The best in heart valve disease Aortic valve stenosis
|
|
|
- Debra Riley
- 5 years ago
- Views:
Transcription

1 The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare
2 Prevalence of moderate or severe valve disease (%) HEART VALVE DISEASES Prevalence of AS < Age (years) Second prevalent heart valve disease in populationbased studies 3-6% of subjects aged over 65 First operated valvular disease in developed countries Mitral regurgitation Mitral stenosis Aortic regurgitation Aortic stenosis Iung et al., Eur Heart J 2003 Nkomo et al., Lancet 2006
3 Outline of the presentation 1. Aortic valve structure Echocardiographic assessment of AS morphology Aortic valve calcifications Multimodality imaging 2. Imaging in clinical decision making Asymptomatic severe AS Paradoxical low-flow, low-gradient Low-flow, low-gradient 3. New interventions and imaging TAVI : alternative strategy? Multimodality imaging



4 Aortic valve structure Echocardiographic assessment of AS morphology Essential in patients with AS who are considered for TAVI 2011;108:
5 Accuracy of 2D echo in determining aortic valve structure in patients having AVR for AS TTE has limited accuracy (66%) in determining aortic valve structure Congenitally malformed aortic valves appear to be more likely when : TTE is uninterpretable Heavily calcified valves Parameters interfering with TTE images interpretation : Location rather than amount of calcium Breast tissue High interobserver variability (62%) which increases with severity of AS Biscupid aortic valve is not rare in > 70 years (37%) At present, TEO remains the more precise technique in determining aortic valve structure in patients with AS Ayad et al., Am J Cardiol 2011;108:

6 Aortic valve structure Aortic valve calcifications Pathophysiology of AS? No effective medical treatment Published online Nov 16, 2011





7 Inflammation-dependent mechanism of calcification Non conventional imaging tools: PET Potential targets for medical therapy Current imaging window using conventional imaging modalities: echo, CT and MRI Aikawa E and Otto CM. Circulation 2011, published online Nov 16 New SE and Aikawa E. Circ Res 2011;108:
 18F-FDG (inflammation quantification) and 18F-NaF (calcification")

8 Assessment of valvular calcification and inflammation by PET in patients with AS 121 patients (20 controls, 20 aortic sclerosis, 25 mild AS, 33 moderate AS, 23 severe AS) 18F-FDG (inflammation quantification) and 18F-NaF (calcification detection) tracers 18F-NaF uptake Progressive rise in uptake with increasing disease severity Calcification rather than inflammation appears to be the predominant process 18F-FDG uptake Dweck MR et al., Circulation published online Nov 16


9 Aortic valve structure Multimodality imaging Valvular anatomic orifice area valvular effective orifice area 2011;13:25
")
 Garcia et al.")
10 Comparison between CMR and TTE for the estimation of EOA in AS Good agreement between CMR and TTE for the estimation of valve EOA Underestimation of LVOT area by TTE (> LVOT elliptic rather than circular) Overestimation of LVOT VTI by TTE (> flow velocity profile is not flat and is skewed with higher velocities along the anterior and right aspects of the LVOT) Garcia et al., J Cardiovasc Magn Res 2011;13:25
11 Outline of the presentation 1. Aortic valve structure Echocardiographic assessment of AS morphology Aortic valve calcifications Multimodality imaging 2. Imaging in clinical decision making Asymptomatic severe AS Paradoxical low-flow, low-gradient Low-flow, low-gradient 3. New interventions and imaging TAVI : alternative strategy? Multimodality imaging
12 Imaging in clinical decision making Asymptomatic severe AS Medical management? Aortic valve replacement The prognosis of asymptomatic patients is highly variable Risk of rapid stenosis progression Risk of irreversible myocardial damage Increased operative mortality rate in severely symptomatic patients Mortality on the waiting list up to 15% Risk related to delayed symptoms reporting Low event-free survival at 2 years
13 Imaging in clinical decision making Asymptomatic severe AS Risk stratification is mandatory Valvular calcifications Exercise Doppler echocardiography Peak aortic jet velocity > 4 m/s Inactivity Inappropriately high LV mass Rapid increase in aortic-jet velocity Symptoms during exercise testing BNP Age CAD Renal failure Valvulo-arterial impedance


14 Imaging in clinical decision making Asymptomatic severe AS 2011;97:
15 Prognostic effect of inappropriately high LV mass (ilvm) in asymptomatic severe AS Measured LVM = 1.05 [(IVS + PW + LVID d ) 3 LVID d3 ] 13.6 g Calculation of predicted LVM Measured/predicted LVM ratio Cut-off value of 110% of the measured/ predicted LVM ratio to predict outcome with best specificity and sensitivity (ilvm) «Cumulative systolic load dose» indicator IIb class of recommandation for AVR in severe asymptomatic AS (ESC) Cioffi G et al., Heart 2011;97:
16 Valvulo-arterial impedance (Zva) LV afterload in AS = valvular load + arterial load SV EOA AA Static pressure LVSP P MG SAP } } valvular load total arterial load } load Flow axis LVSP Z va = SVi = MPG + SAP SVi Courtesy of P. Pibarot, Québec Heart and Lung Institute Hachicha et al., Circulation 2007;115:

17 Imaging in clinical decision making Asymptomatic severe AS 2011;108:
18 Prognostic significance of Zva and LV longitudinal function in asymptomatic severe AS 52 patients, NYHA I, AVA 0.4 ± 0.1 cm2, FEVG 61 ± 5% Baseline: Zva closely associated with Long S (r = -0.56, p = 0.016) Follow-up: Long S correlated with EF (r = 0.66, p < 0.001), mass index (r = -0.46, p = 0.015), indexed AVA (r = 0.37, p = 0.04) no correlation between Long S and MPG ROC curves analysis of Zva and LV long S for prediction of events Zito et al. Am J Cardiol 2011;108:1463-
, the increase in arterial")

19 2011;12: Aortic stiffness index = ln (SBP/DBP) (AoS-AoD)/AoD Independently of the increase of valvular load (= outflow tract obstruction), the increase in arterial load (= proximal aortic stiffness) has a direct detrimental impact on LV function, BNP release and LV filling pressure in patients with asymptomatic severe AS et preserved EF
20 Imaging in clinical decision making Importance of global afterload in asymptomatic severe AS The afterload imposed by valve stenosis and solely assessed using the mean gradient is unable to predict preclinical changes of myocardial function; An increased global afterload affects myocardial function despite preserved EF; High Zva is associated with LV myocardial dysfunction confirmed by regional LV deformation impairment; High Zva ( 5 mmhg/ml/m 2 ) is associated with reduced cardiac eventfree survival; Contribution of «global afterload» in clinical interpretation of symptoms. Lancellotti et al, EJE 2010; Lancellotti et al, Heart 2010; Hachicha et al, JACC 2009; Zito et al, Am J Cardiol 2011
 Normal LVEF Mean gradient < 40 mmhg?")
21 Imaging in clinical decision making Paradoxical low-flow, low-gradient AS Severe AS based on AVA < 1 cm 2 (< 0.6 cm 2 /m 2 ) Normal LVEF Mean gradient < 40 mmhg? Errors in AVA measurements Wrong cut-off value for severe AS Low flow (SVI < 35 ml/m 2 ) Carabello, NEJM 2002 Dumesnil, EHJ 2010
22 Severe AS, preserved LV ejection fraction Normal flow, high gradient SVi > 35 ml/m² Mean gradient > 40 mmhg AVA 0.4 ± 0.1 cm/m² LVEDD 48 ± 5 mm Z va = 4.2 ± 0.8 mmhg/ml/m 2 n = 152 (30%) AVR = 80% Low flow, high gradient SVi 35 ml/m² Mean gradient > 40 mmhg AVA 0.3 ± 0.1 cm/m² LVEDD 43 ± 5 mm Z va = 6.0 ± 1.2 mmhg/ml/m 2 n =44 (8%) AVR = 68% Normal flow, low gradient SVi > 35 ml/m² Mean gradient 40 mmhg AVA 0.5 ± 0.1 cm/m² VEDD 48 ± 5 mm Z va = 4.0 ± 0.6 mmhg/ml/m 2 n = 193 (38%) AVR = 53% Low flow, low gradient SVi 35 ml/m² Mean gradient 40 mmhg AVA 0.5 ± 0.1 cm/m² LVEDD 46 ± 5 mm Z va = 5.2 ± 1.3 mmhg/ml/m 2 n =123 (24%) AVR = 36% Dumesnil et al, EHJ 2009


23 Prevalence of paradoxical low-flow, low-gradient AS Hachicha 2007 Echo 512 pts Barasch 2008 Echo 215 pts Cramariuc 2009 Echo 359 pts Lancellotti 2010 Echo 173 pts Minners 2010 Echo 333 pts Minners 2010 Cath 333 pts Herrmann 2011 Echo 86 pts



24 Paradoxical low-flow, low-gradient AS LVEF markedly underestimates the extent of myocardial systolic impairment Adda et al., Circ Cardiovasc Imaging published online Nov 22, 2011 Lee et al., JASE 2011

25 Patients with PLF AS have abnormal myocardial structure and systolic function Moderate AS Severe AS/high gradient Severe AS/low gradient/preserved EF O Severe AS/low gradient/decresed EF Herrmann et al., JACC 2011;58:




 Hachicha et al,")
26 Physiopathology of paradoxical low-flow, low-gradient AS LVEF 70 % Classical Normal flow 110 ml Older patients Female gender mean pressure gradient LVEF LVEDVI systemic vascular resistance Paradoxical low-flow LVEF 60 % 90 ml Reduced LV filling Intrinsec myocardial dysfonction Higher global afterload SVI > 35 ml/m² Courtesy of P. Pibarot, Québec Heart and Lung Institute Low flow (SVI 35 ml/m 2 ) Hachicha et al, Circ 2007 SVI 35 ml/m²

27 Paradoxical low-flow, lowgradient severe AS 2011;123: A substudy of the SEAS trial
28 Outcome of patients with low-gradient severe AS and preserved LVEF Letter by Dumesnil and Pibarot in Circulation 2011,124:e360 Low-gradient severe AS : AVA <1.0 cm 2 and MPG < 40 mmhg Moderate AS : 1.0 < AVA < 1.5 and MPG < 40 mmhg Severe AS : AVA < 1.0 cm 2 and MPG > 40 mmhg Jander N et al., Circulation 2011;123: PLF group : AVA <1.0 cm 2 and MPG < 40 mmhg NF group : AVA < 1.0 cm 2 and MPG > 40 mmhg Potential explanations for these discrepancies : 1. Small body sizes and overestimation of AS severity in PLFLG group due to nonindexed AVA 2. Measurements errors 3. Patients in PLFLG group were not demonstrating the pathognomonic features of the disease (higher LV global hemodynamic load, more severe LV concentric remodeling, smaller cavity size, decreased LV midwall radius shortening) Hachicha et al., Circulation 2007
29 Paradoxical low-flow, low-gradient severe AS despite preserved LVEF The presence of a moderately increased transvalvular gradient (< 40 mmhg) or velocity (< 4 m/s) does not exclude the presence of severe AS in patients with small AVA and preserved LVEF; Paradoxical low-flow, low-gradient is found in 15 % of AS patients and is often associated with more advanced stage of the disease and worse prognosis; It is important to recognize this entity to avoid to deny surgery to a symptomatic patient with small AVA and low gradient.


30 Imaging in clinical decision making Low-flow, low-gradient AS AVA < 1 cm² (< 0.6 cm²/m²) with LV dysfunction (EF 40%) And MPG 30 (AHA) 40 (ESC) mmhg Approximatively 20% of AS population Poor outcome under conservative management High operative mortality risk : 8-30%

31 Imaging in clinical decision making Low-flow, low-gradient AS Does Zva demonstrates the same prognostic value in low-flow, lowgradient AS as it has been previously demontrated among paradoxical low-flow, low-gradient AS? 184 patients, AVA 1 cm2, EF 40%, MPG 40 mmhg 2011;12:
32 Zva does not improve risk stratification in low EF, low-gradient AS 88 patients (48%) with Zva 5 mmhg/ml/m 2 Based on DES: 12% (15 pts) of pseudosevere AS (DES-induced increased in AVA 0.3 cm 2 associated with peak DES AVA 1 cm 2 ) Zva value similar between true and pseudo-severe AS Follow-up: Zva not predictive of both operative and 5-year postoperative mortality Levy et al., Eur J Echo 2011;12:

33 Zva does not improve risk stratification in low EF, low-gradient AS LVSP Z va = SVi = MPG + SAP SVi Poor LV function = main determinant of outcome in LF/LG AS Lancellotti P and Magne J. Eur J Echo 2011;12:
34 Outline of the presentation 1. Aortic valve structure Echocardiographic assessment of AS morphology Aortic valve calcifications Multimodality imaging 2. Imaging in clinical decision making Asymptomatic severe AS Paradoxical low-flow, low-gradient Low-flow, low-gradient 3. New interventions and imaging TAVI : alternative strategy? Multimodality imaging


35 New interventions and imaging TAVI : alternative strategy for high-risk patients? Edwards SAPIEN Medtronic CoreValve
 trial Results for the high-risk subgroup of patients who were still candidates for surgical valve replacement High")
36 Transcatheter versus surgical aortic valve replacement in high-risk patients Smith CR et al. N Engl J Med 2011;364: Placement of Aortic Transcatheter Valves (PARTNER) trial Results for the high-risk subgroup of patients who were still candidates for surgical valve replacement High risk for operative complications or death = risk of death of at least 15% by 30 days after the procedure (based on the STS score) Patients were randomly assigned to undergo either transcatheter or surgical replacement of the aortic valve

37 TAVI versus surgical AVR in high-risk patients TAVI is similar to AVR with respect to rates of death from any cause at 1 year Smith CR et al. N Engl J Med 2011;364:

38 TAVI versus surgical AVR : a propensity score analysis in patients at high surgical risk Conradi et al., J Thorac Cardiovasc Surg 2011, published online Nov 2
39 New interventions and imaging Multimodality imaging of the aortic root The optimal strategy for planning TAVI has been expanded : 2D TTE- and catheterization-derived measures have been associated to high variability and significantly underestimation of the aortic annulus dimension. For the crucial measurement of the aortic annulus dimension, multimodal imaging is essential. MRI and TEE provide similar and essential assessment of the aortic valve annulus dimension, especially at the limits of the TAVI range. Close agreement and high reproducibility have been demonstrated between cardiac MRI and CT for the determination of aortic root size. Intra- and interobserver variability is lowest with cardiac MRI. Paelinck B et al., Am J Cardiol 2011;108:92-98 Jabbour et al., JACC 2011;58:



.")

40 New interventions and imaging Multimodality imaging of the aortic root The association between aortic valve/root morphology and outcome after TAVI has been evaluated : The presence and severity of AR after TAVI has been associated with larger aortic annulus dimensions measured with cardiac MRI and CT. Calcifications of the aortic commissures and cusps unless the annulus appear to be responsible for paravalvular leaks. TAVI is associated with good post-procedural valve haemodynamics and clinical outcome in high-risk patients with severe AS and small aortic annulus (< 20 mm). When estimating the effective orifice area of Edwards-SAPIEN valves by Doppler-echo, it is recommended to use the LVOT diameter and velocity measured immediately proximal to the stent. Jabbour et al., JACC 2011;58: Colli et al., J Thorac Cardiovasc Surg 2011;142: Clavel et al., JACC Img 2011;4:
41 Take home messages Aortic valve stenosis «New entity» since etiology and pathophysiology have considerably change Older individuals demontrating diffused manifestations of atherosclerosis (AS, hypertension, ischemic cardiomyopathy) More complexe and multifaceted presentation of the disease

42 The clinical spectrum of severe AS is more complex that previously believed and includes 3 entities : Pibarot and Dumesnil. JACC 2011;58:
43 CMR provides a non-invasive and reliable alternative to Doppler-echo for the quantification of AS severity.
44 Adverse outcome more closely related to Zva and regional myocardial dysfunction than to parameters such as AVA and gradients. LVEF markedly underestimates the extent of myocardial systolic impairment. Low-flow severe AS in presence of preserved EF is a confirmed entity that correspond to a more advanced stage of the disease and require close attention.

45 Thank you for your attention
46 2011;32:



47 Longitudinal function Circonferential function Radial function Ng et al., Eur Heart J 2011;32:
48 BNP release according to flow-gradient-valve area Consecutive asymptomatic patients (n=150) with severe AS (AVA<1cm²), preserved LV systolic function (LVEF >55%), normal exercise test Lancellotti et al., JACC 2012 in press



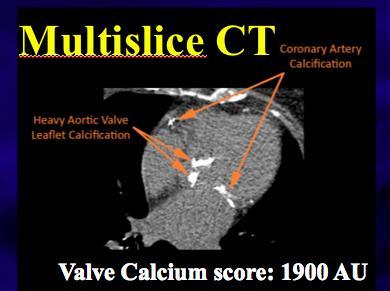

49 Valve Calcium score Valve Weight Clavel et al. ESC 2010
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low gradient severe aortic stenosis with preserved left ventricular ejection fraction
 Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Aortic valve Stenosis: Insights in the evaluation of LV function. Erwan DONAL Cardiologie CHU Rennes
 Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece
 A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment
 Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Workshop Facing the challenge of TAVI 2016
 Workshop Facing the challenge of TAVI 2016 Congrès annuel de la SSC Lausanne 15 Juin 2016 Pitfalls in the severity assessment of aortic stenosis by echocardiography Hajo Müller, unité d échocardiographie,
Workshop Facing the challenge of TAVI 2016 Congrès annuel de la SSC Lausanne 15 Juin 2016 Pitfalls in the severity assessment of aortic stenosis by echocardiography Hajo Müller, unité d échocardiographie,
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
New imaging modalities for assessment of TAVI procedure and results. R Dulgheru, MD Heart Valve Clinic CHU, Liege
 New imaging modalities for assessment of TAVI procedure and results R Dulgheru, MD Heart Valve Clinic CHU, Liege Disclosure of Interest I, Raluca Dulgheru, DO NOT HAVE a financial interest/arrangement
New imaging modalities for assessment of TAVI procedure and results R Dulgheru, MD Heart Valve Clinic CHU, Liege Disclosure of Interest I, Raluca Dulgheru, DO NOT HAVE a financial interest/arrangement
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Paradoxical low flow-low gradient severe aortic stenosis: where are we?
 Journées Européennes de la SFC Paris, 15 janvier 2016 Paradoxical low flow-low gradient severe aortic stenosis: where are we? Nicolas Mansencal Hôpital Ambroise Paré, Boulogne Centre de Réf ce pour les
Journées Européennes de la SFC Paris, 15 janvier 2016 Paradoxical low flow-low gradient severe aortic stenosis: where are we? Nicolas Mansencal Hôpital Ambroise Paré, Boulogne Centre de Réf ce pour les
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes
 Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Mixed aortic valve disease
 Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences
Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Outcome of Patients With Aortic Stenosis, Small Valve Area, and Low-Flow, Low-Gradient Despite Preserved Left Ventricular Ejection Fraction
 Journal of the American College of Cardiology Vol. 60, No. 14, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.12.054
Journal of the American College of Cardiology Vol. 60, No. 14, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.12.054
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
HIGHLIGHT SESSION. Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips
 Disclosures: Speaker Philips") Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR. Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM
 Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM Conflict of Interest Disclosure None Why to assess LV function in asymptomatic
Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM Conflict of Interest Disclosure None Why to assess LV function in asymptomatic
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
What the Cardiologist needs to know from Medical Images
 What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Patient/prosthesis mismatch: how to evaluate and when to act?
 Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Clinical Outcome in Patients with Aortic Stenosis
 Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Comments restricted to Sapien and Corevalve 9/12/2016. Disclosures: Core Lab contracts with Edwards Lifesciences, Middlepeak, Medtronic
 Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
New Imaging for Aortic Valve Disease. Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego
 New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
Role of Transesophageal Echocardiography in the Diagnosis of Paradoxical Low Flow, Low Gradient Severe Aortic Stenosis
 Original Article Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Role of Transesophageal Echocardiography in the Diagnosis of Paradoxical Low Flow, Low Gradient Severe Aortic Stenosis
Original Article Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Role of Transesophageal Echocardiography in the Diagnosis of Paradoxical Low Flow, Low Gradient Severe Aortic Stenosis
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery
 Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
The Role of Imaging in Transcatheter Aortic Valve Implantation
 The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
22/06/2017. Oxford City. Transcatheter aortic valve replacement 2017 guidelines. 1. First time I have heard about it. 2.
 Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons
 Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
TAVR TTE INTERROGATION BY ALAN MATTHEWS
 TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Echo evaluation for TAVR. From the General Cardiologist to the Interventional Echocardiologist
 Echo evaluation for TAVR From the General Cardiologist to the Interventional Echocardiologist Disclosures Proctoring activities for Abbott Vascular I and the HYGEIA Hospital «Heart Team» have received
Echo evaluation for TAVR From the General Cardiologist to the Interventional Echocardiologist Disclosures Proctoring activities for Abbott Vascular I and the HYGEIA Hospital «Heart Team» have received
Reverse left atrium and left ventricle remodeling after aortic valve interventions
 Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Affecting the elderly Requiring new approaches. Echocardiographic Evaluation of Hemodynamic Severity. Increasing prevalence Mostly degenerative
 Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
NEW GUIDELINES PAGE 9
 NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Stenosis, Including Recommendations for Echocardiography in Relation to Transcatheter Aortic Valve Implantation From the British Society
NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Stenosis, Including Recommendations for Echocardiography in Relation to Transcatheter Aortic Valve Implantation From the British Society
Calcific aortic stenosis (AS) is the most frequent valvular
 is the most frequent valvular") Special Report Multimodality Imaging Strategies for the Assessment of Aortic Stenosis Viewpoint of the Heart Valve Clinic International Database (HAVEC) Group Raluca Dulgheru, MD; Philippe Pibarot, DVM,
Special Report Multimodality Imaging Strategies for the Assessment of Aortic Stenosis Viewpoint of the Heart Valve Clinic International Database (HAVEC) Group Raluca Dulgheru, MD; Philippe Pibarot, DVM,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Paravalvular Regurgitation is a Risk Factor Following TAVI
 Paravalvular Regurgitation is a Risk Factor Following TAVI Philippe Pibarot, DVM, PhD, FACC, FESC, FASE Canada Research Chair in Valvular Heart Disease INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE
Paravalvular Regurgitation is a Risk Factor Following TAVI Philippe Pibarot, DVM, PhD, FACC, FESC, FASE Canada Research Chair in Valvular Heart Disease INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
What Determines the Outcome of Aortic Stenosis?
 What Determines the Outcome of Aortic Stenosis? Jutta Bergler-Klein Assoc. Professor of Medicine Dept of Cardiology, Med. Univ. Vienna jutta.bergler-klein @ meduniwien.ac.at AS in Perspective AS most common
What Determines the Outcome of Aortic Stenosis? Jutta Bergler-Klein Assoc. Professor of Medicine Dept of Cardiology, Med. Univ. Vienna jutta.bergler-klein @ meduniwien.ac.at AS in Perspective AS most common
When Does 3D Echo Make A Difference?
 When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
Prof. JL Zamorano Hospital Universitario Ramón y Cajal
 Prof. JL Zamorano Hospital Universitario Ramón y Cajal Fully Automated Quantification Software Adaptive analytical algorithm consists in knowledge-based identification of global shape and specific adaptation
Prof. JL Zamorano Hospital Universitario Ramón y Cajal Fully Automated Quantification Software Adaptive analytical algorithm consists in knowledge-based identification of global shape and specific adaptation
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Low Gradient AS Normal LVEF
 Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Advanced Evaluation of Left Ventricular Function in Degenerative MR. Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium
 Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Improving Assessment of Aortic Stenosis
 Journal of the American College of Cardiology Vol. 60, No. 3, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.11.078
Journal of the American College of Cardiology Vol. 60, No. 3, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.11.078
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Corrado Tamburino, MD, PhD
 Paravalvular leak: acceptable or not Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate School of Cardiology Chief Cardiovascular Department, Director Cardiology Division,
Paravalvular leak: acceptable or not Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate School of Cardiology Chief Cardiovascular Department, Director Cardiology Division,
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Mild paravalvular regurgitation is not an independent predictor of mortality following TAVI
 Mild paravalvular regurgitation is not an independent predictor of mortality following TAVI Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE
Mild paravalvular regurgitation is not an independent predictor of mortality following TAVI Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE
Aortic Regurgitation & Aorta Evaluation
 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
Aortic stenosis with concomitant mitral regurgitation
 Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center
Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center") The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline