OHSU. and Minor Stroke. Sierra Ford, DO
|
|
|
- James Bryan
- 6 years ago
- Views:
Transcription
1 TIA and Minor Stroke Sierra Ford, DO
2 Disclosures No financial disclosures
3 Objectives Introduction Epidemiology Assessment of possible stroke/tia History/Exam Testing Secondary stroke prevention treatments A few words on acute stroke treatments
4 Stroke facts Major cause of disability and death worldwide 5 th leading cause of death in US (moved from 4 th in 2013) ~ 130,000 Americans annually 1 of every 20 deaths 1 death every 4 minutes >795,000 strokes in the US each year ~25% are recurrent stroke Costs $34 billion+ annually in the US
5
6 Definition of Stroke Neurologic symptoms due to vascular lesion of the CNS (Brain, spinal cord, or retina) Infarct = due to ischemia ( clot ) Hemorrhage ( bleeding ) into brain (IPH), ventricles (IVH), or subarachnoid space (SAH) Non-traumatic Not SDH Not EDH Other etiologies excluded
7 Definition of Stroke Infarct / ischemic stroke - 87% Permanent injury OR 24 hours of symptoms infarct <24 hours TIA (typically <1 hour, w/o lesion on CT or?mri) Intracerebral hemorrhage (ICH), intraparenchymal hemorrhage (IPH) % Subarachnoid hemorrhage - 5% Symptoms caused by reversible edema without infarct or hemorrhage do not qualify as stroke. Neither does traumatic IPH
8 When to suspect stroke? - Timing (sudden onset) - Focal deficits - Unilateral weakness (including facial droop) and numbness - Speech impairment (aphasia, dysarthria) - Neglect - Vision impairment (field cut, diplopia) - Ataxia/incoordination, especially if unilateral - Vertigo - Loss of, or decreased level of consciousness? - Risk factors
9 Stroke risk factors Non-modifiable Modifiable Age Hypertension Gender Tobacco use Race/ethnicity Diabetes Genetic factors Dyslipidemia Migraine history Heart disease, Atrial fibrillation Lack of exercise Heavy alcohol use Drug use
10 Assessment of possible stroke/tia History: Current (and prior) symptoms with course Time of onset/lkn PMHx, medications Exam: Mental status including language assessment (fluency, naming, repetition, comprehension) and dysathria Cranial nerves (attention to visual fields, gaze preference, facial droop or subtle flattening, sensation) Motor (pronator drift, subtle weakness) and coordination Sensory including dual stimuli (inattention/neglect) Gait testing
11 Localization where is the stroke? Remember the neuro-anatomy What brain regions could cause the sx? Is there a single region to explain everything? What blood vessels supply that region? Clues to brainstem: Cranial nerve involvement, Clues to cortical localization: Aphasia (dominant hemisphere, Broca s or Wernicke s areas) Neglect (non-dominant parietal) Gaze deviation - towards side of stroke (frontal eye fields) Homonymous hemianopsia (typically occipital cortex) especially if multiple in similar region Diplopia, gaze palsy (CN 3, 4, and/or 6) Crossed face and body findings Really severe bulbar involvement
 ACA Contralateral leg weakness and sensory loss Disinhibition, AMS/personality changes Urinary incontinence PCA Contralateral")
12 Deficits by vascular territory MCA Contralateral hemiparesis and hemi-sensory loss (face/arm > leg) Dominant hemisphere = aphasia, non-dominant = visuospatial & neglect +/- gaze preference toward side of brain lesion +/- homonymous hemi/quadrantopsia (optic radiations) ACA Contralateral leg weakness and sensory loss Disinhibition, AMS/personality changes Urinary incontinence PCA Contralateral homonymous hemianopsia Vertebro-basilar artery Contralateral hemiparesis (face=arm=leg) Severe dysarthria, dysphagia Ataxia/dysmetria, vertigo Diplopia, nystagmus Cranial nerve deficits










