Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
|
|
|
- Cathleen Strickland
- 5 years ago
- Views:
Transcription
1 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic
2 Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative morbidity Recurrent MR/AR?unnecessary repairs Benefits Reduce mortality Avoid LV damage/chf Avoid atrial fibrillation Improve functional class Valve lesion Load Indication Mitral regurgitation Volume Symptoms, LV size, AF, PHT Aortic stenosis Pressure Symptoms,?valve gradients
;")

3 The controversy of early surgery in MR Prevalence: 23 35yo 11% (93% mild MR); 65 yrs 30% (27% moderate severe) Cooper HA, Gersh BJ Am Heart J 1998; 135:
4 %postop LVD %postop LVD LOAD AND FUNCTION IN VALVULAR HEART DISEASE Are standard resting criteria sufficient? < >60 Preoperative EF 0 < >45 Preoperative LVSD Matsumura et al JACC 2003; 42:
5 Pre-operative MR severity
6 Pre-operative LV function
7 Pre-operative LV function
8 Standard resting criteria Criterion Reference LVESD >4.5 cm; LVEF >60% Sarano. Circulation 1994 ESVI > 60 ml/m2 Bonow. Am J Med 1980 LV dp/dt < 1343 mmhg Pai. Circulation 1990 ESWS > 195 mmhg Zile. Am J Cardiol 1985 ESWS/ESVI < 2.6 Carabello. Circulation 1986 Peak elastance slope of LV end systolic P-V loops Starling. JACC 1993
9 Non-standard LV assessment in MR Measurement of contractile reserve - Ejection fraction - Tissue velocity imaging/strain Myocardial tissue characterization - Prediction of fibrosis - Prediction of post-operative outcome



10 POST-EX EF = 75% LOAD AND FUNCTION IN VALVULAR HEART DISEASE Accuracy of predictors of post-op LV function % Sensitivity Specificity all p < REST EF = 60% ESVI EX EF EX EF LV dp/dt >25 l/m 2 <68% <4% <1000
11 EF progress and CR Surgical patients EF(%) EF(%) Pre op p=0.006 p< mo post op p=0.01 p< mo post op 24 to 36 mo post op Follow up EF in surgically treated CR+ and CR- patients. Comparison of post-up EF between CR+ and CR- patients at 6, 12 and 24 to 36 months resulted in. p=0.008 p=0.16 and, p=0.02 p=0.008 p< CR+ CR p=0.20 p=0.65 p=0.83 p=0.20 Baseline 12 mo 24 to 36 mo CR+ CR- Follow up EF in medically treated CR+ and CR- pts. Comparison of follow-up EF between CR+ and CRpts at 12 and 24 to 36 months resulted in p=0.37 and p=0.06. Lee et al, Heart 2004
12 Functional capacity (mets) 1.2 LOAD AND FUNCTION IN VALVULAR HEART DISEASE Fig 4: Survival free from cardiac events in CR, survival and functional capacity surgically treated CR+ and CR- patients CR Log rank = 4.69 p = 0.03 CR No at Risk CR CR Time from surgery (months) Baseline p = 0.05 Follow up Event-free survival post MVR Exercise capacity (medical treatment) Lee et al, Heart 2004
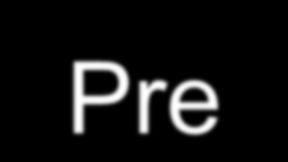
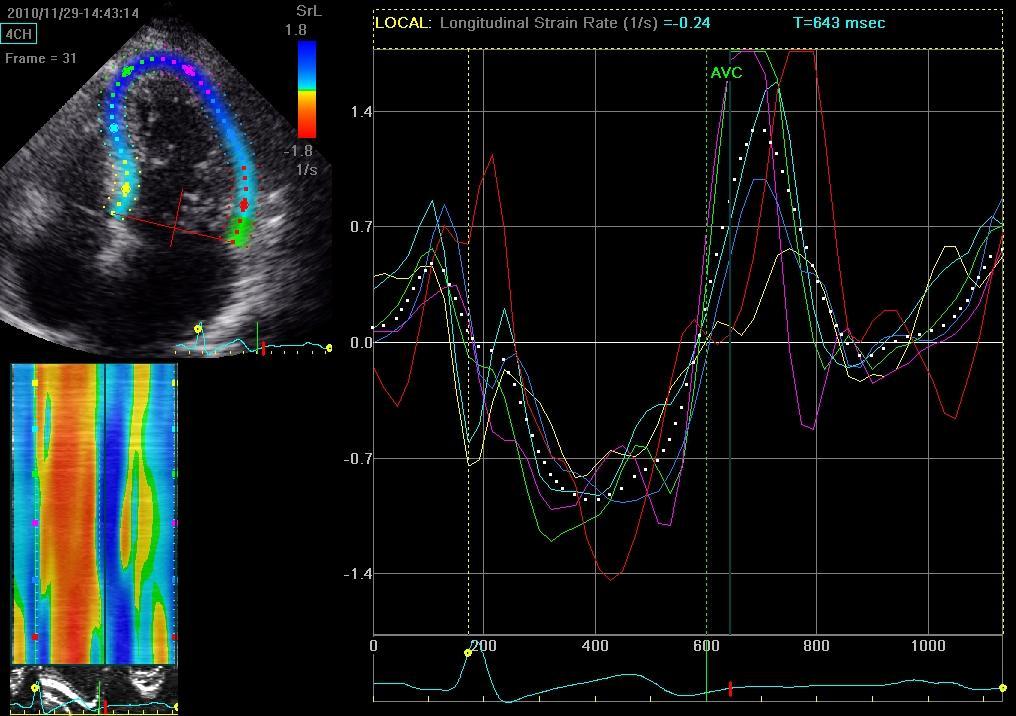
13 Pre-operative LV deformation
14 SR and strain as a function of LV diameter A theoretical model of strain rate and strain as a function of ventricular diameter and its relationship with stroke volume. Marciniak A et al. Eur Heart J 2007;28:
15 Asymptomatic MR and Strain Rate Imaging 32 asymptomatic MR pts (NYHA class I to II) Normal Controls (n=22) ExEcho (ΔEF>4%) CR+ (n=22) CR- (n=10) SRI (rest, long axis) ESS (%) SR (1/s)




16 Strain rate CR+ Strain CR Strain rate CR- SR= -1.45/s Strain CR- ESS= - 33% ESS= - 9% SR= /s
17 SR(1/s) ESS(%) LOAD AND FUNCTION IN VALVULAR HEART DISEASE Strain rate and Contractile reserve CR- CR+ Normal Controls p=0.008 p=0.95 p= p < p = 0.06 p < Strain rate End-systolic strain Lee R. Am J Cardiol 2004
18 Sensitivity percent % LOAD AND FUNCTION IN VALVULAR HEART DISEASE Predictors of Contractile Reserve ROC curves (AUC) 0.4 Peak SR Fx capacity LVESVexe specificity SR (1/s) Fx capacity (mets) LVESVexe (mls) SR Ex Cap 6.1 METS LVESV exe 43 mls

