alveolar condensation syndrome Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Lobule: morphological unit. Dimension: 10 to
Alveolar condensation syndrome Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Lobule: morphological unit. Dimension: 10 to
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
and localized ground glass opacities, or bronchiolar focal or multifocal micronodules;
 E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!!
 The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CARDIO-VASCULAR SYNDROME
 CARDIO-VASCULAR SYNDROME Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) OFCP Right pulmonary artery Left pulmonary artery
CARDIO-VASCULAR SYNDROME Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) OFCP Right pulmonary artery Left pulmonary artery
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Cardio-vascular syndrome. Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
 Cardio-vascular syndrome Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Left pulmonary artery Right pulmonary artery OFCP Left
Cardio-vascular syndrome Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Left pulmonary artery Right pulmonary artery OFCP Left
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai
 Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai Lecture 16 Radiology in diagnosis of Tuberculosis Session 01 So, welcome to the session Radiology in
Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai Lecture 16 Radiology in diagnosis of Tuberculosis Session 01 So, welcome to the session Radiology in
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Radiological Anatomy of Thorax. Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem
 Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Introduction to Radiology for TB Nurses
 Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Complicated echinococcal cyst to Biopsy or not to biopsy. V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center
 Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Radiological Features of Mycobacterium tuberculosis TUBERCULE BACILLUS TUBERCULE BACILLUS DIAGNOSIS. Guy Richards. PATHOGENESIS of TUBERCULOSIS
 Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
THE EARLY DIAGNOSIS OF PULMONARY TUBERCULOSIS
 THE EARLY DIAGNOSIS OF PULMONARY TUBERCULOSIS AM Edwards Lecture Rocky Mountain/ACP Internal Medicine Meeting Banff Park Lodge Banff, AB November 25, 2011 Declaration of Conflict of Interest (This is a
THE EARLY DIAGNOSIS OF PULMONARY TUBERCULOSIS AM Edwards Lecture Rocky Mountain/ACP Internal Medicine Meeting Banff Park Lodge Banff, AB November 25, 2011 Declaration of Conflict of Interest (This is a
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
Right infrahilar nodule
 Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary
 January 28, 2009 Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary Kristina Mirabeau-Beale, Harvard Medical School Year III Gillian Lieberman, MD Agenda Introduce Patient RS Discuss
January 28, 2009 Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary Kristina Mirabeau-Beale, Harvard Medical School Year III Gillian Lieberman, MD Agenda Introduce Patient RS Discuss
100 Chest X Rays for Study Group. by Dr. Suneet Khurana
 100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
1/13/2014. Proper Radiographs. Proper Radiographs. A Review of Pulmonary Patterns
 Live Webinar A Review of Pulmonary Patterns Sofija R. Liles, DVM, DACVR Proper Radiographs Which views? One lateral plus ventrodorsal (at least) Left lateral is best for thorax Three views for full metastatic
Live Webinar A Review of Pulmonary Patterns Sofija R. Liles, DVM, DACVR Proper Radiographs Which views? One lateral plus ventrodorsal (at least) Left lateral is best for thorax Three views for full metastatic
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC
 Interpretation Brent Burbridge, MD, FRCPC") Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Objectives. What is a Chest X Ray? CXR Workshop. Definition (diagnostic tool/internal PE) Types. Cost
 Types. Cost") Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Interactive Lecture. Lecture 7 - Interactive. Radiology of cardiorespiratory disease. Editing File. Done By. Color Coding Important Notes Extra
 Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
Signs in Chest Radiology
 Signs in Chest Radiology Jonathan H. Chung, MD Disclosures No pertinent disclosures Jonathan H. Chung, MD Assistant Professor Institute t of fadvanced d Biomedical Imaging National Jewish Health Denver,
Signs in Chest Radiology Jonathan H. Chung, MD Disclosures No pertinent disclosures Jonathan H. Chung, MD Assistant Professor Institute t of fadvanced d Biomedical Imaging National Jewish Health Denver,
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
X-rays. Dr Will Dooley
 X-rays Dr Will Dooley Plan Chest X-Rays Abdominal X-Rays Exam approach Presentation skills EMQ EMQ- answers Chest X-Ray - Systematic Approach D R Details RIP Image Quality +/- OBVIOUS ABNORMALITY A B C
X-rays Dr Will Dooley Plan Chest X-Rays Abdominal X-Rays Exam approach Presentation skills EMQ EMQ- answers Chest X-Ray - Systematic Approach D R Details RIP Image Quality +/- OBVIOUS ABNORMALITY A B C
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients
 Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients") Cronicon OPEN ACCESS EC BACTERIOLOGY AND VIROLOGY Research Article Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients Ehsan Shahverdi 1 *, Ashkan
Cronicon OPEN ACCESS EC BACTERIOLOGY AND VIROLOGY Research Article Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients Ehsan Shahverdi 1 *, Ashkan
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Role of imaging (images) in my practice. Dr P Senthur Nambi Consultant Infectious Diseases
 in my practice. Dr P Senthur Nambi Consultant Infectious Diseases") Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Lung Cancer Resection
 Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Radiology of the respiratory disease
 Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
INTRATHORACIC TUBERCULOSIS IN CHILDREN
 DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS IN CHILDREN A Guide For Low Income Countries 2003 International Union Against Tuberculosis and Lung Disease DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS
DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS IN CHILDREN A Guide For Low Income Countries 2003 International Union Against Tuberculosis and Lung Disease DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH. Leonard E. Swischuk, M.D. University of Texas Medical Branch
 ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
Approach to CXR. Terminology. 1.Identification. Greg Blecher SCH Respir Fellow. Correct patient Correct date and time Correct examination
 Approach to CXR Greg Blecher SCH Respir Fellow From Rob Posteraro http://home.earthlink.net/~rhpos/cxr_interpret.txt.html ; http://home.earthlink.net/~rhpos/cxr_main.txt.html) Approach to viewing Chest
Approach to CXR Greg Blecher SCH Respir Fellow From Rob Posteraro http://home.earthlink.net/~rhpos/cxr_interpret.txt.html ; http://home.earthlink.net/~rhpos/cxr_main.txt.html) Approach to viewing Chest
Thoracoscopy for Lung Cancer
 Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
Acute pneumonia Simple complement
 Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
B-I-2 CARDIAC AND VASCULAR RADIOLOGY
 (YEARS 1 3) CURRICULUM FOR RADIOLOGY 13 B-I-2 CARDIAC AND VASCULAR RADIOLOGY KNOWLEDGE To describe the normal anatomy of the heart and vessels including the lymphatic system as demonstrated by radiographs,
(YEARS 1 3) CURRICULUM FOR RADIOLOGY 13 B-I-2 CARDIAC AND VASCULAR RADIOLOGY KNOWLEDGE To describe the normal anatomy of the heart and vessels including the lymphatic system as demonstrated by radiographs,
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
Undergraduate Teaching
 Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Introduction to Chest CT Interpretation. Objectives 8/28/2017
 Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis?
. What is the diagnosis?") 1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission: