Electrolyte Emergencies
|
|
|
- Daniela Terry
- 6 years ago
- Views:
Transcription
1 Electrolyte Emergencies
2 Hyponatremia/hypernatremia Hypokalemia/hyperkalemia Hypocalcemia/hypercalcemia Hypomagnesemia/hypermagnesemia Hypophosphatemia/hyperphosphatemia
3
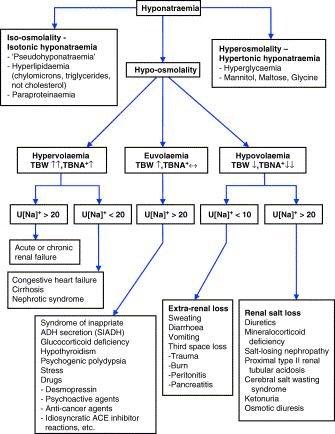
4 Hyponatremia Symptomatic: headaches, nausea, vomiting, decreased mental status, seizures, coma, brain herniation, neurogenic pulmonary edema, respiratory arrest, death Risk is higher in premenopausal females, children Sodium usually <120mEq/L
5 Treatment Correction can be life threatening especially in chronic hyponatremia (hyponatremia > 48 hours) Replete potassium first, remember potassium is an exchangeable cation Use hypertonic saline in symptomatic hyponatremia Patients with seizures and coma should get 2ml/kg bolus infusions or 100ml of 3% saline up to 2 times Do not correct by more than 8mEq/l in 24 hours or 15-20mEq/l in 48 hours. Check sodium q 2 hours Change Na for 1 Liter of IVF= [(infusate Na+ infusate K)- serum Na]/TBW +1
6
7 Hypernatremia Symptomatic: Cerebral dehydration leads to demyelinization, cerebral bleeding, coma and death. Na> mEq/L Acute or Chronic Don t correct >8-10mEq/l in 24 hours Provide 50% of the water deficit in the first hours and the rest over the next 24 hours Check sodium q2 hours [(Desired Na+/serum Na+) -1]xTBW
8
9 Hypokalemia Symptomatic: tachyarrhythmia, muscle weakness K<3mEq/l IV repletion, 20mEq-40mEq/hour via CVC, 10mEq/hour via PIV Continuous EKG monitoring No use of dextrose in IV solutions Make sure magnesium is replete

10 Hypokalemia: long QT interval, ST depression, low T waves, TU wave fusion
11
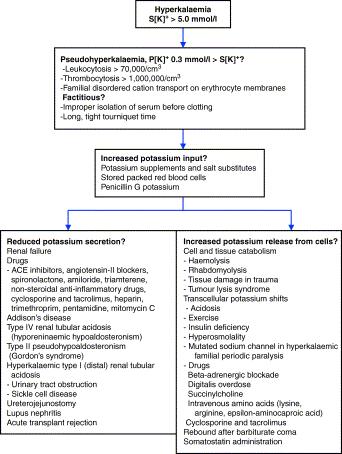
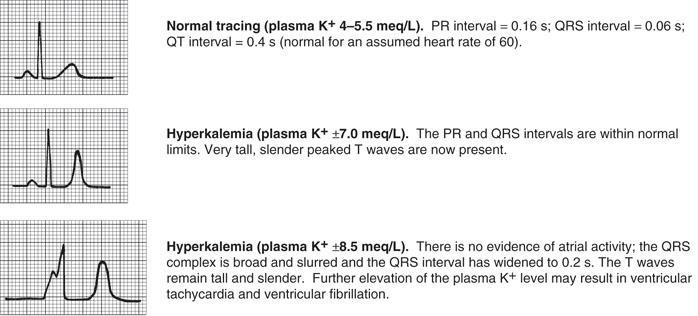
12 Hyperkalemia Symptomatic: fatigue, weakness, paresthesias, paralysis, palpitations K>6mEq/l Treatment: IV Calcium to restore membrane excitability toward normal Fastest-insulin/D50, Beta agonists Furosemide, sodium polystyrene sulfate +sorbitol Bicarbonate? Renal Replacement Therapy: IHD, then continuous therapies
13
14
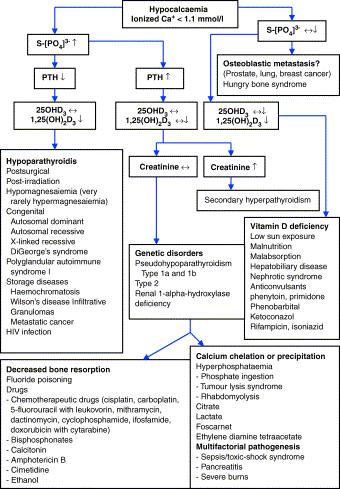
15 Hypocalcemia Symptomatic: tetany, muscle weakness, myalgia, cramps, parasthesia in hands and feet, circumoral numbness, dysphagia, biliary, intestinal colic, laryngospasm, bronchospasm, seizures, papilloedema, CHF from decreased myocardial contractility, hypotension, anxiety, psychosis, confusion, dementia, depression Ionized ca <0.7mmol/l or Ca 7-7.5mg/dl

16 Hypocalcemia: QT prolongation, T wave inversion
17 Treatment Replete Magnesium IV replacement Caution with digoxin? Caution in high phosphorus states >6mg/dl
18
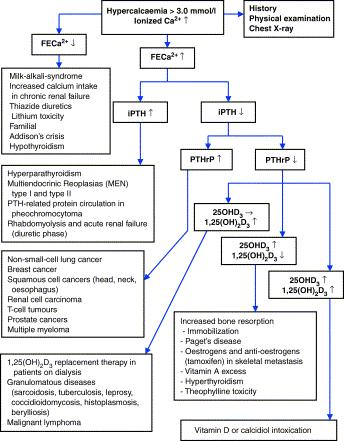
19 Hypercalcemia Symptomatic: fatigue, weakness, anxiety, depression, anorexia, n/v, abdominal pain, constipation, peptic ulcers, nephrogenic DI, Type 1 RTA, nephrolithiasis, acute pancreatitis, hypertension, confusion, psychosis, coma, shortening of QT wave-no clinical importance Calcium > 12mg/dl or ionized Ca 3.0mmol/l Measure ionized ca

20 Hypercalcemia: Short QT interval, Osborn waves
21 Treatment Hydration to a euvolemic to slightly hypervolemic state, then diuresis with loop diuretic Inhibition of osteoclast activity in the bone Avoid immobilization Cinacalcet
22
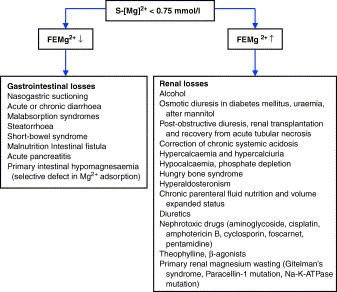
23 Hypomagnesemia Symptomatic: respiratory muscle weakness, fasciculations, cramps, tetany, convulsions, coronary artery vasospasm, atrial tachyarrythmias, supraventricular, ventricular arrythmias, torsades de pointes IV repletion at 1-2g of magnesium sulfate over a 10 minute period, up to 10grams a day Aim to keep above 1.0mg/dl