19 Non-standard LV assessment in MR Measurement of contractile reserve - Ejection fraction - Tissue velocity imaging/strain Myocardial tissue characterization - Prediction of fibrosis - Prediction of post-operative outcome
 & normal resting LVEF ExEcho ( EF>4%)")
 No")
20 37 minimally symptomatic MR pts (NYHA I to II) & normal resting LVEF ExEcho ( EF>4%) CR+ (n=25) CR- (n=12) MV Surgery (n=15) Myocardial Biopsy Fibrosis (n=5) No fibrosis (n=10)




21 DOPPLER MYOCARDIAL IMAGING IN VALVULAR HEART DISEASE Myocardial strain and fibrosis 1.3 S S -1
22 ESS (%) CVIBpw (db) LOAD AND FUNCTION IN VALVULAR HEART DISEASE Predictors of Fibrosis p < p < Fibrosis No fibrosis
23 Baseline between pts with and without fibrosis Fibrosis + Fibrosis - bsr -0.98± ±0.27 bess ± ±3.28 b2sr -0.93± ±0.20 b2ess ± ±2.86 Ave_CVIB_aplax 3.31± ±3.89 bascib_mean ± ±6.989 pwcib_mean ± ±8.609
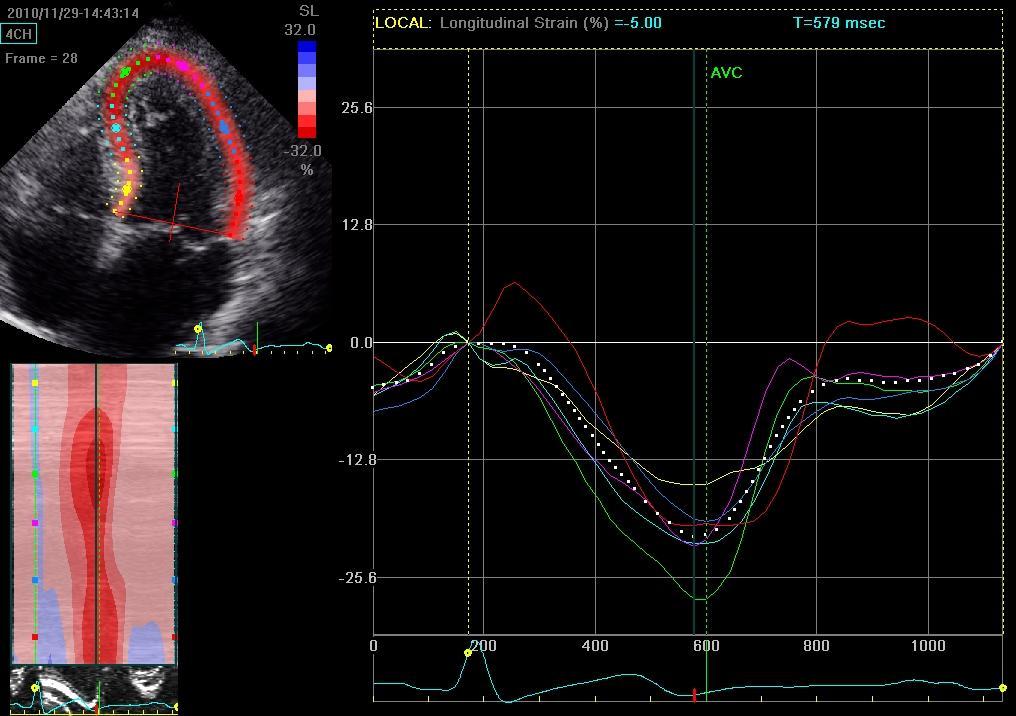
24 Study Design 73 minimally symptomatic pts (NYHA I to II) with > 3+ Mitral Regurgitation & normal resting LVEF (62 ±5%) 28 females; Age 64 ± 10 years CAD, co-existing MS or aortic valve dis and previous cardiac surgery excluded Exercise Stress Echo Contractile reserve = EF>4% SRI (TVI and 2D-SRI) IB Medical FU (n=30) MV Surgery (n=43) 8±5 months Myocardial biopsy (n=25) F/U Echocardiogram SRI (TVI and 2D-SRI) Fibrosis (n=9) No fibrosis (n=16) LV preservation (n=57) LV deterioration (n=16) Mean deterioration -8±6%
25 Baseline SRI in pts with normal and impaired LV at F/U N LV function on follow-up LV impairment on follow-up TVI SR 2D-SR /s % 0 TVI ESS 2D-ESS P< P< P< P< Hanekom L. AHA 2006
26 Baseline SRI in medical pts with preserved LV Baseline Follow-up TVI SR 2D-SR /s % 0 TVI ESS 2D-ESS All p=ns Hanekom L. AHA 2006
 End systolic strain (ESS) TVI SR AUC=0.89 Cut-off<-1.1/s TVI ESS AUC=0.84 Cut-off<-17% 2D SR AUC=0.90 Cut-off<-1.0/s 2D ESS AUC=0.")
27 ROC curves for prediction of impaired LV at F/U TVI SRI Peak systolic strain rate (SR) End systolic strain (ESS) 2D Strain Peak systolic strain rate (SR) End systolic strain (ESS) TVI SR AUC=0.89 Cut-off<-1.1/s TVI ESS AUC=0.84 Cut-off<-17% 2D SR AUC=0.90 Cut-off<-1.0/s 2D ESS AUC=0.84 Cut-off<-17%
28 Accuracy for prediction of impaired LV at F/U % 100 Sensitivity Specificity Contr Reserve SR<-1.1/s ESS<-17% 2D-SR<-1.0/s 2D-ESS<-17% Hanekom L. AHA 2006
29 Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative morbidity Recurrent MR/AR?unnecessary repairs Benefits Reduce mortality Avoid LV damage/chf Avoid atrial fibrillation Improve functional class Valve lesion Load Indication Mitral regurgitation Volume Symptoms, LV size, AF, PHT Aortic stenosis Pressure Symptoms,?valve gradients

30 Indications for surgery in common valve lesions LVH and LVD are markers of increased risk could LV strain?




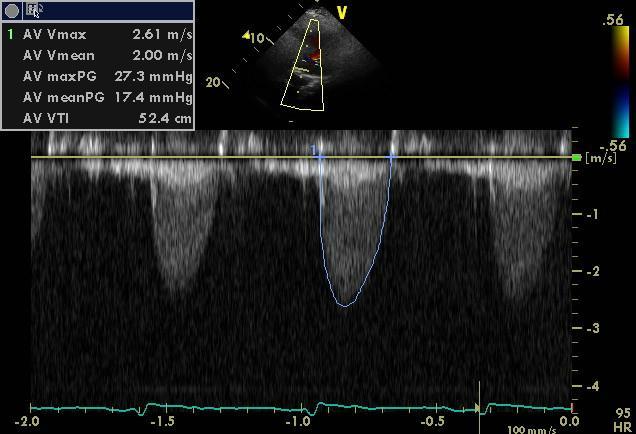
31 Changes in myocardial function with AVR Max. Grad.: 75 mmhg Mean Grad.: 39 mmhg AVA= 0.8 cm² Max. Grad.: 17 mmhg Mean Grad.: 8 mmhg AVA= 2.1 cm² Before AVR After AVR LV EDV: 154 ml LV ESV: 71 ml LV EF: 58 % LV EDV: 169 ml LV ESV: 65 ml LV EF: 62%




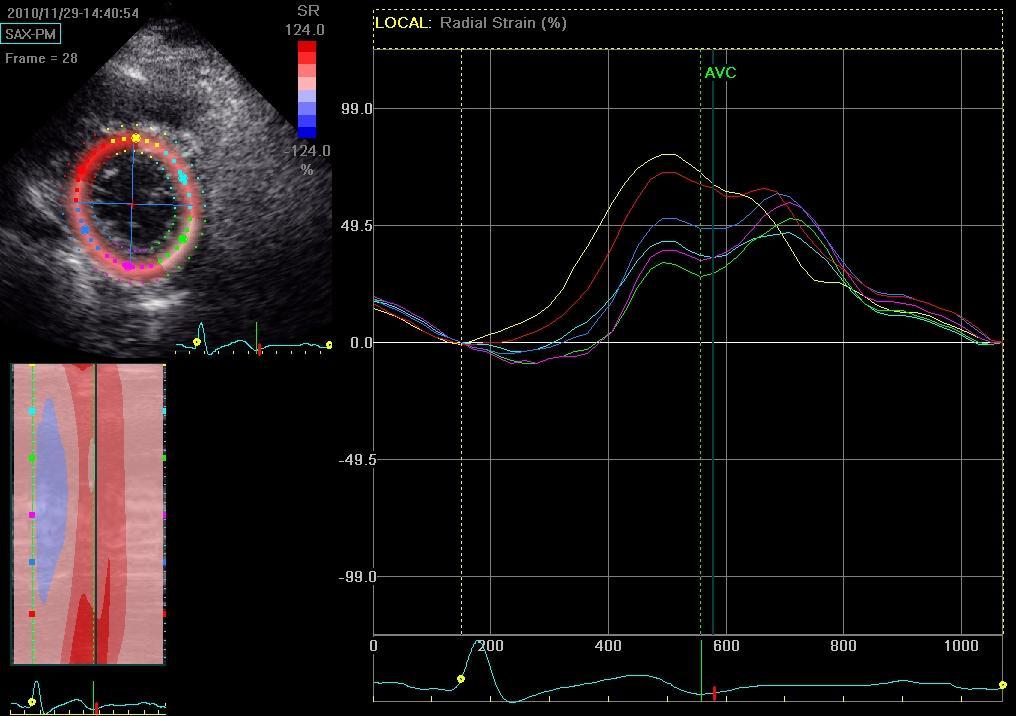
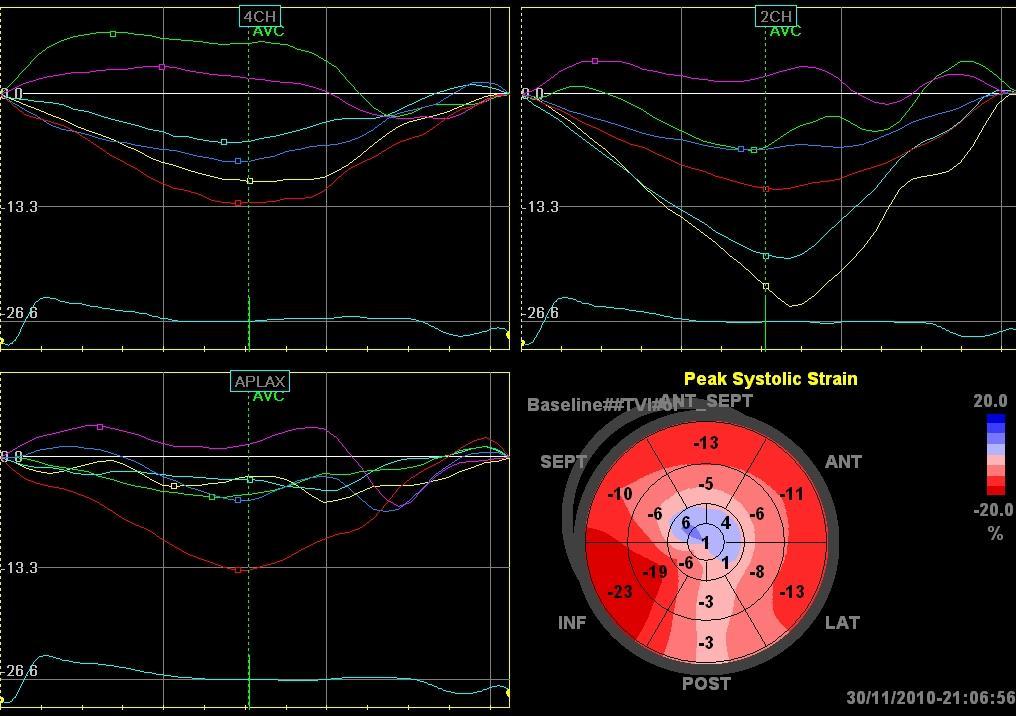
32 Changes in myocardial strain with AVR Long. Strain 11% Long. Strain 17% Before AVR After AVR Circ. Strain 12% Circ. Strain 17%




33 Changes in myocardial mechanics with AVR Rad. Strain 14% Rad. Strain 34% Before AVR After AVR Net Twist 26⁰ Net Twist 16⁰
34 Resolution of afterload mismatch Strain recovery improvement of afterload vs resolution of LVH and fibrosis Radial Circumferential Pre Immed post 6m 53 pts with AVR (AS and AR) pre-, 7d and 6m postop Becker M, JASE AVR pts (AS, normal EF) before and 17 m post AVR Delgado V, EHJ 2009
 At a low increase in LV afterload, 2D- Srad was still preserved whereas 2D- Slong significantly decreased When LV afterload was subsequently increased, both 2D-Srad and 2D-Slong")
35 Acute effect of increased afterload Study of 2DS and sonomicrometry (SS) in an exptal pig model of aortic banding Loading conditions: baseline and graded aortic banding (increase in LV pressure of 10, 20, and 40 mmhg) At a low increase in LV afterload, 2D- Srad was still preserved whereas 2D- Slong significantly decreased When LV afterload was subsequently increased, both 2D-Srad and 2D-Slong significantly decreased (by 50-60%) Difference in dependence to wall stress might explain these different behaviors Donal E, EJE 2009
36 DbEcho for assessment of low gradient AS LV dysfunction (medical Rx) Severe AS (do well with AVR) Ambiguous (bad prognosis) Contractile reserve Valve area Gradient >20% incr WMSI >0.3 cm 2 No change >20% incr WMSI No change No change ± ± Increase Increase in AVA with flow occurs in severe as well as mild AS; use of absolute cutoff >1cm 2 may be better to exclude AS (Carabello) de Filippi CR, Am J Cardiol 1995
37 Surgical outcome of patients with low output AS Monin, Circulation 2003 Connolly, Circulation 2002


38 Rest DSI mcg DSI 0.15


39 Global strain 7% Global strain 10%

40 Conclusions Deformation parameters should not be interpreted independent of load Watchful waiting is a reasonable option in asymptomatic severe MR, and deformation parameters can quantify contractile reserve, are a marker of fibrosis and predict LV response to surgery Disturbances of deformation parameters in severe AS are related to intensity of pressure load, so distinguishing the role of intrinsic myocardial disease is more difficult. However, strain may be used to measure contractile reserve.
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR. Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM
 Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM Conflict of Interest Disclosure None Why to assess LV function in asymptomatic
Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM Conflict of Interest Disclosure None Why to assess LV function in asymptomatic
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Insights into Viability- Function and Contractile Reserve
 Insights into Viability- Function and Contractile Reserve Tom Marwick Cleveland Clinic Conflicts research grants and consulting with GE, Philips, Siemens Off-label use of Definity for assessment of myocardial
Insights into Viability- Function and Contractile Reserve Tom Marwick Cleveland Clinic Conflicts research grants and consulting with GE, Philips, Siemens Off-label use of Definity for assessment of myocardial
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Advanced Evaluation of Left Ventricular Function in Degenerative MR. Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium
 Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Aortic valve Stenosis: Insights in the evaluation of LV function. Erwan DONAL Cardiologie CHU Rennes
 Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
LA Function analysis Marcia Barbosa Vice Presidente - Brazilian Soc of Cardiology President-elect - Interamerican Soc of Cardiology
 LA Function analysis Marcia Barbosa Vice Presidente - Brazilian Soc of Cardiology President-elect - Interamerican Soc of Cardiology Belo Horizonte Brazil DECLARATION OF CONFLICT OF INTEREST Nothing to
LA Function analysis Marcia Barbosa Vice Presidente - Brazilian Soc of Cardiology President-elect - Interamerican Soc of Cardiology Belo Horizonte Brazil DECLARATION OF CONFLICT OF INTEREST Nothing to
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines. Christophe Tribouilloy Amiens, France
 Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines Christophe Tribouilloy Amiens, France I have no financial relationships to disclose related
Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines Christophe Tribouilloy Amiens, France I have no financial relationships to disclose related
When is strain assessment mandatory?
 When is strain assessment mandatory? Geneviève Derumeaux University of Lyon France Presenter Disclosure Information Geneviève Derumeaux When is strain assessment mandatory? DISCLOSURE INFORMATION: None
When is strain assessment mandatory? Geneviève Derumeaux University of Lyon France Presenter Disclosure Information Geneviève Derumeaux When is strain assessment mandatory? DISCLOSURE INFORMATION: None
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation
 Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation Julien Magne, PhD, Kim O Connor, MD, Giuseppe Romano, MD, Marie Moonen, MD, Luc A.
Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation Julien Magne, PhD, Kim O Connor, MD, Giuseppe Romano, MD, Marie Moonen, MD, Luc A.
Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD
 Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD Board Review Course 2017 43 year old health assistant Severe resistant HTN LT BSA 2 Height 64 1 Here is the M mode echocardiogram
Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD Board Review Course 2017 43 year old health assistant Severe resistant HTN LT BSA 2 Height 64 1 Here is the M mode echocardiogram
Exercise PHT in valvular heart disease. Julien Magne CHU Limoges, France
 Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
Alicia Armour, MA, BS, RDCS
 Alicia Armour, MA, BS, RDCS No disclosures Review 2D Speckle Strain (briefly) Discuss some various patient populations & disease pathways where Strain can be helpful Discuss how to acquire images for Strain
Alicia Armour, MA, BS, RDCS No disclosures Review 2D Speckle Strain (briefly) Discuss some various patient populations & disease pathways where Strain can be helpful Discuss how to acquire images for Strain
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
Advanced imaging of the left atrium - strain, CT, 3D, MRI -
 Advanced imaging of the left atrium - strain, CT, 3D, MRI - Monica Rosca, MD Carol Davila University of Medicine and Pharmacy, Bucharest, Romania Declaration of interest: I have nothing to declare Case
Advanced imaging of the left atrium - strain, CT, 3D, MRI - Monica Rosca, MD Carol Davila University of Medicine and Pharmacy, Bucharest, Romania Declaration of interest: I have nothing to declare Case
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling. What is the pathophysiology at presentation?
 Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Prognostic Value of Left Atrial Size and Function
 Prognostic Value of Left Atrial Size and Function James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Conflicts: None
Prognostic Value of Left Atrial Size and Function James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Conflicts: None
History of Stress Testing. Disclosure. Overview. Stress Echocardiography New Applications. and Comparison with Other Stress.
 Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False?
 Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False? Masaki Izumo a, Kengo Suzuki b, Hidekazu Kikuchi b, Seisyo Kou b, Keisuke Kida b, Yu Eguchi b, Nobuyuki Azuma
Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False? Masaki Izumo a, Kengo Suzuki b, Hidekazu Kikuchi b, Seisyo Kou b, Keisuke Kida b, Yu Eguchi b, Nobuyuki Azuma
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Michigan Society of Echocardiography 30 th Year Jubilee
 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Diastology Disclosures: None. Dias2011:1
 Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Strain/Untwisting/Diastolic Suction
 What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
What is the Role of Surgical Repair in 2012
 What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
Clinical Outcome in Patients with Aortic Stenosis
 Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
2/2/2011. Strain and Strain Rate Imaging How, Why and When? Movement vs Deformation. Doppler Myocardial Velocities. Movement. Deformation.
 Strain and Strain Rate Imaging How, Why and When? João L. Cavalcante, MD Advanced Cardiac Imaging Fellow Cleveland Clinic Foundation Disclosures: No conflicts of interest Movement vs Deformation Movement
Strain and Strain Rate Imaging How, Why and When? João L. Cavalcante, MD Advanced Cardiac Imaging Fellow Cleveland Clinic Foundation Disclosures: No conflicts of interest Movement vs Deformation Movement
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Strain Imaging: Myocardial Mechanics Simplified and Applied
 9/28/217 Strain Imaging: Myocardial Mechanics Simplified and Applied John Gorcsan III, MD Professor of Medicine Director of Clinical Research Division of Cardiology VECTORS OF CONTRACTION Shortening Thickening
9/28/217 Strain Imaging: Myocardial Mechanics Simplified and Applied John Gorcsan III, MD Professor of Medicine Director of Clinical Research Division of Cardiology VECTORS OF CONTRACTION Shortening Thickening
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece
 A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
Restrictive Cardiomyopathy
 ESC Congress 2011, Paris Imaging Unusual Causes of Cardiomyopathy Restrictive Cardiomyopathy Kazuaki Tanabe, MD, PhD Professor of Medicine Chair, Division of Cardiology Izumo, Japan I Have No Disclosures
ESC Congress 2011, Paris Imaging Unusual Causes of Cardiomyopathy Restrictive Cardiomyopathy Kazuaki Tanabe, MD, PhD Professor of Medicine Chair, Division of Cardiology Izumo, Japan I Have No Disclosures
Journal of the American College of Cardiology Vol. 44, No. 9, by the American College of Cardiology Foundation ISSN /04/$30.
 Journal of the American College of Cardiology Vol. 44, 9, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.04.062 Relation
Journal of the American College of Cardiology Vol. 44, 9, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.04.062 Relation
The best in heart valve disease Aortic valve stenosis
 The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons
 Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Is normal ejection fraction equivalent to normal systolic function?
 Is normal ejection fraction equivalent to normal systolic function? D. Vinereanu University of Medicine, Bucharest, Romania EAE course, Bucharest No 2 nd criterion (out of 3) for the diagnosis of HFNEF:
Is normal ejection fraction equivalent to normal systolic function? D. Vinereanu University of Medicine, Bucharest, Romania EAE course, Bucharest No 2 nd criterion (out of 3) for the diagnosis of HFNEF:
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Low Gradient AS Normal LVEF
 Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes
 Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
: mm 86 mm EF mm
 37 Vol. 35, pp. 37 42, 2007 2 3 : 9 6 22 68 40 2003 4 Ejection fraction: EF44 IV 70 mm 86 mm EF46 6 24 mm 4 mm EF 80 60 mm 70 mm Aortic Regurgitation: AR 2 3 AR Aortic Valve Replacement: AVR AR 38 : 68
37 Vol. 35, pp. 37 42, 2007 2 3 : 9 6 22 68 40 2003 4 Ejection fraction: EF44 IV 70 mm 86 mm EF46 6 24 mm 4 mm EF 80 60 mm 70 mm Aortic Regurgitation: AR 2 3 AR Aortic Valve Replacement: AVR AR 38 : 68
Late secondary TR after left sided heart disease correction: is it predictibale and preventable
 Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Coronary artery disease (CAD) risk factors
 risk factors") Background Coronary artery disease (CAD) risk factors CAD Risk factors Hypertension Insulin resistance /diabetes Dyslipidemia Smoking /Obesity Male gender/ Old age Atherosclerosis Arterial stiffness precedes
Background Coronary artery disease (CAD) risk factors CAD Risk factors Hypertension Insulin resistance /diabetes Dyslipidemia Smoking /Obesity Male gender/ Old age Atherosclerosis Arterial stiffness precedes
Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications
 24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Aortic Stenosis in the Elderly: Difficulties for the Clinician. Are Symptoms Due to Aortic Stenosis?
 Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Strain and Strain Rate Imaging How, Why and When?
 Strain and Strain Rate Imaging How, Why and When? João L. Cavalcante, MD Advanced Cardiac Imaging Fellow Cleveland Clinic Foundation Disclosures: No conflicts of interest Movement vs Deformation Movement
Strain and Strain Rate Imaging How, Why and When? João L. Cavalcante, MD Advanced Cardiac Imaging Fellow Cleveland Clinic Foundation Disclosures: No conflicts of interest Movement vs Deformation Movement
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
DECISION MAKING DEL CARDIOCHIRURGO NELL INSUFFICIENZA MITRALICA: ISTRUZIONI D USO D CARDIOLOGO
 DECISION MAKING DEL CARDIOCHIRURGO NELL INSUFFICIENZA MITRALICA: ISTRUZIONI D USO D PER IL CARDIOLOGO GUIDELINES IN ASYMPTOMATIC MR ACC/AHA ESC Antonio Miceli Heart Hospital Monasterio Foundation NATURAL/
DECISION MAKING DEL CARDIOCHIRURGO NELL INSUFFICIENZA MITRALICA: ISTRUZIONI D USO D PER IL CARDIOLOGO GUIDELINES IN ASYMPTOMATIC MR ACC/AHA ESC Antonio Miceli Heart Hospital Monasterio Foundation NATURAL/
Tissue Doppler and Strain Imaging
 Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
Ventricular Interactions in the Normal and Failing Heart
 Ventricular Interactions in the Normal and Failing Heart Congenital Cardiac Anesthesia Society 2015 Pressure-volume relations Matched Left ventricle to low hydraulic impedance Maximal stroke work limited
Ventricular Interactions in the Normal and Failing Heart Congenital Cardiac Anesthesia Society 2015 Pressure-volume relations Matched Left ventricle to low hydraulic impedance Maximal stroke work limited
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Echo assessment of the failing heart
 Echo assessment of the failing heart Mark K. Friedberg, MD The Labatt Family Heart Center The Hospital for Sick Children Toronto, Ontario, Canada Cardiac function- definitions Cardiovascular function:
Echo assessment of the failing heart Mark K. Friedberg, MD The Labatt Family Heart Center The Hospital for Sick Children Toronto, Ontario, Canada Cardiac function- definitions Cardiovascular function:
The Patient with Atrial Fibrilation
 Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Paradoxical low flow-low gradient severe aortic stenosis: where are we?
 Journées Européennes de la SFC Paris, 15 janvier 2016 Paradoxical low flow-low gradient severe aortic stenosis: where are we? Nicolas Mansencal Hôpital Ambroise Paré, Boulogne Centre de Réf ce pour les
Journées Européennes de la SFC Paris, 15 janvier 2016 Paradoxical low flow-low gradient severe aortic stenosis: where are we? Nicolas Mansencal Hôpital Ambroise Paré, Boulogne Centre de Réf ce pour les