Indicator Mild Moderate Severe
|
|
|
- Megan Chase
- 5 years ago
- Views:
Transcription
1 Indicator Mild Moderate Severe Jet velocity (m/s) Mean gradient (mmhg) < Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1
2 Abnormal AV with Reduced Systolic Opening Severe AS V max 4 m/sec P mean 40 mmhg V max m/sec P mean mmhg Symptomatic (stage D1) Asymptomatic (stage C) Symptomatic Asymptomatic LVEF < 50% (stage C2) Other cardiac surgery Vmax 5 m/sec P mean 60mmHg Low surgical risk LVEF<50% Yes DSE with AVA 1 cm 2 and V max 4m/sec (stage D2) No AVA 1 cm 2 and LVEF 50% (stage D3*) Other cardiac surgery Abnormal ETT V max 0.3 m/s/y Low surgical risk AS likely cause of symptoms AVR (Class I) AVR (Class IIa) AVR (Class IIb) AVR (Class IIa) 2


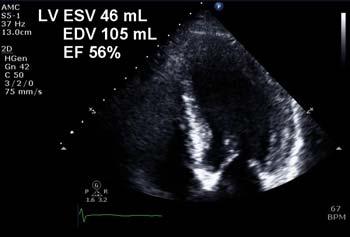

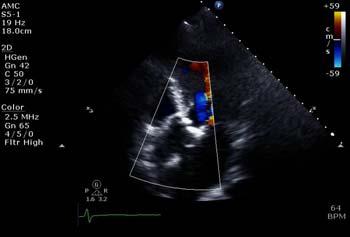
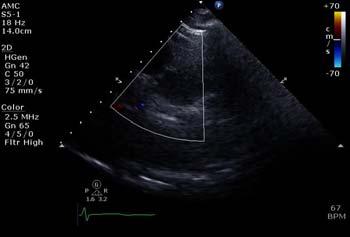

3 Case. Asymptomatic Severe AS Case. Asymptomatic Severe AS AV Vmax = 4.6 m/sec AV Vmax = 5.5 m/sec 3


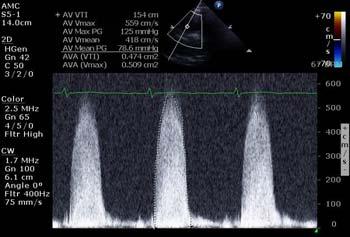
4 Case. Asymptomatic Severe AS LVOT diameter 2.1 cm LVOT TVI 21 cm Vmax = 5.5 m/sec AV TVI 154 cm Comparison of Early Surgery versus Conventional Treatment in Asymptomatic Very Severe Aortic Stenosis Duk-Hyun Kang, Sung-Ji Park*, Ji Hye Rim, Dae-Hee Kim, Jong-Min Song, Kee-Joon Choi, Seung Woo Park*, Jae-Kwan Song, Jae-Won Lee, Pyo-Won Park* Division of Cardiology, Cardiac Surgery Asan Medical Center, Samsung Medical Center* Seoul, South Korea Kang DH, et al. Circulation 2010;121:1502 4
5 Survival Free of Cardiac Death OP versus CONV group Cardiac mortality free survival (%) P<0.001 OP 6-year survival rate 100% CONV 6-year survival rate 76±5% OP CONV years No at Risk OP CONV Abnormal AV with Reduced Systolic Opening Severe AS V max 4 m/sec P mean 40 mmhg V max m/sec P mean mmhg Symptomatic (stage D1) Asymptomatic (stage C) Symptomatic Asymptomatic LVEF < 50% (stage C2) Other cardiac surgery Vmax 5 m/sec P mean 60mmHg Low surgical risk LVEF<50% Yes DSE with AVA 1 cm 2 and V max 4m/sec (stage D2) No AVA 1 cm 2 and LVEF 50% (stage D3*) Other cardiac surgery Abnormal ETT V max 0.3 m/s/y Low surgical risk AS likely cause of symptoms AVR (Class I) AVR (Class IIa) AVR (Class IIb) AVR (Class IIa) 5
 < 20 20-39 > 40 Valve area (cm 2 ) 1.")
6 Indicator Mild Moderate Severe Jet velocity (m/s) < > 4.0 Mean gradient (mmhg) < > 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 6
 35 >35 Classical LF LG AS Paradoxical LF LG AS")
7 Minners J, et al. Eur Heart J 2008;29: AVA 1.0cm2 & Mean PG < 40mmHg LVEF < 50% 50% SV index (ml/m 2 ) 35 >35 Classical LF LG AS Paradoxical LF LG AS Normal-flow LG AS Clavel MA et al., Eur Heart J,







8 67 year old female with exertional dyspnea Case: low gradient AS with depressed LVEF LVOT diameter 2.0 cm LVOT TVI 12.5cm AV Vmax 3.7m/s Mean PG 35mmHg







9 Pibarot P and Dumesnil JG. J Am Coll Cardiol 2012;60: Baseline LVOT TVI 13.2cm Vmax 3.6m/sec PG 51/32mmHg AVA 0.52cm 2 Dobutamine 5 μg LVOT TVI 13.8cm Vmax 4.1m/sec PG 66/41mmHg Dobutamine 10 μg LVOT TVI 14.4cm Vmax 4.8m/sec PG 93/54mmHg AVA 0.50cm 2 9


10 Low-gradient severe AS with depressed LVEF - Low LVEF (<40%) causing low stroke volume - True severe AS versus pseudosevere AS Paradoxical Low-flow, Low-gradient severe AS with preserved LVEF - Severe concentric LVH and smaller LV cavity size - High valvuloarterial impedance and low stroke volume Pibarot P and Dumesnil JG. J Am Coll Cardiol 2012;60:






 60 40 P<0.")
 0 0 1 2 3")
11 Impaired Diastolic Filling Pronounced Concentric Remodeling Atrial Fibrillation Impaired Longitudinal Systolic function Reduced Forward Stroke Volume Reduced Transvalvular flow rate Mitral Regurgitation Mitral Stenosis Tricuspid Regurgitation Low-Flow, Low gradient AS with Preserved LVEF Pibarot P, Dumesnil JG. Circulation 2013: NF group PLF surgical NF surgical Survival (%) P=0.006 PLF group Survival (%) P<0.001 PLF medical NF medical Follow-up (year) Follow-up (year) Hachicha Z, et al. Circulation 2007;115:
 0 12 24 36 48 60 Follow up, (month) Ozkan et al. Circulation 2013;128:622 631 PARTNER-I B (inoperable): Medical vs.")
12 1.0 Unadjusted 1.0 Adjusted 0.8 AVR 0.8 Survival (%) Standard Survival (%) AVR Standard Log rank P< HR: 2.03, P= Follow up, (month) Follow up, (month) Ozkan et al. Circulation 2013;128: PARTNER-I B (inoperable): Medical vs. TAVR 2-Year Death (%) LF-Cohort B-TAVR LF-Cohort B-MM Log Rank P< % 45.9% No. at Risk Time in Days B-TAVR B-MM Year Death (%) LF,NEF and-lg-cohort B-TAVR LF,NEF and LG-Cohort B-MM Log Rank P= % 56.5% No. at Risk Time in Days B-TAVR B-MM Herrman HC et al, Circulation,
13 AVA < 1.0 cm 2 Low gradient (severe?) AS LVEF < 50% Low LVEF 50% Preserved LVEF Classical Low-Flow, Low-gradient AS D2 Stage < 35 ml/m 2 Low Flow Paradox, Low Flow, Low-gradient AS D3 Stage Flow SVi 35 ml/m 2 Normal Flow Normal Flow, Low-gradient AS? Stage Confirm AS severity: 2D echo, DSE, MDCT Assess surgical risk Confirm AS severity: 2D echo, MDCT Assess surgical risk Confirm AS severity: 2D echo, MDCT AVR-Class IIa TAVR > SAVR? AVR-Class IIa TAVR > SAVR? AVR? SAVR or TAVR Pibarot P et al. J Am Coll Cardiol 2016: AVA 1.0cm2 & Mean PG < 40mmHg LVEF < 50% 50% SV index (ml/m 2 ) 35 >35 Classical LF LG AS Paradoxical LF LG AS Normal-flow LG AS Clavel MA et al., Eur Heart J,







14 Case: 70 year old male with low gradient AS and dyspnea Case: low gradient AS with preserved LV ejection fraction LVOT 2.08 cm LVOT TVI 25 cm AV Vmax 3.7 m/s meanpg 35 mmhg AV TVI 90 cm AVA LVOT cm BSA = 1.77 m 2 AVAI = 0.53 cm 2 /m 2 Stroke Volume = 80.0 ml SVI = 45.2 ml/m 2 14
 Mean gradient (mmhg) 3.0 2.9 2.0 6.6 1.0 26 0.9 32 0.8 41 0.7 53 0.")
15 Paradoxical Low-flow, Low-gradient severe AS - Severe concentric LVH and smaller LV cavity size - High valvuloarterial impedance and low stroke volume Normal-flow, Low-gradient severe AS - Measurement error - Small body surface area - Inconsistency between cutoff values of AVA and gradient Aortic valve area (cm 2 ) Mean gradient (mmhg) Carabello BA. N Engl J Med 2002;346:677 15
16 AVA < 1.0 cm 2 Low gradient (severe?) AS LVEF < 50% Low LVEF 50% Preserved LVEF Classical Low-Flow, Low-gradient AS D2 Stage < 35 ml/m 2 Low Flow Paradox, Low Flow, Low-gradient AS D3 Stage Flow SVi 35 ml/m 2 Normal Flow Normal Flow, Low-gradient AS? Stage Confirm AS severity: 2D echo, DSE, MDCT Assess surgical risk Confirm AS severity: 2D echo, MDCT Assess surgical risk Confirm AS severity: 2D echo, MDCT AVR-Class IIa TAVR > SAVR? AVR-Class IIa TAVR > SAVR? AVR? Pibarot P et al. J Am Coll Cardiol 2016: Watchful Observation Versus Early Aortic Valve Replacement for Patients with Normal flow, Low Gradient Severe Aortic Stenosis Duk-Hyun Kang, Jeong Yoon Jang, Sung-Ji Park, Dae Hee Kim, Jong-Min Song, Seung Woo Park, Jae-Kwan Song, Jae Won Lee, Seung-Jung Park Asan and Samsung Medical Center Seoul, Korea Kang DH, et al. Heart 2015;

17 Study Flow Normal flow LG AS (n = 284) Early AVR Group (n = 98, 35%) Early elective AVR within 6 months after initial echocardiography Watchful Observation Group (n = 186, 65%) Referred for late AVR Symptoms worsened Aortic jet velocity > 4 m/s Mean gradient > 40 mmhg Clinical and Echocardiographic follow-up until June 2014 Kang DH, et al. Heart 2015; Overall mortality rate, % p = year overall mortality rate Early AVR Watchful Observation 17 ± 5 % 27 ± 5% No. at Risk Early AVR Watchful Observation Time after baseline, years

18 100 CV mortality rate, % p = year CV mortality rate Early AVR Watchful Observation 11 ± 4 % 18 ± 4 % No. at Risk Early AVR Watchful Observation Time after baseline, years Overall mortality rate, % p = year overall mortality rate Early AVR Watchful Observation 20 ± 5% 22 ± 7 % No. at Risk Early AVR Watchful Observation Time after baseline, years


 Low-flow,")
19 75 year old female with exertional dyspnea AV Vmax 3.8 m/s AV TVI 89 cm LVOT 1.96 cm AVA... LVOT TVI 20.4 cm BSA = 1.57 m 2 AVAI = 0.43 cm 2 /m 2 SVI = 39.2 ml/m 2 Case. What is your diagnosis? 1) Moderate AS 2) High-gradient Severe AS 3) Normal-flow, Low-gradient Severe AS 4) Low-flow, Low-gradient Severe AS 19

 Moderate AS 2) High-gradient Severe")
 Low-flow, Low-gradient Severe AS")
20 75 year old female with high gradient, severe AS AV Vmax 3.8 m/s AV Vmax 4.2 m/s Case. What is your diagnosis? 1) Moderate AS 2) High-gradient Severe AS 3) Normal-flow, Low-gradient Severe AS 4) Low-flow, Low-gradient Severe AS 20

21 Flow gradient pattern, AVA, ejection fraction, symptoms and operative risk should be considered in a decision for AVR in severe AS Clinical trials are required to evaluate benefit of surgical AVR or TAVR for symptomatic patients with LG severe AS and asymptomatic patients with very severe AS 21
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons
 Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes
 Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Paradoxical low flow-low gradient severe aortic stenosis: where are we?
 Journées Européennes de la SFC Paris, 15 janvier 2016 Paradoxical low flow-low gradient severe aortic stenosis: where are we? Nicolas Mansencal Hôpital Ambroise Paré, Boulogne Centre de Réf ce pour les
Journées Européennes de la SFC Paris, 15 janvier 2016 Paradoxical low flow-low gradient severe aortic stenosis: where are we? Nicolas Mansencal Hôpital Ambroise Paré, Boulogne Centre de Réf ce pour les
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment
 Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Low gradient severe aortic stenosis with preserved left ventricular ejection fraction
 Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Severe Asymptomatic Aortic Stenosis
 Severe Asymptomatic Aortic Stenosis The Clinician s Perspective Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
Severe Asymptomatic Aortic Stenosis The Clinician s Perspective Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
The best in heart valve disease Aortic valve stenosis
 The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Outcome of Patients With Aortic Stenosis, Small Valve Area, and Low-Flow, Low-Gradient Despite Preserved Left Ventricular Ejection Fraction
 Journal of the American College of Cardiology Vol. 60, No. 14, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.12.054
Journal of the American College of Cardiology Vol. 60, No. 14, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.12.054
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Affecting the elderly Requiring new approaches. Echocardiographic Evaluation of Hemodynamic Severity. Increasing prevalence Mostly degenerative
 Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Workshop Facing the challenge of TAVI 2016
 Workshop Facing the challenge of TAVI 2016 Congrès annuel de la SSC Lausanne 15 Juin 2016 Pitfalls in the severity assessment of aortic stenosis by echocardiography Hajo Müller, unité d échocardiographie,
Workshop Facing the challenge of TAVI 2016 Congrès annuel de la SSC Lausanne 15 Juin 2016 Pitfalls in the severity assessment of aortic stenosis by echocardiography Hajo Müller, unité d échocardiographie,
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Low Gradient AS Normal LVEF
 Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation
 Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation Julien Magne, PhD, Kim O Connor, MD, Giuseppe Romano, MD, Marie Moonen, MD, Luc A.
Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation Julien Magne, PhD, Kim O Connor, MD, Giuseppe Romano, MD, Marie Moonen, MD, Luc A.
Echo evaluation for TAVR. From the General Cardiologist to the Interventional Echocardiologist
 Echo evaluation for TAVR From the General Cardiologist to the Interventional Echocardiologist Disclosures Proctoring activities for Abbott Vascular I and the HYGEIA Hospital «Heart Team» have received
Echo evaluation for TAVR From the General Cardiologist to the Interventional Echocardiologist Disclosures Proctoring activities for Abbott Vascular I and the HYGEIA Hospital «Heart Team» have received
Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Aortic Stenosis.
 Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Role of Transesophageal Echocardiography in the Diagnosis of Paradoxical Low Flow, Low Gradient Severe Aortic Stenosis
 Original Article Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Role of Transesophageal Echocardiography in the Diagnosis of Paradoxical Low Flow, Low Gradient Severe Aortic Stenosis
Original Article Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Role of Transesophageal Echocardiography in the Diagnosis of Paradoxical Low Flow, Low Gradient Severe Aortic Stenosis
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece
 A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Mixed aortic valve disease
 Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences
Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences
Michigan Society of Echocardiography 30 th Year Jubilee
 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Aortic valve Stenosis: Insights in the evaluation of LV function. Erwan DONAL Cardiologie CHU Rennes
 Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Vinod H. Thourani, MD
 Triggers for Aortic Stenosis and Regurgitation Vinod H. Thourani, MD Professor of Surgery Chair, Department of Cardiac Surgery MedStar Heart and Vascular Institute Georgetown University Washington, DC,
Triggers for Aortic Stenosis and Regurgitation Vinod H. Thourani, MD Professor of Surgery Chair, Department of Cardiac Surgery MedStar Heart and Vascular Institute Georgetown University Washington, DC,
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Clinical Outcome in Patients with Aortic Stenosis
 Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
A new way to look at the aortic valve
 The aortic valve: impedance, misfits and bulges Felix J. Rogers, DO, FASE Oakwood Southshore Medical Center January 24, 2010 A new way to look at the aortic valve Aortic stenosis patients with the same
The aortic valve: impedance, misfits and bulges Felix J. Rogers, DO, FASE Oakwood Southshore Medical Center January 24, 2010 A new way to look at the aortic valve Aortic stenosis patients with the same
Patient/prosthesis mismatch: how to evaluate and when to act?
 Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
New imaging modalities for assessment of TAVI procedure and results. R Dulgheru, MD Heart Valve Clinic CHU, Liege
 New imaging modalities for assessment of TAVI procedure and results R Dulgheru, MD Heart Valve Clinic CHU, Liege Disclosure of Interest I, Raluca Dulgheru, DO NOT HAVE a financial interest/arrangement
New imaging modalities for assessment of TAVI procedure and results R Dulgheru, MD Heart Valve Clinic CHU, Liege Disclosure of Interest I, Raluca Dulgheru, DO NOT HAVE a financial interest/arrangement
A Health Care Professional s Guide Aortic Stenosis in Seniors
 A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes
 Original Article Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes Andrea Colli, Eleonora Bizzotto, Laura Besola, Dario Gregori, Francesca Toto, Erica Manzan,
Original Article Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes Andrea Colli, Eleonora Bizzotto, Laura Besola, Dario Gregori, Francesca Toto, Erica Manzan,
The Incidence and Predictors of Postoperative Atrial Fibrillation After Noncardiothoracic Surgery
 ORIGINAL ARTICLE DOI 10.4070 / kcj.2009.39.3.100 Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright c 2009 The Korean Society of Cardiology The Incidence and Predictors of Postoperative Atrial Fibrillation
ORIGINAL ARTICLE DOI 10.4070 / kcj.2009.39.3.100 Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright c 2009 The Korean Society of Cardiology The Incidence and Predictors of Postoperative Atrial Fibrillation
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
The prevalence of calcific aortic valve disease approaches. Compendium. Current Management of Calcific Aortic Stenosis
 Compendium Circulation Research Compendium on Aortic Valve Disease: Introduction to the Compendium Introduction to Aortic Stenosis Hemodynamic and Cellular Response Feedback in Calcific Aortic Valve Disease
Compendium Circulation Research Compendium on Aortic Valve Disease: Introduction to the Compendium Introduction to Aortic Stenosis Hemodynamic and Cellular Response Feedback in Calcific Aortic Valve Disease
Severe Aortic Stenosis with Low Gradient and Preserved Ejection Fraction
 Severe Aortic Stenosis with Low Gradient and Preserved Ejection Fraction Roney Orismar Sampaio, Lucas José Tachotti Pires, Marcelo Luiz Campos Vieira, Flavio Tarasoutchi Instituto do Coração HCFMUSP; Hospital
Severe Aortic Stenosis with Low Gradient and Preserved Ejection Fraction Roney Orismar Sampaio, Lucas José Tachotti Pires, Marcelo Luiz Campos Vieira, Flavio Tarasoutchi Instituto do Coração HCFMUSP; Hospital
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
TAVR Cases. Disclosures 2/17/2018. February 17, :15 3:30 PM 15 min
 31 st Annual State of the Art Echocardiography San Diego, CA February 17, 2018 3:15 3:30 PM 15 min TAVR Cases Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate Professor
31 st Annual State of the Art Echocardiography San Diego, CA February 17, 2018 3:15 3:30 PM 15 min TAVR Cases Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate Professor
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Calcific aortic stenosis (AS) is the most frequent valvular
 is the most frequent valvular") Special Report Multimodality Imaging Strategies for the Assessment of Aortic Stenosis Viewpoint of the Heart Valve Clinic International Database (HAVEC) Group Raluca Dulgheru, MD; Philippe Pibarot, DVM,
Special Report Multimodality Imaging Strategies for the Assessment of Aortic Stenosis Viewpoint of the Heart Valve Clinic International Database (HAVEC) Group Raluca Dulgheru, MD; Philippe Pibarot, DVM,
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
STRUCTURAL. aortic stenosis, transcatheter aortic valve replacement
 Received: 4 April 2018 Revised: 17 August 2018 Accepted: 20 August 2018 DOI: 10.1111/joic.12561 STRUCTURAL Outcomes after transcatheter aortic valve replacement in patients with low versus high gradient
Received: 4 April 2018 Revised: 17 August 2018 Accepted: 20 August 2018 DOI: 10.1111/joic.12561 STRUCTURAL Outcomes after transcatheter aortic valve replacement in patients with low versus high gradient
Independent Effect of Low Flow on Outcomes in Patients Undergoing Aortic Valve Replacement for Severe Aortic Stenosis
 Circ J 2018; 82: 2199 2205 doi: 10.1253/circj.CJ-17-0900 ORIGINAL ARTICLE Valvular Heart Disease Independent Effect of Low Flow on Outcomes in Patients Undergoing Aortic Valve Replacement for Severe Aortic
Circ J 2018; 82: 2199 2205 doi: 10.1253/circj.CJ-17-0900 ORIGINAL ARTICLE Valvular Heart Disease Independent Effect of Low Flow on Outcomes in Patients Undergoing Aortic Valve Replacement for Severe Aortic
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
TAVI After PARTNER-2 : The Hamilton Approach
 TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVR: Intermediate Risk Patients
 TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
An Integrated Approach to Study LV Diastolic Function
 An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
Diastolic Function Assessment New Guideline Update Practical Approach
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry