Bone Tumors: In 1 Simple Chart
|
|
|
- Belinda Harrington
- 5 years ago
- Views:
Transcription
 Mets/MM Chondroid: Osseous: Osteoid Osteoma")
 Patient s Age 2) Aggressive Zone of Transition Periosteal Reaction 3) Matrix 4) Location Building the Bone Tumor Chart Underlined Text = PowerPoint")
1 Bone Tumors with PowerPoint Interactivity Download this entire slideshow from When running this on your own computer you can jump from slide to slide using these buttons at bottom of each slide: Last slide viewed Overview slide The Chart p 1 of 31 ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Chondroid: Osseous: Osteoid Osteoma Osteoblastoma Osseous & Chondroid: Bone Infarct Stress Fracture Osteomyelitis (Chronic) Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s Overview of this Presentation Why Bone Tumors are Intimidating Describing Bone Tumors 1) Patient s Age 2) Aggressive Zone of Transition Periosteal Reaction 3) Matrix 4) Location Building the Bone Tumor Chart Underlined Text = PowerPoint Interactivity WhyBoneTumorsare Intimidating Bone Tumors are Rare ,500,000 New Cancer Cases in USA Annual Cancer Statistics Review, updated 5/29/09, p34 WhyBoneTumorsare Intimidating Bone Tumors are Rare 15% Renal/GU 180,000 Other 12% 221, ,000 Lung/Oral 18% 13% Breast 194, ,000 Prostate 13% 19% GI 276,000 Bone Tumors 2, % # Radiologists in USA = 30,000 2,570 Only 1-in-12 Radiologists will even see a Bone Tumor per year Bone Tumors: Many Types 30! Annual Cancer Statistics Review, updated 5/29/09, p Categories/SocioeconomicResearc h/practiceofradiologyintheus.aspx GREENSPAN: OrthoRad Ken L Schreibman, PhD/MD 01/10/10 www.
 Names 30% Incidence Bone Tumors 25% by 20% 15% Occur in children 10%")

 Patient s Age Osteogenic Sarcoma Everything else")
 Patient s Age 2) Aggressive vs Non-aggressive (NOT Malignant vs")

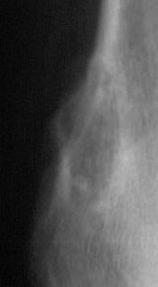
2 WhyBoneTumorsare Intimidating Bone Tumors are Rare Don t see enough to be confident Many types of Bone Tumors Have Confusing (similar) Names 30% Incidence Bone Tumors 25% by 20% 15% Occur in children 10% Essentially only 2 5% bone malignancies 0% >85 occur in children Bone Tumors: by Age p 2 of Bone Tumors: by Age Overview of this Presentation Why Bone Tumors are Intimidating Describing Bone Tumors 1) Patient s Age Osteogenic Sarcoma Everything else benign Could be anything Multiple Myeloma, Metastases Overview of this Presentation Why Bone Tumors are Intimidating Describing Bone Tumors 1) Patient s Age 2) Aggressive vs Non-aggressive (NOT Malignant vs Benign ) Zone of Transition Periosteal Reaction Not everything that looks aggressive is malignant (e.g. osteomyelitis) 2 Cases: Destructive lesions distal fibula Benign? Malignant? Can t tell with radiographs Thus we use the term Aggressive Ken L Schreibman, PhD/MD 01/10/10 www.







3 Zone of Transition Periosteal Reactions p 3 of 31 Zone of Transition Grow Slowly Narrow Geographic Well Defined Can Outline Lesion with Sharp Pencil Sclerotic Margins Grows VERY Slowly! Zone of Transition Grow Slowly Narrow Geographic Well Defined Can Outline Lesion with Sharp Pencil Sclerotic Margins Grows VERY Slowly! Zone of Transition Grow Slowly Narrow Geographic Well Defined Can Outline Lesion with Sharp Pencil Sclerotic Margins Grows VERY Slowly! Asymptomatic, incidental finding Zone of Transition Grow Slowly Narrow Geographic Well Defined Can Outline Lesion with Sharp Pencil Zone of Transition Grow Rapidly Wide Permeative Ill Defined Moth Eaten Cannot tell where Lesion ends and Normal Bone begins Grow Slowly Narrow Geographic Well Defined Can Outline Lesion with Sharp Pencil Sclerotic Margins Grows VERY Slowly! Ken L Schreibman, PhD/MD 01/10/10 www.





4 Zone of Transition Grow Rapidly Wide Permeative Ill Defined Moth Eaten Cannot tell where Lesion ends and Normal Bone begins Grows Rapidly Wide Permeative Ill Defined Moth Eaten p 4 of 31 Zone of Transition Cannot tell where Lesion ends and Normal Bone begins Grows Slowly Narrow Geographic Well Defined Can Outline Lesion with Sharp Pencil W,S 16yoF Periosteal Reaction Grows Rapidly Grows Slowly TOO COMPLI- CATED Simplifying Periosteal Reaction Grows Rapidly Interrupted Grows Slowly Solid Smooth Continuous Simplifying Periosteal Reaction Grows Slowly Solid Smooth Continuous Looks like Healing Callus Bone Model Fx F,A 2moM 1m later Simplifying Periosteal Reaction Grows Slowly Solid Smooth Continuous Bone Model HOA HPOA Hypertrophic Osteo- Pulmonary Arthropathy Osteo- Arthropathy V,T 49yoM Stable over 1y Ken L Schreibman, PhD/MD 01/10/10 www.



")




5 Simplifying Periosteal Reaction Grows Rapidly Interrupted May grow so rapidly it doesn t have time to ossify (Unossified periosteum is not radiopaque) p 5 of 31 Simplifying Periosteal Reaction Grows Rapidly Interrupted Lamellated Onionskin Grows ossifies Grows ossifies Grows ossifies Courtesy of James Choi, MD Simplifying Periosteal Reaction Grows Rapidly Interrupted Lamellated Onionskin Spiculated Hair-on-end Simplifying Periosteal Reaction Grows Rapidly Interrupted Lamellated Onionskin Spiculated Sunburst Codman s Triangles (Growing so rapidly, has time to ossify only at corners) Simplifying Periosteal Reaction Grows Rapidly Interrupted Lamellated Onionskin Spiculated Sunburst Codman s Triangles (Growing so rapidly, has time to ossify only at corners) Simplifying Periosteal Reaction Grows Rapidly Grows Slowly Interrupted Solid Lamellated Smooth Onionskin Continuous Spiculated Looks like Sunburst Healing Callus Codman s Triangles 8w post Fx, ORIF =more mature callus 3w post Fx, ORIF =very early callus S,C 15yoM Ken L Schreibman, PhD/MD 01/10/10 www.
 Aggressive vs Non-aggressive Zone of Transition Periosteal Reaction")




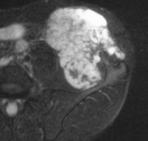
6 Overview of this Presentation Why Bone Tumors are Intimidating Describing Bone Tumors 1) Patient s Age 2) Aggressive vs Non-aggressive Zone of Transition Periosteal Reaction Cortical Destruction p 6 of 31 Cortical Destruction Cortex Absent = Aggressive Similar lytic lesions Both have well defined, sclerotic, medullary borders IR Cortex Intact = Non-aggressive Overview of this Presentation Why Bone Tumors are Intimidating Describing Bone Tumors 1) Patient s Age 2) Aggressive vs Non-aggressive Zone of Transition Periosteal Reaction Radiographs Cortical Destruction MRI Soft Tissue Extension 2 Cases: Aggressive lesions distal fibula Benign? Malignant? Can t tell with radiographs Thus we use the term Aggressive Periosteal Reaction Cortical Destruction 2 Cases: Aggressive lesions distal fibula T2 Soft Tissue Extension Active Osteomyelitis Chronic Osteo. T2 Two YEARS later H,M 13yoF Ken L Schreibman, PhD/MD 01/10/10 www.
















7 Bone Matrix: 4 Types Chondroid rings&arcs Osseous cloud-like amorphous Bone Matrix: 4 Types Chondroid rings&arcs p 7 of 31 Calcified Uterine Fibroid Fibrous Ground Glass Myositis Ossificans None Purely Not necessarily cystic Multiple Myeloma Calcified Uterine Fibroid Bone Matrix: 4 Types Osseous cloud-like amorphous Bone Matrix: 4 Types Fibrous Ground Glass F,C 8yoF Osteogenic Sarcoma Myositis Ossificans H,S 15yoM Fibrous Dysplasia B,C 53yoF Bone Matrix: 4 Types None Purely Bone Matrix: 4 Types None Purely CT Not necessarily cystic S,N 62yoM Multiple Myeloma Not necessarily cystic Intraosseous Lipoma G,B 18yoF Ken L Schreibman, PhD/MD 01/10/10 www.

 Distal Femur Proximal Tibia (where most growth occurs) Matrix: Osseous osteo-genic : makes bone Need to eval for skip")


8 Overview of this Presentation Why Bone Tumors are Intimidating Describing Bone Tumors 1) Patient s Age 2) Aggressive 3) Matrix 4) Location Which bone? Some tumors have propensity for certain bones Which part of the bone? MANY tumors characteristically occur at the: Epiphysis / Metaphysis / Diaphysis p 8 of 31 Osteogenic Sarcoma Pt Age: years (when growth spurt occurs) Location: Metaphyseal (where growth occurs) Distal Femur Proximal Tibia (where most growth occurs) Matrix: Osseous osteo-genic : makes bone Need to eval for skip mets MR entire length of bone Osteogenic Sarcoma Pt Age: years Location: Metaphyseal Matrix: Osseous F,C 8yoF MRI is useful for staging the extent of the tumor T2 Osteogenic Sarcoma F,C 8yoF MRI is useful for staging the extent of the tumor Radiographs show us what we need to know to diagnose type of tumor! Skeletally immature Aggressive lesion Wide zone of trans. Sunburst periost. Osseous matrix Metaphyseal Osteogenic Sarcoma! Osteogenic Sarcoma Sometimes osteosarc is growing SO quickly it doesn t have time to form an osseous matrix R,T 11yoF Patient presents with hair-on-end periosteal reaction After 2 months of chemotherapy tumor growth has slowed enough to form osseous matrix Ken L Schreibman, PhD/MD 01/10/10 www.





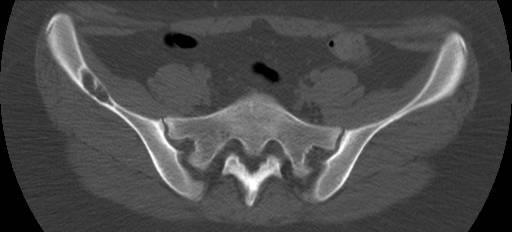
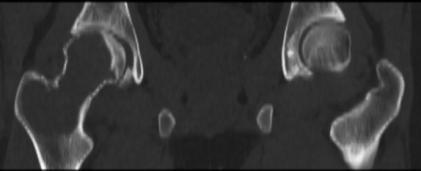
9 Pt Age: 5-25 years Tumor of Bone Marrow Location: Diaphyseal Flat Bones Matrix: Permeative Cortical Destruction Aggressive Periosteal Reaction Soft Tissue Extension >> Bone Extent H,M 13yoF p 9 of 31 T2 Soft Tissue Extension T2 >> Bone Extent common in pelvis Air in colon Things can hide in the pelvis S,B 6yoM Air in colon? 3 months later common in pelvis T2fs Things can hide in the pelvis S,B 6yoM Unlike in the extremities where radiographs are key, the usefulness of radiographs in the pelvis is limited. In the pelvis, cross-sectional imaging is crucial, preferably with MRI. Osteomyelitis resembles Tumor! Whenever doing a bone biopsy, ALWAYS send samples for BOTH surgical pathology AND microbiology culture! Do Not Touch lesions : Do Not Touch! They all present like this: Athletic teenr Just a little periosteal reaction MEDIAL posterior femoral condyle Tug lesion: Adductor longus insertion Q,M 17yoM Medial gastrocnemius origin Ken L Schreibman, PhD/MD 01/10/10 www.








10 : Do Not Touch! CT Just a little periosteal reaction MEDIAL posterior femoral condyle Tug lesion: Adductor longus insertion Q,M 17yoM Cross-sectional imaging doesn t really help T2fs Medial gastrocnemius origin p 10 of 31 ALWAYS consider! is 29x more common than all Bone Tumors combined = 74, ,000 Other 12% 15% Renal/GU 221, ,000 Lung/Oral 18% 13% Breast 194, ,000 Prostate 13% 19% GI 276,000 New Cancer Cases, USA, 2009 Bone Tumors 2, % Tumor of bone marrow Can be lytic or blastic R,H 22yoM Resembles Ewing T2fs Why Age is Important Location: Diaphyseal Soft tissue extension Age: < 20 Age: Age: > 40 Metastases Multiple Myeloma Cartil malignancy Matrix: Chondroid Location: Ends of bones Pelvis Soft tissues Cartil malignancy Matrix: Chondroid Chondroid rings&arcs Radiographs S,B 39yoM Ken L Schreibman, PhD/MD 01/10/10 www.







11 Cartil malignancy Matrix: Chondroid Chondroid rings&arcs Radiographs CT Cartil malignancy Matrix: Chondroid T2fs p 11 of 31 fs +Gd Chondroid MRI T2: Bright Gd: peripheral enhancement Bulk of tumor doesn t enhance S,B 39yoM S,B 39yoM Cartil malignancy Matrix: Chondroid Normal cartil has no blood supply Injured cartil doesn t regrow : poor blood supply Shows very little Gd enhancement Doesn t respond to chemotherapy Treatment: Complete tumor resection Cartil malignancy Matrix: Chondroid Normal cartil has no blood supply Injured cartil doesn t regrow : poor blood supply Shows very little Gd enhancement Doesn t respond to chemotherapy Treatment: Complete tumor resection S,B 39yoM 30yoF 1 year history heal pain other side 1 week later T2fs fs +Gd W,A 30yoF Ken L Schreibman, PhD/MD 01/10/10 www.
 Pt Age: > 20 May involve the bones Secondarily Primarily")

 Conventional Pt Age: 10-20 years Location: Metaphyseal")

12 p 12 of 31 Fibrosarcoma Malignant Fibroblastic Cells Malignant Fibrous Histiocytoma (MFH) Pt Age: > 20 May involve the bones Secondarily Primarily Fibrosarcoma MRI is useful for staging the extent of the tumor T2fs F,B 23yoF Osteogenic Sarcoma Pt Age: years Location: Metaphyseal Matrix: Osseous 4 Subtypes: 1) Conventional 2) Telangiectatic Surface s 3) PERIosteal 4) PARosteal Osteogenic Sarcoma 1) Conventional Pt Age: years Location: Metaphyseal Matrix: Osseous 2) Telangiectatic Highly vascular/bloody Very aggressive Nearly purely lytic Usually present after pathologic fracture Diffuse metastases Ken L Schreibman, PhD/MD 01/10/10 www.

 PERIosteal Looks like aggressive periosteal reaction")




 PARosteal Pt Age: 20-30 years Location:")


13 Osteogenic Sarcoma Surface Pt Age: years Good prognosis if marrow not involved, can resect tumor. If spreads to marrow, conventional OS. 3) PERIosteal Looks like aggressive periosteal reaction Location: Long bones p 13 of 31 Periosteal Aggressive Periosteal Reaction tibia 11yoM 2004 Radiological Society of North America Murphey M D et al. Radiology 2004; 233: Periosteal Aggressive Periosteal Reaction tibia 34yoF 2004 Radiological Society of North America Soft Tissue Extension Sparing Bone Marrow Murphey M D et al. Radiology 2004; 233: Osteogenic Sarcoma Surface Pt Age: years Good prognosis if marrow not involved, can resect tumor If spreads to marrow, conventional OS. 3) PERIosteal Looks like aggressive periosteal reaction 4) PARosteal Osteogenic Sarcoma Surface 4) PARosteal Pt Age: years Location: Back of Femoral Condyles Arise from cortex, grow outward Do NOT contain normal marrow (As opposed to osteochondroma) CT Osteogenic Sarcoma T2fs MRI: No Marrow involvement CT Ken L Schreibman, PhD/MD 01/10/10 www.





14 VERY RARE 0.1% Primary Bone Tumors Pt Age: Matrix: Permeative Location: TIBIA (90%) Diaphyseal Anterior Cortex Soft Tissue Mass: Likely Malignant p 14 of 31 VERY RARE 0.1% Primary Bone Tumors Pt Age: Matrix: Permeative Location: TIBIA (90%) Diaphyseal Anterior Cortex Soft Tissue Mass: Likely Malignant VERY RARE 0.1% Primary Bone Tumors Pt Age: Matrix: Permeative Location: TIBIA (90%) Diaphyseal Anterior Cortex Soft Tissue Mass: Likely Malignant Ken L Schreibman, PhD/MD 01/10/10 www.



 Aneurysmal")

 Bone")



15 ABC UBC CB FCD/NOF EG p 15 of 31 A) Aneurysmal Bone Cyst Pt Age: < 20 Matrix: None (Cyst) Only tumor named for x-ray appearance Aneurysmal & Cystic AVM of Bone MRI: fluid/fluid level Location: Metaphyseal Posterior Spine Hands Pelvis A) Aneurysmal Bone Cyst A) Aneurysmal Bone Cyst CT Aneurysmal Multi-septated looks like soap bubbles N,N 15yoF T2 fluid/fluid level Aneurysmal Multi-septated looks like soap bubbles A) Aneurysmal Bone Cyst A) Aneurysmal Bone Cyst T2 fluid/fluid level fluid/fluid level D,R 12yoM Aneurysmal Multi-septated looks like soap bubbles T2 Aneurysmal Multi-septated looks like soap bubbles Ken L Schreibman, PhD/MD 01/10/10 www.


")













16 B) Unicameral (Simple) Bone Cyst Uni-cameral: Latin one - chamber (in US we have bi-cameral legislature) Pt Age:< 20 Matrix: None (True Cyst) Location:Metaphyseal >50% Proximal Humerus 20-30% Proximal Femur 50% - Incidental Finding 50% - Pathologic Fx Fallen Fragment p 16 of 31 B) Unicameral (Simple) Bone Cyst Normal Side D,C 5yoM B) Unicameral (Simple) Bone Cyst Fractures tend to heal Fracture healed B) Unicameral (Simple) Bone Cyst Cysts tend to recur Although UBCs arise from metaphysis end of bone grows away from cyst Cyst? so cyst becomes diaphyseal D,C 5yoM after 1 month after 3 months 6m later 12m later 18m later B) Unicameral (Simple) Bone Cyst MRI shows cyst extent T2fs B) Unicameral (Simple) Bone Cyst T2fs 18m later Simple cyst M,T 4yoM Fallen Fragment after 3 months Ken L Schreibman, PhD/MD 01/10/10 www.
 Unicameral (Simple) Bone Cyst T2fs")
")


")





17 B) Unicameral (Simple) Bone Cyst p 17 of 31 B) Unicameral (Simple) Bone Cyst T2fs Simple cyst with hemorrh fluid-fluid level P,D 6yoM H,T 18yoM C) Chondroblastoma Pt Age: Skeletally immature Location: Epiphyseal Matrix: Chondroid (No matrix if not calcified) Benign Aggressive appearance! Periosteal Reaction Surrounding Edema Bone Marrow Soft Tissues C) Chondroblastoma T2fs Pt Age: 10 30yo Location: Epiphyseal Matrix: Chondroid (No matrix if not calcified) Benign Aggressive appearance! Periosteal Reaction Surrounding Edema Bone Marrow Soft Tissues 16yoM C) Chondroblastoma Cartil-sensitive sequence C) Chondroblastoma Epiphyseal mass, skeletally immature Aggressive appearance Edema in surrounding marrow & tissues IR Cartil sequence Cartil unfused physis Articular Cartil 16yoM B,Q 15yoM Ken L Schreibman, PhD/MD 01/10/10 www.
")
 If >50% bone diameter Fx Location: Metaphysis")
 Radiographic appearance: Characteristic& Diagnostic If")


 9yo 11yo 13yo G,M 9yoF Fx Healing Callus")

18 D) Fibrous Cortical Defect Non-Ossifying Fibroma (NOF) THE most common bone lesion Occurs up to 40% ALL children (75% occur years old) Regress after skeletal maturity Asymptomatic, incidental finding (e.g. on knee MR for ACL tear) If >50% bone diameter Fx Location: Metaphysis Femur & Tibia p 18 of 31 D) Fibrous Cortical Defect Non-Ossifying Fibroma (NOF) Radiographic appearance: Characteristic& Diagnostic If asymptomatic, no further workup is needed Eccentric, sub-cortical Cortex thinned, expanded Sclerotic margin Scalloped Multi-loculated F,M 18yoF D) Fibrous Cortical Defect Non-Ossifying Fibroma (NOF) Radiographic appearance: IR No aggressive characteristics Characteristic& Diagnostic If asymptomatic, no further workup is needed Eccentric, sub-cortical Cortex thinned, expanded Sclerotic margin Scalloped Multi-loculated B,J 19yoM D) Fibrous Cortical Defect Non-Ossifying Fibroma (NOF) 9yo 11yo 13yo G,M 9yoF Fx Healing Callus Ken L Schreibman, PhD/MD 01/10/10 www.
 Triad: skull lesions, exophthalmos, DI Letterer-Siwe (<3yo, fatal) Pain, swelling, fever, ESR, eosinophilia Diff.")
 Eosinophilic Granuloma Pt Age: < 12 Matrix: None Location: Bone Marrow Skull (most common site) Sharp Punched-out Beveled Edge due to uneven involvement of outer/inner table W,J 2yoM")
 Eosinophilic Granuloma Pt Age: < 12 Matrix: None Location: Bone Marrow Skull (most common site) Spine Pelvis supra-acetabulum Long bones (Femur) diaphysis R,D 5yoM E) Eosinophilic Granuloma Pt")
19 E) Eosinophilic Granuloma Non-neoplastic proliferation histiocytes Langerhans Cell Histiocytosis Pt Age: typically <12yo (can occur young adult) EG (aka Histiocytosis X) Hand-Schuller-Christian (>3yo) Triad: skull lesions, exophthalmos, DI Letterer-Siwe (<3yo, fatal) Pain, swelling, fever, ESR, eosinophilia Diff.Dx: Osteomyelitis (Ewing, Lymph/Leuk) Bone lesions may resolve spontaneously Often get Dx Bx/curett. Steroids? p 19 of 31 E) Eosinophilic Granuloma Pt Age: < 12 Matrix: None Location: Bone Marrow Skull (most common site) Sharp Punched-out Beveled Edge due to uneven involvement of outer/inner table W,J 2yoM E) Eosinophilic Granuloma Pt Age: < 12 Matrix: None Location: Bone Marrow Skull (most common site) Spine vertebra plana Can regrow height with treatment! E) Eosinophilic Granuloma Pt Age: < 12 Matrix: None Location: Bone Marrow Skull (most common site) Spine Pelvis supra-acetabulum Long bones (Femur) diaphysis R,D 5yoM E) Eosinophilic Granuloma Pt Age: < 12 Matrix: None Location: Bone Marrow Skull (most common site) Spine Pelvis supra-acetabulum Long bones (Femur) diaphysis W,J 2yoM F,D 5yoM ABC UBC CB FCD/NOF EG Ken L Schreibman, PhD/MD 01/10/10 www.

 Presents at younger")




")


20 F) Fibrous Dysplasia Pt Age: <30 years Location: Any bone Matrix: Ground Glass Monostotic (one bone) Usually asymptomatic Polyostotic (many bones) Presents at younger Usually symptomatic Syndromes McCune Albright syndrome R L,I 7yoM Base of skull Top of skull p 20 of 31 McCune Albright syndrome Triad Polyostotic Fibrous Dysplasia Unilateral R L R L R L L R L,I 7yoM McCune Albright syndrome Triad Polyostotic Fibrous Dysplasia Unilateral Endocrine Abnormalities Precocious puberty in girls café au lait spots coast of Maine McCune Albright syndrome Triad Polyostotic Fibrous Dysplasia Unilateral Endocrine Abnormalities Precocious puberty in girls café au lait spots coast of Maine (as opposed to coast of California =Neurofibromatosis) wikipedia.org ABC UBC CB FCD/NOF EG Ken L Schreibman, PhD/MD 01/10/10 www.











21 ABC UBC CB FCD/NOF EG GCT Giant Cell Tumor Pt Age: Skeletally Mature (as opposed to Chondroblastoma) THE most common bone tumor in young adults yo Location: Subarticular Arise from Metaphysis Extend across fused Growth Plate Matrix: Purely Narrow Zone of Transition NO SCLEROTIC MARGIN p 21 of 31 Giant Cell Tumor Pt Age: Skeletally T2fs Mature (as opposed to Chondroblastoma) THE most common bone tumor in young adults yo Location: Subarticular Arise from Metaphysis Extend across fused Growth Plate Matrix: Purely Narrow BenignZone of Transition NO Locally SCLEROTIC Aggressive MARGIN V,R 21yoM Giant Cell Tumor Benign Locally Aggressive B,J 25yoM Giant Cell Tumor T2fs fs+gd Giant Cell Tumor Pt Age: Skeletally Mature Physis fused 16yoM 18yoM Solid & Cystic components Histologically, similarities GCT ABC B,J 25yoM C,A 18yoM Ken L Schreibman, PhD/MD 01/10/10 www.
 Chondroblastoma 1 Age: Lung (skeletally mature) Cancer Giant Cell")

 Lesion: Distal Phalanx Giant Cell Tumor : phalanges Tendon")
22 Why Age is Important Location: Subarticular Matrix: Purely Age:< 20 (skeletally immature) Chondroblastoma Age: (skeletally mature) Giant Cell Tumor Age:> 40 Metastases Multiple Myeloma GCT V,R 21yoM Why Age is Important Location: Subarticular Matrix: Purely Age:< 20 (skeletally immature) Chondroblastoma 1 Age: Lung (skeletally mature) Cancer Giant Cell Tumor Age:> 40 Metastases Multiple Myeloma p 22 of 31 Met C,G 61yoM ABC UBC CB FCD/NOF EG GCT Pitts Pit Herniation Pit of the Femoral Neck aka Pitt s Pit Michael Pitt, et.al. AJR 1982 vol 138, 6, p Round lucency Thin sclerotic rim Proximal Superior Anterior courtesy Donna Blankenbaker, MD Incidental finding ⅓ patients Mechanical, not neoplastic ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Lesion: Distal Phalanx Giant Cell Tumor : phalanges Tendon Sheath Pathologic Fx (Localized PVNS) Glomus Tumor Felon Nail bed (Fingertip infection) Dorsal Sarcoidosis Epidermoid Inclusion Cyst Gout Puncture Metastases Volar Lung Ken L Schreibman, PhD/MD 01/10/10 www.






 Triad")




 Volar S,D")

23 Benign rests of hyaline cartil Common Often discovered incidentally Typically asymptomatic 50% small tubular bones Mostly lytic Pathologic Fracture p 23 of 31 Glomus Tumor Benign vascular tumor (neuromyoarterial apparatus) Subungual, erodes bone Dorsal cortex distal phalanx Age: ( 3x> ) Triad Sensitivity to cold Localized tenderness Severe intermittent pain S,D 37yoF Glomus Tumor Dorsal cortex distal phalanx Epidermoid Inclusion Cyst Implantation of epidermal elements Amputation Puncture (seamstress) Volar cortex distal phalanx S,D 53yoM fs fs+gd fs+gd T2fs Epidermoid Inclusion Cyst Gout M,B 78yoM Ken L Schreibman, PhD/MD 01/10/10 www.
 Mets/MM Mets/MM ( POEMS ) POEMS syndrome Polyneuropathy Organomegaly Endocrinopathy")

 Pt s Pt s Disease Becoming less common Three Phases : Wedge with sharp borders")
 Mets/MM Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s")

24 ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Mets/MM ( POEMS ) POEMS syndrome Polyneuropathy Organomegaly Endocrinopathy Monoclonal gammopathy Skin abnormalities (Sclerotic bone lesions) Medial Clavicle Pelvis p 24 of 31 ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s Pt s Disease Becoming less common Three Phases : Wedge with sharp borders Blade of grass, Candle flame Mixed: Bone destruction & formation : Cortical/Trabecular thickening 2 B,S 83yoF ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s Ivory Vertebra Pt Met Breast Prostate Treated Met Chronic Osteo (Sarcoid) rare K,K 76yoM Ken L Schreibman, PhD/MD 01/10/10 www.
 Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s p 25 of 31 Benign rests of hyaline cartil Common")


25 ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Bone Infarct Stress Fracture Osteomyelitis (Chronic) Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s p 25 of 31 Benign rests of hyaline cartil Common Often discovered incidentally Typically asymptomatic can be painful (40%) Pathologic Fracture 50% long tubular bones Metaphyseal Chondroid matrix Benign rests of hyaline cartil Common Often discovered incidentally Typically asymptomatic can be painful (40%) Pathologic Fracture 50% long tubular bones Metaphyseal Chondroid matrix Benign rests of hyaline cartil Common Often discovered incidentally Typically asymptomatic can be painful (40%) Pathologic Fracture 50% long tubular bones Metaphyseal Chondroid matrix 50% small tubular bones Mostly lytic Malignant tumor of cartil Pelvis Ends of bones Presents with PAIN! 99% Painful 40% s Low Grade difficult to differentiate from benign Radiologist Pathologist 30% - Low Grade Histopathology 1: Low Grade 2: Intermediate 3: High Grade Cellularity: markedly increased Nuclei Size: markedly increased Ken L Schreibman, PhD/MD 01/10/10 www.








26 IR Histopathology 1: Low Grade 2: Intermediate 3: High Grade Cellularity: markedly increased Nuclei Size: markedly increased fs + Gd p 26 of 31 Histopathology 1: Low Grade 2: Intermediate 3: High Grade Cellularity: slightly increased Nuclei Size: slightly increased Histopathology 0.5: Borderline 1: Low Grade 2: Intermediate 3: High Grade Histologically: resembles enchondroma Radiologically: aggressive B,B 42yoF T2fs How do you distinguish between them? Very difficult, sometimes you can t Clues: Some Enchon All Chondrosarc Hot on BS Hot on BS Pt was very happy with outcome! She s now pain free She s doesn t have cancer 40% Enchon Painful This pt had pain uncontrollable with oral narcotics All Chondrosarc Painful (never incidental) B,B 42yoF This pt had pain uncontrollable with oral narcotics Histopathology: No malignant cells So was this:? 0.5 Borderline? Ken L Schreibman, PhD/MD 01/10/10 www.
 Mets/MM Bone Infarct Stress")
 Pt s p 27 of 31 Epidermoid,Felon GCTTS,Sarcoid")
 Pt s Osteoid Osteoma")





27 ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Bone Infarct Stress Fracture Osteomyelitis (Chronic) Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s p 27 of 31 ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Chondroid: Osseous: Osteoid Osteoma Osteoblastoma Bone Infarct Stress Fracture Osteomyelitis (Chronic) Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s Osteoid Osteoma (Osteoblastoma) Pt Age: < 30 Presents with PAIN! 98% Painful Night pain, Rx NSAID Matrix: Lucent Nidus Location: Diaphyseal Surrounding Sclerosis Intra-capsular No Sclerosis Posterior Elements (OB) Painful Scoliosis Osteoid Osteoma Radiographs Cortical thickening Bone Scan Hot all 3 phases Flow Blood Pool Delayed W,N 13yoM Osteoid Osteoma Radiographs Cortical thickening MR Edema Enhancement Nidus Pain Marker Marrow Edema Cortical Thicken Sub-Q Edema Osteoid Osteoma CT: Gold Standard for OO Diagnosis Lucent Nidus Central Dot Calcium Rx CT Guided RF Ablation T2fs fs +Gd fs IR +Gd W,N 13yoM W,N 13yoM Ken L Schreibman, PhD/MD 01/10/10 www.
 Term")




 SPECT")
 S,T 16yoM")





28 Osteoblastoma (= Osteoid Osteoma) Term osteoblastoma used for: Larger lesions ( > 1cm) Lesion in spine posterior elements Painful scoliosis (Typically scoliosis is painless) S,T 16yoM p 28 of 31 Osteoblastoma (= Osteoid Osteoma) Bone Scan (Posterior) SPECT (Sagittal) SPECT (Axial) S,T 16yoM Osteoblastoma (= Osteoid Osteoma) CT: Gold Standard Diagnosis Lucent Nidus Central Dot Calcium Osteoblastoma Young woman with back pain Fetus is an incidental finding Years earlier with back pain S,T 16yoM Ken L Schreibman, PhD/MD 01/10/10 www.
 Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s p 29 of 31 Most Common Benign Neoplasm of Bone Exostosis Pedunculated (stalk) Sessile")
 Sessile (flat) Cartil Cap seen only on MR Point away from joint Continuity with underlying bone Cortex continuous with cortex Marrow continuous with marrow Most Common")

29 ABC UBC CB FCD/NOF EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Chondroid: Osseous: Osteoid Osteoma Osteoblastoma Osseous & Chondroid: Bone Infarct Stress Fracture Osteomyelitis (Chronic) Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s p 29 of 31 Most Common Benign Neoplasm of Bone Exostosis Pedunculated (stalk) Sessile (flat) Cartil Cap seen only on MR Point away from joint Continuity with underlying bone Cortex continuous with cortex Marrow continuous with marrow Bone Model Most Common Benign Neoplasm of Bone Exostosis Pedunculated (stalk) Sessile (flat) Cartil Cap seen only on MR Point away from joint Continuity with underlying bone Cortex continuous with cortex Marrow continuous with marrow Most Common Benign Neoplasm of Bone Exostosis Pedunculated (stalk) Sessile (flat) Cartil Cap seen only on MR Point away from joint Continuity with underlying bone Cortex continuous with cortex Marrow continuous with marrow Most Common Benign Neoplasm of Bone Exostosis Pedunculated (stalk) Sessile (flat) Cartil Cap seen only on MR Point away from joint Continuity with underlying bone Cortex continuous with cortex Marrow continuous with marrow Most Common Benign Neoplasm of Bone Exostosis Pedunculated (stalk) Sessile (flat) Cartil Cap seen only on MR Point away from joint Continuity with underlying bone Cortex continuous with cortex Marrow continuous with marrow P,N 20yoF Ken L Schreibman, PhD/MD 01/10/10 www.
 Sessile (flat) Cartil Cap seen")



: 10-30% Signs")
 Cartil")



30 Most Common Benign Neoplasm of Bone Exostosis Pedunculated (stalk) Sessile (flat) Cartil Cap seen only on MR Point away from joint Continuity with underlying bone Cortex continuous with cortex Marrow continuous with marrow p 30 of 31 Most Common Benign Neoplasm of Bone Exostosis Pedunculated (stalk) Sessile (flat) Cartil Cap seen only on MR Point away from joint Continuity with underlying bone Cortex continuous with cortex Marrow continuous with marrow K,J 11yoM T2fs Cartil Cap No aggressive characteristics Cortex continuous with cortex Marrow continuous with marrow K,J 11yoM Most Common Benign Neoplasm of Bone Malignant Transformation to Solitary: 1% Multiple Hereditary Exostoses (MHE): 10-30% Signs of malignant transformation: Growth of lesion after skeletal maturity (can grow during childhood) Cartil cap > 1cm (can be 2-3cm during childhood) Malignant Transformation to Malignant Transformation to Chondroid matrix Aggressive appearance T2fs CT: Tissue Window fs+gd CT: Bone Window Hot on BS c/w Chondrosarc Funny shaped femurs MHE? Ken L Schreibman, PhD/MD 01/10/10 www.

: 10-30% Signs of")

 Cartil cap > 1cm (can")












31 Most Common Benign Neoplasm of Bone Malignant Transformation to Solitary: 1% Multiple Hereditary Exostoses (MHE): 10-30% Signs of malignant transformation: Growth of lesion after skeletal maturity (can grow during childhood) Cartil cap > 1cm (can be 2-3cm during childhood) Can cause mechanical problems p 31 of 31 Can cause mechanical problems Multiple miscarris T2fs W,M 25yoF Can cause mechanical problems Can cause mechanical problems Mass effect on right subclavian artery Rubbing, causing Pes Anserine Bursitis T2fs K,T 18yoM MRA H,P 11yoF PDfs vs PARosteal Cortex continuous with cortex Marrow continuous with marrow Cartil Cap W,K 17yoM T2fs NO cortex/marrow continuity ABC UBCB CB FCD/NO EG GCT Pitts Pit PHALANX: Enchon, Glomus Epidermoid,Felon GCTTS,Sarcoid Gout,Met(lung) Mets/MM Chondroid: Osseous: Osteoid Osteoma Osteoblastoma Osseous & Chondroid: Bone Infarct Stress Fracture Osteomyelitis (Chronic) Ivory Vertebra :,Pt,Met Mets/MM ( POEMS ) Osteomyelitis (Chronic) Pt s Ken L Schreibman, PhD/MD 01/10/10 www.
Bone Tumors Clues and Cues
 William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
The Radiology Assistant : Bone tumor - well-defined osteolytic tumors and tumor-like lesions
 Bone tumor - well-defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - well-defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
MARK D. MURPHEY MD, FACR. Physician-in-Chief, AIRP. Chief, Musculoskeletal Imaging
 ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
APMA 2018 Radiology Track Bone Tumors When to say Gulp!
 APMA 2018 Radiology Track Bone Tumors When to say Gulp! DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine Conflict of
APMA 2018 Radiology Track Bone Tumors When to say Gulp! DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine Conflict of
Bone tumors. RMG: jan
 Bone tumors RMG: jan 217. @Kijohs KIZZA JOHN KIJOHS Diseases arising in bone Lipoma Fibrous cortical defects Non-ossifying fibroma Bone island Benign simple cysts Enchondroma Osteochondroma Osteoid osteoma
Bone tumors RMG: jan 217. @Kijohs KIZZA JOHN KIJOHS Diseases arising in bone Lipoma Fibrous cortical defects Non-ossifying fibroma Bone island Benign simple cysts Enchondroma Osteochondroma Osteoid osteoma
The Radiology Assistant : Bone tumor - ill defined osteolytic tumors and tumor-like lesions
 Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Typical skeletal location and differential diagnosis of bone tumors.
 Typical skeletal location and differential diagnosis of bone tumors. Poster No.: C-2418 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Barros, L. A. Ferreira, Y. Costa, P. J. V. Coelho, F. Caseiro
Typical skeletal location and differential diagnosis of bone tumors. Poster No.: C-2418 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Barros, L. A. Ferreira, Y. Costa, P. J. V. Coelho, F. Caseiro
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell
 Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Bone Tumours - a synopsis. Dr Zena Slim SpR in Histopathology QAH 2009
 Bone Tumours - a synopsis Dr Zena Slim SpR in Histopathology QAH 2009 Aims General approach to diagnosis Common entities.and not so common ones. Mini quiz Challenge of bone tumour diagnosis Bone tumours
Bone Tumours - a synopsis Dr Zena Slim SpR in Histopathology QAH 2009 Aims General approach to diagnosis Common entities.and not so common ones. Mini quiz Challenge of bone tumour diagnosis Bone tumours
Bubbly Lesions of Bone
 Residents Section Pattern of the Month w79 08.18.09 Eisenberg Residents Section Pattern of the Month Residents inradiology Ronald L. Eisenberg 1 Eisenberg RL Keywords: bubbly lesions, fegnomashic, skeletal
Residents Section Pattern of the Month w79 08.18.09 Eisenberg Residents Section Pattern of the Month Residents inradiology Ronald L. Eisenberg 1 Eisenberg RL Keywords: bubbly lesions, fegnomashic, skeletal
Malignant bone tumors. Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7%
 Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
FEGNOMASHIC: from x-ray to MRI
 FEGNOMASHIC: from x-ray to MRI Poster No.: C-2441 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Fouassier, A. L. C. Duarte, C. Ruivo, J. Velez ; Évora/PT, 1 2 1 2 3 1 3 Coimbra/PT, PT Keywords:
FEGNOMASHIC: from x-ray to MRI Poster No.: C-2441 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Fouassier, A. L. C. Duarte, C. Ruivo, J. Velez ; Évora/PT, 1 2 1 2 3 1 3 Coimbra/PT, PT Keywords:
Fluid-fluid levels in bone tumors: A pictorial review
 Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
Bone and Joint Part 2. Leslie G Dodd, MD
 Bone and Joint Part 2 Leslie G Dodd, MD Relative rates of cancer Sarcomas are relatively uncommon tumors New cancer cases 2007 All sites 1.4 million prostate 218,890 lung 213,380 breast 180,510 Soft tissue
Bone and Joint Part 2 Leslie G Dodd, MD Relative rates of cancer Sarcomas are relatively uncommon tumors New cancer cases 2007 All sites 1.4 million prostate 218,890 lung 213,380 breast 180,510 Soft tissue
Introduction to Musculoskeletal Tumors. James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon
 Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Imaging Findings Of Bone Tumors: A Pictorial Review
 Imaging Findings Of Bone Tumors: A Pictorial Review Poster No.: C-2511 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Limeme, N. Benzina, A. BelKhiria, H. Zaghouani, S. Majdoub, N. Mallat, H.
Imaging Findings Of Bone Tumors: A Pictorial Review Poster No.: C-2511 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Limeme, N. Benzina, A. BelKhiria, H. Zaghouani, S. Majdoub, N. Mallat, H.
Bread and Butter Bone Pathology
 Bread and Butter Bone Pathology NICOLE D. RIDDLE, MD RUFFOLO, HOOPER, AND ASSOC. / UNIVERSITY OF SOUTH FLORIDA Goals: Fundamentals of neoplastic bone pathology Bone Producing Cartilage Producing Miscellaneous
Bread and Butter Bone Pathology NICOLE D. RIDDLE, MD RUFFOLO, HOOPER, AND ASSOC. / UNIVERSITY OF SOUTH FLORIDA Goals: Fundamentals of neoplastic bone pathology Bone Producing Cartilage Producing Miscellaneous
Radiography in the Initial Diagnosis of Primary Bone Tumors
 Residents Section Structured Review Costelloe and Madewell Radiography of Primary Bone Tumors Residents Section Structured Review Colleen M. Costelloe 1 John E. Madewell Costelloe CM, Madewell JE Keywords:
Residents Section Structured Review Costelloe and Madewell Radiography of Primary Bone Tumors Residents Section Structured Review Colleen M. Costelloe 1 John E. Madewell Costelloe CM, Madewell JE Keywords:
Radiologic approach to pediatric lytic bone lesions
 Radiologic approach to pediatric lytic bone lesions Poster No.: C-1177 Congress: ECR 2016 Type: Educational Exhibit Authors: J. L. LERMA GALLARDO, I. de la Pedraja, A. Lancharro 1 1 1 2 1 1 Zapata, J.
Radiologic approach to pediatric lytic bone lesions Poster No.: C-1177 Congress: ECR 2016 Type: Educational Exhibit Authors: J. L. LERMA GALLARDO, I. de la Pedraja, A. Lancharro 1 1 1 2 1 1 Zapata, J.
Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples
 Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples Poster No.: C-1741 Congress: ECR 2015 Type: Educational Exhibit Authors: J. Silva, M. A. Ramírez
Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples Poster No.: C-1741 Congress: ECR 2015 Type: Educational Exhibit Authors: J. Silva, M. A. Ramírez
MRI XR, CT, NM. Principal Modality (2): Case Report # 2. Date accepted: 15 March 2013
: Case Report # 2. Date accepted: 15 March 2013") Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
COPYRIGHT 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
 84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
Grading of Bone Tumors
 Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology
 Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology Poster No.: C-2473 Congress: ECR 2013 Type: Educational Exhibit Authors: I. Candelaria, L. B. Barbosa,
Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology Poster No.: C-2473 Congress: ECR 2013 Type: Educational Exhibit Authors: I. Candelaria, L. B. Barbosa,
Key points in the evaluation of focal bone lesions: from plain film to multidetector CT
 Key points in the evaluation of focal bone lesions: from plain film to multidetector CT Poster No.: C-2060 Congress: ECR 2011 Type: Educational Exhibit Authors: I. Rubio Marco, M. Arraiza Sarasa, H. Gómez
Key points in the evaluation of focal bone lesions: from plain film to multidetector CT Poster No.: C-2060 Congress: ECR 2011 Type: Educational Exhibit Authors: I. Rubio Marco, M. Arraiza Sarasa, H. Gómez
VALORACIÒN RADIOLÓGICA DE LA LESIÒN ÒSEA SOLITARIA IMAGENOLOGIA MEDICA UNIVERSIDAD HISPANOAMERICANA
 VALORACIÒN RADIOLÓGICA DE LA LESIÒN ÒSEA SOLITARIA IMAGENOLOGIA MEDICA UNIVERSIDAD HISPANOAMERICANA TUMORES ÓSEOS SE PRESENTAN POR RANGOS DE EDAD, PRINCIPALMENTE: MENORES DE 20 AÑOS 20 A 40 AÑOS MAYORES
VALORACIÒN RADIOLÓGICA DE LA LESIÒN ÒSEA SOLITARIA IMAGENOLOGIA MEDICA UNIVERSIDAD HISPANOAMERICANA TUMORES ÓSEOS SE PRESENTAN POR RANGOS DE EDAD, PRINCIPALMENTE: MENORES DE 20 AÑOS 20 A 40 AÑOS MAYORES
Incidental bone tumors are asymptomatic lesions that are. Incidental Bone Lesions. When to Refer to the Tumor Specialist
 Bulletin of the NYU Hospital for Joint Diseases 2012;70(4):235-40 235 Incidental Bone Lesions When to Refer to the Tumor Specialist LT Suezie Kim, M.D., M.C., U.S.N., Catherine N. Laible, M.D., Leon D.
Bulletin of the NYU Hospital for Joint Diseases 2012;70(4):235-40 235 Incidental Bone Lesions When to Refer to the Tumor Specialist LT Suezie Kim, M.D., M.C., U.S.N., Catherine N. Laible, M.D., Leon D.
SMALL ROUND BLUE CELL LESION OF BONE
 DISCLOSURE SMALL ROUND BLUE CELL LESION OF BONE Dr. Alistair Jordan University of South Alabama No financial support or endorsement OBJECTIVES Describe the more common small round cell lesions of bone
DISCLOSURE SMALL ROUND BLUE CELL LESION OF BONE Dr. Alistair Jordan University of South Alabama No financial support or endorsement OBJECTIVES Describe the more common small round cell lesions of bone
Review Course «Musculoskeletal Oncology» October 6, 2011 UNIKLINIK BALGRIST. Imaging of Bone and Soft Tissue. Tumors
 Imaging of Bone and Soft Tissue Tumors Approach from a radiologist s point of view Florian Buck Radiology Radio- Radio- Oncologist Oncologist Orthopedist Orthopedist Patient Management Oncologist Oncologist
Imaging of Bone and Soft Tissue Tumors Approach from a radiologist s point of view Florian Buck Radiology Radio- Radio- Oncologist Oncologist Orthopedist Orthopedist Patient Management Oncologist Oncologist
Musculoskeletal Sarcomas
 Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Disclosures. Giant Cell Rich Tumors of Bone. Outline. The osteoclast. Giant cell rich tumors 5/21/11
 Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay
 Review Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay Subbarao Kakarla 1,* 1 KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India Abstract
Review Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay Subbarao Kakarla 1,* 1 KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India Abstract
General Approach to Lytic Bone Lesions D. Lee Bennett, MD, MA, Georges Y. El Khoury, MD Appl Radiol. 2004;33(5)
") General Approach to Lytic Bone Lesions D. Lee Bennett, MD, MA, Georges Y. El Khoury, MD Appl Radiol. 2004;33(5) www.medscape.com Abstract and Introduction Abstract When interpreting musculoskeletal radiographs,
General Approach to Lytic Bone Lesions D. Lee Bennett, MD, MA, Georges Y. El Khoury, MD Appl Radiol. 2004;33(5) www.medscape.com Abstract and Introduction Abstract When interpreting musculoskeletal radiographs,
Pictorial Essay Benign and Malignant Bone Tumors: Radiological Diagnosis and Imaging Features
 Clinical Orthopedic Imaging Pictorial Essay Benign and Malignant Bone Tumors: Radiological Diagnosis and Imaging Features Katharina Grünberg, M.D.; Christoph Rehnitz, M.D.; Marc-André Weber, M.D., M.Sc.
Clinical Orthopedic Imaging Pictorial Essay Benign and Malignant Bone Tumors: Radiological Diagnosis and Imaging Features Katharina Grünberg, M.D.; Christoph Rehnitz, M.D.; Marc-André Weber, M.D., M.Sc.
The Radiology Assistant : Bone tumor A-G
 Bone tumor A-G Bone tumors and tumor-like lesions in alphabethic order Henk Jan van de Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor A-G Bone tumors and tumor-like lesions in alphabethic order Henk Jan van de Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Unusual location of bone sarcoma in children
 Unusual location of bone sarcoma in children Poster No.: C-1517 Congress: ECR 2014 Type: Educational Exhibit Authors: S. JERBI, A. Khalfalli, G. Abid, O. Bradai, N. chouchane, H. HAMZA; Mahdia/TN Keywords:
Unusual location of bone sarcoma in children Poster No.: C-1517 Congress: ECR 2014 Type: Educational Exhibit Authors: S. JERBI, A. Khalfalli, G. Abid, O. Bradai, N. chouchane, H. HAMZA; Mahdia/TN Keywords:
Common Primary Tumors of Bone
 Special Report Common Primary Tumors of Bone Primary bone tumors are a relatively rare occurrence, however, they can have serious deleterious consequences. Many possess the ability to degenerate into malignant
Special Report Common Primary Tumors of Bone Primary bone tumors are a relatively rare occurrence, however, they can have serious deleterious consequences. Many possess the ability to degenerate into malignant
ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE
 ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE Richard D. Lackman, MD FACS Director, Orthopaedic Oncology Center Cancer Institute Introduction In the evaluation of a patient with a bone tumor, there are several
ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE Richard D. Lackman, MD FACS Director, Orthopaedic Oncology Center Cancer Institute Introduction In the evaluation of a patient with a bone tumor, there are several
History. 33 y/o F with hx of palpable anterior tibial mass x 2 years, only painful with palpation
 History 33 y/o F with hx of palpable anterior tibial mass x 2 years, only painful with palpation Imaging Photo Album Patient also had a smaller lesion 1 cm proximal to this lesion, not seen radiographically.
History 33 y/o F with hx of palpable anterior tibial mass x 2 years, only painful with palpation Imaging Photo Album Patient also had a smaller lesion 1 cm proximal to this lesion, not seen radiographically.
Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation.
 Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation. Poster No.: C-1451 Congress: ECR 2012 Type: Educational Exhibit Authors: E. Barcina García,
Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation. Poster No.: C-1451 Congress: ECR 2012 Type: Educational Exhibit Authors: E. Barcina García,
Benign Tumors of Bone
 REVIEW ARTICLE Benign Tumors of Bone Subbarao K Padmshri Prof. Dr. Kakarla Subbara, Hyderabad, India. Benign tumors of bone are common while malignant tumors are rare. Benign tumors constitute about 75%
REVIEW ARTICLE Benign Tumors of Bone Subbarao K Padmshri Prof. Dr. Kakarla Subbara, Hyderabad, India. Benign tumors of bone are common while malignant tumors are rare. Benign tumors constitute about 75%
Skeletal Radiology. Solitary (unicameral) bone cyst. The fallen fragment sign revisited
 bone cyst. The fallen fragment sign revisited") Skeletal Radiol (1989) 18:261-265 Skeletal Radiology Solitary (unicameral) bone cyst The fallen fragment sign revisited S. Struhl, M.D., C. Edelson, M.D., H. Pritzker, M.D., L.P. Seimon, M.D., and H.D.
Skeletal Radiol (1989) 18:261-265 Skeletal Radiology Solitary (unicameral) bone cyst The fallen fragment sign revisited S. Struhl, M.D., C. Edelson, M.D., H. Pritzker, M.D., L.P. Seimon, M.D., and H.D.
Benign Fibro-osseous Lesions
 Benign Fibro-osseous Lesions Plus Vision is the art of seeing things invisible. Jonathan Swift 1667-1745 Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Benign Fibro-osseous Lesions A group of lesions
Benign Fibro-osseous Lesions Plus Vision is the art of seeing things invisible. Jonathan Swift 1667-1745 Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Benign Fibro-osseous Lesions A group of lesions
Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older
 Dr Brajesh Nandan Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older patients. Cancers of the breast, prostate,
Dr Brajesh Nandan Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older patients. Cancers of the breast, prostate,
Topics. Musculoskeletal Infection Extremities. Detection of Infection. Role of Imaging in Extremity Infection. Detection of Infection
 Topics Musculoskeletal Infection Extremities Nuttaya Pattamapaspong M.D. Department of Radiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand Role of imaging in extremity infection
Topics Musculoskeletal Infection Extremities Nuttaya Pattamapaspong M.D. Department of Radiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand Role of imaging in extremity infection
"X marks the spot": The skeletal manifestations of Langerhans cell histiocytosis in the paediatric age group
 "X marks the spot": The skeletal manifestations of Langerhans cell histiocytosis in the paediatric age group Poster No.: C-2847 Congress: ECR 2010 Type: Educational Exhibit Topic: Pediatric Authors: A.
"X marks the spot": The skeletal manifestations of Langerhans cell histiocytosis in the paediatric age group Poster No.: C-2847 Congress: ECR 2010 Type: Educational Exhibit Topic: Pediatric Authors: A.
USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors
 USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Outline Common intramedullary tumors Enchondroma
USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Outline Common intramedullary tumors Enchondroma
* I have no disclosures or any
 Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
A 76 year old male presented with sudden increase of dyspnoea on 15 November 2014, following a biopsy. A previous CXR was reviewed.
 Question 1 A 76 year old male presented with sudden increase of dyspnoea on 15 November 2014, following a biopsy. A previous CXR was reviewed. Imaging A CXR was performed on 28 May 2014. A CT of the chest
Question 1 A 76 year old male presented with sudden increase of dyspnoea on 15 November 2014, following a biopsy. A previous CXR was reviewed. Imaging A CXR was performed on 28 May 2014. A CT of the chest
Spectrum of clinical presentations
 Spectrum of clinical presentations Case History A 7-day-old male patient born full-term via uncomplicated vaginal delivery was seen for multiple erythematous red-brown purpuric lesions that were present
Spectrum of clinical presentations Case History A 7-day-old male patient born full-term via uncomplicated vaginal delivery was seen for multiple erythematous red-brown purpuric lesions that were present
A review of Tumoral lesions of the shoulder
 A review of Tumoral lesions of the shoulder Poster No.: P-0109 Congress: ESSR 2013 Type: Scientific Exhibit Authors: M. M. Milán Rodríguez, Á. E. Moreno Puertas, J. M. Giménez, 1 1 1 1 2 1 A. Rubio Fernández,
A review of Tumoral lesions of the shoulder Poster No.: P-0109 Congress: ESSR 2013 Type: Scientific Exhibit Authors: M. M. Milán Rodríguez, Á. E. Moreno Puertas, J. M. Giménez, 1 1 1 1 2 1 A. Rubio Fernández,
ORTHOPAEDIC TUMOURS DJM FRANTZEN 2012 AUGUST TUMOURS 1
 ORTHOPAEDIC TUMOURS DJM FRANTZEN 2012 AUGUST TUMOURS 1 PRINCIPLES STAGING WORKUP RADIOLOGY BIOPSY PROCEDURES CHEMOTHERAPY RADIOTHERAPY 2012 AUGUST TUMOURS 2 STAGING ENNEKING'S SURGICAL STAGES (ENNEKING)
ORTHOPAEDIC TUMOURS DJM FRANTZEN 2012 AUGUST TUMOURS 1 PRINCIPLES STAGING WORKUP RADIOLOGY BIOPSY PROCEDURES CHEMOTHERAPY RADIOTHERAPY 2012 AUGUST TUMOURS 2 STAGING ENNEKING'S SURGICAL STAGES (ENNEKING)
GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT
 Nagoya J. Med. Sci. 59. 151-157, 1996 CASE REPORTS GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT KEIJI SATO!, SHIGEKI YAMAMURA!, HISASHI IWATA!, HIDESHI SUGIURA 2, NOBUO NAKASHIMA 3 and TETSURO NAGASAKA
Nagoya J. Med. Sci. 59. 151-157, 1996 CASE REPORTS GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT KEIJI SATO!, SHIGEKI YAMAMURA!, HISASHI IWATA!, HIDESHI SUGIURA 2, NOBUO NAKASHIMA 3 and TETSURO NAGASAKA
Bone Imaging. Scopes. Objective. Part 1 : bone tumor. Important Factors in Diagnosis of Bone tumor. Part 2 : infection and joint disease
 Scopes Bone Imaging Part 1 : bone tumor Part 2 : infection and joint disease Jitsupa Wongsripuemtet, M.D. Radiology Department Siriraj Hospital Mahidol University Objective ให น กศ กษาแพทย สามารถแปลผลภาพทางร
Scopes Bone Imaging Part 1 : bone tumor Part 2 : infection and joint disease Jitsupa Wongsripuemtet, M.D. Radiology Department Siriraj Hospital Mahidol University Objective ให น กศ กษาแพทย สามารถแปลผลภาพทางร
Residents Section Pattern of the Month
 Residents Section Pattern of the Month Rana et al. Periosteal Reaction Residents Section Pattern of the Month Residents inradiology Rich S. Rana 1 Jim S. Wu Ronald L. Eisenberg Rana RS, Wu JS, Eisenberg
Residents Section Pattern of the Month Rana et al. Periosteal Reaction Residents Section Pattern of the Month Residents inradiology Rich S. Rana 1 Jim S. Wu Ronald L. Eisenberg Rana RS, Wu JS, Eisenberg
Bone/Osteoid Producing Lesions
 Chapter 2 Bone/Osteoid Producing Lesions Introduction There are many lesions that are associated with reactive new bone formation; this chapter predominantly covers those in which deposition of osteoid/bone
Chapter 2 Bone/Osteoid Producing Lesions Introduction There are many lesions that are associated with reactive new bone formation; this chapter predominantly covers those in which deposition of osteoid/bone
A Modified Lodwick-Madewell Grading System for the Evaluation of Lytic Bone Lesions
 Musculoskeletal Imaging Original Research Caracciolo et al. Evaluation of Lytic one Lesions Musculoskeletal Imaging Original Research Jamie T. Caracciolo 1 H. Thomas Temple 2 G. Douglas Letson 3 Mark J.
Musculoskeletal Imaging Original Research Caracciolo et al. Evaluation of Lytic one Lesions Musculoskeletal Imaging Original Research Jamie T. Caracciolo 1 H. Thomas Temple 2 G. Douglas Letson 3 Mark J.
Solitary Bone Cyst of the Lunate: A Case Report
 Cronicon OPEN ACCESS ORTHOPAEDICS Case Report Solitary Bone Cyst of the Lunate: A Case Report MihirDesai* and Shivanand Bandekar Department of Orthopedics, Goa Medical College, Goa, India *Corresponding
Cronicon OPEN ACCESS ORTHOPAEDICS Case Report Solitary Bone Cyst of the Lunate: A Case Report MihirDesai* and Shivanand Bandekar Department of Orthopedics, Goa Medical College, Goa, India *Corresponding
Case 8 Soft tissue swelling
 Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
Mousa Al-Abadi. Abd. Kharabsheh. Rand Abu Anzeh
 7 Mousa Al-Abadi Abd. Kharabsheh Rand Abu Anzeh 1 Recap The histological appearance of Giant cell tumor of bone shows only multi-nucleated giant cells. The histological appearance of Aneurysmal bone cyst
7 Mousa Al-Abadi Abd. Kharabsheh Rand Abu Anzeh 1 Recap The histological appearance of Giant cell tumor of bone shows only multi-nucleated giant cells. The histological appearance of Aneurysmal bone cyst
Advertisement. Osteochondroma
 Advertisement Osteochondroma An osteochondroma is a benign (noncancerous) tumor that develops during childhood or adolescence. It is an abnormal growth that forms on the surface of a bone near the growth
Advertisement Osteochondroma An osteochondroma is a benign (noncancerous) tumor that develops during childhood or adolescence. It is an abnormal growth that forms on the surface of a bone near the growth
FIBROUS CORTICAL DEFECT AND NON-OSSIFYING FIBROMA
 POSTGRAD. MED. J. (1965), 41, 672. FIBROUS CORTICAL DEFECT AND NON-OSSIFYING FIBROMA PETER G. BULLOUGH, M.B., Ch.B. JON WALIFY, F.R.C.S. Nuffield Department of Orthopaedic University of Oxford, Surgery,
POSTGRAD. MED. J. (1965), 41, 672. FIBROUS CORTICAL DEFECT AND NON-OSSIFYING FIBROMA PETER G. BULLOUGH, M.B., Ch.B. JON WALIFY, F.R.C.S. Nuffield Department of Orthopaedic University of Oxford, Surgery,
Paediatric post-traumatic osseous cystic lesion following a distal radial fracture
 Paediatric post-traumatic osseous cystic lesion following a distal radial fracture Joey Chan Yiing Beh 1*, Ehab Shaban Mahmoud Hamouda 1 1. Department of Diagnostic Imaging, KK Women's and Children's Hospital,
Paediatric post-traumatic osseous cystic lesion following a distal radial fracture Joey Chan Yiing Beh 1*, Ehab Shaban Mahmoud Hamouda 1 1. Department of Diagnostic Imaging, KK Women's and Children's Hospital,
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji
 Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
BIOH111. o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system
 BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 TEXTBOOK AND REQUIRED/RECOMMENDED
BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 TEXTBOOK AND REQUIRED/RECOMMENDED
UCLA UCLA Previously Published Works
 UCLA UCLA Previously Published Works Title Benign bone tumors Permalink https://escholarship.org/uc/item/7h86k14t Journal Radiologic Clinics of North America, 49(6) ISSN 0033-8389 Authors Motamedi, K Seeger,
UCLA UCLA Previously Published Works Title Benign bone tumors Permalink https://escholarship.org/uc/item/7h86k14t Journal Radiologic Clinics of North America, 49(6) ISSN 0033-8389 Authors Motamedi, K Seeger,
CASE PRESENTATION. Dr. Faseeh Shahab PGY3 Orthopaedic Resident, Khyber Teaching Hospital, Peshawar, PAKISTAN
 CASE PRESENTATION Dr. Faseeh Shahab PGY3 Orthopaedic Resident, Khyber Teaching Hospital, Peshawar, PAKISTAN CASE PRESENTATION - History Ms. SB, 30yo Afghan National Presented with 3 months history of Swelling
CASE PRESENTATION Dr. Faseeh Shahab PGY3 Orthopaedic Resident, Khyber Teaching Hospital, Peshawar, PAKISTAN CASE PRESENTATION - History Ms. SB, 30yo Afghan National Presented with 3 months history of Swelling
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Essential Dermatopathology. Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center
 Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Radiologic Pathologic Correlation of Intraosseous Lipomas. Tim Propeck 1, Mary Anne Bullard 1, John Lin 1, Kei Doi 2, William Martel 1
 Downloaded from www.ajronline.org by 148.251.232.83 on 04/10/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights reserved Radiologic Pathologic orrelation of Intraosseous
Downloaded from www.ajronline.org by 148.251.232.83 on 04/10/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights reserved Radiologic Pathologic orrelation of Intraosseous
GIANT CELL TUMOR OF LOWER END OF FEMUR IN A SKELETALLY IMMATURE-A RARE CASE
 GIANT CELL TUMOR OF LOWER END OF FEMUR IN A SKELETALLY IMMATURE-A RARE CASE *Surojit Mondal 1, Aniket Chowdhury 2 and Goutam Bandyopadhyay 3 1 Department of Orthopaedics, B.S.Medical College, Bankura,
GIANT CELL TUMOR OF LOWER END OF FEMUR IN A SKELETALLY IMMATURE-A RARE CASE *Surojit Mondal 1, Aniket Chowdhury 2 and Goutam Bandyopadhyay 3 1 Department of Orthopaedics, B.S.Medical College, Bankura,
The role of Imaging in Ewing sarcoma
 The role of Imaging in Ewing sarcoma Poster No.: P-0109 Congress: ESSR 2014 Type: Educational Poster Authors: D. Beomonte Zobel, C. Dell'atti, M. Bartocci, V. Martinelli, N. 1 2 2 2 1 1 1 2 Magarelli,
The role of Imaging in Ewing sarcoma Poster No.: P-0109 Congress: ESSR 2014 Type: Educational Poster Authors: D. Beomonte Zobel, C. Dell'atti, M. Bartocci, V. Martinelli, N. 1 2 2 2 1 1 1 2 Magarelli,
What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington
 What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington What s Do You Need To Know About Bone Pathology? Reactive/pseudosarcomatous
What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington What s Do You Need To Know About Bone Pathology? Reactive/pseudosarcomatous
Small lesions involving scalp and skull in pediatric age.
 Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/KR Keywords: Education and training, Education,
Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/KR Keywords: Education and training, Education,
Case Report Giant Cell Tumor of Bone: Documented Progression over 4 Years from Its Origin at the Metaphysis to the Articular Surface
 Volume 2016, Article ID 9786925, 5 pages http://dx.doi.org/10.1155/2016/9786925 Case Report Giant Cell Tumor of Bone: Documented Progression over 4 Years from Its Origin at the Metaphysis to the Articular
Volume 2016, Article ID 9786925, 5 pages http://dx.doi.org/10.1155/2016/9786925 Case Report Giant Cell Tumor of Bone: Documented Progression over 4 Years from Its Origin at the Metaphysis to the Articular
Lytic Lesion in the Distal Phalanx of the Hand
 Shafa Ortho J. 2015 February; 2(1):e441. Published online 2015 February 15. DOI: 10.5812/soj.441 Research Article Lytic Lesion in the Distal Phalanx of the Hand Khodamorad Jamshidi 1 ; Farid Najd Mazhar
Shafa Ortho J. 2015 February; 2(1):e441. Published online 2015 February 15. DOI: 10.5812/soj.441 Research Article Lytic Lesion in the Distal Phalanx of the Hand Khodamorad Jamshidi 1 ; Farid Najd Mazhar
Downloaded from by on 11/21/17 from IP address Copyright ARRS. For personal use only; all rights reserved
 Downloaded from www.ajronline.org by 46.3.196.1 on 11/21/17 from IP address 46.3.196.1. opyright RRS. For personal use only; all rights reserved T he scapula is a small bone in which many neoplasms can
Downloaded from www.ajronline.org by 46.3.196.1 on 11/21/17 from IP address 46.3.196.1. opyright RRS. For personal use only; all rights reserved T he scapula is a small bone in which many neoplasms can
Radiology Corner. Osteoid Osteoma
 Radiology Corner Osteoid Osteoma Guarantor: COL Timothy G. Sanders, MC, USAF (Ret.) Contributors: COL Timothy G. Sanders, USAF, MC, (Ret.); CAPT John P. Lichtenberger, USAF, MC; COL Les Folio, USAF, MC,
Radiology Corner Osteoid Osteoma Guarantor: COL Timothy G. Sanders, MC, USAF (Ret.) Contributors: COL Timothy G. Sanders, USAF, MC, (Ret.); CAPT John P. Lichtenberger, USAF, MC; COL Les Folio, USAF, MC,
Small lesions involving scalp and skull in pediatric age.
 Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/ Keywords: Education and training, Education,
Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/ Keywords: Education and training, Education,
ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN
 ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN Consultant Musculoskeletal Radiologist Royal National Orthopaedic Hospital Stanmore,UK. INTRODUCTION 2 INTRODUCTION 3 INTRODUCTION Spinal
ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN Consultant Musculoskeletal Radiologist Royal National Orthopaedic Hospital Stanmore,UK. INTRODUCTION 2 INTRODUCTION 3 INTRODUCTION Spinal
Medical Student Rotation Guide Tumor Service
 Medical Student Rotation Guide Tumor Service Overview Welcome to the medical student rotation on the Tumor service in the Department of Orthopaedic Surgery at Rush University Medical Center! We are excited
Medical Student Rotation Guide Tumor Service Overview Welcome to the medical student rotation on the Tumor service in the Department of Orthopaedic Surgery at Rush University Medical Center! We are excited
Fibrous Dysplasia in Children. Professor Nick Shaw Birmingham Children s Hospital, UK
 Fibrous Dysplasia in Children Professor Nick Shaw Birmingham Children s Hospital, UK Overview What is Fibrous Dysplasia? Clinical Presentations Endocrine Problems Skeletal Problems Treatment Options Fibrous
Fibrous Dysplasia in Children Professor Nick Shaw Birmingham Children s Hospital, UK Overview What is Fibrous Dysplasia? Clinical Presentations Endocrine Problems Skeletal Problems Treatment Options Fibrous
Case Report Intramedullary Chondrosarcoma of Proximal Humerus
 Hindawi Publishing Corporation Case Reports in Radiology Volume 2012, Article ID 642062, 7 pages doi:10.1155/2012/642062 Case Report Intramedullary Chondrosarcoma of Proximal Humerus Pratiksha Yadav, Dolly
Hindawi Publishing Corporation Case Reports in Radiology Volume 2012, Article ID 642062, 7 pages doi:10.1155/2012/642062 Case Report Intramedullary Chondrosarcoma of Proximal Humerus Pratiksha Yadav, Dolly
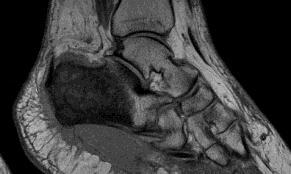
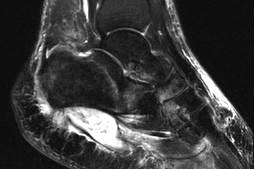
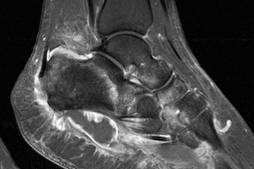
MRI of Pediatric Ankle and Foot. Mahesh Thapa, MD Associate Professor Seattle Children s University of Washington School of Medicine
 MRI of Pediatric Ankle and Foot Mahesh Thapa, MD Associate Professor Seattle Children s University of Washington School of Medicine Disclosures Under contract with Lippincott Williams and Wilkins (LWW)
MRI of Pediatric Ankle and Foot Mahesh Thapa, MD Associate Professor Seattle Children s University of Washington School of Medicine Disclosures Under contract with Lippincott Williams and Wilkins (LWW)
Medical Student Rotation Guide Tumor Service
 Medical Student Rotation Guide Tumor Service Overview Welcome to the medical student rotation on the Tumor service in the Department of Orthopaedic Surgery at Rush University Medical Center! We are excited
Medical Student Rotation Guide Tumor Service Overview Welcome to the medical student rotation on the Tumor service in the Department of Orthopaedic Surgery at Rush University Medical Center! We are excited
A comprehensive review of osseous Ewing sarcoma: clinical data, skeletal location and imaging features.
 A comprehensive review of osseous Ewing sarcoma: clinical data, skeletal location and imaging features. Poster No.: C-2233 Congress: ECR 2014 Type: Authors: Educational Exhibit R. Gil 1, P. Pereira 1,
A comprehensive review of osseous Ewing sarcoma: clinical data, skeletal location and imaging features. Poster No.: C-2233 Congress: ECR 2014 Type: Authors: Educational Exhibit R. Gil 1, P. Pereira 1,
Benign Fibrous Histiocytoma with Cystic Change of the Femur: a Case Report
 pissn 2384-1095 eissn 2384-1109 imri 2016;20:264-268 https://doi.org/10.13104/imri.2016.20.4.264 Benign Fibrous Histiocytoma with Cystic Change of the Femur: a Case Report Jung Ah Park, Sung Gyu Moon,
pissn 2384-1095 eissn 2384-1109 imri 2016;20:264-268 https://doi.org/10.13104/imri.2016.20.4.264 Benign Fibrous Histiocytoma with Cystic Change of the Femur: a Case Report Jung Ah Park, Sung Gyu Moon,
Section II Musculoskeletal Radiology
 Section II Musculoskeletal Radiology Figure 1 25. You are shown a noncontrast CT (Figure 1) of the thigh. What is the MOST LIKELY diagnosis? A. Synovial sarcoma B. Hemangioma C. Organizing hematoma D.
Section II Musculoskeletal Radiology Figure 1 25. You are shown a noncontrast CT (Figure 1) of the thigh. What is the MOST LIKELY diagnosis? A. Synovial sarcoma B. Hemangioma C. Organizing hematoma D.
MRI of the Knee: Part 4 - normal variants that may simulate disease. Mark Anderson, M.D. University of Virginia
 MRI of the Knee: Part 4 - normal variants that may simulate disease Mark Anderson, M.D. University of Virginia discuss the most common normal variants in the pediatric knee that may simulate pathology
MRI of the Knee: Part 4 - normal variants that may simulate disease Mark Anderson, M.D. University of Virginia discuss the most common normal variants in the pediatric knee that may simulate pathology
Plain Film CT. Principal Modality (2): Case Report # [] Date accepted: 15 March 2014
![Plain Film CT. Principal Modality (2): Case Report # [] Date accepted: 15 March 2014](/thumbs/89/100531147.jpg "Plain Film CT. Principal Modality (2): Case Report # [] Date accepted: 15 March 2014") Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): Plain Film CT Case Report # [] Submitted by: Dr. Jason E. Lally, M.D. Faculty reviewer: Dr. Naga Ramesh Chinapuvvula,
Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): Plain Film CT Case Report # [] Submitted by: Dr. Jason E. Lally, M.D. Faculty reviewer: Dr. Naga Ramesh Chinapuvvula,
Lower Extremity Alignment: Genu Varum / Valgum
 Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
The Skeletal System:Bone Tissue
 The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
MR Evaluation of Bone Marrow Disorders. Nisha Patel, MD
 MR Evaluation of Bone Marrow Disorders Nisha Patel, MD 1 Introduction Nearly all imaging modalities evaluate the marrow, which is a site of significant pathology Radiography Nuclear Medicine CT MR 2 Topics
MR Evaluation of Bone Marrow Disorders Nisha Patel, MD 1 Introduction Nearly all imaging modalities evaluate the marrow, which is a site of significant pathology Radiography Nuclear Medicine CT MR 2 Topics
A peculiar location of a rare bone tumor: sternal lipoma
 A peculiar location of a rare bone tumor: sternal lipoma Poster No.: P-0033 Congress: ESSR 2016 Type: Authors: Keywords: DOI: Scientific Poster Z. Akkaya, C. Uzun, S. Enon, G. Kocaman, G. Sahin; Ankara/TR
A peculiar location of a rare bone tumor: sternal lipoma Poster No.: P-0033 Congress: ESSR 2016 Type: Authors: Keywords: DOI: Scientific Poster Z. Akkaya, C. Uzun, S. Enon, G. Kocaman, G. Sahin; Ankara/TR
Primary Intraosseus Xanthoma Involving the Proximal Femur in a Normolipidemic Patient: A Case Report
 CASE REPORT Hip Pelvis 28(3): 182-186, 2016 http://dx.doi.org/10.5371/hp.2016.28.3.182 Print ISSN 2287-3260 Online ISSN 2287-3279 Primary Intraosseus Xanthoma Involving the Proximal Femur in a Normolipidemic
CASE REPORT Hip Pelvis 28(3): 182-186, 2016 http://dx.doi.org/10.5371/hp.2016.28.3.182 Print ISSN 2287-3260 Online ISSN 2287-3279 Primary Intraosseus Xanthoma Involving the Proximal Femur in a Normolipidemic
Department of Radiology, University of Szeged. Imaging of the skeleton
 Imaging of the skeleton Methods of examination: plain x-ray (radiography, densitometry) x-ray with contrast material (fistulography, angiography) ultrasound (b-mode, Doppler, color, duplex) computed tomography
Imaging of the skeleton Methods of examination: plain x-ray (radiography, densitometry) x-ray with contrast material (fistulography, angiography) ultrasound (b-mode, Doppler, color, duplex) computed tomography
Due in Lab. Due next week in lab - Scientific America Article Select one article to read and complete article summary
 Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
Intraosseous lipoma of the talus
 Intraosseous lipoma of the talus Shigeki Maruyama, M.D. 1, Tetsuji Yamamoto, M.D (!). 2, Masataka Hashimura, M.D. 1, and Nobuhiro Ohsaki, M.D. 1, Toshihiro Akisue, M.D. 2, Shinichi Yoshiya, M.D 2 1 Department
Intraosseous lipoma of the talus Shigeki Maruyama, M.D. 1, Tetsuji Yamamoto, M.D (!). 2, Masataka Hashimura, M.D. 1, and Nobuhiro Ohsaki, M.D. 1, Toshihiro Akisue, M.D. 2, Shinichi Yoshiya, M.D 2 1 Department