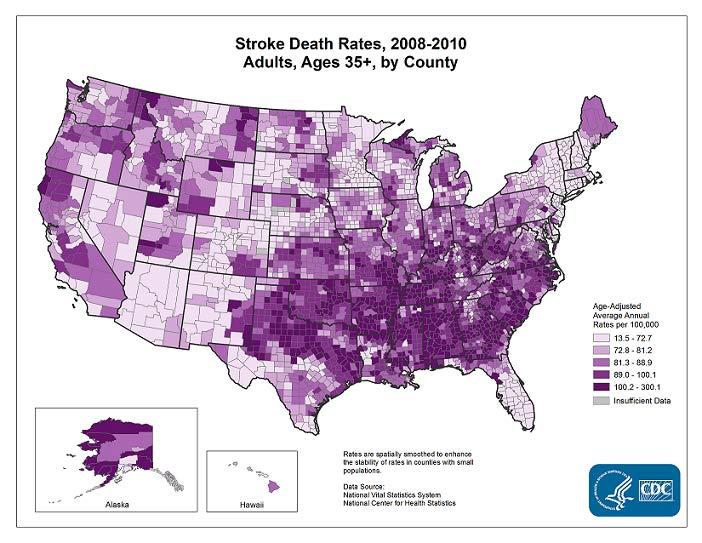
13 Pathophysiology of Ischemic Stroke Small Vessel 20% Large Artery Cryptogenic Atherosclerosis 25% 30% 5% Unusual Ischemic (87% of total strokes(us)) Cardioembolic 20% CDC.Gov
14 Pathophysiology of Ischemic Stroke Cardio-embolic 20% Embolic Athero-embolic 30% 80% Embolic, unknown source* ~25% Non-embolic (small vessel, lacunar, thrombotic, atherothrombotic) 20% Other (paroxysmal emboli, hypercoagulable state, dissection with embolism, etc) 5%
 No cortical features (*unless thalamic")
15 Localization Clues to lacunes Lacunar infarct = small infarct (2 20 mm) in the subcortical structures from occlusion of a single small perforating artery (deep cerebral white matter, basal ganglia, thalamus, or pons) No cortical features (*unless thalamic mimics)
16 Classic Lacunar syndromes: Syndrome Clinical findings Typical location (vessels supplying) Pure motor Motor deficit of face, arm, PL internal capsule (33-50%) and mildly the leg; mild (Lenticulostriate branches, MCA) dysarthria or pons (pontine perforators, BA) Ataxic hemiparesis Weakness and clumsiness of Pons or PLIC (2 nd most the arm and leg, often gait common) changes Clumsy handdysarthria dysdiadochokinesia of the BA) Ataxia, dysmetria, or Basilar pons (pontine perforators, distal upper limb with dysarthria Pure sensory Mixed sensorimotor Sensory deficit (numbness, tingling, pain, or burning) of face/arm/leg Hemiparesis and hemibody sensory deficit Thalamus (PCA branches) Lateral pons or thalamocapsular region Bamford, J et al. Stroke 1987
17 ABCD 2 score Risk assessment tool to predict short term stroke risk after TIA Developed out of UCSF Optimized to assess the 48 hr (2 day) stroke risk, but also gives the 7 day and 90 day stroke risk Higher ABCD 2 scores are associated with greater risk of stroke after TIA Low risk: hospital observation may be unnecessary without another indication Moderate risk: consider hospital observation or urgent assessment and risk factor control High risk: hospital observation often worthwhile Johnston et al, Lancet, 2007.
18 ABCD 2 score Criteria Value Points Age 60 years 1 <60 years 0 BP 140/90 1 <140/90 0 Clinical Unilateral weakness 2 features Speech disturbance without weakness 1 Other 0 Duration of 60 minutes 2 symptoms minutes < 10 minutes 1 0 Diabetes hx 1 Score ranges 0 to 7 Johnston et al, Lancet, 2007.

19 ABCD 2 score and risk calculation Risk Score Prevalence of stroke group 2 days 7 days 90 days Low % 1.2% 3.1% Mode % 5.9% 9.8% rate High % 12% 18% Johnston et al, Lancet, 2007.
20 Higher risk features of TIA Stuttering symptoms Concerning for recurrent occlusion and recanalization of vessel (high grade carotid stenosis or impending occlusion of small vessel) ABCD 3 gives 2 points if dual TIA (within last 7 days) Positive neuroimaging correlate MRI with diffusion restriction (imaging stroke) High risk carotid lesion: identification of >50% stenosis of ICA ABCD 3 -I score gives 2 points for DWI positive lesion and 2 points for ICA stenosis >50%
21 ABCD 2 vs ABCD 3 score Criteria ABCD 2 ABCD 3 Age 60 years 1 point 1 point BP 140/ Clinical features - Unilateral weakness Speech disturbance w/o weak. 1 1 Duration of symptoms ABCD 2-60 minutes minutes 1 1 Diabetes hx 1 1 Dual TIA (hx preceding TIA 7d) NA 2 Imaging: ipsilateral ICA 50% sten. NA 2 Imaging: DWI correlate NA 2 Total possible Bo Song et al, Stroke Kaplan Myer Survival Curves: ABCD 3
22 Workup of possible stroke/tia Urgent assessment: Evaluation within 12hrs and all testing within 48hrs if possible Labs: CBC, electrolytes and Cr, fasting glucose, lipids, A1c* CT head, ±MRI Vessel imaging (Carotid ultrasound*, CTA, MRA, or cerebral angiogram) *carotid U/S does not evaluate the posterior circulation ECG/telemetry, 30 day cardiac monitor TTE

23 Common Stroke Mimics 38.6% of acute stroke patients in a 6 hour time window were found to have a stroke mimic in a recent study (193/498 patients) Rother et al. Stroke 2014
24 Treatment Acute treatments: TPA not given for TIA or minor stroke (NIH ~4) Mechanical thrombectomy Long-term secondary prevention: Antithrombotic agent Hypertension control Lipid control Diabetes control Lifestyle modification: Physical activity Diet Smoking cessation Weight management
25 Antithrombotic agents Depends on the etiology Thrombotic (small vessel): Single antiplatelet agent* If previously on nothing, start ASA 81mg If already on ASA, advance to clopidogrel (consider 5 day overlap or load) Dipyridamole ER with aspirin (Aggrenox) approved for prevention of recurrent stroke, however often poorly tolerated (headaches)
26 Antithrombotic agents CHANCE trial Clopidogrel vs placebo + ASA x 21d TIA and minor stroke w/in 24h Stroke risk: PLX group 8.2%, PBO group 11.7%, p<0.001 Hemorrhage risk (systemic and ICH) 0.3% both groups Applicable? POINT trial: active/ongoing trial sponsored by NIH High risk TIA or minor stroke w/in 12h Clopidigrel vs placebo + ASA x90 days CHANCE trial, NEJM 2013
27 Antithrombotic agents Depends on the etiology Cardio-embolic (AF, cardiac thrombus, mechanical valve): Anticoagulation (warfarin, apixaban, rivaroxaban, dabigitran, edoxaban, heparin, fondaparinux, etc) All patients with non-valvular atrial fibrillation should be anticoagulated to reduce stroke (CHADS2 or CHADSVASc score 2) ASA is not really effective in atrial fibrillation
28 Oral AC vs Aspirin European Atrial Fibrillation Trial: 1007 pt s with non-rheumatic Afib and recent TIA/minor stroke, AC (warfarin, goal INR 3 (2.5-4%)) vs ASA 300mg vs placebo Primary endpoint: Annual rate of vascular event (vascular death, stroke, MI, or systemic embolism) 8% in AC group vs 17% in control group (HR 0.53), p= % in ASA group vs 19% in placebo (HR 0.83), NS difference p=0.12 Low annual major bleeding risk both groups (AC 2.8% vs ASA 0.9% vs PBO 0.7%, p<0.001) AC more effective than ASA 90 events prevented if 1000 pt s treated with AC for 1 year, major bleeds 21 per 1000 pt s Only 40 events prevented if 1000 pt s treated with ASA for 1 year European Atrial Fibrillation Trial, Lancet, 1993

29 Oral AC vs Aspirin Annual stroke rates 4% in AC vs 12% in control group HR 0.34, RRR 66% p< highly significant! 10% in ASA group vs 12% in placebo HR 0.86, RRR 14% p=0.31, NS difference European Atrial Fibrillation Trial, Lancet, 1993
30 NOAC agents vs Warfarin for nvaf Individual NOAC agent studies were underpowered, trend toward benefit over warfarin* RE-LY (Dabigitran) ROCKET AF (Rivaroxaban) ARISTOTLE (Apixaban) ENGAGE AF Meta-analysis (Endoxaban) showed benefit for NOAC agents over warfarin Ruff et al. Comparison of efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomized trials. Lancet 2014.
31 NOAC vs Warfarin Meta-analysis Primary endpoint: 19% reduced risk for stroke or systemic embolism, p< % reduced risk for ischemic stroke, p= % reduced risk for hemorrhagic stroke, p< % reduced risk of death (all cause mortality), p= % lower risk of ICH, p<0.0001, but 25% increased risk of GI bleed, p=0.043 Ruff et al. Comparison of efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomized trials. Lancet 2014.
32 NOAC vs Warfarin Meta-analysis Aggregate risk of major bleeding with a non-significant trend toward lower risk (14% RRR, p=0.06) Individual trials major bleeding shows significantly lower in ARISTOTLE (Apixaban) and ENGAGE AF-TIMI 48 (Endoxaban), and trend lower for RE-LY (Dabigitran) OR of GIB: apixaban 1.23, dabigatran 1.58, endoxaban 0.31, rivaroxaban 1.48 Ruff et al. Comparison of efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomized trials. Lancet 2014.
33 Antithrombotic agents Depends on the etiology Athero-embolic (stenosis 70% in supplying vessel, 50% in ICA) Dual antiplatelet (aspirin + clopidogrel) for 3 month period* (longer is harmful), followed by single antiplatelet lifelong Symptomatic carotid stenosis is often recommended for surgical treatment (CEA, stent for selected patients) Medical therapy can be used for high risk cases or poor surgical candidates Vertebral or intracranial atherosclerosis are treated with medical management initially Stenting in this population is no longer recommended until failure of medical therapy, and is currently being studied for this population
34 Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade stenosis, NEJM, Randomized trial of endarterectomy for recently symptomatic carotid stenosis: Final results of the MRC European Carotid Surgery Trial (ECST), Lancet, Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis, NEJM, Surgical intervention for carotid disease Symptomatic carotid stenosis >50% has been shown to benefit from urgent CEA (or CAS*) NASCET trial CEA reduced ipsilateral stroke, major stroke, and death in patients with symptomatic carotid stenosis 70-99% Ipsilateral stroke at two years: 26% medical arm vs 9% surgical arm (ARR 17%, p<0.001) Major/fatal ipsilateral stroke, 13.1% medical arm vs 2.5% surgical arm (ARR 10.6%) ECST trial: showed benefit at 80% stenosis Follow-up analysis of the NASCET trial data showed more modest benefit for 50-69% stenosis Ipsilateral stroke at 5 years 15.7% surgical arm vs 22.2% medical arm (ARR 6.5%, p=0.045), NNT 15 This same trial showed no statistical benefit for patients with <50% stenosis. Stenting is accepted for patients with high operative risk, due to major stroke and death rates being similar. Classically, it is believed that CEA has higher MI risk and CAS has higher stroke risk
35 Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade stenosis, NEJM, Randomized trial of endarterectomy for recently symptomatic carotid stenosis: Final results of the MRC European Carotid Surgery Trial (ECST), Lancet, Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis, NEJM, Surgical intervention for carotid disease Symptomatic carotid stenosis >50% has been shown to benefit from urgent CEA or CAS*, within 2 weeks NASCET trial CEA reduced ipsilateral stroke, major stroke, and death in patients with symptomatic carotid stenosis 70-99% Risk of any ipsilateral stroke at two years were 26% in medical arm and 9% surgical arm. ARR 17% (P<0.001). For a major or fatal ipsilateral stroke, the corresponding estimates were 13.1% and 2.5 % an absolute risk reduction of 10.6%. ECST trial: showed benefit at 80% stenosis Follow-up analysis of the NASCET trial data showed more modest benefit for 50-69% stenosis 5 year rate of ipsilateral stroke of 15.7% in surgical arm and 22.2% in medical arm. ARR 6.5% (P=0.045), NNT 15 (5 years) This same trial showed no statistical benefit for patients with <50% stenosis. Stenting is accepted for patients with high operative risk, due to major stroke and death rates being similar. Classically, it is believed that CEA has higher MI risk and CAS has higher stroke risk Kaplan Myer curves, >70% stenosis:
, Lancet, 1998.")

36 Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade stenosis, NEJM, Randomized trial of endarterectomy for recently symptomatic carotid stenosis: Final results of the MRC European Carotid Surgery Trial (ECST), Lancet, Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis, NEJM, Surgical intervention for carotid disease Symptomatic carotid stenosis >50% has been shown to benefit from urgent CEA or CAS*, within 2 weeks NASCET trial CEA reduced ipsilateral stroke, major stroke, and death in Stay patients with tuned: symptomatic carotid There stenosis 70-99% are ongoing trials Risk of any ipsilateral stroke at two years were 26% in medical arm and 9% surgical arm. ARR 17% (P<0.001). looking For a major or fatal ipsilateral asymptomatic stroke, the corresponding estimates carotid were 13.1% and 2.5 % an absolute risk reduction of 10.6%. ECST trial: showed benefit at 80% stenosis Follow-up stenosis analysis of the (CREST-2), NASCET trial data showed and more there may modest benefit for 50-69% stenosis be 5 year rate trials of ipsilateral in stroke the of 15.7% in future surgical arm and for current 22.2% in medical arm. ARR 6.5% (P=0.045), NNT 15 (5 years) This same trial showed no statistical benefit for patients with medical <50% stenosis. management vs surgical Stenting is accepted for patients with high operative risk, due to major stroke and death rates being similar. Classically, it is intervention believed that CEA has higher MI risk and CAS has higher stroke risk Kaplan Myer curves, >70% stenosis:
37 Antithrombotics for the other categories Very dependent on etiology Most often single antiplatelet is enough for secondary stroke prevention Ongoing ESUS trials comparing AC with ASA PFO closure? Not typically recommended unless young patient with multiple recurrent strokes
38 Treatment of other modifiable risk factors: Hypertension control Goal BP <140/90 for all stroke patients as outpatient Permissive HTN while admitted or for initial hours (perfusion of pneumbra) Lipid control Goal LDL <100 for all stroke patients (high dose*) <70 for athero-embolic strokes, or if significant other vascular risk factors Diabetes control A1c as near-normal as possible, <7 Evaluation for OSA (high comorbidity rate) AHA guidelines for prevention of stroke stroke.ahajournals.org/content/45/7/2160 SPARCL trial, NEJM 2006
39 AHA guidelines for prevention of stroke, stroke.ahajournals.org/content/45/7/2160 Lifestyle modification after stroke AHA guidelines stress the importance of lifestyle modifications. Physical activity 40 minutes of moderate to vigorous physical activity at least 3-4 days a week Diet Mediterranean diet (emphasis on vegetables, fruits, and whole grains and includes low-fat dairy products, poultry, fish, legumes, olive oil, and nuts; limits intake of sweets and red meats) can reduce stroke up to 18% Smoking cessation Weight management (given effect on CV risk factors) Alcohol use should be limited to light to moderate consumption (2 drinks per day for men and 1 per day for women)



40 A few words about what we are doing for acute stroke therapies







41 Stroke Therapy Timeline Prayer IV tpa IA tpa MERCI/ Solitaire Penumbra /TREVO 1996 (offlabel) Until /
 - NIHSS 34 21 Poor outcomes - Sx ICH 6.4 0.6 NNH 17.2** - Mortality 17 21 Lower?")
42 NINDS trial: tpa in stroke Given within 3 hrs from LKN (select population eligible) tpa (%) Placebo (%) Favorable outcome at 3 mos - Rankin NNT 3.1 (improve by 1+ grades on mrs) - NIHSS Poor outcomes - Sx ICH NNH 17.2** - Mortality Lower?! (NS) ** NNH for worsened outcome on modified rankin related to SICH is between 29.7 and 40.1 NEJM 1995
43 ECASS-3 trial: tpa hours 90 Day Outcomes: Placebo (%) rtpa (%) Rankin 0, NNT 14.2, p = 0.04 NIHSS 0, p = 0.04 Mortality 8% 8% Not that statistically significant! Symptomatic ICH 4% 8% NNH 25 (vs placebo) Higher ICH risk both groups (longer time) # patients treated per ICH that occurs: Hacke, W. NEJM 2008
44 Large vessel occlusions Common: 40-50% of all ischemic stroke Severe: 5x higher mortality, 3-fold reduction in good outcome Respond poorly to intravenous thrombolytic (tpa) Successful opening of occlusion by IV tpa: Middle Cerebral Artery: 35% Carotid Terminus: Less than 10% Successful opening of the artery associated with improved outcome

45 Riedel et al. Stroke 2011 Successful opening of artery and good outcome 138 Patients Acute MCA occlusion All treated with IV-tPA GOOD OUTCOME AT HOSPITAL DISCHARGE 8% Good Outcome If Artery Did Not Open 66% Good Outcome If Artery Did Open
46 Khatri P et al. Neurology 2009 Saver J. Stroke 2006 Time is brain Probability of good clinical outcome over time to technically successful angiographic reperfusion risk The typical LVO patient loses 2 million neurons/min in the territory at




47 Early Randomized clinical trials NEW ENGLAND JOURNAL OF MEDICINE, FEB clinical trials did NOT show benefit of endovascular stroke treatment compared to intravenous tpa treatment. Why? 1. Poor patient selection (Not selected with CT angiography.) 20% of patients randomized to IA had no thrombus 2. First generation mechanical devices did not work better than intravenous tpa. Devices successful 30-45% of the time. IV tpa successful 30-40% of the time.







48 Modern Randomized clinical trials NEW ENGLAND JOURNAL OF MEDICINE, Improved Outcomes Faster Careful times selection Better study design Improved Outcomes Newer devices
49 5 positive Thrombectomy trials in 2015 Trial Outcome Control group (% with outcome) Intervention Group (%) MR CLEAN MR 0-2 TPA* 19% TPA*/INR 33% ESCAPE MR 0-2 TPA 29% TPA/INR 53% EXTEND-IA MR 0-2 TPA 40% TPA/INR 71% SWIFT PRIME MR 0-2 TPA 35% TPA/INR 60% REVASCAT (up to MR 0-2 Control group* 29% INR group 45% 6 hours) (TPA in 80%) (TPA in 70%) TPA* If eligible

50 Number Needed to treat
51 New AHA Guidelines 2015 Endovascular therapy with a stent retriever is recommended (Class 1 Level A) Proximal MCA or ICA occlusion Within 6 hours of symptom onset We have a New Standard of Care for Stroke!
52 Recent Case Example 65yo F, acute onset ALOC with bilateral upper ext weakness with vertigo at 8:30am. Outside ER, Telestroke activated NIHSS was 15 IV tpa given ~11:00 am Worsened somnolence prior to transfer, intubated Transferred to directly to CT
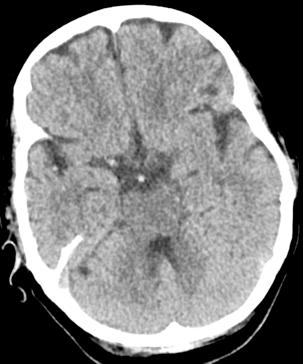


53 Transferred to NIHSS on arrival 19X (X=intubated)


54 Angiography


55 Angiography
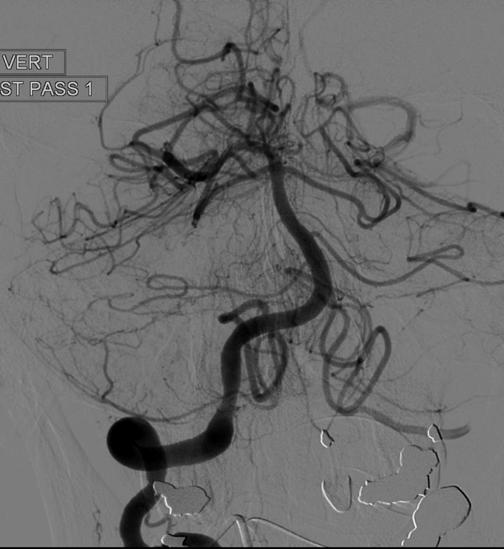

56 Post-Thrombectomy Run

57 CTH 24hr-Post Procedure TICI3 Revascularization (Complete) at 5 hours from onset After Extubation, NIHSS 1 for dysarthria 48 hours post, was NIHSS 0

58 Questions?
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Stroke and TIA. Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne
 Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke P A C I F I C N E U R O. O R G
 Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Stroke Update. Claire J. Creutzfeldt, MD January 12, 2018
 Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Ischemic stroke: management, prevention and follow up. Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute
 Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Long-Term Care Updates
 Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
INTERVENTIONAL MANAGEMENT OF ACUTE ISCHEMIC STROKE: THE EXCITING 1 ST DAY
 INTERVENTIONAL MANAGEMENT OF ACUTE ISCHEMIC STROKE: THE EXCITING 1 ST DAY Hormozd Bozorgchami, M.D. Assistant Professor Department of Neurology Dotter Interventional Institute Oregon Health and Science
INTERVENTIONAL MANAGEMENT OF ACUTE ISCHEMIC STROKE: THE EXCITING 1 ST DAY Hormozd Bozorgchami, M.D. Assistant Professor Department of Neurology Dotter Interventional Institute Oregon Health and Science
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,