24 Torsade de pointes
25 Hypermagnesemia Symptomatic: confusion, depressed level of consciousness, N/V, weakness, paralysis with absence of reflexes, respiratory depression, hypotension, bradycardia, complete AV block PR, QT and QRS intervals are increased, decreased P wave voltage Mg>4.8mg/dl Treatment: Calcium, RRT
26
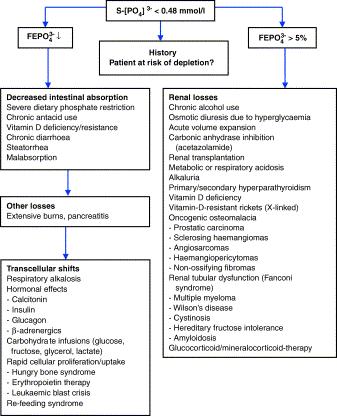
27 Hypophosphatemia Symptomatic: granulocyte dysfunction, arrythmias, respiratory muscle weakness, reduced oxygen delivery to tissues Phosphorus<1.0mg/dl Treatment: IV replacement with 15-30mmol over 2 hours potassium phosphate or sodium phosphate, cannot replace in the same line with calcium Watch out for resulting hypocalcemia
28 6
29 Hyperphosphatemia Acute can be life threatening secondary to hypocalcemia, hyperkalemia: CaPhos product > 60-72mg/dl results in precipitating calcium, decreasing serum calcium levels and causing AKI Symptoms: those of associated hypocalcemia and hyperkalemia Treatment: insulin/d50, IVF, carbonic anhydrase inhibitor, RRT
30 A 71-year-old woman who has had nocturia for several years is admitted to the hospital secondary to increasing weakness and frequency of urination. She has been well until 2 days ago, when she felt weak and could not climb the stairs to her apartment. She has a history of duodenal ulcer many years ago that responded to intensive antacid therapy. She currently takes calcium carbonate for treatment of osteoarthritis, and she takes bicarbonate of soda for heartburn. She has a 40 pack-year history of smoking. On physical examination, she is frail and oriented only to person. Pulse is 106/min, and BP is 110/80 supine and 90/70 mmhg sitting. The remainder of the examination is normal. Laboratory studies reveal the following: Hematocrit 41, Na 152 mmol/l, K 3.0 mmol/l, Cl 100 mmol/l, HCO3 39 meq/l, BUN 98 mg/dl, creatinine 7.1 mg/dl, Ca 14.4 mg/dl, phosphate 6.3 mg/dl, serum 1,25-dihydroxyvitamin D 30 pg/ml (35 to 85 pg/ml), parathyroid hormone 16 pg/ml (30 to 50 pg/ml). Urinalysis shows specific gravity of 1.007, trace protein, Na of 49 mmol/l, creatinine of 70 mg/dl, and urine osmolality of 260 mosm/kgh2o. Renal ultrasound shows normal-sized kidneys and no hydronephrosis. The clinical and laboratory findings are MOST consistent with which ONE of the following? A. Vitamin D intoxication. B. Chronic kidney disease as a result of longstanding hypertension. C. Multiple myeloma. D. Milk-alkali syndrome. E. Primary hyperparathyroidism.
31 A 54 y/o woman comes for a follow-up examination. She was discharged from the hospital 7 days ago after hospitalization for severe SOB. During her hospitalization, a large pleural effusion was found and pleurodesis was performed. At today s visit, she feels tired. She has not had nausea, headache, or irritability and has not vomited. She was diagnosed with met small cell lung CA 13 months ago and was treated with palliative chemo with a good response. Previous surgeries include 2 cesarean sections. She also has a 75 pack year tob hx. On physical exam her T is 36.8, P 84 RR 18 BP 126/84. She appears cachectic. Cardiac exam is normal. On pulm exam there are diminished breath sounds in the R base. There is no pedal edema. Labs: Glc 114 bun 10 cr 0.6 Na 112 K 3.2 Cl 84 bicarb 21 phos 3.1 alb 3.2 serum osm 243 urine osm 542 urine Na 120 urine K 24 Which of the following is the most appropriate therapy? A) 3% saline via infusion pump B) Demeclocycline C) Fluid restriction <1L/d D) Sodium Chloride tabs, 2 grams TID E) HCTZ
32 A 37y/o male with longstanding ETOHism is admitted to the ICU with severe pancreatitis. His friends state that for the last several weeks he has been drinking beer all day and has been eating very little except for salty snacks. Over the next 3 days, he develops sepsis and a pancreatic abscess that requires drainage. 2 days later, he remains on mechanical ventilation and vasopressor support. Labs obtained on hospital day 6: Glc 96 Bun 5 Cr 0.7 Na 136 K 4.3 Cl 105 Bicarb 22 Alb 2.9 Ca 7.1 Phos 2.4 Mg 2.2 He is started on TPN with 2000 total calories, 20% from fat; 120 meq of Na and 80meq of K. The total volume is 2L. Which of the following conditions does this patient have high risk for after TPN is started? A) Rhabdomyolysis B) Leukopenia C) Torsade de pointes D) Cerebral edema E) Fulminant liver failure
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
ISPUB.COM. Electrolyte Replacement: A Review. B Phillips INTRODUCTION ELECTROLYTES I. CALCIUM
 ISPUB.COM The Internet Journal of Internal Medicine Volume 5 Number 1 Electrolyte Replacement: A Review B Phillips Citation B Phillips. Electrolyte Replacement: A Review. The Internet Journal of Internal
ISPUB.COM The Internet Journal of Internal Medicine Volume 5 Number 1 Electrolyte Replacement: A Review B Phillips Citation B Phillips. Electrolyte Replacement: A Review. The Internet Journal of Internal
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Hyponatremia and Hypomagnesemia
 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Electrolyte Abnormalities in the Transplant Recipient
 Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
3.Which is not a cause of hypokalemia? a) insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD
 insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD") Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
VanderbiltEM.com. ACEP 2013 Electrolyte Emergencies. Mastering Emergency Medicine. Electrolyte Emergency Questions. Electrolyte Emergency Questions
 ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
FLUIDS AND ELECTROLYTES
 FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
For The Management Of. Diabetic Ketoacidosis
 Guidelines For The Management Of Diabetic Ketoacidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council
Guidelines For The Management Of Diabetic Ketoacidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council
Saint-Antoine Hospital, Paris. Medical Intensive Unit Care. Hafid Ait-Oufella, MD.PhD. Dyscalcemia. Dyskalemia
 Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris Potassium K + Molecular weight: 39 1gr K + =2.5mmol Potassium disorders in ICU : Our experience
Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris Potassium K + Molecular weight: 39 1gr K + =2.5mmol Potassium disorders in ICU : Our experience
I have no financial disclosures
 Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
A Mnemonic for the Treatment of Hyperkalemia. Nick Wolters, PGY1 Resident Grandview Medical Center
 A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
ECG & ELECTROLYTES IMBALANCE
 ECG & ELECTROLYTES IMBALANCE Ayman Khairy, MD Ass. Prof. of Cardiovascular Medicine Assiut University, EGYPT Mohamed Aboel-Kassem, MD Lecturer of Cardiovascular Medicine Assiut University, EGYPT Systematic
ECG & ELECTROLYTES IMBALANCE Ayman Khairy, MD Ass. Prof. of Cardiovascular Medicine Assiut University, EGYPT Mohamed Aboel-Kassem, MD Lecturer of Cardiovascular Medicine Assiut University, EGYPT Systematic
Chapter 20 8/23/2016. Fluids and Electrolytes. Fluid (Water) Fluid (Water) (Cont.) Functions
 Fluid (Water) (Cont.) Functions") Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyperkalemia. Case Studies in Electrolyte Management. The Lytes & ECG s Danger Signs!! Potassium. Objectives. Disclosures. Julie Miller, RN, BSN, CCRN
