CSIM/ACP Annual Meeting Banff AB October Scott McKee MD MPH FACP
|
|
|
- Shannon Curtis
- 5 years ago
- Views:
Transcription

1 CSIM/ACP Annual Meeting Banff AB October 2018 Scott McKee MD MPH FACP
2
3 Scott McKee MD MPH FACP General Internal Medicine and Critical Care Shuswap Hospital, Salmon Arm, BC UBC Department of Medicine The diagnostic approach/definition Evidence-based management strategies What is the role of steroids?
4 The diagnostic approach: THINK about it Evidence-based management strategies: Give fluids and antibiotics early What is the role of steroids? Try it when everything else isn t working...
5 Temp Pulse Respirations White count
6
7 Proposed in Was revalidated in the 2003 International Sepsis Definitions Conference -Ultimately revamped in 2016 (SEPSIS-3)
8 Mervyn Singer,MD, FRCP; Clifford S. Deutschman, MD, MS; ChristopherWarren Seymour,MD, MSc; Manu Shankar-Hari, MSc,MD, FFICM; Djillali Annane,MD, PhD; Michael Bauer, MD; Rinaldo Bellomo, MD; Gordon R. Bernard, MD; Jean-Daniel Chiche,MD, PhD; Craig M. Coopersmith, MD; Richard S. Hotchkiss, MD; Mitchell M. Levy, MD; John C. Marshall, MD; Greg S. Martin, MD, MSc; StevenM. Opal, MD; Gordon D. Rubenfeld, MD, MS; Tomvan der Poll, MD, PhD; Jean-Louis Vincent,MD, PhD; Derek C. Angus, MD, MPH
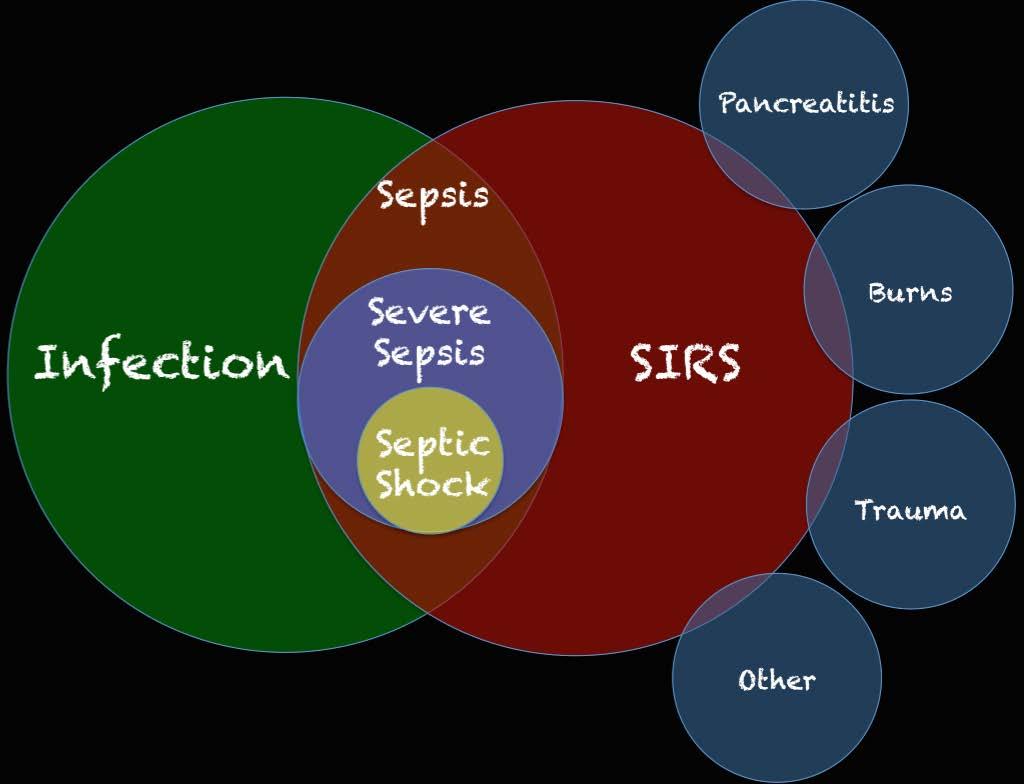
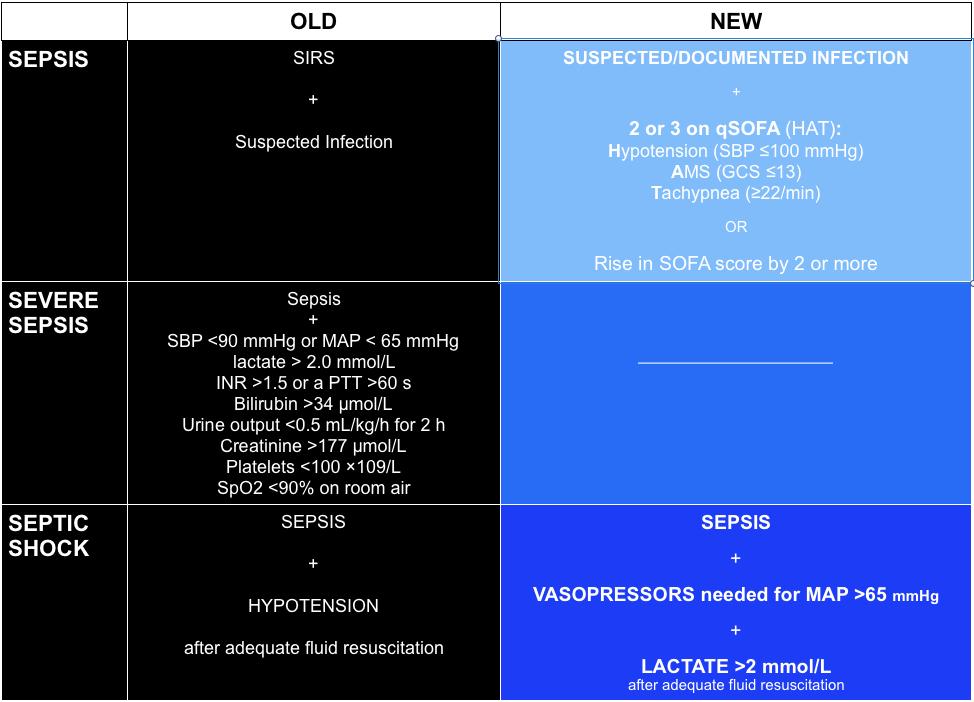
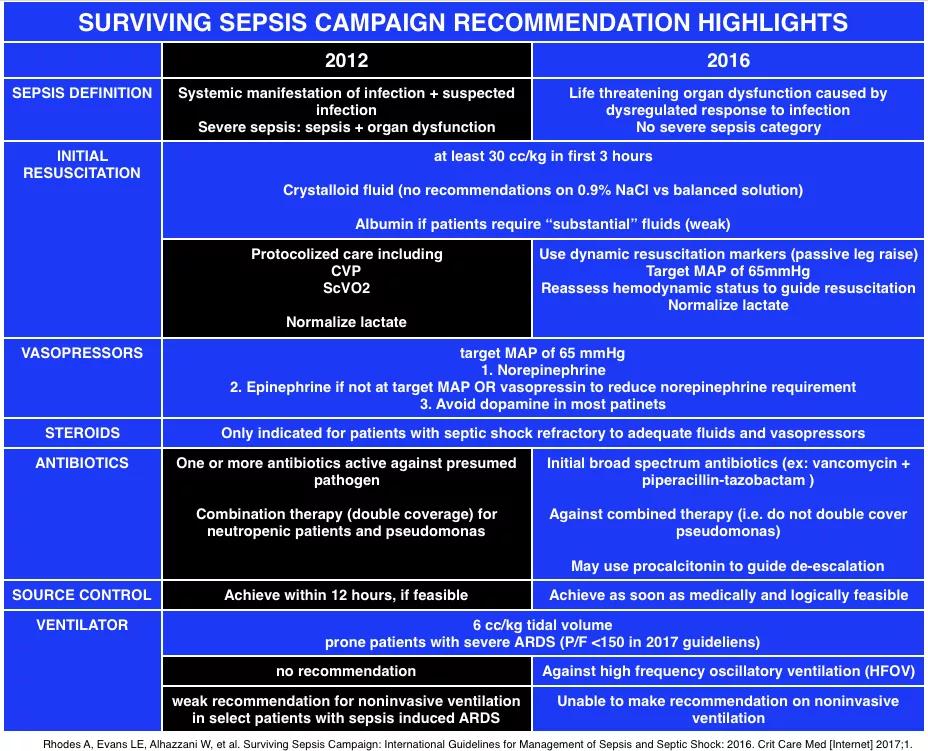
9 Limitations of previous definitions included an excessive focus on inflammation, the misleading model that sepsis follows a continuum through severe sepsis to shock, and inadequate specificity and sensitivity of the systemic inflammatory response syndrome (SIRS) criteria. Multiple definitions and terminologies are currently in use for sepsis, septic shock, and organ dysfunction, leading to discrepancies in reported incidence and observed mortality. The task force concluded the term severe sepsis was redundant.
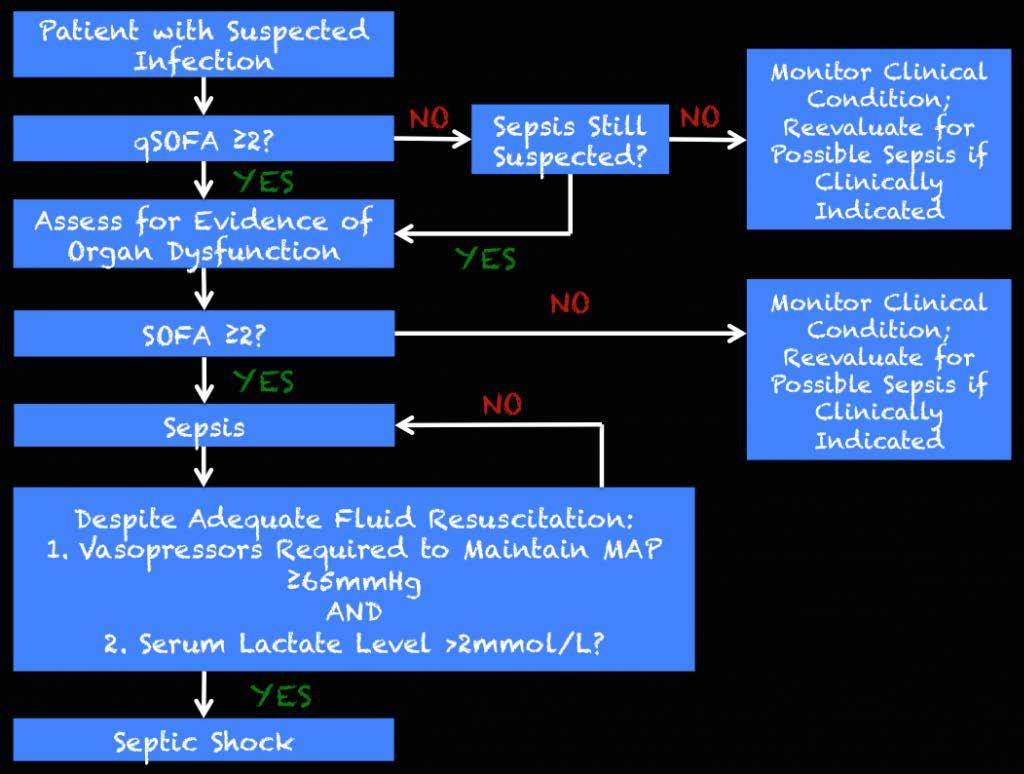
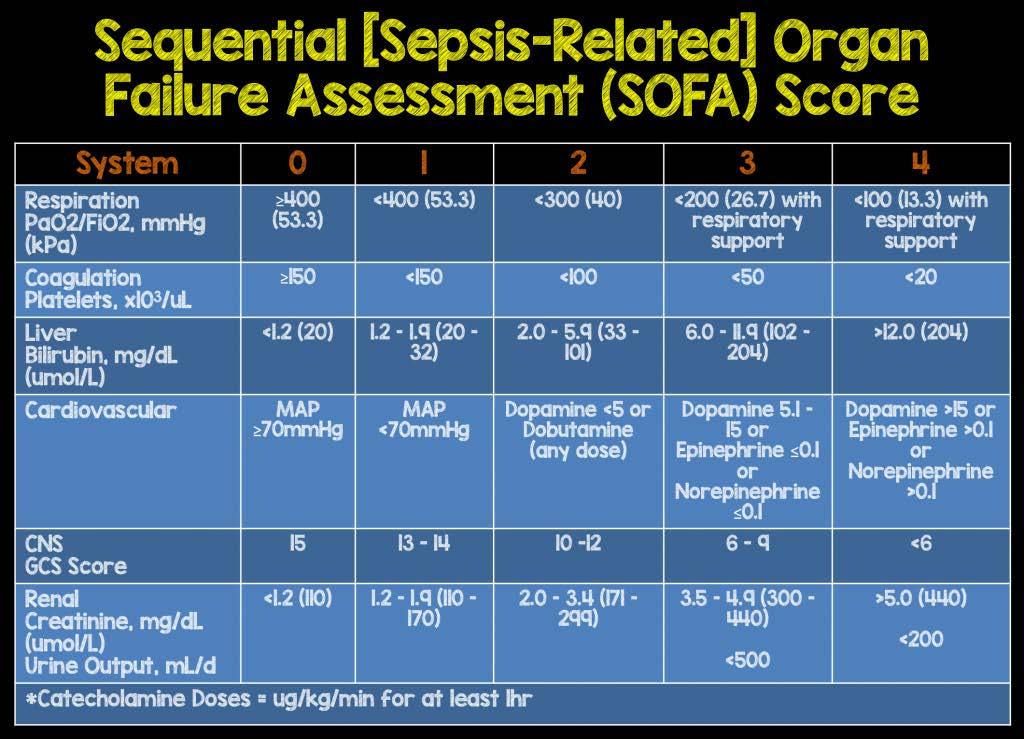
10 - Sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. - Organ dysfunction can be represented by an increase in the Sequential [Sepsis-related]Organ Failure Assessment (SOFA) score of 2 points or more, which is associated with an in-hospital mortality greater than 10%.
11 - Septic shock can be clinically identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and serum lactate level greater than 2 mmol/l (>18 mg/dl) in the absence of hypovolemia.
12 CONCLUSIONS AND RELEVANCE: These updated definitions and clinical criteria should replace previous definitions, offer greater consistency for epidemiologic studies and clinical trials, and facilitate earlier recognition and more timely management of patients with sepsis or at risk of developing sepsis.
13
14 Lung: Respiration PaO 2 /FiO 2 >400 (0 points) PaO 2 /FiO to 400 (1 point) PaO 2 /FiO (2 points) PaO 2 /FiO to 200 with ventilatory support (3 points) PaO 2 /FiO with ventilatory support (4 points) Coagulation: Platelets >150 x10 3 /mm 3 (0 points) 101 to 150 x10 3 /mm 3 (1 point) 51 to 100 x10 3 /mm 3 (2 points) 21 to 50 x10 3 /mm 3 (3 points) 20 x10 3 /mm 3 (4 points) Liver: Bilirubin <1.2 mg/dl (20 mcmol/l) (0 points) 1.2 to 1.9 mg/dl (20 to 32 mcmol/l) (1 point) 2 to 5.9 mg/dl (33 to 101 mcmol/l) (2 points) 6 to 11.9 mg/dl (102 to 204 mcmol/l) (3 points) >12 mg/dl (>204 mcmol/l) (4 points) Cardiovascular: Blood pressure Hypotension absent (0 points) Mean arterial pressure <70 mmhg (1 point) On dopamine 5 mcg/kg/min or any dobutamine (2 points) On dopamine >5 mcg/kg/min, epinephrine 0.1 mcg/kg/min or norepinephrine 0.1 mcg/kg/min (3 points) On dopamine >15 mcg/kg/min or epinephrine >0.1 mcg/kg/min or norepinephrine >0.1 mcg/kg/min (4 points) Brain: Glasgow coma score 15 (0 points) 13 to 14 (1 point) 10 to 12 (2 points) 6 to 9 (3 points) <6 (4 points) Kidney: Renal function Creatinine <1.2 mg/dl (110 mcmol/l) (0 points) Creatinine 1.2 to 1.9 mg/dl (110 to 170 mcmol/l) (1 point) Creatinine 2 to 3.4 mg/dl (171 to 299 mcmol/l) (2 points) Creatinine 3.5 to 4.9 mg/dl (300 to 440 mcmol/l) or urine output 200 to 500 ml/day (3 points) Creatinine >5 mg/dl (440 mcmol/l) or urine output <200 ml/day (4 points)

15
16 Initial resuscitation IVF and rate Vasopressor use Source Control identification Antimicrobials Steroids Blood products Mechanical Ventilation Sedation/Bicarb/Glucose control/rrt DVT prophylaxis Nutrition Goals of Care

17 ABCs IV Access Investigations: -All the usual, PLUS: Cultures and serum lactate Maybe procalcitonin Consider the Zebra: immunosuppressed, nosocomial, fungal, splenectomy, hardware Goal: within 1 hour
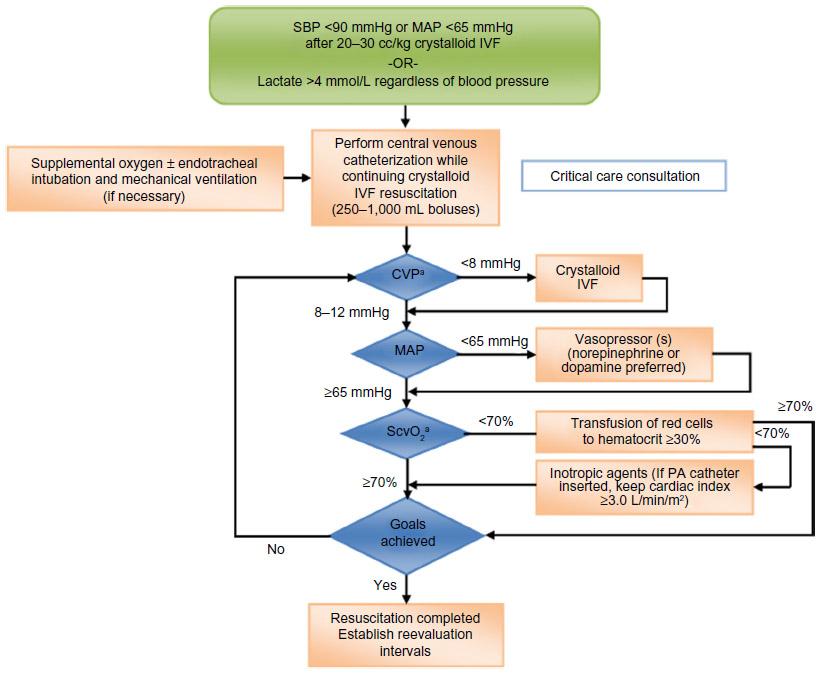
18 30ml/kg crystalloid, minimum 1L, in 3 hours No hetastarches or hypertonic saline Albumin a weak (2b) recommendation Consider echo (eval other causes of hypotension) Goal is lactate clearance and normotension (MAP > 65) (ScvO2, CVP, discarded) REASSESS FREQUENTLY
19
20 Administer within 1 hour for sepsis or septic shock Consider all access options: IO, Port-A-Cath, IM (i.e. don t delay if periph access difficult) Broad-spectrum, consider double coverage for shock De-escalate asap 7-10 days duratiion adequate for most (weak recommendation)
21 Begins with history and physical Appropriate imaging Invasive procedures (aspiration, BAL, I&D, hardware removal) Prioritize control asap (<6 hours preferred)
22 Those failing IVF or in pulmonary edema Norepi 1st choice but consider the clinical scenario Vasopressin, epinephrine, phenylephrine, dopamine OK Dobutamine if low CO Prepare to change if arrhythmias, or aggravated hypotension Arterial line REASSESS FREQUENTLY
23 -If endpoints not met by initial measures. Hydrocortisone 200mg/day IV No role for stim testing or ACTH administration
24 Suggested transfusion threshold 70mg/L No to EPO, empiric FFP Suggested platelet transfusion threshold = if bleeding risk 50 if bleeding,surgery
25 Just say no Numerous IVIG preparations available
26 LTV Strategy Keep plateau pressures <30 cm H2O Weak recommendations: Higher PEEP Recruitment maneuvers Go Prone (P/F <150 Limit paralysis <48 hrs No to Swans/beta agonists/ Yes to daily wean trials, elevated HOB, conservative IVF
27 No NaCO3 for ph >7.15 (or probably any ph) Protocolized glucose control targeting glucose at 180 mg/dl (10.0 mmol/l Dialyze for firm indications (not for oliguria or just because )
28 Just say yes. UFH >> mechanical PPI or H2B if bleeding risk factors present (MV > 48 hrs and coagulopathy)
29 Avoid if patient can be fed enterally Avoid in the first 7 days Avoid Omega-3-fatty acids, selenium/arginine/glutamine (?carnitine)
30 Start early and make it a priority
31
32 32 y/o M h/o TBI (remote) and resultant seizures. Complains of 1 week of cough, worsening pleuritic chest pain. Remote bioavr for endocarditis. Upon presentation to ED, T = 39.1 ; R = 24 ; P = 110 ; BP = 124 / 76; SPO2 89% 2L Decreased breath sounds on right base with crackles throughout left side Chemistry unremarkable; Lactate 2.4 WBC 16.5; 75% segs; 10% bands

33
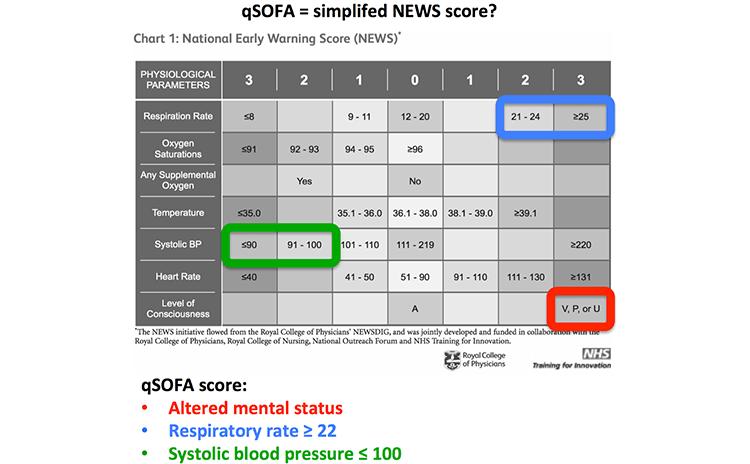
34 SIRS = 4 + infection source = sepsis qsofa = 1-2 = 6% risk of bad outcome SOFA = 1+??...more data needed.
35 What is your admit diagnosis? Pneumonia? Pleural effusion? Sepsis? Severe sepsis?
36
37 71 yo female with progressive SOB x 3 days. Also c/o small heel ulcer x 1 year, managed by WOC. On 10L O2 in triage. A&O but distressed. T = 37.1, P = 110, RR = 26 BP 84/66 MAP = 75 LAB: WBC 11, Plts 425, LFTs 2x normal, Tbili = 24, Creat 188 (baseline 120). Lactate = 5.2. ABG = 7.46/35/74 on 50% FiO2

38

39
40 SIRS = 2 qsofa = 2 SOFA = = 4
41 Lung: Respiration PaO 2 /FiO 2 >400 (0 points) PaO 2 /FiO to 400 (1 point) PaO 2 /FiO (2 points) PaO 2 /FiO to 200 with ventilatory support (3 points) PaO 2 /FiO with ventilatory support (4 points) Coagulation: Platelets >150 x10 3 /mm 3 (0 points) 101 to 150 x10 3 /mm 3 (1 point) 51 to 100 x10 3 /mm 3 (2 points) 21 to 50 x10 3 /mm 3 (3 points) 20 x10 3 /mm 3 (4 points) Liver: Bilirubin <1.2 mg/dl (20 mcmol/l) (0 points) 1.2 to 1.9 mg/dl (20 to 32 mcmol/l) (1 point) 2 to 5.9 mg/dl (33 to 101 mcmol/l) (2 points) 6 to 11.9 mg/dl (102 to 204 mcmol/l) (3 points) >12 mg/dl (>204 mcmol/l) (4 points) Cardiovascular: Blood pressure Hypotension absent (0 points) Mean arterial pressure <70 mmhg (1 point) On dopamine 5 mcg/kg/min or any dobutamine (2 points) On dopamine >5 mcg/kg/min, epinephrine 0.1 mcg/kg/min or norepinephrine 0.1 mcg/kg/min (3 points) On dopamine >15 mcg/kg/min or epinephrine >0.1 mcg/kg/min or norepinephrine >0.1 mcg/kg/min (4 points) Brain: Glasgow coma score 15 (0 points) 13 to 14 (1 point) 10 to 12 (2 points) 6 to 9 (3 points) <6 (4 points) Kidney: Renal function Creatinine <1.2 mg/dl (110 mcmol/l) (0 points) Creatinine 1.2 to 1.9 mg/dl (110 to 170 mcmol/l) (1 point) Creatinine 2 to 3.4 mg/dl (171 to 299 mcmol/l) (2 points) Creatinine 3.5 to 4.9 mg/dl (300 to 440 mcmol/l) or urine output 200 to 500 ml/day (3 points) Creatinine >5 mg/dl (440 mcmol/l) or urine output <200 ml/day (4 points)
42 Sepsis? Septic shock? ARDS? Something else?
43 EKG = NSR with new anterolat Q waves Troponin I = 4.7 BNP = 3800 Bedside echo: global LV dysfunction with hypervolemia and congestive hepatopathy Admitting Dx: ischemic CM
44 Sepsis care, pre-2001: 1. recognize it early. 2. give antibiotics, fluids, and vasopressors if needed. Monitor attentively. Sepsis care, : See above. (Do it better.)

45
46
47
48
49
50

51
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sepsis 3.0: pourquoi une nouvelle définition?
 Sepsis 3.0: pourquoi une nouvelle définition? Jean-Daniel Chiche, MD PhD MICU & Dept Infection, Immunity & Inflammation Hôpital Cochin & Institut Cochin, Paris-F JAMA 2016; 315(8) WHY 1991 & 2001 Definitions:
Sepsis 3.0: pourquoi une nouvelle définition? Jean-Daniel Chiche, MD PhD MICU & Dept Infection, Immunity & Inflammation Hôpital Cochin & Institut Cochin, Paris-F JAMA 2016; 315(8) WHY 1991 & 2001 Definitions:
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Basics from anatomy and physiology classes Local tissue reactions
 Septicaemia & SIRS Septicaemia is a life-threatening condition that arises when the physical reaction to an infection, causes damage to tissue and organs Basics from anatomy and physiology classes Local
Septicaemia & SIRS Septicaemia is a life-threatening condition that arises when the physical reaction to an infection, causes damage to tissue and organs Basics from anatomy and physiology classes Local
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Sepsis-3: clarity or confusion
 Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Rodolfo Sbrojavacca SOC Medicina d' Urgenza - Pronto Soccorso AOU di Udine
 Rodolfo Sbrojavacca SOC Medicina d' Urgenza - Pronto Soccorso AOU di Udine In Italy, Spain, the UK, France and the USA, a mean of 88% of interviewees had never heard of the term sepsis and of people who
Rodolfo Sbrojavacca SOC Medicina d' Urgenza - Pronto Soccorso AOU di Udine In Italy, Spain, the UK, France and the USA, a mean of 88% of interviewees had never heard of the term sepsis and of people who
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center
 UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Sepsis as Seen by the CMO. Randy C. Roth, MD Chief Medical Officer
 Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Chapter 5: Sepsis Stephen Lo
 Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Is nosocomial infection the major cause of death in sepsis?
 Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Surviving Sepsis Campaign Updates
 Surviving Sepsis Campaign Updates Emily Kauffman, DO, MPH OSU Wexner Medical Center DISCLOSURE STATEMENT It is the policy of the American Osteopathic Association (AOA) and Ohio University Heritage College
Surviving Sepsis Campaign Updates Emily Kauffman, DO, MPH OSU Wexner Medical Center DISCLOSURE STATEMENT It is the policy of the American Osteopathic Association (AOA) and Ohio University Heritage College
Effectively Managing Sepsis Denials
 Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Sepsis - A Year in Transition
 Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of
 Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
 Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Looking for sepsis. Sepsis: Update. Prevalence of High Profile Dzs. Screening and risk stratification. Mortality of High Profile Diseases
 Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania
 AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Sepsis: Mitigating Denials Amid Definition Disparity
 Sepsis: Mitigating Denials Amid Definition Disparity White Paper - April 2017 Sepsis Criteria at a Glance The Society of Critical Care Medicine (SCCM) met in 2016 to update the definition of sepsis. During
Sepsis: Mitigating Denials Amid Definition Disparity White Paper - April 2017 Sepsis Criteria at a Glance The Society of Critical Care Medicine (SCCM) met in 2016 to update the definition of sepsis. During
Sepsis: Update on Diagnosis, Evaluation and Management
 Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
The Management of Septic Shock
 The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
Critical Care Medicine Update for Non-Intensivists 2015
 27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
TERMINOLOGY SIRS 10/30/2014 SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU
 Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
12/12/2017. Notice. Sepsis is defined as life-threatening organ dysfunction due to a dysregulated host response to infection.
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis Update Allina Critical Care Conference February 28, 2018
 Sepsis Update Allina Critical Care Conference February 28, 2018 Sandy Fritzlar, MD Medical Director of the Allina Sepsis Program Emergency Care Consultants OBJECTIVES A brief HISTORY of Sepsis Understand
Sepsis Update Allina Critical Care Conference February 28, 2018 Sandy Fritzlar, MD Medical Director of the Allina Sepsis Program Emergency Care Consultants OBJECTIVES A brief HISTORY of Sepsis Understand
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
9/15/2017. Joyce Turner RN Director of Clinical Program Development
 Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Welcome! While we wait, please open PollEv.com/jhhicu012
 Welcome! While we wait, please open PollEv.com/jhhicu012 Login username jhhicu012 Password jhhicupoll OR Text JHHICU012 to 0427541357 once to join the poll response and be able to answer polls by SMS Same
Welcome! While we wait, please open PollEv.com/jhhicu012 Login username jhhicu012 Password jhhicupoll OR Text JHHICU012 to 0427541357 once to join the poll response and be able to answer polls by SMS Same
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,