 Case Studies in Electrolyte Management Julie Miller, RN, BSN, CCRN Objectives Link altered electrolytes to potential life threatening complications Evaluate emergent treatment options for altered electrolyte
Case Studies in Electrolyte Management Julie Miller, RN, BSN, CCRN Objectives Link altered electrolytes to potential life threatening complications Evaluate emergent treatment options for altered electrolyte
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 2. Fluid, Electrolyte, and Acid-Base Imbalances
 Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA
 Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA Why Electrolytes are Important? IMMEDIATE LIFE THREAT. You can Save or KILL the patient fixing it. USEFUL CLUE to the UNDERLYING
Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA Why Electrolytes are Important? IMMEDIATE LIFE THREAT. You can Save or KILL the patient fixing it. USEFUL CLUE to the UNDERLYING
Remember Taking Care of Patients & Managing Electrolytes is a Team Sport! EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities
 EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities 11 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Clinical Professor of Medicine Nephrology
EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities 11 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Clinical Professor of Medicine Nephrology
DBL MAGNESIUM SULFATE CONCENTRATED INJECTION
 DBL MAGNESIUM SULFATE CONCENTRATED INJECTION NAME OF MEDICINE Magnesium Sulfate BP DESCRIPTION DBL Magnesium Sulfate Concentrated Injection is a clear, colourless, sterile solution. Each ampoule contains
DBL MAGNESIUM SULFATE CONCENTRATED INJECTION NAME OF MEDICINE Magnesium Sulfate BP DESCRIPTION DBL Magnesium Sulfate Concentrated Injection is a clear, colourless, sterile solution. Each ampoule contains
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09. Terminal Learning Objective. References. Hours: 2.0 Last updated: November 2015
 SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
*Excess sodium loss through N-V-D, skin and kidneys *Excess diuretic dosage *Liver Failure *CHF *Increased hypotonic IV fluids
 I. Blood Chemistries Sodium: Hyponatremia Normal: 135-145 meq/l Patho Ranges Causes Treatments Nsg. Considerations Serum below 135mEq/L *Most abundant cation in EXTRAcellular fluid *Maintains osmotic pressure
I. Blood Chemistries Sodium: Hyponatremia Normal: 135-145 meq/l Patho Ranges Causes Treatments Nsg. Considerations Serum below 135mEq/L *Most abundant cation in EXTRAcellular fluid *Maintains osmotic pressure
50% Concentrated Injection
 NAME OF THE MEDICINE. The molecular weight of the compound is 246.5 and the CAS registry number is 10034-99-8. The molecular formula is MgSO4, 7H2O. DESCRIPTION MAGNESIUM SULFATE HEPTAHYDRATE 50% CONCENTRATED
NAME OF THE MEDICINE. The molecular weight of the compound is 246.5 and the CAS registry number is 10034-99-8. The molecular formula is MgSO4, 7H2O. DESCRIPTION MAGNESIUM SULFATE HEPTAHYDRATE 50% CONCENTRATED
Liquid Consumption, Your Health, And Hyponatremia
 Liquid Consumption, Your Health, And Hyponatremia It is vital to remain hydrated at all times. The consumption of water is the most common way to do so. De-Hydrated Hydrated Over-Hydrated TWI: Total Water
Liquid Consumption, Your Health, And Hyponatremia It is vital to remain hydrated at all times. The consumption of water is the most common way to do so. De-Hydrated Hydrated Over-Hydrated TWI: Total Water
Chapter 24 Water, Electrolyte and Acid-Base Balance
 Chapter 24 Water, Electrolyte and Acid-Base Balance Total body water for 150 lb. male = 40L 65% ICF 35% ECF 25% tissue fluid 8% blood plasma, lymph 2% transcellular fluid (CSF, synovial fluid) Water Movement
Chapter 24 Water, Electrolyte and Acid-Base Balance Total body water for 150 lb. male = 40L 65% ICF 35% ECF 25% tissue fluid 8% blood plasma, lymph 2% transcellular fluid (CSF, synovial fluid) Water Movement
Fluids, Electrolytes and Hydration. Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University
 Fluids, Electrolytes and Hydration Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Discuss optimum hydration and effects of dehydration
Fluids, Electrolytes and Hydration Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Discuss optimum hydration and effects of dehydration
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
Fluid & Electrolyte Balances in Term & Preterm Infants. Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital
 Fluid & Electrolyte Balances in Term & Preterm Infants Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital Objectives Review maintenance fluid & electrolyte requirements in neonates Discuss
Fluid & Electrolyte Balances in Term & Preterm Infants Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital Objectives Review maintenance fluid & electrolyte requirements in neonates Discuss
H 2 O, Electrolytes and Acid-Base Balance
 H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter
 Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Electrolyte abnormalities are commonly associated with
 Electrolyte abnormalities are commonly associated with cardiovascular emergencies. These abnormalities may cause or contribute to cardiac arrest and may hinder resuscitative efforts. In some cases therapy
Electrolyte abnormalities are commonly associated with cardiovascular emergencies. These abnormalities may cause or contribute to cardiac arrest and may hinder resuscitative efforts. In some cases therapy
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
SODIUM POLYSTYRENE SULFONATE Suspension, USP
 SODIUM POLYSTYRENE SULFONATE Suspension, USP DESCRIPTION Sodium Polystyrene Sulfonate Suspension, USP can be administered orally or in an enema. It is a cherryflavored suspension containing 15 grams of
SODIUM POLYSTYRENE SULFONATE Suspension, USP DESCRIPTION Sodium Polystyrene Sulfonate Suspension, USP can be administered orally or in an enema. It is a cherryflavored suspension containing 15 grams of
Instruct patient and caregivers: Need for constant monitoring Potential complications of drug therapy
 Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University
 RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
Open Access Journal ISSN
 Open Access Journal www.ijirms.in ISSN - 2455-8737 Comparison of Serum Electrolyte Levels in Patients Who Presented at The Emergency Room of Rajavithi Hospital with Atrial Fibrillation with Rapid Ventricular
Open Access Journal www.ijirms.in ISSN - 2455-8737 Comparison of Serum Electrolyte Levels in Patients Who Presented at The Emergency Room of Rajavithi Hospital with Atrial Fibrillation with Rapid Ventricular
2/1/2013. Poisoning pitfalls. The original pitfall
 The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ
 Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
With Dr. Sarah Reid and Dr. Sarah Curtis
 5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
Hypoglycemia, Electrolyte disturbances and acid-base imbalances
 Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
CALCIUM BALANCE. James T. McCarthy & Rajiv Kumar
 CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
Acute Kidney Injury in the ED
 + Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
+ Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
Acids, Bases, and Salts
 Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Acid/Base Disorders 2015
 Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Resting Membrane Potential & Goldman Equation
 Resting Membrane Potential & Goldman Equation V m RT F log P K P K [ K [ K ] o ] i P P Na Na [ Na [ Na ] ] o i P P cl cl [ Cl [ Cl ] ] o i P = permeability at rest: P K : P Na : P Cl = 1.0 : 0.04 : 0.45
Resting Membrane Potential & Goldman Equation V m RT F log P K P K [ K [ K ] o ] i P P Na Na [ Na [ Na ] ] o i P P cl cl [ Cl [ Cl ] ] o i P = permeability at rest: P K : P Na : P Cl = 1.0 : 0.04 : 0.45
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017
 CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
CVICU EXAM. Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery
 CVICU EXAM 1111 North 3rd Street Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery 1. Nursing standards for a patient on an IABP device include: a. Know results of
CVICU EXAM 1111 North 3rd Street Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery 1. Nursing standards for a patient on an IABP device include: a. Know results of
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Nephrology / Urology. Hyperkalemia Causes and Definition Lecturio Online Medical Library. Definition. Epidemiology of Hyperkalemia.
 Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Volume and Electrolytes. Fluid and Electrolyte Management. Why 125ml? Question. Normal fluid requirement. Normal losses
 Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Vitamins. Vitamins (continued) Lipid-Soluble Vitamins (A, D, E, K) Vitamins Serve Important Roles in Function of Body
 Lipid-Soluble Vitamins (A, D, E, K) Vitamins Serve Important Roles in Function of Body") Vitamins Drugs for Nutritional Disorders Organic substances are needed in small amounts Promote growth Maintain health Vitamins Human cells cannot produce vitamins Exception: vitamin D Vitamins or provitamins
Vitamins Drugs for Nutritional Disorders Organic substances are needed in small amounts Promote growth Maintain health Vitamins Human cells cannot produce vitamins Exception: vitamin D Vitamins or provitamins
Understanding Blood Tests
 PATIENT EDUCATION patienteducation.osumc.edu Your heart pumps the blood in your body through a system of blood vessels. Blood delivers oxygen and nutrients to all parts of the body. It also carries away
PATIENT EDUCATION patienteducation.osumc.edu Your heart pumps the blood in your body through a system of blood vessels. Blood delivers oxygen and nutrients to all parts of the body. It also carries away
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
Final Case Study: Renal Disease Due 3/19/14 60 points
 NUT 116BL Name: CHRISTINE WOO Winter 2014 Section: 1 Final Case Study: Renal Disease Due 3/19/14 60 points Part I: Initial Presentation Present Illness: Jenny is a 19 yo F student referred to the renal
NUT 116BL Name: CHRISTINE WOO Winter 2014 Section: 1 Final Case Study: Renal Disease Due 3/19/14 60 points Part I: Initial Presentation Present Illness: Jenny is a 19 yo F student referred to the renal
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
TELEMETRY EXAM. 1. Match the numeral in the right column with the correct drug in the left column. a. Pronestyl 1. Hypotension
 TELEMETRY EXAM 1. Match the numeral in the right column with the correct drug in the left column. a. Pronestyl 1. Hypotension b. Digitalis 2. Tachycardias c. Potassium 3. Assists in repolarization d. Inderal
TELEMETRY EXAM 1. Match the numeral in the right column with the correct drug in the left column. a. Pronestyl 1. Hypotension b. Digitalis 2. Tachycardias c. Potassium 3. Assists in repolarization d. Inderal
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Electrolytes: Opposites Attract. Brian Dubiel RD, LD, CNSC
 Electrolytes: Opposites Attract Brian Dubiel RD, LD, CNSC Disclosure No conflict of interest exists. Overview Fluids Electrolytes Causes and common treatments for electrolyte abnormalities Shortages Trends
Electrolytes: Opposites Attract Brian Dubiel RD, LD, CNSC Disclosure No conflict of interest exists. Overview Fluids Electrolytes Causes and common treatments for electrolyte abnormalities Shortages Trends
Fluid and Electrolytes P A R T 4
 Fluid and Electrolytes P A R T 4 Mechanisms that control acid-base homeostasis Acids and bases continually enter and leave body Hydrogen ions also result from metabolic activity Acids Hydrogen ion donors
Fluid and Electrolytes P A R T 4 Mechanisms that control acid-base homeostasis Acids and bases continually enter and leave body Hydrogen ions also result from metabolic activity Acids Hydrogen ion donors
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Body water content. Fluid compartments. Regulation of water output. Water balance and ECF osmolallty. Regulation of water intake
 Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
ELECTROLYTES, Electrolytes are chemical substances that separate in solution (usually water. Fluids, and the Acid Base Balance
 80 Vol. 22, No. 2 February 2001 Peer-Reviewed CE Article #2 ELECTROLYTES, Fluids, and the Acid Base Balance KEY POINTS Electrolytes have multiple and varied responsibilities but are unable to function
80 Vol. 22, No. 2 February 2001 Peer-Reviewed CE Article #2 ELECTROLYTES, Fluids, and the Acid Base Balance KEY POINTS Electrolytes have multiple and varied responsibilities but are unable to function
PACKAGE LEAFLET: INFORMATION FOR THE USER. CALCICLO STEROP 11 meq 10 ml Solution for injection. Dihydrated Calcium Chloride
 PACKAGE LEAFLET: INFORMATION FOR THE USER CALCICLO STEROP 11 meq 10 ml Solution for injection Dihydrated Calcium Chloride Read all of this leaflet carefully before you start using this medicine because
PACKAGE LEAFLET: INFORMATION FOR THE USER CALCICLO STEROP 11 meq 10 ml Solution for injection Dihydrated Calcium Chloride Read all of this leaflet carefully before you start using this medicine because
PACKAGE LEAFLET: INFORMATION FOR THE USER. SODIPHOS 22mEq / 10ml Concentrate for solution for infusion. Disodium phosphate dihydrate
 PACKAGE LEAFLET: INFORMATION FOR THE USER SODIPHOS 22mEq / 10ml Concentrate for solution for infusion Disodium phosphate dihydrate Read all of this leaflet carefully before you start using this medicine.
PACKAGE LEAFLET: INFORMATION FOR THE USER SODIPHOS 22mEq / 10ml Concentrate for solution for infusion Disodium phosphate dihydrate Read all of this leaflet carefully before you start using this medicine.
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia
 BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
CHF for Clinician. AtHomeCare.com
 CHF for Clinician AtHomeCare.com CONTACT INFORMATION FOR CLIENTS Client s Name: SOC Date: Case Manager s Name: Phone #: Physician s Name: Phone: Emergency Contact Person s Name: Phone Number: MISSION STATEMENT
CHF for Clinician AtHomeCare.com CONTACT INFORMATION FOR CLIENTS Client s Name: SOC Date: Case Manager s Name: Phone #: Physician s Name: Phone: Emergency Contact Person s Name: Phone Number: MISSION STATEMENT
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital
 Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic